Download - Siemens Healthcare
Download - Siemens Healthcare
Download - Siemens Healthcare

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Medical SolutionsThe Magazine for <strong>Healthcare</strong> LeadershipMay 2010 – US editionMedicine in 2050How today’s babies will grow into the future of healthcare
Will Jimmy be able to afford goodmedical care when he is my age?The world needs better and more affordable healthcare. That’s whywe’ve developed better technologies and more efficient IT solutions.With life expectancy on the increase, healthcare is becoming more expensive. We offer innovative solutions to improve the qualityof care and streamline hospital processes before, during and after treatment. From imaging and lab systems that help providemore accurate diagnosis to managing hospitals more efficiently, we can save money that can be put to better use – saving lives.siemens.com/answersA91CC-9084-A1-7600
EditorialTransforming <strong>Healthcare</strong>In a time of unprecedented global focuson healthcare delivery, healthcare systemsall over the world seem to have agreedon a common denominator: completeoverhaul! <strong>Healthcare</strong> reforms are beingtriggered or are already underway inmany societies. And, as different as theirscopes and debates may be, reforms ofhealthcare systems are largely drivenby the need to increase access to healthcare,improve the quality of care, anddecrease costs.These demands will be both challengedand supported by incisive societal developmentsand groundbreaking innovationswithin the next 40 to 50 years. Demographicswill change dramatically, medicinewill develop from reactive to morepreventive care, and medical knowledgewill be streamlined and distributed forunlimited access worldwide. As an integratedhealthcare company, <strong>Siemens</strong> isa key driver of this trend. By means ofthe convergence of imaging, laboratorydiagnostics, and healthcare IT, we aimto transform healthcare along the entirecontinuum of care, working towardpersonalized medicine – together withyou, our customers.In light of this objective, the cover storyin this issue of Medical Solutions isdevoted to visualizing the future of healthcareup to 2050. Thinking beyond products,we asked healthcare experts fortheir perspectives: How will patientsbenefit from medical progress in thefuture, and what can they expect fromtheir respective healthcare systems?How can healthcare providers integrateadvances in medical technology for preventionand early diagnosis while optimizingcosts at the same time? Frommolecular medicine through reimbursementdiscussions to data management,you will get an exciting, multi-perspectiveview on healthcare in 2050. Start offwith following the fictitious, 2010-bornbabies Peter and Louise on their journeysthrough future healthcare systems onpage 12.Further into the magazine, several storiesshow how our successful customersare already working toward advancinghealthcare in their countries.As an example, the Sourasky MedicalCenter in Israel (page 42) shows howthe organizational convergence betweenhospitals, technology innovators, andgovernment regulators efficiently supportsimproving a healthcare system.Together with nine other governmentalhospitals, Sourasky Medical Centerimplemented the hospital informationsystem i.s.h.med in the course of aHermann Requardt,Member of the Managing Board of <strong>Siemens</strong> AGand CEO of the <strong>Healthcare</strong> Sectorgovernmental hospital computerizationproject. Clinical departments at Souraskynow benefit from the interoperability ofa common data platform. Simultaneously,the hospital and the Ministry of Healthare already working with <strong>Siemens</strong> todevelop two additional i.s.h.med modulesto further incorporate the needs of differenthealthcare facilities participatingin the project.I hope you will enjoy reading this issueas an example of <strong>Siemens</strong>’ true commitmentto partnering with our customers inshaping tomorrow’s healthcare systems!Sincerely,Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine 3
ContentContent28BRAHMS procalcitonin:Identifying Sepsis Patients Early34Hybrid Rooms:Trauma TreatmentCover Story03 Editorial10 Catching a Glimpse of <strong>Healthcare</strong> in 2050Within the next 40 to 50 years, medicinewill face many challenges, prospects, andgroundbreaking technological developments.Medical Solutions took a step forward andasked experts to look into the future of healthcareup to 2050. We accompany fictitiousbabies Peter and Louise as they grow up intohealthcare systems of the future and giveoutlooks on healthcare IT, branding in healthcare,and reimbursement. Finally, twoexperienced representatives of the healthcareindustry and medical research sharetheir view on the future of medicine.06 News70 Essay Series:Germany75 Further Reading80 Imprint81 Subscription4 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Content52PET-CT:Enhancing <strong>Healthcare</strong> in Serbia62Intraoperative 3D Scans:Better than Good in the ORFeatures24 Rural healthcare facilities oftentake a backseat when it comes tostate-of-the-art mammographytechnology and workflow. DickinsonCounty <strong>Healthcare</strong> System provesthe opposite.28 The measurement of BRAHMSprocalcitonin, a diagnostic biomarker,aids clinicians in identifying patientswith sepsis and has also beenshown to reduce unnecessary antibioticuse.34 Karolinska University Hospital inStockholm has built one of theworld’s first hybrid rooms dedicatedto treating trauma patients.38 The innovative Center for Orthopedicsand Sports Medicine in Munichis dedicated to advancing knowledgeand diagnostic technology inthe field of sports medicine.42 After implementing the hospitalinformation system i.s.h.med,the Sourasky Medical Center inTel Aviv experienced a boost inefficiency.46 Cedars-Sinai Medical Center and<strong>Siemens</strong> collaborate to improvethe identification of cardiovasculardisease with molecular imaging.52 The National PET Center in Belgradewas planned and suppliedin turnkey condition by <strong>Siemens</strong> aspart of a governmental initiativeto introduce molecular imaging inSerbia.56 Regarding service for its medicalequipment, the Nuremberg Hospitalrelies on the <strong>Siemens</strong> GuardianProgram, as part of which the Tube-Guard option plays an importantrole.59 Denver Health was an early adopterof CPOE ten years ago. Now, with95 percent of orders entered electronically,the hospital is taking itsprocess to the next level by migratingto the <strong>Siemens</strong> Soarian platform.62 Intraoperative 3D imaging is avaluable process control during surgeryto achieve better clinical outcomes,as surgeons at the BG TraumaHospital Ludwigshafen confirm.67 Flexible financing options offeredby <strong>Siemens</strong> Finance & Leasingenabled the Diagnosticum Ingolstadt,a state-of-the-art radiology practice,purchase the latest in diagnosticimaging.Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine 5
NewsOnline Subscription for CADExpanding the <strong>Siemens</strong> portfolio of computer-aided detection(CAD) applications, <strong>Siemens</strong> launched a Software as a Service(SaaS) model for chest X-ray (CXR) at the European Congressof Radiology (ECR). syngo® CXR CAD Subscription 1 works inconjunction with digital radiography systems, such as Ysio andAXIOM® Aristos, and allows clinicians to receive CAD resultsvia remote processing.Similar to receiving an online subscription for a medical journal,the technology is available on demand and at the clinician’s convenience.For the initial deployment, syngo CXR CAD Subscriptionwill be available with the Ysio for a seamless CAD workflowexperience. A separate workstation is no longer requiredto be installed in a clinic or practice, and offsite processingoccurs remotely on a <strong>Siemens</strong>-owned server. Users will alsohave automatic access to syngo CXR CAD Subscription updates.“syngo CXR CAD Subscription is the next step toward a fullyintegrated, virtualized imaging environment,” said PeterHerzog, MD, attending physician, Amper Kliniken AG, Germany.The client software extracts a CAD Image Signature (CIS)from the digital image, which contains the necessary informationfor the CAD algorithm to process the image and produceCAD results. The CIS does not contain any private information,such as patient name and date of birth. The CAD results arethen transferred back to the clinic or practice, where they areappended to the corresponding patient and stored in an applicationsuch as the picture archiving and communication system(PACS). This makes the CAD data available to the doctoras a “second reader” for the detection of lesions.syngo CXR CAD works as a second reader to help the cliniciandetect potential lung nodules. Validated for use with computedradiography (CR)/digital radiography (DR) systems, the applicationis used for the analysis of digital radiographic images ofthe thorax. syngo CXR CAD helps detect potential nodules fromeight to 30 millimeters in size.“When reviewing chest X-ray, CAD helps identify larger nodulesthat are partially obscured by superimposed structures,” saidHerzog. “The use of CAD tools can substantially help reducethe number of lesions missed during routine X-ray readings.”With syngo CXR CAD Subscription, <strong>Siemens</strong> provides updatesfor the CAD algorithms on its servers for improved detectionperformance. The date of the algorithm release used is shownnext to the version number on the resulting radiographic image.Herzog is excited about the new dissemination method forCAD tools. “In the future, the use of CAD will be a standard ofcare in almost all modalities,” he concluded.1Not available for sale in the U.S. For availability in other countries, please check withyour <strong>Siemens</strong> representative.Cardiology Care in the Heart of AfricaIn summer 2009, Francesco Gentile, MD, Director at the CardiacHospital Bassini in Milano, Italy, installed a temporary cardiologycenter in Mambasa, Democratic Republic of the Congo. For hismission, Gentile was provided with the first dedicated personalimaging tool designed to enhance the physical exam – the<strong>Siemens</strong> ACUSON P10 ultrasound system, which assisted himin overcoming the tough working conditions in Mambasa.The ACUSON P10 system revolutionizes clinical assessmentat the point of care by improving patient care, workflow, andoutcomes in cardiology, emergency medicine, and obstetrics.With a start-up time of only about ten seconds and exceptionalimage quality, the ACUSON P10 system helps physicians makefaster and more confident diagnoses. The system, whichonly weighs 700 grams, helped Gentile examine almost 200patients in about 14 days – not only in the hospital center,but also in the surrounding jungle area. Having been informedabout the temporary station, the local population made useof Gentile’s medical expertise every day from 8:30 a.m. to4:00 p.m. A broad range of diseases were diagnosed, includinghigh blood pressure and cardiac valve dysfunction. Thanksto Gentile’s readiness to help others and with support from<strong>Siemens</strong>, the mission in Mambasa was a great success.Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine 7
NewsOne Mouse, One Keyboard,One MonitorAfter the market introduction of the Artis zee® LargeDisplay for the examination room last year, <strong>Siemens</strong>now clears up control room space with a new 30-inch(76.2-centimeter) display to control multiple systemsduring interventions.Today’s interventional control room is the hub formultiple data sources and systems. With this comesthe need to visualize and interact with many differentwork consoles, leading to numerous monitors, keyboards,and mice. The information these systems provideis vital to support the interventionalist duringprocedures, but leads to many different points of control– sometimes resulting in a more complex workflowand a cluttered environment.The new Artis zee Cockpit can put an end to this. Itconsolidates the various imaging and data signalsrouted to the control room into one 30-inch medicalgradedisplay. Fast, simple, and user-intuitive operationsupports efficient workflows. The user can choose thelayout of the display to meet the requirements of theprocedure and move the sources around the screenas required. A double click on any screen lets the usertake complete control of that system, all with onemouse, one keyboard, and one monitor. And just asimportant, Artis zee Cockpit frees up valuable spacein the department.The solution is available for use with the Artis zeeportfolio of interventional radiology, cardiology, andsurgery systems. These are available in biplane, multiaxial,ceiling-mounted, floor-mounted, and multipurposeconfigurations.www.siemens.com/artis-zee-cockpitAnterior wall myocardial ischemia with reduced blood flow at peakstress periodNew PET ApplicationHelps Detect CoronaryArtery Diseasesyngo® Dynamic PET with Myocardial Blood Flow, a newcardiac imaging software application for <strong>Siemens</strong>’ industryleadingBiograph PET·CT (positron emission tomography/computed tomography) scanners, may have significant impacton the diagnosis of patients with advanced coronary arterydisease (CAD) – specifically, in patients with multivessel diseaseor in those who are asymptomatic. Offering a new method forquantitatively evaluating the extent of ischemia via high-performancePET/CT imaging and advanced applications, this firstsoftware from a major vendor enables the more definitivemeasurement of myocardial blood flow during PET perfusionstudies as compared to regular myocardial perfusion studies 1 .Clinical literature estimates that five to ten percent of CADpatients have balanced vessel disease, and up to eight percentare asymptomatic at-risk patients. Especially within this highriskgroup, the new software offers additional diagnostic value.Specific quantification of perfusion levels in each vessel canhelp improve the identification of multi-vessel disease.According to Britta Fünfstück, CEO Molecular Imaging,<strong>Siemens</strong> <strong>Healthcare</strong>, syngo Dynamic PET also supports effectivecost management: “Technological innovations, such asthe ability to quantify blood flow in at-risk patients, continueto reinforce the critical role that molecular imaging can playin the delivery of high-quality, cost-effective healthcare.”The 30-inch medical-grade display of the Artis zee Cockpitprovides more space in the control room.1Data on file8 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
NewsTaking UltrasoundImaging to the NextLevelThe 2.0 release of the ACUSON S2000 ultrasound systemoffers significant advancements. Best-in-class image qualityand diagnostic confidence combined with innovative applicationsand knowledge-based workflow efficiencies provideadvanced solutions for the most demanding clinical environments.<strong>Siemens</strong>’ implementations of Acoustic Radiation Force Imaging(ARFI), Virtual Touch Tissue Imaging and Virtual TouchTissue Quantification 1 , have been further optimized on the2.0 release of the ACUSON S2000 ultrasound system. Theseexclusive Strain Imaging applications expand the use of ultrasoundby allowing a classification of tissue stiffness oftenassociated with pathology.Furthermore, the system integrates advancements forCadence contrast pulse sequencing technology 2 , providingexceptional sensitivity. Knowledge-based applications suchas eSieScan Workflow Protocols enhance clinical workflowsand reduce exam times, enabling better throughput andVirtual Touch Tissue Quantification of a liver hemangiomaimproved consistency. The new HD Zoom feature enablesdetailed examination of small anatomical regions, whileadvanced fourSight imaging technology offers comprehensive3D/4D acquisition, data rendering, and postprocessing.1Not available in the U.S.2At the time of publication, the U.S. Food and Drug Administration has clearedultrasound contrast agents only for use in LVO. Check the current regulation for thecountry in which you are using this system for contrast agent clearance.Tips and Tricks for MR Orthopedic ImagingThe “Advisory BoardOrthopedic Diagnostics”now providesoptimized parametersand protocols forOrthopedic andMusculoskeletal (MSK)magnetic resonanceimaging (MRI) on the<strong>Siemens</strong> MAGNETOM®World Website.<strong>Siemens</strong>’ commitmentto innovation in MRtechnology is notrestricted to the development of new products or solutions; itincludes the examination of existing MR imaging parametersand protocols. The Advisory Board members – seven top expertsin the field of MSK imaging – work with <strong>Siemens</strong> in order toachieve these goals. During RSNA 2009 (the Radiological Societyof North America’s 2009 Annual Meeting), they launched theirWeb presence, offering a unique platform to share insightsfrom daily practice and research experiences with <strong>Siemens</strong>customers worldwide. Detailed protocols, phoenix images, andapplication tips including videos are available for ankle, elbow,hip, knee, shoulder, and wrist exams with MAGNETOM Avanto,Trio, and Verio systems.All board members are open to contacts and happy to answerspecific questions. The information provided helps MAGNETOMcustomers keep up-to-date as well as speed up their examinations.As a result, they might also increase throughput. And inthe daily routine, patients benefit from the latest technologicaladvancements. By combining valuable clinical information from<strong>Siemens</strong> with the Advisory Board’s tips and tricks, MAGNETOMWorld is helping physicians get the best out of their system.www.siemens.com/magnetom-worldMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 9
Catching a Glimpseof <strong>Healthcare</strong> in 2050Within the next 40 to 50 years, medicine will face many challenges,prospects, and groundbreaking technological developments.Demographics will change dramatically, and medicine will developfrom reactive to preventive care. <strong>Healthcare</strong> systems are alreadyin a state of transition today. What kind of care will today’s babiesexperience as they grow older? Medical Solutions takes a stepforward and asks experts to look into the future of healthcare.Overview:12 A Future Scenario: The journey of Peter and Louise through healthcare systems of the future14 Opinion on Brands: How will healthcare providers convince their “consumers”?17 <strong>Healthcare</strong> IT: What lies ahead for electronic health records and information technology?18 Reimbursement: Who will pay for the future of healthcare?21 Discussion: Two “elder statesmen“ from healthcare academia and industry talk about their viewson healthcare 2050
<strong>Healthcare</strong> in 2050The story of Peter and Louise and theirjourneys through the changing healthcaresystems of the future.By Linda BrookesGrowing Up IntoPreventive CareSee imprint on page 80 for a listing of experts whoprovided input for the composition of this scenario.In 2010, a girl, let’s call her Louise, anda boy, whom we’ll call Peter, are bornto two families. This is the story of howadvances in healthcare could impact thelives of these two babies as they growup over the coming decades. Both ofthem are fortunate: their parents livein developed countries that have nationwidehealthcare systems intended tocover the whole population. However,the success of these systems in keepingLouise and Peter in good health will dependon a number of factors, includingadvances in medical and technologicalresearch, and how these will be incorporatedinto future healthcare services.Despite living in comparatively highincomecountries, Louise and Peter mayhave different experiences within thehealthcare system. Louise’s family is welleducatedand relatively wealthy, withsufficient means of purchasing additionalhealthcare above the basic services guaranteedby their provider. Peter’s accessto healthcare is less secure because hisfamily receives its healthcare throughhis father’s temporary employment. IfPeter’s father loses his job, he could loseaccess to all but basic healthcare. Louise’sparents do not smoke, avoid junk food,moderate their alcohol intake, and exerciseregularly; Peter’s parents live a lesshealthy lifestyle. Children usually followthe example of their parents.Louise’s parents are concerned that shemay be at risk for breast or ovarian cancerlater in life. Genetic testing has revealedLouise’s mother has a breast cancersusceptibility gene 1 (BRCA1) mutation.This means her chance to develop breastcancer or ovarian cancer during her lifetimeis greatly increased, and she also hasa higher risk for other cancers. Louise’smother is screened regularly with ultrasound,mammography, and magneticresonance imaging (MRI) for breast cancer,as well as transvaginal ultrasound,blood test for CA-125 antigen, and clinicalexaminations for ovarian cancer.Luckily, no tumors have been identifiedto date. Louise’s parents know that theirdaughter possesses a very high risk ofhaving inherited the gene variant andare sure to have her tested as well. Thisused to involve having a blood sampletaken by a doctor and sent to a laboratoryand waiting several days for the result.Now, this is done using a portable device(“lab-on-a-chip”) and the result is availablewithin minutes. It shows that Louisedoes carry the BRCA1 variant. Her physicianassures her parents that counselingwill be available for the family and thatLouise will have regular cancer screeningfrom age 30 onward.Lifestyle DiseasesBy age ten, Peter is already overweight,like one-third of schoolchildren in12 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
<strong>Healthcare</strong> in 2050Direct Interaction Will Define Future<strong>Healthcare</strong> BrandsBy Gil BasheDuring the next 50 years, healthcare providers will face amore challenging competition that will demand perceptiblemarketing initiatives: health services will be increasinglyevaluated and selected autonomously by well-informed,responsible patients – their prospective customers. Moreover,expectations and decisions of these customers willincreasingly intertwine with the reimbursement decisionmakers’final tabulation or intuitional budget – especiallywhen the ‘pay-for-quality’ approach will be gaining groundworldwide. After all, social media and patients’ immediateability to connect and influence physicians, payers, andpolicymakers will be everyday practice.Look up any given product today – medical devices, treatments,or health services – on the Internet and you caninstantly access testimonials, conversations, and debates.Second opinions and crowd-sourcing are available atpatients’ fingertips, and are a trusted source of information.Gil Bashe, Executive Vice President, HealthPractice Director at Makovsky + Company,has devoted 30 years to helping health professionals,patients, payers, policymakers,and health-product innovators find commonground. He is coeditor of BrandingHealth Services: Defining Yourself in theMarketplace.Only the most trusted companies will have a voice in theconversation. Digital communications will not only changethe way we interact, they will alter how we act on healthcareneeds or wants. Going forward, memorable brandswill edge out competitors by incorporating immediategratification power (e.g., knowledge) into their designs.Whether for women at risk of breast cancer or patientswith a cardiovascular disease history: the considerationswill be accuracy, speed, cost, transparency, and sustainability.In the future, customers who come in contact with data,diagnosis, and health delivery will be voicing their opinionson the brand publicly and in real-time. Interacting, listening,and responding almost immediately to these patientswill be key to ensuring relevancy in their lives. These consumerswill want accurate information at eye-blinkingspeed and will increasingly attach importance to guaranteedsustainability. Personnel desires will weave togetherwith societal concerns.We will find that as Generation X and Y consumers entertheir senior years, healthcare providers and policymakerswill be confronted by consumers who react less to flashybells and whistles and are more interested in engagingin a two-way dialogue. For medical brand builders, the keyto good performance lies in the ability to communicateimmediately as much as it does in the ability to innovateconsistently. It will be all about championing customerexpectations – now.developed countries. This places him atincreased risk for future adverse healtheffects, including hypertension, hyperlipidemia,and diabetes. His grandfatherhad heart disease, and his father andmother are overweight with a body massindex (BMI) above 25, with high bloodpressure, high LDL cholesterol, and type2 diabetes. Both parents are taking appropriatemedications, but are at high riskfor cardiovascular disease. By age 20,Peter also is obese and already has highblood pressure, LDL cholesterol, highblood sugar, and high sensitivity C-reactiveprotein (hs-CRP). “Smart” pill bottlesrelay information to his doctor and pharmacistabout whether he has been adheringto his prescribed medication regimen.In 2035, Peter’s 55-year-old father haschest pain, and an ambulance is called tothe small town where he lives. His healthdata on record has already been accessedby the paramedics in the ambulance aswell as the hospital to which he will betaken. With portable technology in theambulance, the paramedics run an ECGand perform a troponin test along withother biomarkers. The ECG shows that heis having an ST segment elevation myocardialinfarction (STEMI) and that he couldbenefit from interventional revascularization.The area of infarction is identifiedby 3D echocardiography and relayed tothe cardiologist, who now knows exactlywhere the coronary artery is blockedand where to intervene. Diagnostic testsare used to assess the risk of potentialcomplications, such as bleeding, whichcan be induced by additive drugs that are14 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
<strong>Healthcare</strong> in 2050What Lies Ahead for Electronic HealthRecords and Information Technology?In the coming decades, the cost of healthcare will continueto rise as a result of increases in chronic diseasesand the aging population. Organizations that fund healthcarewill face the challenge of streamlining healthcareservices, making them more effective and keeping costsdown. A major part of this will be achieved through theglobal introduction and use of electronic healthcare records(EHRs). In the past, most EHR systems were designed torecord occasional clinical encounters between patientsand healthcare professionals and/or the diagnosis andtreatment of diseases. The next generation of EHRs willinclude a patient’s individual genome, proteome, metabolome,and health data, including results of diagnostictests, imaging, and treatment history, entered automaticallyfrom birth into computerized databases. EHRs areintended to eliminate paper records, although opinionsvary as to whether this will actually happen.Although EHRs will be managed by healthcare organizations,patients will be able to access their own personalinformation online. Authorized healthcare personnel,including emergency paramedics, will also be able toaccess patients’ EHRs directly, but will require authorizationfrom each patient to do so. Ownership of individualdata will remain with the patient. Patients will be able toaccess their own EHRs from different locations at any time.By 2050, everyone may have an implanted electronicchip containing an access code that allows wireless accessto their personal data. Patients could also use electronicdevices similar to smart phones to move data from homemonitoring devices to their EHRs. EHR databases mustbe compatible for the generation and exchange of healthinformation and data security worldwide. By 2050, it isanticipated that there will be robust global standards forEHRs based on those currently emerging in the UnitedStates and Europe.The use of the information will drive standards, whichis important not only to access information, but for theability to apply computer-modeled knowledge to it. By2050, computing power up to 100,000 times greater thanexists today will be available to provide the kind of informationtechnology needed for access and security. Inorder to address concerns about privacy, all the data willbe encrypted – by 2050, computing power will be sufficientto achieve this.The EHR database will also be used as a knowledgeengine of best practices by physicians to help them reachdiagnoses and prescribe treatment by comparing theirown patients with other, similar cases worldwide. The datacould also be made available for research – for example,for use in observational follow-up studies of drug treatments.This would afford the opportunity of studying reallifedata, as compared with data from clinical trials, toestimate the effectiveness of a specified therapy. Sincepatients would own their own data, each individualwould be able to decide whether or not their personaldata would be made available for use in this way.administerd during interventional revascularization.Peter’s father is then treatedwith percutaneous coronary intervention(PCI) with a stent.Breast Cancer TreatmentAt age 30, Louise is being monitored forbreast cancer. Imaging techniques, wheretumor-sensitive tracers are applied, specificallymammography, ultrasound, andMRI, are now able to detect tumors up toa decade earlier than tumor markers andwith less risk of false-positive results. Thescreening process is also more comfortablefor the patient. Louise’s mother hashad a positive test and undergoes treatmentat a specialist center, which she haslocated from databases comparing hospitals’success rates in treatment of hertype of breast cancer. Her treatment isbased on tailored therapy with chemotherapyand radiation delivered by nanotechnologicalmicroscopic robots thattarget malignant tumor cells with highspecificity.By 2040, high-income countries withaging populations, such as those whereLouise and Peter live, are having to copewith increased costs for treatment andlong-term care. <strong>Healthcare</strong> payers seekto prevent chronic conditions by lifestyleimprovements, and they are reluctant topay for treatment for “diseases of civilization”such as those previously sufferedby Peter and his family.Taking Personal ResponsibilityAffected by this trend, as well as hisown tests, including molecular imagingof his atherosclerosis, which shows hisown increased risk of myocardial infarction,Peter takes control of his health. Withthe help of educational material providedby his local healthcare center, he startsbicycling with his son and eating healthierMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 17
<strong>Healthcare</strong> in 2050and at home. He measures his ownblood pressure, cholesterol, blood glucoselevels, and other risk markers. Theresults are transmitted wirelessly to hisphysician and stored as part of his electronichealth record by a device he usesat home. All relevant information is automaticallytransferred to specific databasesat local and worldwide servers. WhenPeter achieves normal readings over aconsistent period, his physician receivesa ’pay-for-performance’ fee.Both Louise and Peter and their partnersdecide to have their first children testedwith genome sequencing as babies,which is now inexpensive. It reveals thediseases they are most at risk for and alsohow they would respond to a range ofdiagnostic tests and treatments. Louisealready knows that her baby daughterdoes not carry the same cancer risk asshe and her mother do. She was alreadyscreened as an embryo: neither she norher descendants will face this geneticform of breast cancer or ovarian cancerin their adult lives. Louise’s cousin, whocarries the same gene mutation, hopesthat during her pregnancy, the defectivegene can be repaired by gene therapy inutero.In 2045, new screening methods andimaging techniques have revealed thatPeter’s mother has early signs of Alzheimer’sdisease. Although no definite cureis yet available, following early detectionand definitive diagnosis, medical treatmentis available to slow down the onsetof the disease. By 2050, Louise’s mother’scancer is still in remission. She has animplantable sensor that can detect tumormarkers and relay the information to herso that she can immediately contact herphysician and begin treatment, if necessary.A new, more specific urine and genetest for prostate cancer has also allowedLouise’s father to have early, cancer-preventivevaccine treatment.The outlook for Louise and Peter andtheir children is bright. The children willbe part of the first generation to benefitfrom personalized medicine throughouttheir lives. Advances in medicine andtechnology mean that, in their countries,life expectancy in 2050 is more than 90years for women and more than 85 yearsfor men.Linda Brookes is a freelance medical writer andeditor who divides her time between Londonand New York, working for a variety of clients inthe healthcare and pharmaceutical fields.Further Informationwww.siemens.com/personalized-medicineReimbursing Quality and EffectivenessMedical Solutions asked an expert journalist to cast a look into the futureof reimbursement. Read why the ‘episode-of-care’ or ‘pay-for-quality’approach will become commonplace across the globe, while personalizedmedicine will become firmly established during the period 2030 to 2050.By Anthony BeacheyWestern European countries and theUnited States have traditionally reimbursedhealthcare providers by using a‘fee-for-service’ approach, whereby a paymentis received following the provisionof a service. However, one of the maindrawbacks of this system is that there isn’tnecessarily a relationship between theactual cost of the service and the amountof money that is reimbursed, whichinevitably has implications for cost containment.What’s more, the fee-for-service approachevolved before the advanced economiesbegan to face the increasing healthcareburden associated with aging populations.The epidemiological environmenthas partly shifted, and the highly sophisticatedtechnology commonplace todayhad yet to be introduced.Unsurprisingly, in light of demographicand other changes and its disadvantagesin terms of cost containment, the feefor-serviceapproach is now giving wayaround the globe to payment of a lumpsum for all services related to a conditionor a disease. Hence, a provider receivesa single, bundled fee for an episode ofcare, such as a hip implant, a few months’cancer therapy or the treatment of achronic disease.Certainly, the lump-sum approach facilitatesa more effective containment ofcosts than the fee-for-service concept.This is even more so with the pay-forqualityapproach, where predefined qualityindicators are strongly tied to thereimbursement and healthcare providersthus rewarded to deliver high-qualitycare. By contrast, under fee-for-service,providers are rewarded for fixing problemsthat better care might have prevented,and there are hardly incentivestied to predefined quality standards.Episode-of-care was first introduced inthe U.S. and Australia and was adoptedin Germany in 2003. The U.K. is currentlyin the process of rolling out episode-ofcarereimbursement, and it seems likelythat episode-of-care, as well as pay-forquality,will sweep across the globe in the18 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
<strong>Healthcare</strong> in 2050coming decades. Pay-for-quality is certainlygaining ground in the USA, whereepisode-of-care has already graduallytaken over from fee-for-service. Indeed,there appears little doubt that, even ifthe healthcare reform does not run asplanned, pay-for-quality will also gainground and will have certainly becomepreeminent by 2050.Pay-for-quality not for Japan?However, industry analysts that I havespoken to have cast doubt on the prospectsof the pay-for-quality approach inJapan. They argue that for cultural reasons,this strategy is less appealing tothe Japanese than to the Americans andEuropeans. It is certainly true that theJapanese generally do not embrace individualfinancial incentives (even tippingis rare), and these schemes have hadlimited success where they have beenintroduced.The system of reimbursement of healthcareproviders in Japan currently workson a points system, determined by agovernment-sponsored committee. Pointsare given for every type of medical procedureor service. Yet year-to-year, theauthorities have reduced the number ofpoints awarded in the case of every procedure,as medical costs have risen alongwith the aging population. So while aprivate healthcare provider in the U.S.will currently reimburse a patient requiringa magnetic resonance imaging examinationat a rate of around US$4,000, aprovider of the same service in Japan willreceive the equivalent of just US$500.However, it remains questionable whetherreducing fees in this manner would workin all countries. Anyone visiting Japanwill have encountered the culture of servicein that country, and healthcare professionalsare no exception. They arededicated to providing the best possibleservice in the world (and having thebest technology to accomplish this goal),despite falling payment levels.Japanese governments have also encouragedpatients to co-pay for treatment.This sum has increased from around tenpercent of a service to 30 percent currently.Authorities hope that as well asreducing the burden on the healthcarebudget, this development will encouragepatients to question what doctorsare doing, and that the country’s citizenswill no longer visit a doctor unless this isreally necessary.It is always difficult to look far into thefuture, but I think it is possible to makesome predictions with a reasonabledegree of certainty. I definitely believethat personalized medicine will becomefirmly established during the period2030 to 2050. People will benefit fromindividual diagnostic tests and treatmentand a healthcare path tailored totheir needs. Of course, this will requiremajor investments in IT so that a person’shealthcare records are available to medicalpractitioners. Indeed, they will beable to download this information frommicrochips embedded in the patient.Research Progress Saves CostTechnological advances will also havea major impact on healthcare costs andreimbursement strategies in the decadesahead. New products are already beingintroduced in imaging and other areas,which will boost standards of care andalso promote personalized medicine. Thepotential of stem cell research may havebeen realized, and stem cell technologycould be used to produce replaceabletissues or organs and to repair defectivetissues damaged by many of our mostdevastating diseases during the period2030 to 2050. Nanotechnology will alsohave revolutionized the way we detectand treat damage to the human body anddisease. Advances in molecular medicinewill allow the earlier treatment of manyillnesses and lead to new therapeuticregimens and the replacement of defectivegenes through gene therapy. Combined,these technological breakthroughsshould lead to huge cost savings.Outlook on DemographicsIt shouldn’t be forgotten that the patternof aging societies that will characterizedeveloped economies over the nextdecades will be even more distinct by2050. The share of the world populationolder than 65 may even have doubledby then, and this will have an impact ondemand for healthcare services. It alsomeans that there will be fewer taxpayers(in absolute terms and relative to theelderly) to pay for the latter’s healthcare.This development could have a significantimpact on the attitude toward reimbursementregimes in developed economies.I believe governments will adopt a numberof measures during the period 2030to 2050 to contain the pressure of risinghealthcare costs on the public purse.Germany has already adopted the copaymentapproach taken by Japan, and Ibelieve that this system could expand inother countries in the coming decades,and will have been adopted by mostcountries by 2050.Taxing IrresponsibilityTaxes on unhealthy foods and incentivesto keep fit, such as lower insurance onpeople who do not exceed a waistband/height ratio, could also be introduced.There will certainly be an increasing focuson personal responsibility over the next40 years.Of course, it is impossible to guess exactlywhat the world will be like in 2050. ButI believe the pay-for-quality reimbursementapproach will have conquered mostof the world (perhaps with the exceptionof Japan), the demographic outlook willbe far more benign than at present, andindividuals will be forced to take greaterresponsibility for their own healthcarethan is currently the case. Moreover,advances in technology will ensure thatindividuals (and their doctors) will havethe information they need to look afterthemselves and prevent serious illnessesfrom developing.Anthony Beachey worked for the BBC WorldService as an Economics Editor covering theAsia-Pacific region before embarking on a freelancecareer in 1997. He specializes in financeand economics, working for clients suchas Goldman Sachs, Threadneedle, Gartmore,J.P. Morgan, and Barclays.The opinions reflected in this article do not necessarilyreflect those of <strong>Siemens</strong> <strong>Healthcare</strong>.20 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
<strong>Healthcare</strong> in 2050Professor Erich Reinhardt, PhD (left), and Professor Detlev Ganten, MD, PhD, (right) have given impetus to progress in the healthcare industryand medical research for decades.Discussing <strong>Healthcare</strong>:Where Will We Be in 40 Years?Two long-standing representatives from the medical industry andresearch came together with Medical Solutions to talk about theirvisions of treatment, patient management, and general prospectsin future healthcare systems.By Linda BrookesIn January 2010, Professor Detlev Ganten,MD, PhD, and Professor Erich Reinhardt,PhD – representing the viewpoints ofacademia and industry, respectively – metat <strong>Siemens</strong> <strong>Healthcare</strong> headquarters inErlangen, Germany, to exchange ideasabout how healthcare is likely to developin the decades ahead. Ganten, formerlyCEO of the Charité University HospitalBerlin, is President of the World HealthSummit – an annual meeting of politicaldecision-makers, members of the scientificcommunity, and representatives ofindustry and society from all over theworld who come together to discuss globalhealthcare challenges. Reinhardt is theformer CEO and President of <strong>Siemens</strong><strong>Healthcare</strong>, and currently consultant to<strong>Siemens</strong>. Below, you can read an extractfrom their discussion.What do you consider to be themain advances in medicine by 2050?REINHARDT: I believe that by 2050,because of better understanding of disease,particularly at the molecular level,we will be able to detect diseases at veryearly stages using innovative technologiesbased on blood tests or imaging.It will be possible to predict individualresponse to treatment, which means thatwe will be able to realize so-called ’personalizedmedicine’. By 2050, we willhave seen significant progress in this field.GANTEN: Personalized medicine is basedon the concept that every individual isunique. It means making a detailed analysisby genetic testing, imaging, anddetermining biomarkers for an individualpatient, which will predict treatment success.However, there is another type ofpersonalized medicine that I alwaysemphasize, which is personal responsibilityfor health.Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine 21
<strong>Healthcare</strong> in 2050“Personal responsibilityhas to come into play:a healthcare system cannotbe expected to continuetreating a person for up to40 years for diseases ofcivilization.”Professor Detlev Ganten, MD, PhD, CEO of Charité University HospitalBerlin until 2008, Chair of the Charité Foundation, Berlin, Germany“By 2050, we will be ableto detect diseases at veryearly stages using innovativetechnologies basedon blood tests or imaging.”Professor Erich Reinhardt, PhD, former CEO of <strong>Siemens</strong> <strong>Healthcare</strong>,Executive Advisor CEO, <strong>Siemens</strong> AG, Erlangen, Germany22 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
<strong>Healthcare</strong> in 2050What do you believe will be the biggestfactor driving healthcare by 2050?GANTEN: In the future, chronic diseaseswill probably dominate healthcare. Withgood medical care, acute diseases can bemanaged and patients do not usually die.Chronic diseases are the bigger challenge,because they require long-term medicalcare, which is expensive. Again, personalresponsibility has to come into play,because a healthcare system cannot beexpected to continue to treat a personfor up to 40 years for diseases of civilizationsuch as cardiovascular disease,type 2 diabetes, asthma, or chronic liverdisease.Do you think that people born in2010 have a better chance of avoidingdiseases of civilization?GANTEN: Yes, because they will receivebetter health education.REINHARDT: I believe the sum of theproblems remains constant, althoughthe diseases may differ.How will patient data be managed inthe year 2050?GANTEN: All important individual patientdata, including the complete genome,proteome, and metabolome, will beentered into a computer and attachedphysically to each patient. The data willfollow patients when they visit a physicianor a hospital and in that way, becontinuously available for use in makingdiagnoses and prescribing treatment.Thus, management of disease will beimproved.REINHARDT: By 2050, physicians will haveaccess not only to all their own patients’data, but also to relevant informationabout similar cases that have been treatedworldwide. This will be used to reach themost professional, competent decisionsfor their patients. It will make life easierfor physicians, because it will enable themto be more productive, more efficient,and more effective, and it will allow themto spend more time with patients.GANTEN: In addition, all the data will beavailable for research, allowing us tostudy the real outcomes of specifiedtreatments. At present, treatment recommendationsare based on clinical trials,which involve a select group of patientsand relatively short observation periods.When we can get data from daily life, wewill know what is going on in practiceand have better estimates of how effectivewe are.How will these data be organized?REINHARDT: I do not think that one companywill own all the data. Althoughthere will be open access for research,I would rather imagine business modelsfor distribution and application of thedata.GANTEN: We need an organization tomake the database compatible betweeninsurance systems, academic healthcenters, clinical companies, and researchorganizations. Of course, in dealing withpatients and diseases, data protectionand ethics of handling data are extremelyimportant.REINHARDT: We will have to ensure thatprivacy is protected. I believe that by2050, technical solutions will be availablefor integration and compatibility indealing with huge amounts of datawhile applying high ethical standards.Are you optimistic or pessimisticabout the state of healthcare in2050?GANTEN: One of the greatest philosophersof modern times, Karl Popper, said thatthe future is uncertain. He also said thatthe more discoveries are made, the moreuncertain the future is. I think it is importantto keep this in mind when discussingthe future of health, medicine, andtechnology. Many people say that it ispessimistic to believe that the future isuncertain, but the optimistic view is thatwe have a responsibility for the future,and if you have a personal idea of howthe future should be, then you have aresponsibility to work for it. Health is ahuman right, and it is our responsibilityto work for this human right. We mustdo everything we can to improve healthnot only in wealthy populations that canafford everything available for their ownpersonal health, but also for people whoare underprivileged and do not have thesame access to healthcare.REINHARDT: I agree that the future isuncertain, but I think there are opportunitiesto create the future by developingscenarios for possible alternatives inorder to be prepared. A prerequisite is torespond quickly to changes so that theycan be integrated into healthcare. I amconvinced that we will see significantimprovement in knowledge about health.Personally, I am an optimist, so I thinkthat there are very positive opportunitiesahead.Linda Brookes is a freelance medical writer andeditor who divides her time between Londonand New York, working for a variety of clients inthe healthcare and pharmaceutical fields.SummaryChallenge:• To integrate advances in medicaltechnology for prevention and earlydiagnosis of disease while streamliningpatient services and optimizingcosts and reimbursement structuresSolution:• Understand the patient’s disease(imaging, laboratory diagnostics)• Understand the patient’s biology(molecular applications)• Streamline acquisition, storage, translation,and distribution of all medical data• Optimize all patients’ enrollmentin primary and secondary preventionprograms• Assess similar cases from state-of-theartdatabasesResult:• Wider application of personalizedmedicine• Optimal knowledge of patients’ healthstates for both patients and healthcareproviders• Minimization of preventable prematuremorbidity and mortality• Greater cost effectiveness withinhealthcare systemsMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 23
Breast CareMAMMOMATImage transfer to syngo ImagingHIS Terminalsyngo Imaging (PACS)RIS with Mammo modulefor result reportingPatient Admission –Dismissal – Triageinformation(ADT)PrefetchPriorsRIS sendsSigned Offstatus tosyngoImagingFilm Digitizerfor prior filmsArchivingDICOMModalityWorklistImage Transferto CAD (raw data)CADReport with BIRADSprompts auto patientletter stream to print.Patient study launchesvia RIS Bridgesyngo Workflow (RIS)Prior digitized imagesto syngo MammoReportLong-Term Archivesyngo MammoReportCurrent images withCAD and prior studiesPACS/syngo MammoReportSend saved new seriesor query prior imagesEfficient data flow in DCHS’mammography department24 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Breast CareRural System TakesMammography to a New LevelWhile boasting ultra-dedicated physicians and staff, ruralhealthcare facilities traditionally have taken a backseatto their big city cousins when it comes to state-of-the-artmammography technology and workflow. Then there’sDickinson County <strong>Healthcare</strong> System.By Diana SmithDickinson County <strong>Healthcare</strong> System(DCHS) is located in Iron Mountain, Michigan,USA, in the state’s Upper Peninsula– a vast region bordered by Canada, Wisconsin,and two Great Lakes. The systemserves a rural area comprised primarilyof the south-central Upper Peninsula andadjoining counties in neighboring northeasternWisconsin. All told, approximately35,000 people live in the area, hardysouls who can endure 100 to 250 inches(250 to 635 centimeters) of snow eachyear. The closest city to Iron Mountain istwo hours away.The area was once known for its prolificcopper and iron ore mining operations.Now, thanks to imaging and workflowtechnology from <strong>Siemens</strong>, DCHS is promotingits new “gold“ standard: superior,patient-focused, full-field digital mammography.With new technology andimproved workflow, patients receivebreast care as advanced as that found inany urban setting.A State-of-the-art VisionThe rural surroundings did not dissuadeleaders at the 100-bed hospital, whoenvisioned nothing less than state-ofthe-artmammography services at DCHS.“Two years ago, we decided to transformour mammography services and tobecome one of the best-in-class mammographyservice providers, statewideand nationwide,” says William (Bill)Johnson, ARRT (American RegisteredRadiology Technician), RDMS (RegisteredDiagnostic Medical Sonographer), CRA(certified Clinical Research Associate),Radiology/Imaging Services Manager atDCHS. “We believed that a combinationof workflow rethinking and the use ofthe latest technology in image acquisition,viewing, reporting, and storage werethe necessary tools to implement a newmammography paradigm,” Johnsonexplains. “The importance of workflowefficiency is especially evident today withthe demands of public awareness and anaging population, which has increasedthe demand for mammography.”The answer for DCHS was to acquire afull-field digital mammography (FFDM)system to replace analog film-basedmammography, says Radiologist EmmaDiPonio, MD. At the same time, the teamcombined the transition to digital mammographywith the reengineering of themammography workflow with thefollowing goals:• Improving the quality of patient care• Increasing patient comfort• Improving efficiency• Extending outreach• Lowering total operating costGoing DigitalTo meet these lofty goals, the teamturned to <strong>Siemens</strong> for the latest technologysolutions. “We decided to select aRIS-[radiology information system-]drivenmammography workflow with imagesstored in syngo® Imaging, our existingPACS [picture archiving and communicationsystem],” says RIS/PACS AdministratorSharleen (Sherry) Koepp, ARRT, RDMS,CIIP (Certified Imaging Informatic Professional),a 30-year veteran of the imagingfield. “We purchased the mammographymodule as an adjunct to our RIS, syngoWorkflow, in order to electronically storeand access patient mammography historyand to provide access to prior reports.<strong>Siemens</strong>’ syngo MammoReport work-Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine 25
Breast Care“We looked at digital imaging for mammographyand thought it was just superior and would be muchmore cost-effective in the long run.”Sharleen Koepp, ARRT, RDMS, CIIP, RIS/PACS Administrator,Dickinson County <strong>Healthcare</strong> System, Iron Mountain, Michigan, USAstation was selected as our solution forreading mammography exams.”For imaging, the MAMMOMAT®Novation DR full-field digital mammographyacquisition system was installed.The all-in-one mammography solutionallows for screening, diagnostics, magnification,spot imaging, needle localization,and galactography. It is equippedwith a pivoting bucky to enable 100 percentsystem utilization. “This way, if apatient is in a wheelchair or semi-recumbent,we can get the image at any angle,”Koepp explains. Combined with syngoOpdima®, vacuum and core needle biopsyand specimen radiography can be performed.“We looked at digital imaging for mammographyand thought it was just superiorand would be much more cost-effectivein the long run,” says Koepp. “Certainly,it is a big expense to begin with, but filmcosts and processing costs with filmbasedmammography become offset bythe digital world, and you eventuallyrecoup those costs. It is also importantto be able to share those images withothers. Especially if you are in a remotearea, as patients do go to other facilities,for example, for reconstructive surgery.Thanks to our digital capabilities, we areable to provide images to those facilities.“Upon acceptance, the images are autoroutedto the PACS, syngo Workflow, thesyngo MammoReport workstation, andthe computer-aided detection (CAD)system. syngo MammoReport, the highspeedworkplace for reading and reportreports.The patient is taken into the examroom to change while mammographyhistory data is drawn up on the RIS.After the exam is explained to the patient,the patient is positioned and images aretaken. They are available as soon as theexam has been completed. The newlyacquired images are viewed by the technologistfor quality assurance (QA) purposes,such as checking for the correctpatient positioning. This is done on athree-megapixel monitor, while imagesof prior examinations are viewed on anadjacent 1.5-megapixel monitor. “Thosewere innovations we insisted upon,” saysKoepp. “Normally, an image would beviewed for QA by a tech on a 1.5-megapixeldisplay device. The radiologist readsthe image, however, on a five-megapixeldisplay. By having a three-megapixel dis-play for QA, the technologist can viewan image that looks much closer to whatthe physician will see. By also having a1.5-megapixel display, the technologistcan compare images of a prior exam andnew images side by side to view similaritiesand inconsistencies. That is huge.With film, we would put prior and newfilms side by side on a light box. Wewanted to be able to do the same withelectronic images.”Improved Efficiency andWorkflowInnovation in the Exam Roomand BeyondThe new system resulted in a brand-newworkflow paradigm that has increasedcomfort and peace of mind for patients,while improving images and workflowfor physicians and staff. “When a patientarrives in the imaging department, shechecks in with central scheduling, andthe display screen in the mammographyroom informs the technician that thepatient is in the waiting room,” KoeppRadiologist Dr. Emma DiPonio reviews studies on DCHS’ customized syngo MammoReportworkplace. The syngo Workflow (RIS) monitor is mounted on the left. When a patient isselected on the RIS worklist, new and prior studies are retrieved from the PACS and appear onthe syngo MammoReport’s diagnostic display.26 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Breast Careing FFDM mammograms, comes equippedwith a keypad designed for the specificrequirements of the digital mammographyworkflow. For example, by pushingthe center button on the keypad, thesystem switches immediately betweenscreening and diagnostic mammograms.The CAD software identifies regions ofinterest on the mammography imagesand brings them to the attention of theradiologist. This helps decrease falsenegativereadings and more effectivelyidentify masses, architectural distortions,and microcalcifications in a diverse screeningpopulation.“Diagnostic exams are reviewed with theradiologist and, if needed, extra viewsare taken. If the patient is willing to wait,we’ll work them in as soon as possible,usually within a few hours or less,” saysKoepp. “If indicated, an ultrasound orneedle biopsy can be done on the sameday with notification to the referringphysician.” If breast magnetic resonanceimaging (MRI) is recommended, it isscheduled as soon as possible afterinsurance pre-authorization is obtainedand the physician is notified.DCHS uses a markable breast diagramto identify clinical findings, and syngoWorkflow automatically generates theassociated result report for review, editing,and signature, according to Koepp.Based on the finding, the system canassign a follow-up letter stream for thepatient, factoring in any specific conditionsdesired. For example, a patientbelow the age of 40 with a negativescreening can be sent a reminder letterin two years, but a 52-year-old patientmight receive an annual reminder.“We use the stored data in syngo Workflowfor statistical reports for accreditationneeds, including positive predictivevalue [PPV], false positive/negative predictivevalue, as well as technologist andradiologist productivity, as required forthe American College of Radiology [ACR]and the Mammography Quality StandardsAct [MQSA],” says Koepp. Prior to the RISimplementation, this information waskept in a binder and had to be compiledmanually. Now, reports are generatedautomatically, resulting in tremendoussavings in time and effort.With 6,000 mammography exams performedeach year at DCHS, the newworkflow helps provide fast and reliableservice for patients and facilitates theworkload of the mammography team.Patients experience virtually no waitingtimes when examinations are scheduledin advance, and the total examinationtime does not exceed 15 minutes.Patient-centered ProcessPatient comfort is enhanced by the useof a “mammo pad,” a foam pad that isattached to the equipment allowing compressionto be more tolerable for mostpatients. Additionally, the health systemhas added a considerate touch, a comfortableroom that is available for confidentialdiscussion with the radiologistwhen needed. While patients may notrealize the improved, stellar quality oftheir images, they do appreciate theremodeling of the mammography andwaiting rooms, which provide improvedcomfort, privacy, and relaxation.In 2008, DCHS set out to provide superiormammography services to the residentsof Northern Michigan and nearby Wisconsin.Staff members believe they haveachieved this through the combinationof syngo MammoReport, syngo Workflow,syngo Imaging, and the MAMMOMATsystem. Together, these solutions metDCHS’s quality and workflow requirements– from patient registration and imageacquisition to reading and reportingthrough final data storage.“As we have progressed with the conversionto a filmless, all-digital environment,[<strong>Siemens</strong>] technology has been the bestfit for Dickinson and is very reliable,”says Johnson. “<strong>Siemens</strong> products providethe connectivity and high imagingquality that meets the expectations ofour patients and their physicians.” Evenoutside the big cities.Diana Smith is a freelance writer specializingin medical topics. She is based in Liberty Hill,Texas, USA.Further Informationwww.siemens.com/breastcareSummaryChallenge:• Improve quality of breast cancerscreening, diagnosis, and treatmentin a rural area to become one of thebest-in-class mammography providersnationwide• Increase patient comfort and physiciansatisfaction• Accelerate workflow and increaseefficiency• Decrease total operating costSolution:• A state-of-the-art, full-field digitalmammography system from <strong>Siemens</strong>offering advanced screening,diagnostic, and treatment solutions• Innovations in mammography forincreased patient comfort• Reengineered, improved workflowincreasing efficiency and access toinformation• New systems that allow excellentimage quality and immediate accessto completed exams• Improved information system thatallows for the use of stored data tocreate statistical reports for accreditationneedsResult:• Advanced breast care screeningand diagnosis, close to home,rendering travel to a large urbancenter unnecessary• Increased patient comfort and satisfaction,with virtually no waitingtimes when scheduled in advance, andexams that do not exceed 15 minutes• Excellent image quality, increasingdiagnostic confidence and guidingtreatment and follow-up, available assoon as an exam has been completed• Seamless integration of multimodalitydata• Streamlined processes• Lower operational costs, increasedreimbursement over film screensMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 27
ImmunoassayA New Aid forIdentifying SepsisThe measurement of BRAHMS procalcitonin, a diagnostic biomarker,aids clinicians in identifying patients with sepsis and has also beenshown to reduce unnecessary antibiotic use. The positive outcomesexperienced at hospitals such as the Swedish Covenant Hospital inChicago, Illinois, USA, are confirmed by several clinical trials, includinga recent large, multicenter study conducted in Switzerland.By Sameh Fahmy, MSA patient in the intensive care unit (ICU)has a fever, a rapid heart rate, an elevatedrespiratory rate, or an abnormal whiteblood cell count. These symptoms couldherald the onset of sepsis, a life-threateningsystemic inflammatory responseto infection, or they could be the resultof trauma or a host of other conditions.Results from blood cultures have a highrate of false negatives – 40 percent in onestudy 1 – and will not be available for upto 72 hours. The clock is ticking, andevery hour of delayed treatment increasesthe likelihood of death. 2 Inappropriateantibiotic use can cause adverse sideeffects for the patient and encouragethe development of drug-resistant bacteria.Fortunately, there is a better option. Bymeasuring serum levels of the proteinprocalcitonin (PCT), clinicians can identifypatients at risk for sepsis early and begintreatment when it is most likely to beeffective. The BRAHMS PCT assay is avail-able on the <strong>Siemens</strong> ADVIA Centaur® XPand ADVIA Centaur CP ImmunoassaySystems*. This PCT assay also allowsclinicians to monitor response to treatmentand tailor antibiotic therapyaccordingly.“PCT gives you more confidence in yourdecision-making about when to startantibiotics, when antibiotics are not working,and when to stop antibiotics,” saysEric Gluck, MD, Director of Critical CareServices at Chicago’s Swedish CovenantHospital and Professor of Medicine atFinch University of Health Sciences/TheChicago Medical School. “Nothing elsecorrelates with those three endpoints aswell as PCT does.”Swedish Covenant, a 323-bed academichospital, has been using the BRAHMSPCT assay on Kryptor® since 2007 andhas seen significant decreases in antibioticusage in the ICU and a decreasedaverage length of stay in patients withsepsis. Performance evaluation trials of* CE Mark. Not available for sale in the U.S.Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine 29
ImmunoassayBRAHMS PCT on ADVIA Centaur XP wereconducted at Swedish Covenant usingperformance evaluation-only reagents,calibrators, and controls. Several studies3–8 within the past decade have shownthe benefits of BRAHMS PCT guidance inreducing unnecessary antibiotic usageas well as associated adverse side effects,including a large multicenter clinical trialrecently published in the Journal of theAmerican Medical Association (JAMA). 9“Patients in the BRAHMS PCT grouphad a 30-percent reduction in therate of antibiotic-related side effects.”Philipp Schuetz, MD, Department of Emergency Medicine,Beth Israel Deaconess Medical Center, Boston, Massachusetts, USAA Growing ThreatAn estimated 215,000 annual deathsare attributed to sepsis in the UnitedStates alone, making it more deadly thancommon cancers such as lung cancer,colon cancer, and breast cancer. Worldwide,18 million cases occur annually,with an average cost per patient ofUS$22,100. 10 An aging population andthe increasing use of invasive proceduresare making sepsis even more common,with the rate of sepsis increasing by anestimated 1.5 percent every year. 10A rapid and accurate diagnostic tool iscritical, because the prognosis for patientswith sepsis is best when the condition isrecognized and treated early. 11 If a patientprogresses to severe sepsis, defined assepsis and organ dysfunction, mortalitycan jump to 52 percent. If a patient entersseptic shock, the mortality rate can jumpto 82 percent. 12 “The data has demonstratedvery clearly that the sooner youstart antibiotics, the better the outcomeswill be,” says Gluck.Rapid, Accurate DiagnosisPCT is a protein that is normally producedin small amounts in the thyroid gland.In patients with sepsis, however, the proteinis produced in large quantities bythe liver, kidney, fat cells, and muscle.Increasing serum PCT concentrationsindicate increased severity of infectionand a worse prognosis for the patient.Using the ADVIA Centaur XP and ADVIACentaur CP Systems*, clinicians canreceive results in less than 30 minutes.Swedish Covenant began using theBRAHMS PCT assay on Kryptor in 2007after conducting clinical trials to assess* CE Mark. Not available for sale in the U.S.its sensitivity and specificity. “We foundthat the assay had a sensitivity of 91percent in the identification of patientswho were septic and a specificity of 98percent to identify patients who do nothave sepsis,” Gluck said. “And that wasbetter than anything else that we hadavailable to us at the bedside in our hospital– none of the blood tests or physicalfindings got us anywhere near thosekind of results.”Gluck says that in many cases, patientswould have received a much later diagnosisof sepsis and would have likely hada worse outcome had it not been for thePCT assay. One patient, for example, wasbrought to the emergency departmentby family members after intentionallyoverdosing on prescription medications.An elevated white blood cell count wasthought to be the result of stress of theoverdose. However, the treating physicianran a PCT assay to corroborate the finding,now a routine practice at SwedishCovenant. An elevated PCT level stronglysuggested infection, so the patient wasgiven antibiotics. When results from bloodcultures became available the next dayand were followed by an ultrasound, itbecame clear that the patient had cholecystitis,or inflammation of the gallbladder,accompanied by infection. “In thisparticular patient, I’m not sure if we wouldhave ever made the diagnosis,” Glucksays, “because the patient couldn’t giveus a history.”Measurable Reductions inAntibiotic UseA large-scale, multicenter trial recentlypublished in JAMA, led by Philipp Schuetz,MD, University Hospital in Basel, Switzerland,showed that the use of BRAHMS PCTcan help rule out bacterial infection,especially in patients with chronic obstructivepulmonary disease (COPD) andbronchitis, and reduce the duration ofantibiotic use in patients with diagnosedinfection. Schuetz says that while previousstudies were consistent with thesefindings, they were not large enough toassess whether patients treated withPCT-based guidelines had comparablerates of disease-related complications.To answer that question, Schuetz and ateam of researchers compared treatmentbased on PCT guidance against standardcare in a randomized controlled trialinvolving more than 1,300 patients withlower respiratory tract infections at sixtertiary care hospitals in Switzerland.According to the study’s guidelines, antibioticswere strongly discouraged if PCTwas less than 0.1 μg/L, discouraged iflevels were 0.25 μg/L or lower, encouragedif PCT was higher than 0.25 μg/Land strongly encouraged if levels wereabove 0.5 μg/L. Overruling of the guidelineswas possible by prespecified criteria,such as immediate need for ICU admissionor respiratory or hemodynamicinstability. In patients given antibiotics,PCT measurements were repeated afterthree, five, and seven days of treatment.The guidelines recommended stoppingantibiotics if PCT levels decreased by80 percent.“We found that in patients treated withknowledge of procalcitonin levels andIn a study recently published in JAMA,Philipp Schuetz, MD, showed that themeasurement of the biomarker BRAHMS PCTcan help rule out bacterial infection and reducethe duration of antibiotic use in patients withdiagnosed infection.30 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
The BRAHMS PCT test is available on the <strong>Siemens</strong> ADVIA Centaur XP andADVIA Centaur CP Immunoassay Systems*.SummaryChallenge:• Identifying patients with sepsis early, when treatment is most likelyto be effective• Reducing the high cost associated with treating patients with severesepsis and septic shock• Differentiating sepsis from other inflammatory diseases, trauma,and other conditions, whose symptoms can mimic sepsis• Reducing unnecessary antibiotic usage and its associated costs andside effectsSolution:• Measurement of serum levels of the biomarker BRAHMS procalcitonin,allowing physicians to rapidly identify patients with sepsis• Early identification of sepsis using procalcitonin, allowing for treatmentto be initiated sooner, potentially reducing costly complicationsassociated with sepsis• Measuring procalcitonin levels, helping rule out bacterial infection inpatients whose symptoms mimic those of sepsis• Negative BRAHMS PCT result indicates that antibiotics may not benecessary; in patients with bacterial infection, serial measurementof PCT helps guide treatment, helping ensure that patients receiveoptimum duration of antibioticsResult:• Patients receive appropriate treatment quickly, improving likelihoodof survival 2• Early and appropriate treatment for sepsis may result in reducedco-morbidities, with potential cost savings associated with shorterlengths of stay 7• Antibiotics given only to patients who need them, and for optimumduration, resulting 5, 6, 7, 9 in reduction of adverse side effects and minimizationof potential for the development of drug resistant bacteria 9• Inappropriate antibiotic usage dramatically reduced 5, 6, 7, 9 , resultingin potential cost savings, fewer adverse side effects 9 , and potentiallyshorter lengths of ICU stay 7those treated without knowledge ofprocalcitonin levels, the risk for adverseevents was the same,” says Schuetz, whois currently engaged in research at theDepartment of Emergency Medicine atBeth Israel Deaconess Medical Centerin Boston, Massachusetts, USA. “Patientshad the same mortality, they had thesame ICU admissions rate, and – importantly– they had the same rate of recurrentinfections.”Notably, the researchers also found thatpatients in the procalcitonin group hadan average antibiotic exposure nearly35 percent less than the control group.Schuetz points out that the pattern ofreduction varied depending on diagnosis.The study found that patients with pneumoniawere treated with fewer days ofantibiotics than the control group, whilepatients with exacerbations of chronicobstructive pulmonary disease (COPD)and bronchitis were less likely to haveantibiotics initiated than the controlgroup.The reduction in antibiotic use also translatedto better patient care. Schuetzpoints out that patients in the PCT grouphad a 30-percent reduction in the rateof antibiotic-related side effects such asnausea, diarrhea, and rash.Integrating PCT into ClinicalRoutinesBRAHMS PCT guidance has also beenshown to be useful in reducing antibioticuse in primary care settings, and preliminarydata from Gluck and his colleaguessuggest that measuring PCT when apatient presents to the emergency departmentcan reduce unnecessary bloodcultures.Administering the assay is inexpensive,Gluck notes, especially when comparedto the high cost of treating a septicpatient and the potential cost savingsfrom reductions in antibiotic use andshorter lengths of stays.Although the data regarding the valueof PCT guidance are convincing, bothSchuetz and Gluck acknowledge thatphysicians are initially hesitant to alterwell-established treatment practices.* CE Mark. Not available for sale in the U.S.32 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Immunoassay“By treatingpatients with antibioticswhen theydon’t need them,you’re exposingthem to some possibilityof harm.”Eric Gluck, MD, Director of Critical CareServices, Swedish Covenant Hospital, Chicago,Illinois, USASepsis by the Numbers“In the beginning, you have to reassurephysicians that the algorithm is safe,”Schuetz says, “but once physicians startusing it, they realize that what they havebeen doing for all of these years – overtreatingpatients with antibiotics – wasnot necessary.”Gluck introduced his colleagues at thehospital to the BRAHMS Kryptor PCTassay in a large, general instruction sessionthat covered the benefits of theassay and emphasized that it does notreplace medical judgment or other diagnostictests. The assay, he explained, isa tool to help physicians make moreinformed decisions. An initial utilizationin the ICU was later expanded to infectiousdisease physicians, the emergencydepartment, and eventually to the entirehospital. Gluck says that Swedish Covenanthas so much confidence in theassay that it has implemented a hospitalwidepolicy indicating that physiciansshould discontinue antibiotics if PCTlevels are negative in two measurements24 hours apart.“One of the most important dictums inmedical ethics is ‘do no harm’,“ Glucknotes. “And by treating patients with antibioticswhen they don’t need them,you’re exposing them to some possibilityof harm. So, it makes my consciencemuch clearer to know that when I leavethe hospital, I have significantly reducedthe number of patients who receiveunnecessary antibiotics. And it also makesme feel comfortable that in the likelihoodthat the patient needs antibiotics,I will know about it as fast or faster thananybody else practicing critical caremedicine.”Sameh Fahmy, MS, is an award-winning freelancemedical and technology journalist basedin Athens, Georgia, USA.Sepsis is not a specific disease, but rather a continuum of events triggeredby the body’s inflammatory immune response to bacterial, fungal, parasitic,or viral infections. The statistics below demonstrate the high toll it exacts.• Approximately 18 million sepsis cases estimated yearly worldwide 1• Sepsis affects more than 35 percent of ICU patients 1 and manifests inapproximately 2/3 of these patients as severe sepsis or septic shock 13• Approximately 28.6 percent average overall mortality for sepsis, severesepsis, and septic shock 12• Up to 82 percent mortality for patients with septic shock 12• Once a patient is in septic shock, survival rates can drop 7.6 percent forevery hour that antibiotic therapy is delayed 2• U.S. estimated cost exceeds US$17 billion annually, with average cost perpatient of US$22,100 10• Incidence of sepsis is increasing by approximately 1.5 percent per year andis expected to continue growing as the population ages 101Vincent J.L., et al. Sepsis in European intensivecare units: results of the SOAP study. Crit CareMed. 2006 Feb; 34(2):344-53.2Kumar A. et al. Duration of hypotension prior toinitiation of effective antimicrobial therapy is thecritical determinant of survival in human septicshock. Crit Care Med. 2006; 34(6):1593.3Briel M., Schuetz P., Mueller B., et al. Procalcitoninguidedantibiotic use vs a standard approach foracute respiratory tract infections in primary care.Arch Intern Med. 2008; 168(18):2000-2007.4Briel M., Christ-Crain M., Young J., et al. Procalcitonin-guidedantibiotic use versus a standardapproach for acute respiratory tract infections inprimary care. BMC Fam Pract. 2005; 6:34.5Christ-Crain M., Jaccard-Stolz D., Bingisser R.,et al. Effect of procalcitonin-guided treatment onantibiotic use and outcome in lower respiratorytract infections. Lancet. 2004; 363(9409):600-607.6Christ-Crain M., Stolz D., Bingisser R., et al.Procalcitonin guidance of antibiotic therapy incommunity acquired pneumonia: a randomizedtrial. Am J Respir Crit Care Med. 2006; 174(1):84-93.7Nobre V., Harbarth S., Graf J.D., et al. Use ofprocalcitonin to shorten antibiotic treatmentduration in septic patients. Am J Respir Crit CareMed. 2008; 177(5):498-505.8Stolz D., Christ-Crain M., Bingisser R., et al.Antibiotic treatment of exacerbations of COPD.Chest. 2007; 131(1):9-19.9Schuetz, P., et. al. Effect of procalcitonin-basedguidelines vs. standard guidelines on antibioticuse in lower respiratory tract infections. JAMA.2009; 302(10):1059-1066.10Angus D.C., Linde-Zwirble W.T., Lidicker J.,Clermont G., Carcillo J., Pinsky M.R. Epidemiologyof severe sepsis in the United States: Analysisof incidence, outcome, and associated costs ofcare. Crit Care Med. 2001; 29(7):1303-1310.11Rivers E., et al. Early goal-directed therapy inthe treatment of severe sepsis and septic shock.NEJM. 2001; 345(19):1368-77.12Salvo I., et al. The Italian sepsis study: preliminaryresults on the incidence and evolutionof SIRS, sepsis, severe sepsis, and septic shock.Intensive Care Med. 1995; 21 Suppl 2:S244-9.13Kumar A. et al. Duration of hypotension priorto initiation of effective antimicrobial therapyis the critical determinant of survival in humanseptic shock. Crit Care Med. 2006; 34(6):195314Brun-Buisson C. The epidemiology of the systemicinflammatory response. Int Care Med. 2000;26:s64-74.15Vincent J.L., et al. Sepsis in European intensivecare units: results of the SOAP study. Crit CareMed. 2006 Feb; 34(2):344-53.16Alberti C., et al. Epidemiology of sepsis andinfection in ICU patients from an internationalmulticentre cohort study. Int Care Med. 2002;28:108-21.Further Informationwww.siemens.com/sepsisMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 33
Hybrid Rooms RevolutionizeTrauma Treatment in SwedenKarolinska University Hospital in Stockholm has built one of the world’s firsthybrid rooms dedicated to treating trauma patients. This was made possibleby implementing Artis zeego, the multi-axis C-arm system based on robotictechnology from <strong>Siemens</strong>. The system met all the criteria set up by thehospital: advanced imaging technology, an extremely clean working environment,and a design allowing the staff to move freely.By Nils Lindstrand34 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
The hybrid room at Karolinska’s trauma center simplifies the physicians’ choice betweeninterventional technology and surgical procedures and enables them to combine both.“This is a hybrid room without compromise,”says Linus Blohmé, Deputy Headof Vascular Surgery at Karolinska UniversityHospital in Stockholm. The solutionbased on Artis zeego® has made it possibleto use advanced imaging technologyand still create a room where the staffcan move around freely.Artis zeego is an extremely flexible floormountedsystem that does not containany ceiling-mounted components. Thesystem is, therefore, ideally suited forhybrid rooms, because equipment in theceiling may contaminate the laminar airflowof the extremely clean environmenton which the hospital prides itself. Informationtechnology installed in the hybridroom provides the needed information tothe staff taking part in the procedure.The hybrid room at Karolinska UniversityHospital is used to treat trauma cases forthe entire Stockholm region. This meansvery high demands, and the room hasbeen designed to meet extremely highstandards. “We’ve raised the bar forhybrid rooms,” says Pär Olofsson, retiringHead of Vascular Surgery. The projectteam got the go-ahead from the hospitalin 2006 to build this optimal hybrid roomfor trauma treatment. The efficiency thisroom promised convinced the hospitalboard that this would be a sound investment.Construction work on the hybridroom at Karolinska University Hospitalstarted in the fall of 2008. In the summerof 2009, the room was first used to treatpatients.The former trauma center at Karolinskawas designed according to usual standards:a helicopter pad, a triage roomwith a computed tomography (CT) scanunit, and an operating room (OR). Thedistance to the operating suite was 20meters (nearly 66 feet), which is quitegood. However, the distance to the interventionalsuite was about 600 meters(nearly 2,000 feet).“This distance could still be okay,” saysOlofsson. “The problem is that, with thisdistance, you want to be very sure that’swhere you need to go. You don’t want topush a severely traumatized patient thatdistance and then back again, whichmight be necessary if you don’t have theimaging equipment to make a definitedecision between interventional treatmentand a surgical one. In practice, thismeant that we sometimes probably chosesurgery to save a life. With a hybrid room,we can use minimally invasive proceduresin many cases.”A few years back, the decision to makeKarolinska University Hospital a regionalcenter for the treatment of traumapatients gave further reasons for buildinga hybrid room. “Before we startedMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 35
SurgeryContinuing to Improve HybridInterventional Methodologies inOsloThe hybrid room at Rikshospitalet in Oslo, Norway, one of the first Artiszeego installations in a hybrid environment, was installed in 2007 and has acontinuing focus on developing methods for treating patients within a widerange of needs. Moreover, the hybrid room is used to test cutting-edge interventionaldevices such as stents or valves for endo-vascular use. “Testingmethods and devices is made more efficient using the advanced imagingpossibilities provided by Artis zeego,” says Per Kristian Hol, MD, Manager ofRadiology Research at the Interventional Center. “We get fuller and moredetailed information by using this technology.”The Interventional Center at Rikshospitalet is an innovative imaging departmentand a reference facility for a number of hybrid rooms built in recentyears, including the Karolinska University Hospital. “Yes, we’ve experienceda lot of interest from other hospitals,” says Hol. “We’ve had guests from allover the world, mainly from Scandinavia, Europe, and the U.S., but also fromChina and Japan.”Hol is still very pleased with the features of Artis zeego and the enhancedsupport that advanced imaging brings to the critical-decision process. “Today,we’re using this equipment and the hybrid room to develop a large numberof procedures. Cardiology and vascular treatments are still in focus, but weget a lot of interest from other fields such as audiology, where imaging technologyis very useful for developing methods for Cochlea implants in theinner ear, for example.”The hybrid room at Rikshospitalet is still being developed in many ways.One is the “stage light” OR lighting concept in which the center is developinga system to provide perfect lighting at any moment of any treatment.“The next challenge will be to develop methods within neurology and neurosurgery,”says Hol.The hybrid room in Oslo continues to meet new challenges through innovative methodand device testing.this project, hybrid rooms were far awayfrom emergency cases,” says Blohmé.“They were used for treatment andresearch primarily in angiography andangioplasty, in well-planned cases. For us,the reason for using a hybrid room wasto simplify the choice between interventionaltechnology and surgical procedures,or to combine the two.”Focus on Trauma PatientsThe hybrid room at Karolinska is, therefore,primarily used for trauma patients.But to make the work in the hybrid roomefficient, the staff needs to use it as muchas possible. This is, of course, also importantin order to maintain economic efficiencyand to provide patients with thetreatment advantages the hybrid roomoffers.“The time between recovering from anintervention and from open surgery maybe weeks or even months,” says Olofsson.This means a great difference in thepatient’s well-being and also a major differencein economic terms, both for thehospital and for healthcare in general.To be able to choose the right treatment,without increasing any risk for thepatient, is a major step forward.The medical staff was so convinced ofthe economic efficiency provided bythe hybrid room that it wanted to makeit an economic unit of its own. “This wasnot possible, due to the establishedeconomic systems of the hospital,” saysOlofsson. “But we’ll monitor the fiscalresults as closely as we can to create agood follow-up on the efficiency of thehybrid room as we learn to use it to itsfull potential.”The decision to go with <strong>Siemens</strong> andArtis zeego was based on three criteria:the necessity of an extremely cleanatmosphere, the staff’s need to movearound without being hindered by theequipment, and the need for high-qualityimaging. “There was alternative technologyavailable that met one of thesedemands,” says Blohmé. “<strong>Siemens</strong>’ Artiszeego solution was, however, the onlyone that met all of them. Mobile unitswould have solved the space issue, butthe imaging quality was too low. We alsolooked at solutions with equipment in36 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Linus Blohmé, Deputy Head of Vascular Surgery (left) and Pär Olofsson, retiring Head of VascularSurgery (right) appreciate the advantages of a hybrid room for trauma treatment.Summarythe ceiling and on the floor, but they allblocked either the floor space or theclean laminar airflow we wanted to use.”Artis zeego made it possible to createa hybrid room with no compromise –advanced imaging with the C-arm thoroughlyparked out of the way when notin use and nothing blocking the air supplyfrom the ceiling.Using a hybrid room for trauma treatmenthas advantages that may very well savemany lives. People with trauma injuriesoften have major damages to blood vessels.Getting the optimal treatment forinjuries like this is vital, and time is oftenof absolute critical importance.“Bleeding is not good,” says Blohmé,using an obvious truism. “When a patientis bleeding internally, we need to get agood image and find a way to the optimaltreatment as fast as possible. The expression‘the golden hour’ holds a reality, andthe hybrid room means we have a muchbetter chance to save lives and to minimizepatient suffering by using advancedimaging to get a picture of damages,allowing us to choose the right treatment.”Major Educational EffortResponsibility for treating trauma patientsfrom all over the Stockholm region,which consists of more than two millionpeople, obviously means a round-theclockwatch. But even specialist doctorsneed to sleep, and, at least some nights,preferably in their own homes. To beable to have specialist surgeons and interventionalspecialists present when theyare needed, Karolinska University Hospitalhas taken on a major educational taskto train more of the hospital staff andreduce the reliance on the few certainspecialists.“We are in the process of teaching 300of the hospital staff to work in the hybridroom,” says Blohmé. “Obviously, not allof these 300 will be able to do everythinga specialist can do. The aim is tomake all these people confident workingwithin the hybrid room, helping thepatient to breathe and to limit bleeding.This way, we can push the time limit forspecialists to arrive, and also give thesedoctors a better opportunity to get usefulinformation about the patient as theyapproach the hospital.”To further enhance the informationcoming from the hybrid room, all imagingdata are distributed to an adjacentcontrol room. This information can alsobe seen in an observation room close byand in a lecturing hall in the universityhospital.“Congratulations to Stockholm”Filippa Reinfeldt, Counselor for HealthCare in the Stockholm region, said at theinauguration on December 9, 2009, thatshe wanted to extend her congratulationsto the people of Stockholm for nowhaving better healthcare. “This hybridroom is truly technology and science inthe service of mankind,” said CounselorReinfeldt. “This is exactly how we wantthe healthcare system to work.”Nils Lindstrand is a freelance business andtechnology writer based in Stockholm, Sweden.Challenge:• Finding effective and minimallyinvasive treatments for traumapatients• Allowing for a large number ofpeople to work on trauma patientswithout being hindered• Keeping the air in the hybrid roomextremely clean• Taking care of trauma patients fromthe entire Stockholm regionSolution:• First-ever hybrid room solution fortrauma care with Artis zeego• Using the Artis zeego C-arm to keepthe room space open• No equipment in the ceiling,thanks to robotic technology usedfor the C-arm• Good communication and informationsystems allow for faster andmore accurate decisionsResult:• No surgical treatment needed if lessinvasive methods are sufficient• Extremely efficient workflow thanksto the hybrid room, making itpossible to treat patients correctlyand without wasting time• Hybrid room operations worksmoothly even in a crowded room• The air hygiene meets the highstandards required by the hospitalFurther Informationwww.siemens.com/surgeryMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 37
Sports injury as shown in MRI: image ofa bundle rupture of the rectus femorismuscle, displaying the contiguous,non-injured secondary muscle bundles.
MRI in OrthopedicsHans-Wilhelm Müller-Wohlfahrt, MD, is dedicated to further standards inthe diagnosis of muscle injuries, especially in the field of sports medicine.Leadership in Sports MedicineThe internationally renowned specialist in orthopedics and sportsmedicine, Hans-Wilhelm Müller-Wohlfahrt, MD, has establishedan innovative “micro-clinic“ for the diagnosis and treatment of orthopedicand sports-related injuries. With its highly experienced team,the Center is considered a model for the future of medical care.Medical Solutions visited the Center to learn more.By Matthias ManychNot far from one of Munich’s most famouslandmarks, the new city hall (Neues Rathaus)on Marienplatz square, the cobbledDienerstrasse takes visitors a few hundredmeters further to the Alter Hof (OldCourt) – Louis IV’s former imperial residence.The first floor of one of the buildingshouses the Center for Orthopedicsand Sports Medicine. Stepping throughits doors, the visitor leaves the bustle ofthe center of Munich behind. The lobbyis spacious and bright, welcoming visitors.The center’s aim to offer patientscomprehensive care at the highest possiblemedical and technical level is evidentas soon as you walk in. Moreover, themicro-clinic implements a unique concept,as Müller-Wohlfahrt explainstogether with his medical colleagues LutzHänsel, MD, and Peter Ueblacker, MD.Decades of medical experience and aholistic approach are combined with thelatest in imaging diagnostics as well asdata management and communicationstechnology. The center maintains fastlines of communication and decisionmaking,because everything from themagnetic resonance imaging (MRI) systemto physiotherapy is located underone roof.With 35 years of treating top athletesand more than 30,000 muscle injuries,Müller-Wohlfahrt has developed themanual diagnosis of sports-related muscleinjuries into a reliable method. As themedical consultant for the Germannational soccer team and the team doctorfor the soccer club FC Bayern München,he is frequently required to make soundmedical decisions within just a fewminutes. Müller-Wohlfahrt has also successfullyapplied his method to the treatmentof complex, long-term diseases anddisorders of the entire musculoskeletalsystem. His approach focuses on theperson as a whole and on examiningand treating each patient’s health issuesin a wider context, including additionalMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 39
MRI in OrthopedicsLutz Hänsel, MD, is a specialist fororthopedics, trauma surgery, and sportsmedicine.Franco Renzo is the President and CEO ofthe MW Group AG, which aims to propagate thecenter’s concept.Peter Ueblacker, MD, supports theacademical verification of the MW Center’smedical approaches.medical factors, rather than symptoms inisolation. In Müller-Wohlfahrt’s approachto treatment, the medications used arealmost exclusively biological or organic,purely plant-based, or homeopathic. Hisaim in opening the micro-clinic was totake his experience of sports medicineand the treatments he has developed andstandardize them on a scientific basis,making them reproducible for others.“I worked alone for far too long, and myintent was to pass along the methods Ihad developed to my younger colleaguesso that they are not lost,” Müller-Wohlfahrtemphasizes.A Model FacilityThose were the primary factors behindthe establishment of the new center.The idea first came up nearly five yearsago. Thanks to cooperation with theinvestor Dietmar Hopp, co-founder of thesoftware company SAP, and with FrancoRenzo, currently President and CEO ofMW (Müller-Wohlfahrt) Group AG, theCenter for Orthopedics and Sports Medicinewas able to open just a short whilelater, in 2008. This micro-clinic is part ofthe MW Group and serves as the nucleusfor further developments for the future:new care structures for the internationalhealth market. The MW Group aims toestablish additional micro-clinics worldwideto offer high-quality healthcareservices in various disciplines. In thiscontext, the Munich center serves as amodel. The group’s vision, says Renzo, is“not to wait until we see actual patients,but instead to treat people prophylacticallybefore they become ill.” The group’sgoals include ensuring that, in the future,anyone who needs to know is able to getinformation on his or her current healthstatus via telemedicine anywhere in theworld and can access additional informationsuch as specific medical tips.Cooperative Structures toBenefit PatientsThe MW Group AG can rely on a globalnetwork of experts for cooperations invarious fields, <strong>Siemens</strong> <strong>Healthcare</strong> amongthem. For Renzo, it was evident from thestart that “we need a global player – apartner with whom we can turn our ideasinto reality.” Thus, <strong>Siemens</strong> <strong>Healthcare</strong>was the partner for the micro-clinic’sradiology hardware and software fromthe very beginning. First, a 1.5-Tesla MRIsystem, a radiography system with adigital flat detector, a total of five ultrasoundunits, and a picture archiving andcommunication system were installed.A 3-Tesla MRI unit is scheduled to followsoon. The stated aim of the team ofphysicians is “to offer the best possiblesolution in the field of orthopedicsand sports medicine,” Hänsel explains.To have “one-stop” imaging is one ofthe major factors emphasizing thisapproach.A strong interaction with a large medicaland scientific network also ensures thatpatient care is state-of-the-art. Forinstance, the center has long maintainedclose contact with the Steadman HawkinsClinic, one of the leading centers fororthopedic treatment and sports medicinein the United States. And regardingmuscle injuries, the center’s cooperationwith Swedish Professor Jan Ekstrand,MD, is particularly important: he is thehead of a large injury study conductedby the European soccer federation UEFA.In the area of fundamental research,the clinic works together with the Departmentof Osteology and Biomechanicsat the University of Hamburg, whereUeblacker has a teaching assignment.The university unit studies the molecularbiological mechanisms behind the therapiesdeveloped by Müller-Wohlfahrt. Inaddition, the flow of information is reinforcedthrough participation in conferencesand presentations across Europe.Another goal of the MW Center is tofind the primary cause of orthopedic andsports medicine-related problems. Inpursuit of this aim, the team of physicians40 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
MRI in Orthopedicsand physical therapists spends far moretime on their patients than is customary.And although high patient throughputis not a goal in itself, efficient workingprocesses still play an important role.When treating top athletes, it is crucialfor medical providers to be able to pinpointand solve the problems quickly. Theadvantage that the clinic can now offerthrough its cooperation with <strong>Siemens</strong> isthat the results of manual diagnosis canbe supplemented with state-of-the-artimaging right away. The clinic’s staff hasgained experience through its work withtop athletes. The methods used for thoseathletes also benefit the non-athleteswho make up approximately 80 percentof the micro-clinic’s patients.Researching Orthopedics andSports MedicineMüller-Wohlfahrt is known for his noninvasivemethods of diagnosis and treatment.In particular, his ability to detectinjuries and ascertain their extent throughpalpation alone, and his ability to acceleratethe healing process with pinpointedinjections of medications have earnedhim the trust of international top athletesand others. His colleagues, Hänsel andUeblacker, have also perfected thesetechniques.Thirty percent of all sports injuries involvemuscle damage. Nonetheless, this topichas seldomly been addressed in a systematicway to date. Among the complicationsin this field, the system of classifyingmuscle injuries is still very imprecise –the only distinctions drawn are betweenslight, moderate, and severe injuries.Now, all this stands to change thanks tothe scientific work being done at the MWCenter in Munich. “The major factorbehind our classification system is theempirical findings by Müller-Wohlfahrt.These will now be given additional scientificsupport through biomolecularmethods, the injury study, and the consensusmeetings we are calling in orderto achieve international agreement,”explains Hänsel.In collaboration with numerous coauthors,the three doctors just recentlysummarized their entire diagnostic andtherapeutic knowledge about muscleinjuries in the comprehensive and uniquemonograph Muskelverletzungen imSport (Muscle Injuries in Sports) 1 . Thepublication also features a large chapterdescribing state-of-the-art muscle injurydiagnostics with MRI, including numerouscase studies.Focus on MRIAlthough MRI scanning will not replacemanual examinations of muscles, thisis a crucial part of the work performedat the MW Center. As Ueblacker explains,“We aim to set standards for imagingbased on our vast manual experience.”If technical options, such as sequencing,slice angling, and, where applicable,surface coils are selected optimally athigh-field strength, MRI scans can providegood images of muscle injuries. Ifthis is not the case, these injuries areoften overexposed, leading to incorrectassessments of their severity. It is alsonot unusual for a facility to lack the necessaryexperience in the interpretationof such MRI scans. And that, says Müller-Wohlfahrt, is why “we have taken on theobligation of giving clear, unambiguousrecommendations with our standards.”To that end, clinical and sonographic findingsare correlated with those obtainedthrough MRI. To be able to grasp the fullcomplexity of the musculature and theinjuries, a large number of correlativesmust be established. That way, Müller-Wohlfahrt and his colleagues are closinga major gap in sports medicine.But the work performed at the microclinicgoes beyond muscle injuries.Another area of focus is the connectionsbetween problems in the extremitiesand the spine as their site of origin. Theupcoming goals on the three physicians’“wish list” show how important it is forthem to keep up with current developmentsin MRI use: detection of biochemicalchanges that precede the morphologicaldegeneration in cartilage andoptimization of image precision throughfilter techniques. The close cooperationbetween the MW Center and <strong>Siemens</strong>1The German title will be published by Thieme in May2010. Publication of an English version is planned forthe end of 2010.<strong>Healthcare</strong> is of great importance toachieve these goals. Moreover, comprehensivecardiovascular diagnostics forboth professional and amateur athletesis under development.Matthias Manych is a biologist and freelancescientific journalist and editor specializing inmedicine. He regularly writes about imagingtechnology, among other topics.SummaryChallenge:• Optimum solutions for orthopedicand sports medicine problems• Precise MRI images to supplementmanual and sonographic findings• Scientific standardization of Müller-Wohlfahrt‘s empirical findingsSolution:• Detailed classification of muscleinjuries• The latest imaging options froma single source• Use of MRI precision and efficientworkflows• Establishment of standards in MRIdiagnosis of muscle injuries• Global networking with scientificand medical technology partnersResult:• Micro-clinic with optimized, stateof-the-artholistic care• Groundbreaking combination ofclassic orthopedics and sportsmedicine with methods of scientificresearch and radiology• Unique experience in orthopedicand sports medicine provided asstandards for physicians worldwideFurther Informationwww.siemens.com/sports-medicineMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 41
Breaking Down Tower WallsServing the more than 360,000 residents of the greater Tel Avivmetropolitan area as well as more than a million people whoenter the city daily, the Sourasky Medical Center handles a greatdeal of medical and administrative information. Back in the1990s, the center was more like a ’Tower of Babel’ with archaicmedical and clinical information systems that were unable tospeak with each other.By Abigail Weldon42 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Sourasky Medical Center in Tel Aviv serves the largest metropolitan area and the commercial center of Israel.Owned by Israel’s Ministry of Health, theSourasky Medical Center incorporatesthree hospitals, including 1,100 hospitalbeds, nearly 60 departments and institutes,and 150 outpatient clinics, whichall attest to this large network of possibledata sources. Growing competition fromother medical facilities further instigatedthe need to become more effective andefficient in the handling of information.A common platform to support the growingamount of acquired information,providing operational and medical staffwith comprehensive and up-to-date information,appeared to be the order ofthe day.A Tiger is ConceivedWhen Professor Gabriel Barbash, MD,MPH, was appointed General Director ofFrom the left: Professor Gabriel Barbash, MD, MPH, Esther Saiag, MD, Ronni Gamzu, MDTel Aviv Sourasky Medical Center in 1993,he was immediately confronted withthe lack of information for running themedical center. “I found that the IT thatsupported Sourasky’s activity, as well asnine other governmental hospitals, wasbased on IT that was programmed 34years ago,” says Barbash. After persuadinghis colleagues and the Israeli Ministryof Health that the hospitals needed tospeak a common language and were inneed of a common information system,Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine 43
Hospital ITso i.s.h.med was a clear choice.” Withthat, the hospital computerization projectcalled NAMER began – an acronym forthe Hebrew words for administrationof medical centers, which also meansTiger.i.s.h.med helps Sourasky Medical Center benefit from the availability of data and systeminteroperability.“The i.s.h.med system acts as acommunication system. We canspeak to each other about ourpatients, preventing mistakes.”Esther Saiag, MD, Director of Information and Computer Systems,Sourasky Medical Center, Tel Aviv, Israelhe was appointed General Director ofthe Ministry of Health. There, he was ableto convince the Ministry of Finance toallocate the financial resources togetherwith the Ministry of Health and governmentalhospitals to establish a new ITstrategy. This resulted in a new clinicalinformation system.Barbash’s persuasion efforts began totake form in 1999, when Israel’s governmentcomputerization project was initiatedwith the aim of computerizing theadministrative and operational systemsof the 11 governmental hospitals andcreating a common, comprehensive ITsystem. As Barbash notes, “From the outset,we stated that whatever system wasimplemented should meet the highestrequirements of the more complex facilitieslike ours. A hospital requiring lesscomplexity should be able to use the systemand utilize only part of what it offers.”The ministries and hospitals decided ondeveloping one system for all of the hospitals,reaching an agreement on whatwas going to be developed.Following a public tender, SAP for <strong>Healthcare</strong>as well as complementing modulesof <strong>Siemens</strong>’ i.s.h.med® 1 Hospital InformationSystem (HIS) were chosen. AsBarbash reports, “We were looking fora system that can talk to the SAP system,A Tiger is BornThe NAMER project went live at theTel Aviv Sourasky Medical Center in June2003 with the installation of the SAP for<strong>Healthcare</strong> infrastructure. The implementationof i.s.h.med followed in 2004,including the basis and radiology modules,followed by the i.s.h.med surgerymodule. Implemented in the hospitalwards, the basic module streamlineseffective order management by findingmanagement and medical documentation,enabling efficient and integratedmanagement of these processes, and providingthe infrastructure for additionali.s.h.med modules.Esther Saiag, MD, Director of Sourasky’sMedical Systems Operation and Informationand Computer Systems, reports thatthe implementation expanded with easeto other departments, including angiographyand cardiology: “The generic tools,like parameterized documents, makei.s.h.med highly adaptable to our individualrequirements at the hospital.” Saiagfurther reports satisfaction in being ableto adapt the modules to the center’sspecific needs. As an example, she listsbeing able to use the surgery and radiologymodules not only in angiography,but in the operating room (OR) as well.Implementation of additional i.s.h.medmodules continues to be an ongoingproject. In fact, due to the successfulexperiences with the system, theSourasky Medical Center – in line withan overall Ministry of Health decision –has decided to acquire all other i.s.h.medmodules. Currently, the center is operatingunder seamless interoperability1i.s.h.med is available in Austria, Belgium, Chile,Colombia, Germany, Hong Kong, Italy, Luxembourg,Mexico, Netherlands, New Zealand, Singapore, SouthAfrica, Spain, and Switzerland by <strong>Siemens</strong> and infurther countries via trusted Partners. Please alwaysconsult with <strong>Siemens</strong> HS EU for availability questions.44 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Hospital ITbetween SAP/i.s.h.med and the laboratorysystem. It is also pursuing the i.s.h.medimplementations in various units, such ascardiology and angiography.A Tiger RunsWith the successful implementation ofthe NAMER project, Barbash points to theavailability of data as being a key benefit.“Whatever I expected – we got it,” hesays. “The amount of data that today iscritical to our management, to our competitiveenvironment, is really a gift.”Clinical and administrative data alongwith information about reimbursementpayments and various hospital activities– now readily available thanks toNAMER – proves to be a vital componentto staying competitive in the healthcareenvironment.Saiag notes the seamless interoperabilitybetween i.s.h.med and other clinicalinformation systems in the hospital. “Invarious locations in the hospital, i.s.h.medserves as the backbone, while at thesame time receiving information fromother medical information systems,” shesays.In terms of OR efficiency, Ronni Gamzu,MD, Director of the General Hospitalat Sourasky, notes the benefits of centrallylocated screens providing informationabout specific operating rooms.i.s.h.med’s surgery and radiology modulesallow the center to produce utilityreports based on department, providinginformation as to who is in the respectiveoperating room and the downtimein each. Gamzu stresses the importanceof efficiency: “With limited time in theOR, running the facility in a more efficientway is a must for the hospital manager.i.s.h.med helps leverage your managementskills in such a huge complex.”A Tiger Takes OffAs part of a developmental partnershipwith <strong>Siemens</strong>, a team comprised ofmembers from Sourasky Medical Center,the Ministry of Health, and other hospitals,is working to develop and shape twonew modules with key functionalities incharting and ward support. The partner-ship’s primary focus is enhancing thesupport of clinical processes and charting.A documentation workstation integratingthe various i.s.h.med functionalities,a progress note computerizing patients’courses of treatment, and clinical overviewsof key treatment information areall part of the effort to improve clinicalprocesses. As part of the charting focus,the Tel Aviv Sourasky Medical Center iscurrently cooperating with <strong>Siemens</strong> todevelop the next-generation electronicpatient record system, which is plannedto be timeline-based with a graphicalinterface. The new applications will alsofocus on the various functionalitiesrequired for managing inpatient careprocesses, and be deployed at SouraskyMedical Center in 2010.Barbash expects the additional i.s.h.medmodules to further increase the availabilityof clinical data and is looking forwardto being able to analyze data fromboth a financial and a quality perspective.He explains, “We will then have aconsiderable volume of clinical data atour fingertips to allow us to analyze andassess quality. The major benefit is thatavailability, quality assessment, and efficiencyassessment of the hospital are allgoing to be much, much easier.”And is Sourasky a Tower of Babel no more?Saiag remarks, “The i.s.h.med systemacts as a communication system, and wespeak to each other about our patients,preventing mistakes.” This common languagehelps the staff perform its dailyroutines more efficiently and economically.She adds, “Now, we can save moneythat previously was wasted because ofa lack of knowledge, mistakes, and soon. The benefits of i.s.h.med are trulyimpressive!”Abigail Weldon is a member of the MedicalSolutions editorial team.Further Informationwww.siemens.com/ishmedSummaryChallenge:• Integrating the handling andcreation of medical and administrativeinformation• Modernizing and computerizing outdatedmedical and clinical systemsthat are unable to speak with eachother• Incorporating the needs of smallerand larger, more complex facilitiesinto one implementation projectSolution:• NAMER hospital computerizationproject encompassing SAP and<strong>Siemens</strong> i.s.h.med hospital informationsystems• i.s.h.med system that is able to talk,correspond, exchange data, and integratewith the SAP system• Customizable i.s.h.med modules forimplementation in various hospitaldepartmentsResult:• Greater availability of data on onecommon platform• Seamless interoperability betweeni.s.h.med and other clinical informationsystems, enabling varioussystems to talk to one another• Greater efficiency, quality, andserviceMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 45
Molecular ImagingThe Future of Vulnerable PlaqueDiagnosis: Molecular Imaging<strong>Siemens</strong> <strong>Healthcare</strong> and Cedars-Sinai MedicalCenter in Los Angeles, California, USA, arecurrently collaborating on studies designed toimprove the identification of cardiovasculardisease with molecular imaging. While theclinical use of this technology is still years away,the studies are expected to provide valuableinsight into how plaque can be diagnosed beforeit becomes hazardous.By Robert L. BardHartmuth Kolb, PhD, Vice President of<strong>Siemens</strong> Molecular Imaging BiomarkerResearch, is working with Cedars-SinaiMedical Center scientists to evaluate novelmolecular biomarkers in cardiovasculardisease. Currently, two proprietary positronemission tomography (PET) tracersthat have been developed by <strong>Siemens</strong>are being evaluated, 18F-RGD-K5 (K-5)and 18F-HX-4 (HX-4). Daniel S. Berman,MD, Director of Cardiac Imaging Research,and Balaji Tamarappoo, MD, ResearchFellow in Cardiac Imaging, are leadingthe studies at Cedars-Sinai. The ultimategoal of this line of research is to improveidentification and evaluation of cardiovasculardisease.Currently, imaging in cardiovascularmedicine is limited to the identification ofischemia or obstruction in the vascularlumen. Even if artherosclerotic plaque inartery walls can be visualized, cardiologistsare not yet able to determine howactive the disease process is. This problemis particularly important for the heart.As Berman remarks, “In stable heartdisease, the most prevalent form of heartMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 47
Molecular Imaging“Currently, we arechasing plaquesthat are notrupture-prone.”Daniel S. Berman, MD, Director,Cardiac Imaging Research,Cedars-Sinai Medical Center,Los Angeles, California, USAdisease, we do not have very good toolsto determine who is at the highest riskfor a heart attack and, therefore, wouldneed the most specific, aggressive therapy.Currently, we are often performingexpensive procedures such as angioplastyor bypass surgery in patients with stableplaques, in whom these procedures maynot be necessary.”Imaging Challenges in CardiovascularMedicineBerman adds that recent clinical trialsshow the majority of stable patients willnot suffer a cardiac event if they weresimply treated medically. “Patients withischemia and stenoses can go for yearswithout an event while others with noblockages but a vulnerable plaque rupturecan have an event.”biomarkers can be incorporated intoimaging strategies to identify high-riskpatients. Vulnerable plaques exhibit acomplex disease biology, comprising aninflammatory component, cap ruptureand healing, intraplaque angiogenesisand hemorrhage, calcification, andthrombus formation. A ruptured plaqueis dangerous, because it is likely to interruptthe blood flow and cause a heartattack. The K-5 tracer can potentiallyidentify angiogenesis, and it is hypothesizedto improve the identification ofvulnerable plaques in patients at risk forcardiovascular events.Tamarappoo further explains that anadditional trait of plaques is a lack of oxygencontent, or hypoxia, that is directlyrelated to inflammation. The inflammatoryresponse within a vulnerable plaqueHartmuth Kolb, PhD, of <strong>Siemens</strong> Molecular Imaging Biomarker Research (left) is working closelyA primary challenge in clinical cardiovascularmedicine is ’high-risk plaqueidentification’, or identifying the plaquesthat are rupture-prone or ’vulnerable’.<strong>Siemens</strong> has developed molecular biomarkersspecific to the characteristicsof vulnerable plaques and hopes theseinvolves the consumption of oxygen, andthe HX-4 tracer was specifically designedto identify hypoxic cells. When oxygenis not present, HX-4 will stay within thecell. Therefore, when plaques are imaged,an elevated presence of HX-4 may differentiatethose that may be rupture-prone48 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Molecular Imagingand thus likely to cause a cardiac eventfrom those that are stable and thereforeless likely to be clinically significant. Kolbreports that Phase II clinical studies havefound the tracers may be effective forimaging cancerous tumors and that bothK-5 and HX-4 are cleared rapidly fromthe body.The collaborative studies betweenCedars-Sinai and <strong>Siemens</strong> are the firststudies to assess the use of these agentsin cardiology. They are also exploringnew PET myocardial perfusion agents thatare likely to be beneficial because theyare taken up linearly across the range ofblood flow, unlike current agents thatdegrade or have a ’roll-off’ effect overtime. The linear uptake allows for thedetection of perfusion deficits that wouldotherwise not be visualized with theto identify a vulnerable plaque. CurrentPET scans already use FDG as a tracer forimaging vulnerable plaque. However,vulnerable plaques may be undetectablebecause the FDG is taken up by both thevulnerable plaque and the myocardium(heart muscle). Thus, the myocardiumcan mask the signal from a vulnerableplaque. The new tracers are not taken upby the myocardium, potentially circumventingthis problem.Collaborative StudiesImaging of the coronary vessels has specificchallenges related to the size andlocation of potential lesions. The coronaryvessels are located on the surfaceof the heart, and any potential lesionsare moving targets, because the heart isalways beating and the patient is always“Patients with noblockages but avulnerable plaquerupture can havean event.”Daniel S. Berman, MD, Director,Cardiac Imaging Research,Cedars-Sinai Medical Center,Los Angeles, California, USAwith Daniel S. Berman, MD, of Cedars-Sinai’s cardiac imaging unit (right).standard SPECT (single photon emissioncomputed tomography) approach. Theseinvestigators are also exploring the useof PET scans with FDG (fluorodeoxyglucose).FDG works in a much differentmanner; it identifies the presence of glucosemetabolism and can limit the abilitybreathing. Furthermore, lesions withinthe coronary arteries are very small,typically only a few millimeters in lengthand width. Because of these limitationsand the fact that these new tracers havenot been evaluated in cardiology, thecurrent studies are focusing on carotidMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 49
The K-5 tracer may identify angiogenesis and improve the identification of vulnerable plaques in patients at risk for cardiovascular events.disease as a proof of principle prior toassessments in the coronary arteries.Berman and Tamarappoo are currentlyevaluating these new molecular biomarkersin a study of 20 patients at Cedars-Sinai Medical Center who have carotidartery disease and require surgical intervention.Prior to the intervention, eachpatient will have a PET scan with CT(computed tomography); ten patientswill be injected with the K-5 tracer andten patients will be injected with theHX-4 tracer to determine where the radioactivityis localizing. Patients will undergocarotid endarterectomy to remove theplaque, and the plaques will be histologicallyevaluated with an emphasis onidentifying inflammatory markers. Theability of the new scanning techniquesto identify inflammatory plaques willthen be compared to these inflammatorymarkers to determine the effect of theseagents to identify vulnerable plaques.<strong>Siemens</strong> and Cedars-Sinai are also collaboratingon a preclinical study of themolecular biomarkers to determinewhether angiogenesis is increased duringthe progression of atherosclerosis.These studies are likely to give insightinto the ability to identify vulnerableplaques at an earlier stage, potentiallyidentifying a plaque before it becomeshazardous. The study involves apoE(Apolipoprotein E) knockout mice, whichis a well-established mouse model forhuman atherogenesis. These mice aregenetically engineered to develop atherosclerosiswithin 24 weeks. The protocolalso involves feeding the mice a high-fatdiet to accelerate their plaque development.The mice are given baseline andfollow-up PET scans with CT after 14weeks, and the tracers are expected tobind to the atherosclerotic plaques.50 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Molecular ImagingSummaryChallenge:• Proper risk stratification of patients’likelihood of having an event such asa heart attack• Poor accuracy of current clinicalpractice and imaging modalities thatfocus on the amount of obstructionthat a plaque causes within an arteryand/or on the amount of ischemiathat the obstruction causes• Often, rupture-prone plaques thatare likely to cause a cardiovascularevent are not identifiedSolution:• Molecular tracers that are specificto the characteristics of ruptureprone,vulnerable plaque are currentlybeing evaluatedBerman foresees a scenario where molecularbiomarkers are more widely used inresearch projects to identify cardiovasculardisease. He also notes that molecularbiomarkers would be useful to currentstudies that involve stem cells.Future Uses of MolecularImaging BiomarkersCurrent stem cell studies are usingmagnetic resonance imaging to quantifyareas of myocardial injury. In these studies,patients with cardiovascular diseasehave heart muscle removed by transvenousmyocardial biopsy, and the cellsare cultured and then injected back intothe heart. Berman believes that, if theinjected cells are labeled with a molecularbiomarker, molecular tracers may providevaluable, specific information tounderstanding the process. Such tracingmay provide mechanistic informationassociated with the therapeutic response.The clinical use of molecular biomarkerimaging is several years away and pendingstringent assessments in multiplehuman studies in the evaluation of cardiovasculardisease. But thus far, the useof molecular biomarkers is promising forthe discrimination of benign plaquesand vulnerable plaques that are likely tocause a cardiovascular event.Robert L. Bard is a freelance medical writercertified by the American Medical Writers Association,who also conducts clinical research atthe University of Michigan’s Division of CardiovascularMedicine.The Cedars-Sinai Medical Center has a cooperationcontract with <strong>Siemens</strong> <strong>Healthcare</strong>.Further Informationwww.siemens.com/biomarkersResult:• Collaboration of <strong>Siemens</strong> MolecularImaging Biomarker Research andCedars-Sinai Medical Center scientistson studies designed specifically toinvestigate the use of molecular biomarkersin cardiovascular medicine• A preclinical study is investigatingthe ability of these tracers to identifynot only the presence, but also theprogression of atherosclerosis• Human studies of carotid atherosclerosisare being conducted, wheremolecular imaging results are beingcompared to inflammatory markersin the removed plaque• Thus far, the use of molecular biomarkersis promising for discriminatingbetween plaques that are benignand plaques that are vulnerable andlikely to cause a cardiovascular event• The clinical use of molecular imagingis several years away and pendingstringent assessments in multiplehuman studies in the evaluation ofcardiovascular diseaseMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 51
A Leap into 21 st Century DiagnosticsWith the National PET Center for medical diagnostics, whichwas supplied in turnkey condition by <strong>Siemens</strong>, the ClinicalCenter of Serbia has made a giant step forward in raising thecountry’s standards of diagnosis and treatment control tothose of Western European levels. Vladimir Obradovic,Director of the Institute of Nuclear Medicine, explains theimportance of this project against the backdrop of healthcarereform in Serbia.By Andreas Ernst52 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
The Clinical Center of Serbia, located inBelgrade and completed in the mid-1980s,is one of the world’s largest hospitals,with 3,500 beds, a staff of 7,500, and1,200 physicians. The facility has beenmarked not only by the proud history ofthe Yugoslavian healthcare system, whichled the region in the 1970s, but also bythe effects of the Balkan War in the 1990s.Things began to improve again ten yearsago when the Serbian healthcare systemfirst started to look like a bustling constructionsite. Across the board, fromfinancing to training to infrastructure,reform is still in progress, with the aim ofhelping the Serbian healthcare systemcatch up to Western European standards.And nowhere more so than in the basementof the Clinical Center, which hasbeen home to the National PET (positronemission tomography) Center since thefall of 2009. When Professor VladimirObradovic opens the door to the PETCenter for us, he tells us with a smile,“Now we’ve arrived in the 21 st century!”The contrast to the dark corridors in theClinical Center above us is impressive:The walls of the department, which occupies700 square meters of space, gleamin a soft pink tone. Behind thick greenishsteel-reinforced safety glass is the center’sheart – and its pride and joy: a <strong>Siemens</strong>Biograph 64 TruePoint PET·CT unit.To help ensure that this system is put tooptimum use, <strong>Siemens</strong> worked togetherwith clinic management and local serviceproviders to develop a comprehensivesolution covering everything fromthe center’s integration into the clinic interms of business administration to constructionplanning and even the efficientorganization of workflows. As a result,employees are offered the best possibleworking conditions, while the clinic’sdiagnostic capacity is greatly increased.Professor Obradovic, what does thenew PET Center mean for healthcarein Serbia?OBRADOVIC: The new PET Center putsus where we want to be: at the forefrontof modern diagnostic technology. PET,as a diagnostic method in nuclear medicine,represents a quantum leap in thequality of our healthcare system.What is your role in this project?OBRADOVIC: The Ministry of Healthappointed me to serve as the presidentof a project group made up of radiologists,oncologists, and neurologists, in2005. The group was commissioned withmaking preparations for the introductionMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 53
Turnkey SolutionsBiographyProfessor Vladimir Obradovic, MD, PhD, isone of the leading nuclear medicine specialistsin Serbia. Since 1995, he has been the Directorof the Institute of Nuclear Medicine at theClinical Center of Serbia in Belgrade. After completinghis studies of medicine in Belgrade, heearned a second doctorate in natural sciences.He went on to further study in Paris, France,and in Tübingen, Germany, before taking thehelm at the Institute of Nuclear Medicine. Since1996, he has taught at the medical school atthe University of Belgrade as a full professor.Obradovic is married to Zorica Petrasinovic,who also works at the Clinical Center of Serbiaas an internist and cardiologist.<strong>Siemens</strong> in Serbia<strong>Siemens</strong> has been active in Serbia since 1887. The company wasresponsible for building the country’s first power plants and forinstalling the first public lighting systems in the city of Belgrade in1887. The Yugoslavian division of <strong>Siemens</strong> AG, based in Zagreb,was founded in what was then the “Kingdom of Serbs, Croats, andSlovenes.” The office in Belgrade was responsible for supplying powercars for the streetcar lines in the capital city. A department focusingon medical technology was also founded there in 1929. The Serbiancompany <strong>Siemens</strong> Elektrizitäts AG (Electricity Corp.) was foundedduring the German occupation in 1941. In communist Yugoslaviaas well, <strong>Siemens</strong> remained an important supplier for the staterailway and telephone services. Today, the company is responsiblefor serving Serbia and Montenegro. After the country embraceddemocracy in 2000, <strong>Siemens</strong> was involved in rebuilding the countryas a leading provider of infrastructure and technology.of this technology. The focus was notonly on the National PET Center, whichis ready here, but also on introducingPET throughout the country. Our centeris the basis for satellite centers, smallerunits located throughout the countrythat are supposed to provide full-coveragecare. The national center has a clinicalmandate, but at the same time, itserves to train specialists and is used forresearch purposes in the area of diagnostics.What is special about planningand equipment at the National PETCenter?OBRADOVIC: The project has two phases.The first was the construction of a turnkeyPET Center by <strong>Siemens</strong>, which cameinto operation in the fall of 2009. Thecenter has a hybrid PET/CT unit, whichwill soon be joined by a second unit.For the next step, we are planning toinstall a cyclotron so that we can producethe radiolabeled tracers for PET/CTscanning ourselves. Because some ofthese radionuclides have short half-lives,it is important for us to produce themin close proximity to where they will beused. At the site, we will operate a smallfactory for radiopharmaceuticals to supplynot only our center, but also thesatellites throughout the country.Will your in-house production ofradionuclides also yield economicbenefits for you?OBRADOVIC: Yes, it will help us cutcosts. Today, the costs of an exam runat about 1,000 euros. If we producethe radionuclides ourselves, we canreduce that figure by about 60 percent.We will be the first center in the regionto produce radionuclides. It is a definitepossibility that we could produce radionuclidesfor PET centers in neighboringcountries, such as Croatia, Macedonia,or Romania.Why did you choose <strong>Siemens</strong> for theimplementation of the PET center?OBRADOVIC: We ran a request for proposals,and <strong>Siemens</strong> came out with thebest results. That was primarily due tothe value for the money; the technologyoffered by the various providers is verysimilar, but <strong>Siemens</strong> was also willing totake special technical requests into consideration.In fact, we want to use thesystems not only to perform routineexaminations, but also to implementresearch projects. We were also quicklyable to reach an agreement regardinghow to finance the training of specialists.And finally, there is the fact that<strong>Siemens</strong> has a very good, longstandingbasis in our region. That is advantageouswhen it comes to service.How many PET centers does Serbianeed?OBRADOVIC: Each PET unit serves theneeds of about a million people. Thatmeans that to cover Serbia’s populationof nearly seven million, we need sevensystems. That’s the medical side of theequation – whether it can be put intopractice, of course, depends on the country’sability to finance it.What will change for patients thanksto the new center?OBRADOVIC: We will be able to diagnosecommon diseases, such as cancers, neurologicaldisorders, and cardiac diseasesmore quickly and with greater precision.Following a primary diagnosis, whichserves as an indication for diagnosis withPET, the process of establishing overallfindings will be fast. That helps improveour patients’ chances of recovery. Theincidence of malignant tumors is on therise in this country, a fact that is prob-54 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Turnkey SolutionsTurnkey Solution:The National PET Center in Serbia<strong>Siemens</strong> doesn’t just supply equipment, it offers holistic solutions. “TheClinical Center provided us with 800 square meters in the basement of thefacility, and just told us, ‘okay, get to work’,” explains Ratko Krakovic of<strong>Siemens</strong> <strong>Healthcare</strong>. The project management activities included the fullplanning for the unit in cooperation with architects and engineers. In addition,the company had to coordinate the work performed by nine suppliercompanies, which had been called in to provide a range of services fromradiation protection to computer equipment and furnishings. One extremelyimportant factor was the close cooperation between <strong>Siemens</strong> and Neimar,a leading construction company in Serbia. <strong>Siemens</strong> was even able to obtaina building permit – no easy task in Belgrade’s bureaucratic jungle – within avery short period. In total, 19 sub-projects were implemented, some of themin parallel, until finally, after just one-and-a-half years, the government-runInstitute of Nuclear Sciences for Radiation Protection in the town of Vincagranted its approval for the facility to start work.ably connected to the many aspects ofphysical and mental strain that affect usin our postwar society. At present, weexamine ten patients per day. Later, whenwe are producing radiopharmaceuticalsourselves, thanks to the cyclotron andthe radiochemical lab, the number willbe at least 30 each day.Serbia’s healthcare system was isolatedfor a long time. What kind of internationalnetworks are in place today?OBRADOVIC: In our field, there is intensiveinternational cooperation with bodiessuch as the International Atomic EnergyAgency, which finances research projectsat our institute. We also regularly sendspecialists abroad for continuing educationand training, and experts from elsewherein Europe, the United States, andAsia visit us as well. These contacts showthat Serbia is being integrated more andmore into the international research landscape.But Serbia also has its own 50-yeartradition of nuclear medicine: The CentralLaboratory for Nuclear Medicine wasfounded in Belgrade in 1958.What will be the greatest challengesfacing the Serbian healthcare sectorover the next few years?OBRADOVIC: A technological shift indiagnostics, such as the one representedby the introduction of the PET method,is critically important. A lot has been donewith regard to the infrastructure of ourhospitals and institutes – but there is stilla long way to go. The pace of reform, ofcourse, depends on the general economicdevelopment in the country. Luckily,we still have most of our specialists – atleast in my specialty. I hardly know anyonewho left during these difficult years.All of us have stayed here, and we areall working enthusiastically on furtherdeveloping nuclear medicine. Thanks tothe cutting-edge technology we havehere, and in light of our intensive cooperationwith colleagues from all over theworld, there’s no reason to go anywhereelse!Andreas Ernst is a correspondent for variousGerman-language newspapers. He lives inBelgrade, Serbia.Further Informationwww.siemens.com/biographSummaryChallenge:• Improve diagnosis of oncological,neurological, and cardiologicaldiseases• Shorten waiting times for patients• Regionalize high-tech diagnosticsSolution:• Integral planning and developmentof a turnkey PET/CT center incooperation with the clinical facilityand suppliers• <strong>Siemens</strong> Biograph 64 TruePoint PET·CTfor diagnosis, treatment control, andresearch work• Independent production of radiopharmaceuticalsto reduce costs andfor distribution to PET centers in thesurrounding area• Development of satellite units atregional hospitalsResult:• Faster diagnoses• Infrastructure not only for clinicalapplication, but also for researchand education• Long-term partnership with <strong>Siemens</strong>for countrywide development of thediagnostic infrastructureMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 55
ServicesService Provides HighAvailabilityWhen it comes to service for its medical equipment, the NurembergHospital (Klinikum Nürnberg) in Germany relies on the <strong>Siemens</strong>Guardian Program, as part of which, the TubeGuard option plays animportant role.The availability of medical equipment isone of the most crucial factors affectingeconomic efficiency at any clinical facility.Unexpected failures and downtimes canquickly lead to gaps in the provision ofcare and significantly affect the facility’sincome. With the Guardian Program,<strong>Siemens</strong> has put together an extensiveservice package that continuouslyremotely analyzes equipment in real time,making it possible to predict failures anddowntimes, and, thereby, helps ensuresystem availability. The Nuremberg Hospitaldecided on this service as part ofa facility-wide service and maintenanceagreement.“We feel thatwe are a kindof premiumcustomer for<strong>Siemens</strong>.”Reinhard Loose, MD,Head of the Department of Diagnosticand Interventional Radiology,Nuremberg North Hospital, GermanyWith nearly 5,600 staff members andabout 2,180 beds at two locations in thenorthern and southern parts of Nuremberg,the hospital serves 90,400 inpatientsand 93,300 outpatients each year.At the Center for <strong>Healthcare</strong> Professionals,about 360 trainees and apprenticesare currently learning and being trainedin their specialties.Keeping a major medical facility like thisone up and running largely depends onthe service and maintenance of its medicalequipment. With the aim of ensuringthe availability of medical equipmentwithin the facility, the Nuremberg Hospitalhas now signed an extensive facilitywideservice and maintenance agreementwith <strong>Siemens</strong> <strong>Healthcare</strong>. The agreementis scheduled to run for a five-year termand encompasses all radiological andimaging procedures, which – for the facilityin Nuremberg – means computedtomography (CT), magnetic resonanceimaging (MRI), and X-ray systems.The new agreement also covers nuclearmedicine. It provides standard servicesas well as essential maintenance contractsand full-service agreements, coveringeverything from replacement parts to theavailability of <strong>Siemens</strong> technicians. Theagreement was drafted in close cooperationwith the Nuremberg Hospital management,so it was possible to take all ofthe hospital’s requests and local particularitiesinto account. “Of course, we haveto be able to rely on rapid response fromservice experts. This works excellentlywith <strong>Siemens</strong>,” explains Michael Wucherer,PhD, Head of the Department of MedicalPhysics at the Nuremberg Hospital.“<strong>Siemens</strong> is an important partner for us,and our experience with them has beenexcellent, so it was an obvious step forus to sign this agreement with <strong>Siemens</strong>.It’s also a sign of how much trust andconfidence we place in them!”Sensor Readouts via Data LinkThe services provided as part of the agreementare grouped into various serviceoptions. One of them is the remotemonitoring of the medical equipment.As part of this service, the system proactivelysends performance data to the<strong>Siemens</strong> Service Center so that <strong>Siemens</strong>UPTIME Services is able to detect potentialdisruptions early on and can eliminatethem right away.<strong>Siemens</strong> UPTIME Services not only allowstechnicians to monitor and automaticallyupdate system software via data link,but also enables rapid problem analysisand repairs via remote access. This meansthat the system is able to detect potentialdisruptions early and eliminate themright away, before they cause any problems.Once an error message is received,the data that have been transmitted areanalyzed right away. In the event of anerror, the experts at <strong>Siemens</strong> contact theappropriate service technicians at theNuremberg Hospital within 15 minutes.If possible, faults are resolved via remoteaccess. If this is not possible, a <strong>Siemens</strong>technician arrives onsite within just afew hours.Of course, the appropriate staff membersat the Nuremberg Hospital are able tocontact <strong>Siemens</strong> service representativesdirectly if worst comes to worst. Andthanks to the service and maintenanceagreement, this service is not limited to56 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
ServicesLeft to right: Roland Simmler, IT Manager, Reinhard Loose, MD, Head of the Department of Diagnostic and Interventional Radiology,and Michael Wucherer, PhD, Head of the Department of Medical Physics at the Nuremberg Hospitala specific kind of equipment or subjectto different rules: “The different kinds ofservices have been harmonized. There isa standing rule on how to reach servicetechnicians. This way, we feel that we area kind of premium customer for <strong>Siemens</strong>,”says Reinhard Loose, MD, a universitylecturer with a double doctorate and theHead of the Diagnostic and InterventionalRadiology Department at the hospital’sNorthern site. “I am very happy with the<strong>Siemens</strong> Service Center because I alwayshave a contact person who understandsmy problems,” Wucherer adds.Rapid Response Times MoreImportant than AvailabilityWhen preparing for the service call aswell as during the actual service, the techniciancan access the monitoring dataanytime, which facilitates fast resolutionof the issue.The conditions that apply in a major hospitalare, of course, different from thoseone would find in a smaller practice. Evenwhen medical equipment is guaranteedto be available 97 percent of the time, itdoes not mean that it will not be downfor a couple of days during the year. Forcases like these, a medical facility wouldhave to report that the piece of equipmentin question – such as a CT unit – isout of service. “I would have to reroutea number of processes, even calling offthe helicopters,” Loose explains. “If thereis an error, it is very important for me toMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 57
Serviceshave the technician arrive onsite quicklyand resolve the error.” The proactiveremote monitoring of the <strong>Siemens</strong>Guardian Program provides the fastestpossible technician response times:Technicians respond within four hours,and the contract guarantees that theerror will be resolved within 24 hours.TubeGuard Monitors CT UnitsAnother option available through the<strong>Siemens</strong> Guardian Program is TubeGuard,which is available for <strong>Siemens</strong>’SOMATOM® Definition computed tomography(CT) scanners. System availabilitydepends, to a crucial degree, on the X-raytubes used in the unit. Each tube is apart that is subject to replacement forwear and tear, and they see varying levelsof use. If their performance deterioratesslowly over time, they may fail at anytime, without clear warning signs.The result is an unplanned system failure,termed a ’hard down’. Loose reports,Service Agreementfor the NurembergHospitalThe extensive facility-wide serviceand maintenance agreementbetween the Nuremberg Hospitaland <strong>Siemens</strong> <strong>Healthcare</strong> is scheduledto run for a five-year termand encompasses all radiologicaland imaging procedures as wellas nuclear medicine at the hospital.One important option of the<strong>Siemens</strong> Guardian Program isTubeGuard, which can be used toreliably predict CT tube failures ofSOMATOM® Definition scannersearly on, preventing the unscheduledfailures known as ’harddowns’. The ability to scheduletube replacements minimizesworkflow disruptions, helpsschedule patient appointmentsproactively, and contributes tosignificant gains in equipmentreliability and patient satisfaction.“Any unplanned failure is, of course, amini-worst-case scenario.” With theGuardian Program including TubeGuard,it is now possible to predict critical lossesin performance – and thus tube failure –reliably and in due time. The tube canbe replaced at the best possible time,resulting in only a ’soft down’. Loose continues,“For us, service downtime hasbecome something we can schedule. Thisis good for the patients and for our facilityon the whole, because we can avoidbottlenecks.” More than ten sensors proactivelymonitor the CT unit’s primaryfunctions, such as tube current, anoderotation, and oil temperature. Using thisinformation as a basis, <strong>Siemens</strong>’ expertsapply complex algorithms to calculate atube’s remaining life span and determinethe likelihood of a failure and when itwill occur. Then, the Nuremberg Hospitalis promptly notified of the deviatingparameters and a date is set for a scheduledtube replacement, for instance,during downtime that has already beenscheduled. This minimizes disruptions inthe hospital’s workflow. “With TubeGuard,<strong>Siemens</strong> has taken on a pioneering role,”Wucherer explains. “With this factorembedded in the service agreement, notonly can we plan better, but <strong>Siemens</strong> canas well. The technicians have to makefewer unscheduled service calls.“The facility-wide service and maintenanceagreement yields a number of benefitsfor the Nuremberg Hospital. The ongoingremote monitoring of medical equipmentenhances operational reliabilityand system availability. Service calls arecompleted quickly and can be scheduledas needed. This results in fewer systemfailures and thus, less waiting time andimproved patient throughput. The serviceagreement with the Nuremberg Hospitalalso includes a reimbursement component.The more service <strong>Siemens</strong> performs,the greater the discount to the hospitalduring the billing process. This representsa win-win situation for both partners.“This kind of discount structure was acrucial factor in our decision in favor ofthis service agreement,” Loose explains.“We have service costs of over one millioneuros a year – so every percentagedifference has a definite impact.”SummaryChallenge:• Keeping CT and other imagingequipment up and runningwith minimum downtime despiteheavy wear and tear• Maintaining patient satisfactionand comfort level• Tight appointment schedulingat CT, MRI, ultrasound, and angiographysystems• System failure impedes workflowSolution:• <strong>Siemens</strong> Guardian Program includingTubeGuard for predictingand proactively avoiding potentialCT tube failures• Ongoing assessment via proactiveand real-time remote monitoringwith <strong>Siemens</strong> Remote Service• Proactive service, for example,faster response and repair timethrough real-time monitoringof system parameters with the<strong>Siemens</strong> Guardian ProgramResult:• Reduction of system downtime• Improved workflow in theradiology department and in theentire hospital• Ability to have necessary tubechanges done during prescheduledservice calls• No breakdowns means no waitingfor patients• Less revenue lossFurther Informationwww.siemens.com/guardian-programwww.siemens.com/remote-service58 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Improving Care, Reducing Costs:Successful CPOE Implementation atDenver HealthDenver Health implemented CPOE ten years ago with the goal ofimproving patient care, safety, and efficiency. Now, with 95 percent oforders entered electronically, this early adopter is taking its process tothe next level by migrating to the <strong>Siemens</strong> Soarian platform.By Amy Erickson VaughanDenver Health and Hospital Authority, inDenver, Colorado, U.S., ranks in the topfive percent of US hospitals in terms ofthe implementation of health informationtechnology. It provides care to morethan 160,000 individual patients – oneout of every four people in Denver – annually.The hospital has invested more thanUS$330 million in healthcare informationtechnology (HIT), and over 250,000orders per month are generated via ComputerizedPhysician Order Entry (CPOE)capabilities. According to Andrew Steele,MD, Director of Medical Informatics forDenver Health, “The driving force behindDenver Health’s implementation of CPOEwas to support our initiatives for improvingpatient safety and the quality, effectiveness,and efficiency of care.”Steele is proud of the many efficienciesgained at Denver Health from applyingthe CPOE process, including a reductionin the human element in medicationerrors, a standardization of care, and legi-ble physician orders. The major ancillarydepartments, like laboratory, radiology,and pharmacy, have bidirectional interfaces,which allow for rapid communicationof orders and less transcribing andreentering of data. “A clearly legible, electronicorder does not require additionalinterpretation and results in fewer callbacksfor clarification, leading to moretimely and efficient care,” explains Steele.“With standardized CPOE, we now getcomplete orders. The clinicians puttingMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 59
Medication ManagementBarcoding helps verify the five patient rights: the right drug in the right dose at theright time given to the right patient via the right route.has been an 83-percent reduction in timebetween medication order and availabilityfor administration, and a 62-percentreduction in radiology turnaround time. 1Steele credits the effective rollout ofCPOE to careful planning, strong leadership,and having physicians, nurses, pharmacists,and HIT staff involved at manylevels to provide ongoing feedback. Healso attributes the project’s success toDenver Health’s partnership with <strong>Siemens</strong>.“We wanted to have a long-term partner,and in looking at where we wanted to bein ten to 20 years, we selected <strong>Siemens</strong>.They seemed to be committed to thelong term, and that was important to usat Denver Health,” says Steele. “We havestructured our relationship to make surethe service is there every single day, andI think on the flip side, they truly want tobe there for us.”in the order have to dot every ‘i’ and crossevery ‘t’. The computer is not ambiguous.”Patient-Centered CareDenver Health combined CPOE capabilitieswith barcoding to create a seamless,interoperable process that promotes continuityof care for each patient throughoutthe entire course of treatment. “Barcodingand CPOE create a closed-loopmedication process,” says Steele. “Whenan order is placed in CPOE by a physician,that order is transmitted to the pharmacyfor validation, then released electronicallyto a large dispensing machine, calleda Pyxis, which contains about 80 percentof the medications that nurses commonlyuse. Then, the nurse uses a hand-heldscanner to scan her own identificationbadge so we know who administered themedication. She also scans the barcodeof the medication, as well as a barcodeon the patient’s wrist band.” If the patientand the medication order match, thenshe administers the drug. “This closedloopprocess allows us to confirm that theright drug is given in the right dose atthe right time to the right patient via theright route,” Steele says.In addition to more consistent patientcenteredcare, the CPOE process alsooffers a significant cost benefit. “Whenpeople look at the cost of care, about 80percent of the cost is controlled by thephysician or clinician. It is up to the physicianto order an expensive test. The testis not given unless a physician orders it,so the cost and quality of care is in thehands of the ordering physician,” explainsSteele. At Denver Health, evidencebasedassistance for clinicians has beenembedded into the CPOE workflowimplementation, which gives physiciansinstant access to best-practice information.Additionally, Steele has the abilityto generate individual customizationsthat save money. For example, in collaborationwith the HIT department, hewas able to create a solution in four daysthat reduced misordering of a US$125test by 82 percent. 1Launching CPOEDramatic changes have occurred sinceDenver Health began applying its CPOEprocess in 2001. According to Steele,before CPOE, lab turnaround time was142 minutes; following CPOE initiation,turnaround time was 63 minutes. There1The outcomes achieved by the <strong>Siemens</strong> customersdescribed herein were achieved in the customer’s uniquesetting. Since there is no “typical” hospital and manyvariables exist (e.g., hospital size, case mix, level of ITadoption), there can be no guarantee that others willachieve the same results.Soarian MigrationAs Denver Health celebrates its 150 thanniversary this year, the hospital systemcontinues its early adopter status bymigrating from INVISION® to a Soarian®platform. “We want to be using the mostadvanced technology, and moving to theSoarian platform creates better integrationfor our major clinical applications,”says Steele. “The applications all have asimilar look and feel. Previously, we hadto jump to different applications to seeinformation, but now, with Soarian, wehave a more complete view of patientinformation.”Another advantage of moving to theSoarian platform, according to Steele, isthe ability to make changes to the system.“Moving from INVISION to Soarian,we gain enhancements through bettertechnology and can make changes tothe system in order to tailor it to DenverHealth’s needs,” he says. “Because Soarianis more integrated with the patient,we will have greater ability to filter theinformation to give the doctors whatthey want. It’s a much more integratedproduct compared to what we havecurrently.”Because of the collaborative nature ofthe <strong>Siemens</strong>/Denver Health partnership,solutions found at Denver Health mayalso help other institutions as they set60 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Medication Managementup their own CPOE process. “Our partnershipwith <strong>Siemens</strong> has allowed us totest a process to convert CPOE ordersets from INVISION to Soarian, whichwill provide a template that can be usedby other sites as they transition fromINVISION to Soarian,” says Steele. “Thereis now a tool set in development thatcan help smooth the transition.”American Recovery andReinvestment ActThe acceptance of CPOE in the U.S. hasbeen relatively slow for reasons such ascost, the need for HIT infrastructure, andphysician buy-in. Following last year’sdebut of the American Recovery andReinvestment Act (ARRA), stimulus fundingcould be the key to widespread CPOEuse. According to legislation, incentivefunds will be provided to U.S. hospitalsthat achieve “meaningful use” of CPOE“A clearly legible,electronic orderresults in fewercallbacks forclarification.”Andrew Steele, MD,Director of Medical Informatics,Denver Health and Hospital Authority,Denver, Colorado, USAtechnology by 2011. With Denver Health’sapplication of the CPOE process as ablueprint for success, <strong>Siemens</strong> standsready to provide hospitals with the HITplatforms needed to receive ARRA funding.“ARRA has drawn a line in the sand,”explains Steele. “It is no longer a decisionof what should we do about this, butan argument of when and how to bestleverage the technology. The longer youwait, the higher the bar is set. Right now,for early adopters, the bar is lower than,say, in five years, when the standards formeaningful use might be higher.”For those hospital systems gearing up tomeet the ARRA guidelines by applyingthe CPOE process, Steele has two piecesof advice: “One of the major lessons wehave learned at Denver Health is thateven though you need the HIT departmentto support the project, ultimatelyit needs to be turned over to and run bythe clinical department. The second lessonis not to think about it as launchinga CPOE technology program, but to seeit as an opportunity to really readdressand transform the care you are providing,”he says.With the implementation of CPOE adecade ago, Denver Health, supportedby <strong>Siemens</strong> technologies, is a leadingexample of the success of integratedclinical care. “The real power of CPOE isthat it can combine the electronic orderprocess and barcoding with evidencebasedbest practices to promote the highestquality and most effective care,” saysSteele. “As we move forward, I envisionthat people will start sharing their ordersets and their best practices for certainconditions, and this could evolve into ahigher level of standardized care for allpatients across the country.”Amy Erickson Vaughan is a journalist basedin Chicago, Illinois. She has traveled throughoutthe USA covering a wide variety of health andmedical topics. Her work has been publishedin numerous magazines, including CURE andNature Medicine.1The outcomes achieved by the <strong>Siemens</strong> customersdescribed herein were achieved in the customer’s uniquesetting. Since there is no “typical” hospital and manyvariables exist (e.g., hospital size, case mix, level of ITadoption) there can be no guarantee that others willachieve the same results.SummaryChallenge:• Provide timely, efficient, accurate, andstandardized treatment and therapy• Support an integrated approach toclinical patient care• Installation of CPOE with 100 percentadoption by clinicians• Support the organization’s patientsafety initiatives while offering costeffectivecareSolution:• The <strong>Siemens</strong> Soarian platform, whichis designed to help physicians, nurses,and pharmacists improve efficiencyand accuracy• The CPOE process, which can reducethe human element in medicationerrors, standardize care, and providelegible physician orders• Barcoding and CPOE, which createsa closed-loop medication process thatconfirms that the right drug is givenin the right dose at the right time tothe right patient via the right route• <strong>Siemens</strong> HIT systems, which are amongthe best platforms for implementingCPOE to receive ARRA fundingResult:• Ninety-five percent of orders(250,000 orders per month) generatedvia the CPOE process at Denver Health• A complete view of the patient’s information,promoting continuity of carethrough the entire course of treatmentand helping the organization ensurethat healthcare is delivered in the mostcost-effective setting• After CPOE implementation, DenverHealth reports an 83-percent reductionin time between medication orderand administration, a 55-percentreduction in laboratory turnaroundtime, and a 62-percent reduction inradiology turnaround time 1• Clearly legible, unambiguous physicianorders that do not require additionalinterpretation or callbacks for clarificationMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 61
Intraoperative ImagingBetter than Good: 3D Scans in the ORMany instances of malpositioning might go unnoticed ifonly two-dimensional images are used during surgery to checkwhether a complicated bone fracture was aligned and fixedproperly. They can only be seen when the reconstructedanatomy is represented spatially.By Hildegard Kaulen, PhD62 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Intraoperative ImagingWith 20,000 operations performed eachyear, the BG Trauma Hospital Ludwigshafen(Berufsgenossenschaftliche UnfallklinikLudwigshafen) is one of Germany’slargest trauma centers. Nearly half ofthose operations are performed withinthe Clinic for Trauma Surgery and Orthopedics,which is headed by ProfessorPaul A. Grützner, MD. The unit has workedwith three-dimensional (3D) intraoperativeimaging since 2001. The experiencegathered by Grützner and his team showsthat wherever the correct alignment ofcomplex osteosynthesis is inspectedusing only two-dimensional (2D) images,malpositioning cannot be avoided. Somearticular surfaces and improperly placedfixations can only be seen in 3D images.Many of these errors should actually becorrected in revision surgery, but thatisn’t always done because the healthstatus of the patient may not allow asecond surgery.Improper positioning is not rare. From2001 to 2009, Grützner and his colleaguestracked nearly 3,000 intraoperative 3Dscans, 1,841 of which were taken afterosteosynthesis. One in every five osteosynthesiscategorized as correct from 2Dimages had to be revised after an intraoperative3D scan. Corrections to theheel bone, the upper ankle joint, and thearticulation between the tibia and theankle joint were necessary. “Whereverwe see complex anatomy, where variousjoint facets have to be rejoined together,2D images without any spatial depth –and with the overlays of other anatomicalstructures – are not meaningful enoughto be able to assess the reposition ofa complicated fracture with sufficientcertainty,” Grützner says. “Our figuresshow that with the heel bone, almosthalf of the intraoperative 3D scans performedled to the correction of osteosynthesis;and the figure was almost athird for the upper ankle joint. These areMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 63
Intraoperative ImagingIntraoperative 3D imaging helps prevent revision surgery.not fringe phenomena, but relevantclinical numbers. That’s why we considerintraoperative 3D imaging to be so important.For many indications, we no longerdo without it.”Experience not a Substitute for3D ScanThe eight-year data collected by Grütznerand his colleagues also show that thenumber of revisions performed duringsurgery itself did not decrease after theintroduction of the 3D scan. This figure,therefore, does not depend on the surgeon’slevel of experience, but rather onthe fact that the 2D images simply donot picture complex anatomy correctly.Grützner says, “I can’t say it clearlyenough: Experience is no substitute for a3D scan. If anything, it is the experiencedsurgeons, in particular, who do not wantto do without this intra-operative processcontrol. They know very well that byusing this method, they achieve betterclinical outcomes and prevent postoperativerevisions. It is more often the young,inexperienced surgeons who think theycan get by without a 3D scan now andthen.”The team at the facility in Ludwigshafenworks with two generations of imagingunits: SIREMOBIL® Iso-C 3D , installed in2001, which was joined in 2005 by itssuccessor model, ARCADIS® Orbic 3D.Both units have a mobile C-arm with afixed iso-center and supply computedtomography-(CT-)likeimages. In bothunits, the middle of the connecting linebetween the radiation source and camerais always focused on one point – theisocenter – during the 190-degree turn.During orbital rotation, 50 or 100 imagesare taken at fixed angle increments.These individual images are then usedto create a cube-shaped volume of datawith a length of twelve centimeters to aside. The 3D reconstruction is presentedto the surgeon in real time, togetherwith the 2D X-ray images, which take theform of a film sequence. Surgery onlyhas to be interrupted for a few minutesfor this process. Grützner and his colleaguesuse intraoperative 3D scanningespecially where complex joint surfaceshave to be aligned; such as in the case ofthe upper ankle joint, the spinal column,and the pelvic ring; but also during surgery,where there is little tolerance forosteosynthesis, such as those involvingthe cervical spine. The 3D scanningmethod is not suitable for checking jointreplacements, because large amounts ofmetal in the field of view lead to imagingartifacts.To Grützner and his colleagues, there isno question about it: intraoperative 3Dimaging prevents postoperative revisions.There are, however, no numbers regardinghow many of the osteosynthesiscases that are categorized as correct from2D images, but are in fact improperlyplaced and have to be corrected later.Grützner avoids these kinds of postoperativerevisions by correcting malalignmentsright away during the surgery itself.He views a prospective randomizedstudy to compare 2D and 3D imaging asunethical because it is clear that 3D64 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Intraoperative Imaging115–145°Non-Isocentricity• The central beam moves out of the isocenter, making repositioningnecessary. Repositioning of the C-arm is time-consuming and can leadto additional radiation exposure.• The distance between the image intensifier or X-ray tube and thebody region being imaged varies with each change of the orbital angle.The image size thus varies for different projections.• The orbital movement is restricted to 25 to 55 degrees of ’overscan’,depending on the C-arm model and manufacturer.190°Isocentricity• The central beam always remains in the isocenter, which eliminates theneed for repositioning and enables both time and dose savings.• The distance between the image intensifier or X-ray tube and the bodyregion being imaged always remains the same, thus ensuring a constantimage size with varying projections.• Large orbital rotation of up to 190 degrees (+95°/-95°).• Prerequisite for 3D imaging via orbital movement.intraoperative imaging leads to betterclinical outcomes. It is unacceptable towithhold this better quality of treatmentfrom patients.Faster Decision-makingin the ORThe 3D scanning method has even moreadvantages. Because the 3D images areavailable quickly in high quality, decisionsin the OR can also be made more quickly.And that has a direct effect on the risk ofinfection, because a patient who undergoesa longer operation is at greater riskof contracting a wound infection than onewho undergoes just a short one. Grütznersays, “Infections involving osteosynthesisof calcaneal fractures used to be a realproblem. Because we are now able tomake faster decisions, with greater certaintyregarding the quality of the repositioning,we have cut the infection ratefor these operations to zero. That’s a bigaccomplishment.” To evaluate the 3Dscans, Grützner and one of his leadingsurgeons, Bernd Vock, MD, have developeda standardized procedure. A crucialpart of this is that images taken duringsurgery should correspond to thoseknown from CT. This enables surgeons3D Scans taken after osteosynthesisNo. of CasesIntraoperative revisions done after 3D ScansNo. of CasesCalcaneusAnkle jointTibial headDistal radiusLumbar spineThoracic spinePilonCervical spineAcetabulumTalusTarsusPelvic girdleOthers9.07.67.06.76.25.53.32.72.04.613.211.620.5Values inPercentage37724321316614012912411510260503785CalcaneusAnkle jointPilonTibial headAcetabulumTalusDistal radiusTarsusSpine9.414.713.312.012.018.830.929.040.3Values inPercentage152753640158206360 5 10 15 20 2518410 10 20 30 40 50388Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine 65
SummaryProfessor Paul Alfred Grützner, MD, studied at the Universities of Mainz,Germany, and Edinburgh, UK. He specializes in trauma surgery and orthopedics,with additional training in emergency medicine and physical therapy. He didhis postdoctoral work to qualify as a professor in the field of trauma surgery andhas worked at the City Hospital of Worms, the BG Trauma Hospital Ludwigshafen,and the Stuttgart Hospital (Katharinenhospital). Since 2009, he has beenthe Medical Director at the BG Trauma Hospital Ludwigshafen and the headphysician at the facility’s Clinic for Trauma Surgery and Orthopedics. Grütznerteaches surgery at the University of Heidelberg and performs various roles inGerman and international industry associations. He also serves as an experton the mediation committee of the state board of physicians.to get their bearings quickly, from aspatial point of view, and lets them comparethe 3D scan with the CT imagestaken before surgery. Other, less typicalsettings are also possible.Intraoperative imaging is also a high priorityin minimally invasive surgery, suchas percutaneous screw fixation for bonefractures. In these types of operations,the soft tissue is protected, but the actualsite of the operation is barely visible dueto the narrow approach. This means thatminimally invasive surgery is prone to malpositioning.Therefore, intraoperative 3Dscanning is an important process controlfor minimally invasive surgery, Grütznersays. It is also important in computerassistednavigation. Of the nearly 3,000scans the team at the Ludwigshafenfacility has evaluated over the eight-yearperiod, 14 percent served navigationpurposes. The 3D scans can be useddirectly for navigation, where they thenreplace the CT images taken before theoperation and eliminate the search forlandmarks.In Germany, the public health insurersdo not provide separate reimbursementfor intraoperative 3D imaging. Hospitalsonly receive a case-based lump-sumpayment for the operation. “The betterquality of the outcomes that we achievewithout any doubt with the 3D scans isnot reflected in the reimbursement ofcosts. Nonetheless, we have no intentionof doing without it anymore,” Grütznersays. “We do not want to withhold thatbetter outcome quality from the patients.Because we no longer have to performpostoperative control examinations, andbecause postoperative revisions are alsono longer necessary, intraoperative 3Dimaging is justified, even with heavy costpressure.”Hildegard Kaulen, PhD, is a molecular biologist.After positions at Rockefeller University in NewYork and the Harvard Medical School in Boston,Massachusetts, USA, she has worked since themid-1990s as a freelance science journalist forleading newspapers and scientific journals.Challenge:• When relying on just 2D images in theoperating room while aligning complexfractures, one in every five operationswill end in a malpositioning that cannotbe seen in the 2D images• Experience is not a substitute for a 3Dscan. The fact that the revision ratefollowing 3D scanning remains constantover time has to do with the 2Dimages inadequately reflecting complexanatomy• Germany’s public health insurers donot acknowledge the better outcomeof operations following intraoperative3D scanning with a higher case-basedlump sumSolution:• Intraoperative 3D scanning reducesthe number of postoperative revisionsin the case of complex bone fractures• In 40 percent of all fractures of theheel bone and one-third of fracturesof the upper ankle joint, the 3D scanningmethod leads to correction ofrepositions found to be in order in 2Dimages• Intraoperative 3D scanning is a highpriority in minimally invasive surgery,where surgeons have a limited view ofthe site of the operation, and in computer-assistednavigation. The 3Ddataset can be used directly for navigationpurposes, without the needfor surgeons to look for landmarks fororientationResult:• Corrections initiated while the operationis still in progress lead to bettertreatment outcomes• Because intraoperative 3D scanningleads to fewer follow-up examinationsand surgical interventions, it is justifiedeven where there is heavy cost pressure• For many indications, intraoperative3D imaging is the clinical standardFurther Informationwww.siemens.com/surgery66 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
TopicThe Diagnosticum Ingolstadt is a bright, spacious, and modern radiology center.All from One SourceAt the new Medical Center at Ingolstadt Hospital, all specializations, fromdentistry to ophthalmology, can be found under one roof. It is also hometo the Diagnosticum, a state-of-the-art radiology practice equipped withthe latest systems from <strong>Siemens</strong>. The flexible financing options offered by<strong>Siemens</strong> Finance & Leasing helped make these purchases possible.By Felix SparkuhleMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 67
Financing SolutionsBefore moving into the new Medical Centerin 2009, the Diagnosticum had twolocations in Ingolstadt, Germany – inthe old Medical Center and in IngolstadtHospital itself. “This was associatedwith tremendous logistical and financialcosts. At that time, we also expandedour team of physicians from six radiologiststo eight and were already lookingfor premises for our practice for thisreason,” recalls Rudolf Conrad, MD, ManagingPartner at the Diagnosticum.Once hospital management had notifiedthe partners at the Diagnosticum ofthe plans for the construction project, itdidn’t take long for the practice’s physiciansto decide in favor of a site in thenew complex and thus, in favor of intensifyingthe cooperation that alreadyexisted between their practice and thehospital. It was clear to the radiologiststhat, in the context of the relocationand upgrading of their equipment, newmedical equipment should be purchasedas well. Their interest turned to productsfrom <strong>Siemens</strong> <strong>Healthcare</strong>. Plans weremade to use the 3 Tesla (3T) magneticresonance imaging (MRI) systemMAGNETOM® Verio and the fully digitalX-ray system AXIOM® Aristos MX in thefuture. Not long afterward, however, thequestion came up as to how to financethe systems. After all, the costly move andthe new equipment had already causedsignificant financial strain.“Pay as You Earn” – SituationalFinancingIn this difficult financial situation, a flexible,customized solution was needed.And that is just what <strong>Siemens</strong> Finance& Leasing (SF&L), the German leasingsubsidiary of <strong>Siemens</strong> Financial Services,put together for the partners in the Diagnosticumin the form of a situational,demand-based financing package. Nodown-payment was required, and a threemonthstart-up period with no installmentpayments helped the radiology practiceconserve liquidity during the relocationand the initial phase in the new site.Another three months of particularly lowinstallment payments followed. Basedon the “Tech-X-Change” and “med-Dr. Rudolf Conrad is one of three partners of the practice.prodynamic” financing models, <strong>Siemens</strong>was able to put a progressive installmentpayment structure into place, followingthe “pay-as-you-earn” principle.“In addition to the technical and qualityfactors, the financing service was definitelyan important positive aspect thathelped us choose <strong>Siemens</strong>. And our regularbank was also happy to not haveto provide us with even more financing,especially because they had a hard timeassessing the risk involved in these kindsof investments,” Conrad says.In addition to a digital full-field X-raysystem with substantially lower radiationexposure for patients, Conrad and hiscolleagues are now one of the first teamsof physicians in the region to have a 3TMRI system.Completely New OptionsAlthough the premises of the Diagnosticumare located between a pharmacyand a dialysis ward, the installation ofthe high-field unit from <strong>Siemens</strong> waspossible without problem. The new MRIsystem at the radiology practice supplementsthe examination methods atIngolstadt Hospital and opens up completelynew options for the radiologists– and their patients. “For instance, whenit comes to stroke diagnosis, we havegotten faster and, with new features formeasuring perfusion, we are now evenmore precise. This is crucially importantwhen it comes to treatment. When weacquire angiograms with the 3T MRIsystem, even without the use of contrastagents, we are able to achieve images ata level of sharpness and detail that wehave never been able to achieve before.We often also examine patients’ hands,and these high-resolution systems helpus obtain sharp, detailed images of themany small bones and ligaments,” Conradexplains.When it comes to preventive examinations,cutting-edge <strong>Siemens</strong>’ medicaltechnology is also enabling the physiciansin Ingolstadt to break new ground.Starting this year, the physicians at theDiagnosticum will also be offering magneticresonance spectroscopy (MRS)of the prostate. The Prostate Center atIngolstadt Hospital has already indicatedan interest in cooperating closely withthe Diagnosticum in this area. And thatmeans outstanding preventive cancercare for men – in line with the practice’smotto, “Committed to the patient.” Thephysicians have officially been committedto this motto for five years now, and68 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Financing SolutionsLatest digital X-ray equipment ...and the 3 Tesla MRI are the highlights of the practice.it is backed by a certificate in qualitymanagement from the German TÜV testingand validation agency.Enhanced Patient Comfort andMore Efficient WorkflowsIn addition to new diagnostic possibilities,the purchases also have positiveimpact on patient comfort and a helpfuleffect on workflow.The cramped, narrow bores of manyMRI systems used to cause a problem formany patients, especially those withclaustrophobia. With a diameter of 70centimeters (27.6 inches), MAGNETOMVerio opens up MRI for a wider rangeof patients. And if the system, which isrelatively short, is also installed in a spaciousexamination room such as that atthe Diagnosticum, patients have a morepleasant experience. Conrad confirmsthat since the Diagnosticum purchasedMAGNETOM Verio, it has had no furtherissues with claustrophobic patients fearingMRI scans. It also facilitates scanningchildren, because the large opening letsparents hold a child’s hand during theimaging process. And the wide gantryeven lets physicians treat obese patients,up to a body weight of 250 kilograms(approximately 550 pounds), with ease.Furthermore, the shorter scan timesoffered by MAGNETOM Verio make it possibleto scan more patients in the sametimeframe. At the Diagnosticum, physiciansplan to use the time freed up bythe new unit to improve their service byestablishing open periods so that theycan react more flexibly to emergencies.As for workflow, the usability of the ITsystems was another crucial factor forConrad and his team. The physicians havebeen working with <strong>Siemens</strong> systems intheir practices since 1992. The latest purchasesfor the Ingolstadt facility also featurethe current syngo® software, whichis already familiar to the staff. “When wemoved, it was not just the flexible financingservice, but also the established ITsystems that helped us to save on costs.A new user interface would have requiredretraining all 16 of our radiology assistants.In this way, we were able to upgradeour equipment without tremendousexpense or risk.”Felix Sparkuhle has a degree in politicalscience with political economics. He works for<strong>Siemens</strong> Corporate Communications andGovernment Affairs.SummaryChallenge:• Cutting-edge technology is animportant unique selling point whencompeting with other providers• Time and cost pressures in radiology• Pressure to modernize equipmentSolution:• SF&L financing makes it possible touse the latest in <strong>Siemens</strong> technology• Flexible installment payment structures• Pay as you earnResult:• Latest technology• Enhanced image quality, better detail• Liquidity secured during the start-upphase• Shorter waiting times for patients• Greater flexibility in appointmentmanagement• High levels of patient comfortFurther Informationwww.siemens.com/sfsMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 69
Essay Series: <strong>Healthcare</strong> Systems – Germany<strong>Healthcare</strong> in Germany:Great Leeway for MajorPlayersby Jürgen Wasem, Alfred Krupp von Bohlen und Halbach Foundation Endowed Chair for Medicine Management,University of Duisburg-Essen, Germany“Reform is dead. Long live reform.” It is asentiment heard time and again throughoutthe German healthcare sector. Afterall, the past 35 years have seen the countryenact six sweeping reform packagesand an array of smaller ones. The newgovernment majority under ChancellorAngela Merkel that emerged in the lastparliamentary elections in September2009 announced in its coalition agreementthat it planned to enact anotherhealthcare reform, this one scheduled totake effect in 2011.Financial Development as aDriver of <strong>Healthcare</strong> ReformIn my opinion, a reform of the financingstructure of Germany’s statutory healthinsurance system is urgently needed. Thenew federal government intends on addingcontributions that are independentof income levels (flat per-capita contributions)to the existing system of incomedependentcontributions. A model thatcombines these two kinds of contributionsis in place in some other countries,such as the Netherlands. I consider this asensible step. It will help ensure that thehealthcare system is financed more sustainably.If enacted, however, a form ofsocial compensation would be needed,financed through taxes, for insured partieswith low incomes. Because the governmentis also determined to cut its incomefrom taxes via a major tax overhaul, it isentirely possible that we will lack the taxrevenue needed to pay for this socialcompensation. I therefore believe ourpolicymakers will need to choose betweentax reform and reforming the financingof our healthcare sector.There is a contentious debate regardingwhether our high healthcare expendituresyield proportionate benefits. Accordingto various international studies (such asthe OECD Health Care Quality IndicatorsProject or the measurements taken underthe European Union’s Open Method ofCoordination), the German healthcaresector’s outcome is only moderate. Thecouncil of healthcare experts convenedby the federal government has foundthat overtreatment, undertreatment,and provision of wrong or inappropriatehealthcare services are widespread.Patient satisfaction, on the other hand,is generally high, and waiting times aremostly short.Do the Benefits Outweighthe Costs?I am convinced that the sharp dividingline between outpatient and inpatientcare is one of the reasons for the comparativelyunfavorable cost-benefit curve.Hospitals are permitted to provide outpatienttreatment only within very narrowlimits. Instead, this is reserved forphysicians in private practice, even whenspecialist care is needed. Since 2004,medical care centers have also been permittedto participate in outpatient care.Such centers are being built by hospitals,for example. I believe we need to reconsiderthe division of labor between hospitalsand physicians in private practice.Looking at the international landscape,the role taken by the German governmentin controlling and directing the course ofthe healthcare sector is rather modest.That means that the major players in thehealthcare sector traditionally enjoy tremendouslatitude. The central body inthis regard is the Federal Joint Committee,whose membership is made up of representativesfrom health insurance companies,physicians, dentists, and hospitals.Patients’ representatives have the rightto attend and speak at its meetings, buthave no voting rights.The central task of the Federal JointCommittee is to specify the catalog ofservices approved and paid for underthe statutory health insurance system.Physicians can therefore use new methodsof outpatient diagnosis or new treatmentmethods only on the condition thatthey are approved by the Federal JointCommittee as medical services providedunder statutory health insurance. As aresult, it is possible to assess the benefitsand cost-benefit ratio of specific therapies.Physicians also receive informationon how to prescribe medications for maximumeconomic efficiency. The decisionsmade by the Federal Joint Committeeare central in terms of quality assuranceas well. For example, it sets the minimumquantity standards for operations.A Stronger Role for HealthInsurersSince the beginning of 2009, insuredparties and employers have been payingtheir contributions to a newly establishedcentral health fund (see Fig. 3).The health fund distributes moneys to theContinued on page 7470 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Essay Series: <strong>Healthcare</strong> Systems – GermanyMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 71
Essay Series: <strong>Healthcare</strong> Systems – GermanyFacts & Figures<strong>Healthcare</strong> ExpendituresGermany is one of the countries with the highest level of healthexpenditures expressed as a portion of GDP, after the UnitedStates, Switzerland, and France. In terms of per-capita spending,Germany ranked near the top among OECD countries in2006 at US$3,371 (measured at purchasing power parity).Contribution RatesAs Fig. 2 (see opposite page) shows, the percentage of GDPconsisting of healthcare spending has also risen sharply, from5.7 percent in 1970 to 10.4 percent in 2007. The rising contributionrates charged by health insurers are also attributableto the fact that incomes subject to mandatory contributions(particularly employee wages) have grown slower than GDP.Fig. 1: Average contribution rate charged by health insurers(as % of income) 116151413121110981970 1975 1980 1985 1990 1995 2000 2005Statutory Health InsurersThe development of contribution rates under the statutory healthinsurance system regularly drives healthcare reform cycles inGermany. Nearly 90 percent of the population is covered byapproximately 170 statutory health insurers. The statutory healthinsurance system collects income-based contributions to financethe costs of care. As Fig. 1 shows, the average contributionrate for health insurers has risen from eight percent in 1970 tomore than 15 percent in 2009, in spite of the many healthcarereforms enacted during that period.Private SubscribersThe German Health Insurance Act permits employees witha high income (the threshold for 2010 is €49,950), the selfemployed,and civil servants to decide whether they wish tobelong to a statutory health insurance plan or would ratherobtain insurance from a private health insurer. As a result,about ten percent of the population has private coverage.<strong>Healthcare</strong> Policy in Recent DecadesTo curb spending in the healthcare sector, healthcare policyover the past three decades has tended to favor health insurersover the providers of healthcare services. One of the very firststeps was to call on health insurers to act more consistentlyand uniformly, and there was a substantial push to centralizedecision-making authority. At the federal level, an industryassociation of health insurance companies was established.Its responsibilities include establishing fixed prices for pharmaceuticalsand medical aids, with its decisions binding forall health insurers. This association works together with thegroup that represents the interests of physicians in privatepractice, the National Association of Statutory Health InsurancePhysicians, to establish the required fee schedule and therules capping physician compensation. The association alsoworks with the German Hospital Federation to decide on thelump-sum payment system (German Diagnosis-Related Groups),which is also binding for all health insurers.Competition Among Health InsurersThe German legislative branch has consistently and deliberatelyencouraged competition among health insurers. Since 1997,all insured parties generally have the right to change healthinsurers. About five percent of insured parties do so each year– a significant enough figure to put pressure on insurancecompany managers to compete. The major competitive parameterfor health insurance companies in the past was the contributionrate: Insured parties and their employers paid contributionsdirectly to the health insurers, which had to calculatecontribution rates to be sufficient to cover their own costs.1Source: German Federal Ministry of Health76 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Essay Series: <strong>Healthcare</strong> Systems – Germany$$$$$$ $ $General Government Expenditure on Health as %of Total Expenditure on Health: 76.6 (2006)Population in Thousands: 82,641 (2006)12,010,08,06,04,02,00,0Fig. 2: Total expenditure on health as % of GDP 219701975 1980 1985 1990 1995 2000 2005Per Capita Total Expenditure on Health:US$3,669 (2006)2Source: German Federal Statistical Office.All other data: WHO Statistical Information System (WHOSIS),http://www.who.int/whosis/en;last accessed February 5th, 2010.Number of Hospital Beds per 10,000Resident Population: 83 (2006)Number of Dentists per 10,000Resident Population: 8 (2006)Number of Physicians per 10,000Resident Population: 34 (2006)Number of Nurses per 10,000Resident Population: 80 (2005)80Male Life Expectancy at Birth in Years: 777782Female Life Expectancy at Birth in Years: 82
Essay Series: <strong>Healthcare</strong> Systems – Germanyhealth insurance companies accordingto the risk structure of their insured parties.If the health insurers cannot covertheir expenses with these allocations,they have to charge the insured an additionalcontribution. On the other hand,they can provide the insured with a reimbursementif the amount they are allocatedby the fund turns out to be greaterthan their needs. The amount of thisadditional contribution is developing intoa major competitive factor. While thebasic contribution to the health fund ispaid in about equal portions by theemployer and the insured, the insuredparty alone pays the additional contribution.The additional contribution to the healthinsurance company, like the basic contributionrate, depends largely on the healthinsurer’s expenditures. The individualhealth insurance companies have recentlybeen given an increasing number oftools for managing their expenses. Forexample, individual health insurers cansign discount agreements with pharmaceuticalcompanies, giving the drug companypreferential supplier status withtheir insured parties in return. The insurancecompanies can also sign selectivecontracts with physicians’ networks orintegrated care providers. The effort tocurb expenses is at the heart of theseactions.Increasingly, however, the health insurersare coming to see these selectiveFig. 3: Flows of payment in the statutory health insurance systemGovernmentFederal subsidyIncome-dependentcontributionsEmployer, Pension Insurer, etc.agreements as an opportunity to maketheir own particular mark on the healthcaresector and thereby position themselvescompared to competitors.I believe it is necessary to encouragecompetition among health insurers withregard to the quality and economic efficiencyof care. This way, insured partiescan obtain health insurance coveragethat is in line with their preferences.A Two-class System ofMedicine?Private health insurers do not assessincome-dependent contributions. Instead,they calculate premiums according tothe individual risk levels for each subscriber.By taking out health insurance,young subscribers are saving toward theincreasing costs they will face as they age(“provisions for aging expenses”).By law, those with private health insur-Health FundStatutoryHealth InsurersAllocationsRemunerationIndividual additional contribution orpremium according to health insurerPremium-paying MembersServiceProvidersance pay higher prices to obtain servicesfrom physicians, hospitals, and pharmaciesthan those insured under the statutoryhealth insurance system. This hastriggered some debate regarding whetherthese patients are given preferentialmedical treatment, with others receiving“second-class” medicine. Empiricalevidence shows that privately insuredpatients receive appointments for medicalcare more quickly and are more frequentlygiven expensive new drugs. Thatleaves us with the question of whetherwe are moving increasingly toward thiskind of “two-class” medical system. Thus,I am firmly convinced that we urgentlyneed to reform the financing of the statutoryhealth insurance system.The opinions reflected in this article do not necessarilyreflect those of <strong>Siemens</strong> <strong>Healthcare</strong>.Jürgen Wasem studied Economicsand Political Science at PennsylvaniaState University, USA, the Universityof Sussex, UK, and the University ofCologne, Germany. After earning hisdoctorate, he became a consultantwith the German Federal Ministry ofHealth. After holding professorshipsat the University of Munich and theUniversity of Greifswald, he moved to the University ofDuisburg-Essen, where he has held the Alfred Krupp vonBohlen und Halbach Foundation Endowed Chair for MedicineManagement since 2003.Professor Wasem was the chairman of a commission ofexperts assembled by the German Federal Government onthe reform of premium calculations in the private healthinsurance sector; the legislature acted on the majorityof the commission’s findings. He is also the chairman ofthe federal board in charge of mediating disputes on feesbetween health insurers and physicians who provide outpatientcare, and the Chairman of the Academic AdvisoryCouncil of the Federal Social Insurance Office, which isresponsible for comparing risk structures between the healthinsurers. Professor Wasem also played a major role indeveloping a network of health technology assessment (HTA)task forces in Germany; his institute regularly performsHTAs and systematic reviews for the appropriate federalagencies. In his work, he also focuses on evaluations of thehealth and economic efficiency of medical products andpharmaceuticals.74 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Further ReadingFurther Reading<strong>Siemens</strong> offers a variety of customer magazines and informationchannels. “Further Reading“ introduces a selection of articlesand topics featured that may be of interest to you. To learn more,follow the link below each article. To subscribe to any of themagazines, see page 81.Small Dose for Small PatientsThe Arnold Palmer Medical Center with the Arnold Palmer Hospital for Children (left) and Winnie Palmer Hospital for Women & Babies (right)Arnold Palmer Hospital for Children in Orlando, Florida, USA,prides itself on providing advanced, specialized care for children.It comes as no surprise, then, that it was the first pediatric hospitalworldwide to purchase <strong>Siemens</strong>’ SOMATOM® DefinitionFlash computed tomography (CT) scanner, one of the fastestscanners with the lowest dose on the CT market. The systemcombines Dual Source technology with the fastest availablehardware component and innovative features, enabling thoracicscanning without breath holds and, in many cases, highqualityimages with doses of less than one millisievert (mSv).John Bozard, President of the Arnold Palmer Medical Center,remarks, “It is certainly going to give patients and their familiesa higher level of comfort about CT.”While reducing radiation exposure is important for all patients,pediatric patients in particular are more vulnerable to theadverse effects of ionizing radiation. This makes SOMATOMDefinition Flash an especially attractive choice for pediatrics.Joseph Foss, MD, Chair of Pediatric Radiology, adds, “Wereviewed all of the systems available, and the Definition Flashdefinitely provided the lowest dose possible for our patients,which was very important to us.”The requirement for breath holding during CT scans has alwaysbeen a challenge with pediatric patients and often resulted inthe need for sedation. SOMATOM Definition Flash’s speed caneliminate the need for breath holding and, therefore, result ina scan that is less burdensome and safer for patients. For thecomplete story about Arnold Palmer Medical Center’s scanneracquisition, please use the link below.www.siemens.com/SOMATOM-Sessions-lowdoseMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 75
Further ReadingKnowledge-based Automated Fetal Biometrics Usingsyngo Auto OB MeasurementsMeasuring fetal biometry has becomestandard practice in prenatal care to determinethe growth development and wellbeingof the fetus. Obtained manually,fetal measurements are time-consumingand highly user-dependent. In addition,due to the multitude of keystrokesrequired to perform each measurement,users are prone to develop repetitivestress injury (RSI). <strong>Siemens</strong> <strong>Healthcare</strong>has developed an application addressingthese issues. syngo® Auto OB measurementsautomate the manual process offetal biometry measurements saving upto 75 percent of the keystrokes in routinefetal exams and improving standardizationand reproducibility of results.Common fetal biometric measurementsinclude: biparietal diameter (BPD), headcircumference (HC), abdominal circumference(AC), femur length (FL), humeruslength (HL), and crown rump length (CRL).The American Institute of Ultrasoundin Medicine (AIUM) publishes guidelinesfor measuring these values. They helpdiagnose fetal pathology including growthrestriction, microcephaly, and macrosomia.In addition, they are utilized toestimate the gestational age (GA) of thefetus (i.e., length of pregnancy in weeksand days). Accurate estimation of GAis important to determine the expecteddelivery date, assess the fetal size, andmonitor fetal growth.The most common current workflowrequires expert users to perform biometricmeasurements manually. This paradigmyields several challenges, such as userdependency, time intensity, or RSI due tothe multiple keystrokes needed to performeach measurement. syngo Auto OBmeasurements are based on advancedstatistical pattern recognition technologyenabling rapid automated measurementof fetal biometrics to increase consistencyof results among users.Example of biparietal diameter measurementwith syngo Auto OBA whitepaper published by <strong>Siemens</strong>highlights the advantages of syngo AutoOB measurements and how it can beutilized to address the challenges of fetalbiometry. It can be accessed using thelink below.www.siemens.com/clinical-OBGYNE-prescribing: The Path to Physician Adoption of HITAdoption of health information technology(HIT) by physicians in the U.S. hasprogressed at a very slow pace. Admittedly,a recent confluence of developmentsin the specific HIT area of “e-prescribing”has opened the door for its widergeneral implementation. A whitepaperrecently published by <strong>Siemens</strong> focuses one-prescribing in the U.S. It summarizesvarious studies and lists the benefits thatare being realized by physicians who haveadopted either a full or basic system.Two factors contributing to the successof such efforts are the technical characteristicsof these solutions and the practicalworkflow benefits that e-prescribingtechnology delivers. In general, thesesolutions are easy to install, maintain,and use. The implementations are efficientfrom a time and resource standpointand do not, as a rule, disrupt thenormal physician workflow. On the con-trary, e-prescribing data and workflowenhancements address a set of readilyidentifiable pain points common to almostevery practice.These pain points include frequentmedication-related phone calls eitherfrom patients or pharmacies, excessivechart pulls, lack of satisfactory medicationhistory data, incomplete allergy anddrug interaction data, and cumbersomeformulary data access and management.By addressing these pain points with oneuser-friendly, relatively inexpensive solution,the chances for more widespreadadoption and subsequent ongoing useof e-prescribing are greatly enhanced.As a result, the healthcare system shouldsee broad adoption by physicians acrossthe practice spectrum.To download the full whitepaper, entitledE-Prescribing – The Path to PhysicianAdoption of HIT, please use the link below.www.siemens.com/e-prescribing76 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Further ReadingStep-by-step IT ImplementationBrookhaven Memorial Hospital MedicalCenter, a 306-bed, acute-care, non-forprofit,independent community hospitalin East Patchogue, Long Island, New York,USA, strives to provide leading-edgehealthcare solutions through a compassionateteam as well as technologicallyadvanced facilities. Serving a populationof more than 350,000, Brookhaven’s laboratorycurrently runs about 3.3 milliontests per year. This, coupled with thefacility’s focus on providing quality healthcarewith the leading technology, ledBrookhaven to adopt an IT initiative withthe help of <strong>Siemens</strong> and its comprehensiveportfolio of performance-drivenhealthcare IT products and solutions.In 2000, Brookhaven installed theNOVIUS® laboratory information system(LIS) to meet growing demands and providequality care by improving turnaroundtimes, delivering quicker clinical results,and expediting patient care. The LIS isconfigured to handle hematology, chemistry,urinalysis, coagulation, microbiologylab workflows, and reporting, aidingin workflow optimization and seamlessinteroperability between multiple labsettings. Joe Bak, Brookhaven’s LIS manager,appreciates its scalability, “It hasbeen able to grow with us to meet ourneeds and has given us great flexibilityin configuring the system, especiallywith reporting.”In 2007, Brookhaven deployed <strong>Siemens</strong>’Soarian® Clinicals, a complete hospitalinformation system (HIS) that helpsensure a seamless flow of informationwithin the hospital enterprise. The LISinfrastructure was further complementedin 2009 with the fully integrated WebbasedEasyLink Informatics System toimplement autoverification, managequality-control data, and optimize theperformance and productivity of the laboratory.By connecting the lab’s multipleinstruments to its LIS through EasyLink,Brookhaven can now consolidate patientdata management while at the same timegain greater control over its workflowand operational performance. “Now thatwe’ve gone to autoverification, we’veachieved a 19-percent improvement inSTAT turnaround times,” AdministrativeDirector Jim Carr says. “That’s one of thebiggest changes we’ve ever seen and it’ssignificant because our work predominantlycomes out of the ED [emergencydepartment].” To provide Brookhaventhe tools to quickly build interfaces andenable the exchange of complex information,<strong>Siemens</strong> suggested the implementationof OPENlink. This applicationindependentinterface engine can bridgelab, clinical, imaging, financial, administration,and other systems that requireonline data. This allows users to transferPatientDatadata between heterogeneous systemsand applications, even when they utilizedifferent communication standards andprotocols. Step-by-step, <strong>Siemens</strong> hashelped Brookhaven meet its objectiveswith solutions – NOVIUS Lab, SoarianClinicals, EasyLink, and OPENLink – thatimprove performance and productivityas well as connect every patient touchpointacross the care continuum. To readin more detail about the implementationsas well as Brook-haven’s future plansfor the initiative, use the link providedbelow, and click on “case studies.”www.siemens.com/diagnostics-itMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 77
Further ReadingJustifying the InvestmentMore than two years ago, the Instituteof Diagnostic Radiology at the UniversityHospital Zurich invested in two uniquesystems from the high end of <strong>Siemens</strong>’computed tomography (CT) scannerrange: Dual Source SOMATOM® Definitionand SOMATOM Definition AS. The institute’shead of radiology, Professor BorutMarincek, MD, justified the investmenton the basis of reduced dosage. “For thesake of our patients,” he says, “we willalways opt for the latest technology thatoffers the best results with the lowestpossible dosage.“ Now, after having timeto evaluate the new technology, <strong>Siemens</strong>’CT customer magazine, SOMATOMSessions, went back to the institute to askthe burning question: Was the investmentworthwhile?“Definitely,” answers Marincek’s colleague,Sebastian Leschka, MD. With the newscanners, the institute is not only loweringpatient exposures, it also is savingtime, money, and hassle in the day-todayworkflow as a result of the systems’high scanning speeds and optimizedworkflows. “They have provided significanteconomic benefits,” says Leschka,adding that the “next-next” generationscanner, the SOMATOM Definition Flash,promises to trump these improvementseven more. To read the entire storyregarding the hospital’s investments,including improvements in cardiac CTand thoracic scanning, use the link providedbelow.www.siemens.com/SOMATOM-Sessions-investmentWhole Blood Total BilirubinDetermination in NeonatesAbout 60 percent of newborn babiesdisplay mild jaundice (yellowing of theskin) within the first two days after birthdue to shortened lifespan of red bloodcells coupled with slow maturation ofliver glucuronyl transferase activity.Mild jaundice is usually not detrimental;however, some newborns develop severejaundice from high levels of unconjugatedbilirubin circulating in the blood.Nearly 60 percent of newborn babiesdisplay mild jaundice, which can be a resultof unconjugated bilirubin circulating in thebloodstream.If left untreated, unconjugated bilirubinmay deposit in the basal ganglia andbrainstem, causing irreversible neurologicdamage, a condition known askernicterus. Kernicterus can cause cerebralpalsy; problems with hearing, vision,and teeth; and mental retardation.Simple and noninvasive phototherapy isthe first approach to reduce high levelsof neonatal bilirubin. However, if phototherapydoes not lower the baby’s bilirubinblood levels, an exchange transfusionmay be required. Since untreatedhyperbilirubinemia may cause severepermanent health problems, all newbornsshould be checked for jaundice.The practice guidelines of the AmericanAcademy of Pediatrics include provisionsfor measurement of total bilirubin toevaluate the degree of jaundice and thenecessity for intervention.Because of the complication of collection,limited blood volume, and higher hematocrit,testing neonatal blood can bechallenging. Large reagent-based chemistryanalyzers require the separationof plasma from the red blood cells priorto analysis. Blood gas analyzers offer analternate method for assessing the riskof developing kernicterus using directmulti-wavelength spectrophotometry onsmall volumes of whole blood.<strong>Siemens</strong> <strong>Healthcare</strong> Diagnostics magazinePerspectives presents a neonatalwhole-blood total bilirubin performanceevaluation of two blood gas systems:the RAPIDLab® 1245 from <strong>Siemens</strong><strong>Healthcare</strong> Diagnostics compared to theRadiometer ABL 735, a member of theRadiometer ABL 700/800 family of systems.As demonstrated in the hospital settingusing diverse clinical specimens fromneonates, whole-blood total bilirubinanalysis on the <strong>Siemens</strong> RAPIDLab 1245blood gas analyzer is accurate and precisewhen compared to the RadiometerABL 735. Analysis of unhemolyzedwhole blood using the RAPIDLab 1245 orRAPIDLab 1265 is a clinically acceptablemethod for monitoring the developmentof pathologic concentrations of bilirubinin neonates. The full results for this newalternative for monitoring bilirubin innewborns can be accessed using the linkbelow.www.siemens.com/bili78 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Further Reading3D High-resolution MRI of the KneeMagnetic resonance imaging (MRI) of the knee is justifiablyone of the most commonly performed MRI examinations,as it offers excellent direct depiction of cartilage, ligaments,menisci, and periarticular soft tissue. This can be achieved bystandard application of fat-saturated moderately T2-weighted2D Turbo Spin Echo (TSE)-sequences in three orientations.However, conventional TSE-sequences are not isotropic, hencestructures and signal alterations/lesions with a size less thanthe usual slice thickness of three to six millimeters (mm), i.e.,meniscal roots, may not be completely detected. A slice thicknessbelow three mm is rarely acquired because of its reducedsignal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR)as well as the prolonged acquisition time for complete jointcoverage. Furthermore, postprocessing options are limitedfor 2D sequences for the assessment of structures which arecaptured in an oblique course through several slices, like theanterior cruciate ligament or the femoral trochlear cartilage.In this setting, the introduction of a highly resolved 3D moderatelyT2-weighted (3D-T2w-TSE) sequence may be useful. Inresearch, time-efficient 3D-T2w-TSE sequences have alreadybeen evaluated for the central nervous system and recently forthe body trunk. They enable data acquisition with high isotropicspatial resolution and allow for interactive three-dimensionalvisualization. Such postprocessing after an initial isotropicdata acquisition has been proven successful in many other MRIand computed tomography-based applications.The application syngo® SPACE, a 3D-TSE-sequence withmoderate T2-weighting standing for ’Sampling Perfectionwith Application optimized Contrasts using different flip angleEvolutions’ might establish a new approach to MRI for theknee. Parallel imaging facilitates blockwise 3D-data acquisitionwith isotropic spatial resolution for evaluation of the wholeknee in a reasonable time window. Radiologists at the UniversityHospital of Munich’s Department of Clinical Radiologyinvestigate the application of syngo SPACE for imaging the kneeand present their results, including shorter acquisition timesas compared to two-dimensional datasets, in a recent articlepublished in <strong>Siemens</strong>’ MRI customer magazine, MAGNETOMFlash. That article can be accessed using the link below.www.siemens.com/MAGNETOM-Flash-kneeAs compared to the T2w-2D-TSE-fs in 3 mm (far left), coronal syngo SPACE reconstructions in 0.5 mm (middle left), 1 mm (middle right),and 2 mm (far right) show good homogeneity throughout the image.Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine 79
Imprint© 2010 by <strong>Siemens</strong> AG, Berlin and Munich,All Rights ReservedPublisher:<strong>Siemens</strong> AG<strong>Healthcare</strong> SectorHenkestrasse 127, 91052 Erlangen, GermanyResponsible for Contents: act. Silke SchumannDirector of Customer Communications: Silke SchumannChief Editors: Sonja Fischer, Doris PischitzEditorial Team: Dorothee Degel, Annalisa Greger,Eva-Katharina Lang, Matthias Schwethelm, Abigail WeldonProduction: Norbert MoserAll at: Henkestrasse 127, 91052 Erlangen, GermanyPhone: +49 9131 84-7529, Fax: +49 9131 84-4411email: editor.medicalsolutions.healthcare@siemens.comDesign and Editorial Consulting:independent Medien-Design, Munich, Germanyin cooperation with Primafila AG, Zurich, SwitzerlandArt Direction: Horst MoserLayout: Lucie Schmid, Claudia Diem, Mathias FrischEditorial Coordination: Christa LöberbauerPhoto Editor: Susanne NipsAll at: Widenmayerstrasse 16, 80538 Munich,GermanyPrePress: Reinhold Weigert, Typographie und mehr ...Schornbaumstrasse 7, 91052 Erlangen, GermanyPrinter: Mediahaus Biering GmbH,Freisinger Landstrasse 21, 80939 Munich, GermanyPhoto Credits:Cover: Johanna EkmarkCover Story: Johanna Ekmark, Golden Section Graphics,Kurt Paulus, privateBreast Care: Beth Rooney/Aurora, Golden Section GraphicsAdvanced Visualization: Yohanne Lamoulére/Agentur Focus,<strong>Siemens</strong>Financing Solutions: Christian Höhn, <strong>Siemens</strong>Immunoassay: SPL/Agentur Focus, Jez Coulson/insight-visualSurgery: Eivind Natvig/Agentur FocusMRI in Orthopedics: Frank Bauer, privateHospital IT: <strong>Siemens</strong>Interventional Radiology: Kurt PaulusMolecular Imaging: Johannes KrömerTurnkey Solutions: Ivan Blazhev/Agentur AnzenbergerServices: Frank Schmitt/tm studiosMedication Management: Jez Coulson/insight-visualIntraoperative Imaging: Sven Paustian/Agentur FocusEssay Series: Orlando Illustration, privateThanks to the following experts from <strong>Siemens</strong> for providingtheir knowledge for the Cover Story: Carsten Bertram(Women’s Health); Sam Brandt (Hospital IT); Dr. Friedrich Fuchs(Cardiology); Dr. Christoph Gauer (Business); Dr. Oliver Heid(Innovations); David Hickey (General Laboratory); Dr. BerndHofmann (Neurology); Tom Miller (General); Eric Olson(Laboratory IT); Dr. Erhard Schnapka (Molecular Medicine);Marianne Vorbuchner (Oncology); Eleanor Kerr, Eugene Lee,Stefan Nardi-Hiebl, Heinrich von Wulfen (Reimbursement).Note in accordance with § 33 Para.1 of the German FederalData Protection Law: Dispatch is made using an addressfile which is maintained with the aid of an automated dataprocessing system.We remind our readers that when printed, X-ray films neverdisclose all the information content of the original. Artifacts inCT, MR, ultrasound, and DSA images are recognizable by theirtypical features and are generally distinguishable from existingpathology. As referenced below, healthcare practitioners areexpected to utilize their own learning, training, and expertisein evaluating images.Partial reproduction in printed form of individual contributionsis permitted, provided the customary bibliographicaldata, such as author’s name and title of the contribution aswell as date and pages of Medical Solutions, are named.The editors request that two copies be sent to their attention.The consent of the authors and editors is required for thecomplete reprint of an article. Manuscripts submitted withoutprior agreement as well as suggestions, proposals, and informationare always welcome; they will be carefully assessedand submitted to the editorial conference for attention.DISCLAIMERS: Practice of Medicine: “The information presented in this magazine is for illustration only and is not intendedto be relied upon by the reader for instruction as to the practice of medicine. <strong>Healthcare</strong> practitioners reading this informationare reminded that they must use their own learning, training, and expertise in dealing with their individual patients.This material does not substitute for that duty and is not intended by <strong>Siemens</strong> <strong>Healthcare</strong> to be used for any purpose in thatregard.“ Contrast Agents: “The drugs and doses mentioned herein are consistent with the approved labeling for uses and/orindications of the drug. The treating physician bears the sole responsibility for the diagnosis and treatment of patients, includingdrugs and doses prescribed in connection with such use. The Operating Instructions must always be strictly followed whenoperating your <strong>Siemens</strong> system. The source for the technical data is the corresponding data sheets.” Trademarks: “All trademarksmentioned in this document are property of their respective owners.“ Results: “The outcomes achieved by the <strong>Siemens</strong>customers described herein were achieved in the customer’s unique setting. Since there is no “typical” hospital and manyvariables exist (e.g., hospital size, case mix, level of IT adoption), there can be no guarantee that others will achieve the sameresults.”80 Medical Solutions · May 2010 · www.siemens.com/healthcare-magazine
Subscription<strong>Siemens</strong> <strong>Healthcare</strong> – Customer MagazinesOur customer magazine family offers the latest information and background for everyhealthcare field. From the hospital director to the radiological assistant – here, you canquickly find information relevant to your needs.Medical SolutionsInnovations and trendsin healthcare. Themagazine is designedespecially for membersof hospital management,administrationpersonnel, and headsof medical departments.eNewsRegister for the<strong>Siemens</strong> <strong>Healthcare</strong>global eNewsletteratwww.siemens.com/healthcare-eNewsto receive monthlyupdates on topicsthat interest you.AXIOM InnovationsEverything from the worldsof interventional radiology,cardiology, fluoroscopy,and radiography. This semiannualmagazine is primarilydesigned for physicians,physicists, researchers, andmedical technical personnel.MAGNETOM FlashEverything from the worldof magnetic resonanceimaging. The magazinepresents case reports,technology, product news,and how-to articles. It isprimarily designed forphysicians, physicists, andmedical technical personnel.SOMATOM SessionsEverything from the worldof computed tomography.With its innovations, clinicalapplications, and visions,this semiannual magazineis primarily designed forphysicians, physicists,researchers, and medicaltechnical personnel.PerspectivesEverything from the worldof clinical diagnostics. Thissemiannual publication providesclinical labs with diagnostictrends, technical innovations,and case studies.It is primarily designed forlaboratorians, clinicians, andmedical technical personnel.For current and older issues and to order the magazines, please visit www.siemens.com/healthcare-magazineMedical Solutions · May 2010 · www.siemens.com/healthcare-magazine 81
Global <strong>Siemens</strong> Headquarters<strong>Siemens</strong> AGWittelsbacherplatz 2D-80333 MunichGermanyGlobal <strong>Siemens</strong><strong>Healthcare</strong> Headquarters<strong>Siemens</strong> AG<strong>Healthcare</strong> SectorHenkestrasse 127D-91052 ErlangenGermanyTelephone: +49 9131 84-0www.siemens.com/healthcarewww.siemens.com/healthcare-magazineOrder No. A91CC-00038-M1-4A00 | Printed in Germany |CC 00038 ZS 05107. | ISSN 1614-2535 | © 05.10, <strong>Siemens</strong> AGOn account of certain regional limitations ofsales rights and service availability, we cannotguarantee that all products included in thisbrochure are available through the <strong>Siemens</strong>sales organization worldwide. Availability andpackaging may vary by country and is subjectto change without prior notice. Some/All ofthe features and products described herein maynot be available in the United States.The information in this document containsgeneral technical descriptions of specificationsand options as well as standard and optionalfeatures which do not always have to be presentin individual cases.<strong>Siemens</strong> reserves the right to modify the design,packaging, specifications, and options describedherein without prior notice.Please contact your local <strong>Siemens</strong> salesrepresentative for the most current information.Note: Any technical data contained in thisdocument may vary within defined tolerances.Original images always lose a certain amountof detail when reproduced.Local Contact InformationAsia/Pacific:<strong>Siemens</strong> Medical SolutionsAsia Pacific HeadquartersThe <strong>Siemens</strong> Center60 MacPherson RoadSingapore 348615Telephone: +65 9622-2026Canada:<strong>Siemens</strong> Canada Limited<strong>Healthcare</strong> Sector2185 Derry Road WestMississauga, ON L5N 7A6CanadaTelephone: +1 905 819-5800Europe/Africa/Middle East:<strong>Siemens</strong> AG, <strong>Healthcare</strong> SectorHenkestr. 127,91052 ErlangenGermanyTelephone: +49 9131 84-0Latin America:<strong>Siemens</strong> S.A., Medical SolutionsAvenida de Pte. Julio A. Roca No 516, Piso 7C1067ABN Buenos AiresArgentinaTelephone: +54 11 4340-8400USA:<strong>Siemens</strong> Medical Solutions USA, Inc.51 Valley Stream ParkwayMalvern, PA 19355-1406USATelephone: +1 888 826-9702
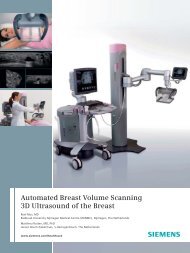
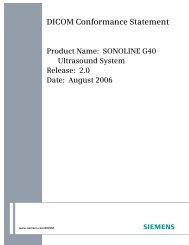


![WalkAway plus Technical Specifications [41 KB] - Siemens Healthcare](https://img.yumpu.com/51018135/1/190x253/walkaway-plus-technical-specifications-41-kb-siemens-healthcare.jpg?quality=85)