Incident reporting policy - Homerton University Hospital
Incident reporting policy - Homerton University Hospital Incident reporting policy - Homerton University Hospital
In cases where there may be legal implications for the Trust, the Risk Manager must forward a copy of thefinal report to the Legal Services Officer for safe-keeping as a `potential claim'.Copies of investigation reports must not be released outside the Trust until ratified by the Patient SafetyCommittee and then only with the permission of the Chief Nurse or the Medical Director.22.17 LiabilityThe Homerton University Hospital NHS Foundation Trust is vicariously liable for the acts/ omissions of itsemployees and so will take full responsibility in the event of legal action taken against the Trust which arisesfrom a Serious Untoward Incident.In situations where staff behaviour is considered to be malicious, criminal or gross professional misconductand/or where action is taken by the police or other external agency the Trust may not be vicariously liablefor the acts or omissions in question.23.0 Monitoring & Review of Incident Reporting & Investigation Policy23.1 This policy should be kept under review in the light of changing circumstances and requirements. As aminimum it should be reviewed routinely every three years. If there are significant changes this should bereturned to the ratifying body for approval.The processes for monitoring compliance with this procedure are outlined in the table below:Measurable Policy Objective Monitoring/Audit Frequency ofmonitoringReview of all incidents toinclude validation ofappropriate scoringLessons learnt sharedReport to IncidentReview GroupReview of allongoing andcompletedSerious Incidentand SeriousUntowardIncidentInvestigationsUpdatesThree times amonthMonthlyResponsibilityfor performingthe monitoringRiskManagementDepartmentRiskManagementDepartmentMonitoring reported to whichgroups/committees, incresponsibility for reviewingaction plansIncident Review GroupPatient Safety CommitteeClinical BoardRiskManagementNewsletterQuarterlyRiskManagementDepartmentTrust WideReview of ActionsIncident ReviewMeetingThree times amonthRiskManagementDepartmentIncident Review GroupQuality Audit of Datix RiskManagement SystemSummary Reportof ActionsOutstanding fromSIIs and SUIsIncidentReportingPerformanceMonthlyQuarterlyRiskManagementDepartmentRiskManagementDepartmentPatient Safety CommitteeIncident Reporting GroupPage 26 of 47
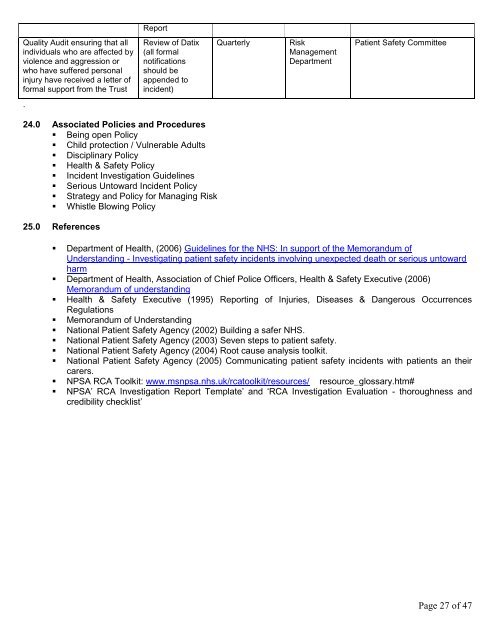
ReportQuality Audit ensuring that allindividuals who are affected byviolence and aggression orwho have suffered personalinjury have received a letter offormal support from the TrustReview of Datix(all formalnotificationsshould beappended toincident)QuarterlyRiskManagementDepartmentPatient Safety Committee.24.0 Associated Policies and Procedures• Being open Policy• Child protection / Vulnerable Adults• Disciplinary Policy• Health & Safety Policy• Incident Investigation Guidelines• Serious Untoward Incident Policy• Strategy and Policy for Managing Risk• Whistle Blowing Policy25.0 References• Department of Health, (2006) Guidelines for the NHS: In support of the Memorandum ofUnderstanding - Investigating patient safety incidents involving unexpected death or serious untowardharm• Department of Health, Association of Chief Police Officers, Health & Safety Executive (2006)Memorandum of understanding• Health & Safety Executive (1995) Reporting of Injuries, Diseases & Dangerous OccurrencesRegulations• Memorandum of Understanding• National Patient Safety Agency (2002) Building a safer NHS.• National Patient Safety Agency (2003) Seven steps to patient safety.• National Patient Safety Agency (2004) Root cause analysis toolkit.• National Patient Safety Agency (2005) Communicating patient safety incidents with patients an theircarers.• NPSA RCA Toolkit: www.msnpsa.nhs.uk/rcatoolkit/resources/ resource_glossary.htm#• NPSA‟ RCA Investigation Report Template‟ and „RCA Investigation Evaluation - thoroughness andcredibility checklist‟Page 27 of 47
- Page 3: 1.0 Version ControlVersion Date Aut
- Page 6 and 7: 6.0 Policy Definitions6.1 Adverse I
- Page 8 and 9: The person in charge at the time of
- Page 10 and 11: • Review sessions throughout the
- Page 12 and 13: They refer serious incident investi
- Page 14 and 15: Level of Incident Process Investiga
- Page 16 and 17: 17.3 Communication with StaffIt wil
- Page 18 and 19: Trust‟s Raising Concerns at Work
- Page 20 and 21: o action or lack of action by a mem
- Page 22 and 23: In the event of a suspected SUI it
- Page 24 and 25: managers determine how staff can be
- Page 28 and 29: Appendix 1: Incident Risk Assessmen
- Page 30 and 31: Table 2 Likelihood score (L)What is
- Page 32 and 33: Community• Unplanned homebirth•
- Page 34 and 35: Appendix 4: Reporting to External A
- Page 36 and 37: Appendix 5: Reportable injuries or
- Page 38 and 39: Appendix 6MEMORANDUM OF UNDERSTANDI
- Page 40 and 41: Appendix 8: Infection Control Serio
- Page 42 and 43: Appendix 10 - 24 Hour Meeting Agend
- Page 44 and 45: Equalities Impact AssessmentThis ch
- Page 46 and 47: Policy Submission FormPolicy Submis
ReportQuality Audit ensuring that allindividuals who are affected byviolence and aggression orwho have suffered personalinjury have received a letter offormal support from the TrustReview of Datix(all formalnotificationsshould beappended toincident)QuarterlyRiskManagementDepartmentPatient Safety Committee.24.0 Associated Policies and Procedures• Being open Policy• Child protection / Vulnerable Adults• Disciplinary Policy• Health & Safety Policy• <strong>Incident</strong> Investigation Guidelines• Serious Untoward <strong>Incident</strong> Policy• Strategy and Policy for Managing Risk• Whistle Blowing Policy25.0 References• Department of Health, (2006) Guidelines for the NHS: In support of the Memorandum ofUnderstanding - Investigating patient safety incidents involving unexpected death or serious untowardharm• Department of Health, Association of Chief Police Officers, Health & Safety Executive (2006)Memorandum of understanding• Health & Safety Executive (1995) Reporting of Injuries, Diseases & Dangerous OccurrencesRegulations• Memorandum of Understanding• National Patient Safety Agency (2002) Building a safer NHS.• National Patient Safety Agency (2003) Seven steps to patient safety.• National Patient Safety Agency (2004) Root cause analysis toolkit.• National Patient Safety Agency (2005) Communicating patient safety incidents with patients an theircarers.• NPSA RCA Toolkit: www.msnpsa.nhs.uk/rcatoolkit/resources/ resource_glossary.htm#• NPSA‟ RCA Investigation Report Template‟ and „RCA Investigation Evaluation - thoroughness andcredibility checklist‟Page 27 of 47


