

Y5 OSCE feedback from examiners Phase 1 Part 2 2010-11.
Y5 OSCE feedback from examiners Phase 1 Part 2 2010-11.
Y5 OSCE feedback from examiners Phase 1 Part 2 2010-11.
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
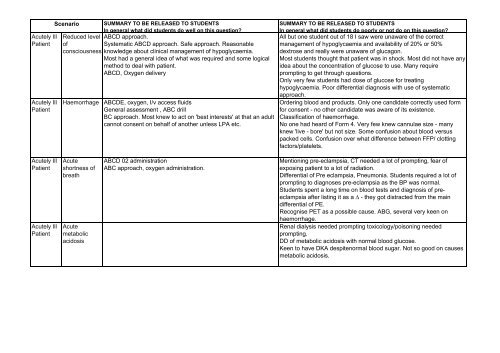
Acutely IllPatientAcutely IllPatientScenarioSUMMARY TO BE RELEASED TO STUDENTSIn general what did students do well on this question?Reduced level ABCD approach.ofSystematic ABCD approach. Safe approach. Reasonableconsciousness knowledge about clinical management of hypoglycaemia.Most had a general idea of what was required and some logicalmethod to deal with patient.ABCD, Oxygen deliveryHaemorrhage ABCDE, oxygen, I/v access fluidsGeneral assessment , ABC drillBC approach. Most knew to act on 'best interests' at that an adultcannot consent on behalf of another unless LPA etc.SUMMARY TO BE RELEASED TO STUDENTSIn general what did students do poorly or not do on this question?All but one student out of 18 I saw were unaware of the correctmanagement of hypoglycaemia and availability of 20% or 50%dextrose and really were unaware of glucagon.Most students thought that patient was in shock. Most did not have anyidea about the concentration of glucose to use. Many requireprompting to get through questions.Only very few students had dose of glucose for treatinghypoglycaemia. Poor differential diagnosis with use of systematicapproach.Ordering blood and products. Only one candidate correctly used formfor consent - no other candidate was aware of its existence.Classification of haemorrhage.No one had heard of Form 4. Very few knew cannulae size - manyknew 'live - bore' but not size. Some confusion about blood versuspacked cells. Confusion over what difference between FFP/ clottingfactors/platelets.Acutely IllPatientAcutely IllPatientAcuteshortness ofbreathAcutemetabolicacidosisABCD 02 administrationABC approach, oxygen administration.Mentioning pre-eclampsia, CT needed a lot of prompting, fear ofexposing patient to a lot of radiation.Differential of Pre eclampsia, Pneumonia. Students required a lot ofprompting to diagnoses pre-eclampsia as the BP was normal.Students spent a long time on blood tests and diagnosis of preeclampsiaafter listing it as a ∆ - they got distracted <strong>from</strong> the maindifferential of PE.Recognise PET as a possible cause. ABG, several very keen onhaemorrhage.Renal dialysis needed prompting toxicology/poisoning neededprompting.DD of metabolic acidosis with normal blood glucose.Keen to have DKA despitenormal blood sugar. Not so good on causesmetabolic acidosis.
PED History taking - Almost all took an adequate HX.various HX taking good, presentation good.scenarios General interview skills good or very good, most students eliciteda good history of preventing symptoms summary and differentialdiagnosis overall good. Most were familiar with growth charts andtheir interpretation.Gathered appropriate information.Generally good rapport with odd exceptions asked appropriatespecific questions relating to the symptoms. Good at summarisinghistory.Many students struggled with systematic paediatric history taking. I.e.after presenting illness, moving onto past medical HX/ Family HX.Birth/pre natal HX. Immigration. Development/growth/schoolSome students still in 'adult' mode.I expected them to be slicker on asthma history taking by now.Some students ran out of time for history taking.Development, FHX, differential diagnosis.History taking was often unsystematic. Family history, smoking history,communication history full medical history often forgotten or brief.Some students forgot to ask about obstetrics and birth history. Somestudents ran out of time.Often did not ask about social history school, milestones,immunisations even though there was sufficient time.Timing - most spent longer on history than allocated, and many movedback and forth in history.PED Patient exam -variossystems anddevelopmentassessment.General approach to child and parent good.Examined methodically.Good approach, good systematic exam, methodical,developmental exam much better than last year.General standard was fine. Good at Respiratory and abdomenexaminations.Most were systematic and followed a sequence well.Musculoskeletal examination not done as well as other systems. Notall students washed their hands.Sometimes tried to find signs even if not present.The overall standard of musculoskeletal examination was poorcompared with other systems. CVS variable.Not too good at observation before starting in with both hands.Approach to assessment for locomotor/ musculoskeletal case. It isclear which have seen pGALS video / teaching.Overall I was disappointed that very few managed to do the wholething well. Differential diagnosis poor. Much better at clinicalexamination.Older developmental assessment e.g. in 3 yr olds.Assessing speech development.PSYInfo aboutdiagnosis 1It is a good question to test communication and empathy, and Students found it really hard to convey prognosis, and overall, theremost did well, putting a worried mother at ease. They generally did was a really poor awareness of the genetic factors at play.ok on discussing what Schizophrenia is, but not so well on Some students struggled to explain prognosis of Schizophrenia andaetiology.unable to explain in a satisfactory manner whether the patient onNature and aetiology was explained well by most students. discharge would pose a risk to his sister. Most students forgot to offerwritten information (leaflets, websites etc) to the patient's mother.
PSYTreatmentinformation(Venlafaxine)Explaining about how drug works. Caution about not stoppingabruptly.Explanation of depression and antidepressants treatment andCBT.Very vague about what CBT is and how it works.Several students were uncertain if depression could run in families(have a genetic loading). One or two were unsure if the medicationneeded to be continued for 6 months <strong>from</strong> the time medication wasstarted vs. <strong>from</strong> the time patient improved.












