Risk factors for healthcare-associated urinary tract infection and their ...
Risk factors for healthcare-associated urinary tract infection and their ...
Risk factors for healthcare-associated urinary tract infection and their ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Journal of Hospital Infection 82 (2012) 219e226Available online at www.sciencedirect.comJournal of Hospital Infectionjournal homepage: www.elsevierhealth.com/journals/jhinReview<strong>Risk</strong> <strong>factors</strong> <strong>for</strong> <strong>healthcare</strong>-<strong>associated</strong> <strong>urinary</strong> <strong>tract</strong><strong>infection</strong> <strong>and</strong> <strong>their</strong> applications in surveillance usinghospital administrative data: a systematic reviewC. King a, *, L. Garcia Alvarez a , A. Holmes a, b , L. Moore c , T. Galletly b , P. Aylin a, da The National Centre <strong>for</strong> Infection Prevention <strong>and</strong> Management, Imperial College, London, UKb Infection Prevention <strong>and</strong> Control, Imperial College Healthcare NHS Trust, London, UKc Department of Infectious Diseases, Imperial College Healthcare NHS Trust, London, UKd Dr Foster Unit at Imperial, School of Public Health, Imperial College London, London, UKA R T I C L EI N F OS U M M A R YArticle history:Received 12 January 2012Accepted 4 May 2012Available online 15 June 2012Keywords:Urinary <strong>tract</strong> <strong>infection</strong>Administrative data<strong>Risk</strong> <strong>factors</strong>Healthcare <strong>associated</strong>SurveillanceUrinary catheterizationBackground: Healthcare-<strong>associated</strong> <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong>s (HCA UTI) account <strong>for</strong> a largeproportion of hospital <strong>infection</strong>s, with recently launched surveillance in the UK focusing onreducing catheter-<strong>associated</strong> <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong>s. However, a wealth of administrativein<strong>for</strong>mation already collected routinely by hospitals is currently not used to its maximumpotential <strong>for</strong> surveillance.Aim: To quantify the evidence base of HCA UTI risk <strong>factors</strong> <strong>and</strong> to determine <strong>their</strong>potential <strong>for</strong> shaping <strong>and</strong> in<strong>for</strong>ming innovative surveillance tools using local hospital data.Methods: A systematic literature review was undertaken to find established risks <strong>for</strong> HCAUTI. Population-attributable risk percentages (PAR%) were calculated <strong>for</strong> these risk<strong>factors</strong>, generating a hierarchy of risks. Administrative hospital data were subsequentlyinterrogated <strong>for</strong> these quantified risks.Findings: Over 30% of the risk <strong>factors</strong> identified from the systematic literature review wereindependent predictors of <strong>infection</strong>. The highest PAR% was <strong>associated</strong> with <strong>urinary</strong> catheterization,with the calculation that 79.3% of UTI would be prevented if catheterization wasnot per<strong>for</strong>med. PAR% calculations were per<strong>for</strong>med <strong>for</strong> 60% of the independent predictors <strong>for</strong>HCA UTI. Sixty-five percent of the identified independent risk <strong>factors</strong> were found to becoded within the administrative hospital dataset, including <strong>urinary</strong> catheterization.Conclusion: This work has quantified established HCA UTI risks <strong>and</strong> demonstrates thatthere is potential <strong>for</strong> more effective use of administrative hospital data <strong>for</strong> risk monitoring<strong>and</strong> surveillance of HCA UTI.Ó 2012 The Healthcare Infection Society. Published by Elsevier Ltd. All rights reserved.Introduction* Corresponding author. Address: Imperial College, Charing CrossCampus, 3rd Floor, The Reynolds Building, St Dunstan’s Road, LondonW6 8RP, UK. Tel.: þ44 (0) 2075940779; fax: þ44 (0) 207594 0854.E-mail address: c.king09@imperial.ac.uk (C. King).Healthcare-<strong>associated</strong> <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong>s (HCA UTI)contribute a significant burden to <strong>healthcare</strong> services globally. 1In the UK, it is estimated that the National Health Service (NHS)incurs 66,160 cases of HCA UTI per year, costing £68 million inexcess bed-days. 2 In the 2006 UK <strong>and</strong> Republic of Irel<strong>and</strong>prevalence survey of <strong>healthcare</strong>-<strong>associated</strong> <strong>infection</strong>s (HCAI),0195-6701/$ e see front matter Ó 2012 The Healthcare Infection Society. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.jhin.2012.05.004
220UTI accounted <strong>for</strong> 19.9% of HCAI, second in frequency only togastrointestinal <strong>infection</strong>s (20.6%). 3 The high rate of UTI withinhospitals is commonly attributed to the use of <strong>urinary</strong> catheters,with 31.8% of the NHS patient population having undergone<strong>urinary</strong> catheterization or bladder instrumentation on theday of the survey or in the preceding seven days. 4Traditional surveillance has long been established as anessential component to any <strong>infection</strong> prevention <strong>and</strong> controlprogramme, 5 despite the fact that it can be costly to implement<strong>and</strong> time consuming to conduct. 6 In the UK, there arem<strong>and</strong>atory surveillance systems <strong>for</strong> several HCAI, such asClostridium difficile (since January 2004) <strong>and</strong> meticillinresistantStaphylococcus aureus (MRSA) bloodstream <strong>infection</strong>s(since early 2001). 7,8 Surveillance of catheter-<strong>associated</strong><strong>urinary</strong> <strong>tract</strong> <strong>infection</strong>s (CA UTI) is now per<strong>for</strong>med as part of aninitiative launched by the UK Department of Health in January2011 in order to reduce patient harm. 9 However, despite thehigh burden that HCA UTI represents to the NHS, this surveillancescheme is voluntary, focuses exclusively on CA UTI, <strong>and</strong> isstill in its infancy. The potential utility of innovative HCA UTIsurveillance tools is apparent, with current work focusing onthe development of automated systems to identify UTI usingtraditional clinical definitions. 10Hospitals routinely collect <strong>and</strong> store large amounts ofadministrative data, including in<strong>for</strong>mation on admissions,microbiology, diagnoses <strong>and</strong> procedures. 11 Although thiswealth of data has not been widely exploited <strong>for</strong> HCAIsurveillance, integrative approaches towards the more effectiveuse of administrative data are being pioneered. 11e13Determining the utility of established risk <strong>factors</strong> <strong>for</strong> HCA UTIwithin administrative hospital data presents the opportunity todevelop <strong>and</strong> test innovative surveillance tools with thepotential to enhance traditional surveillance of UTI within the<strong>healthcare</strong> environment.The aim of this study was to quantify the existing evidencebase of risk <strong>factors</strong> <strong>for</strong> HCA UTI, create a hierarchy of risk,identify these risks within administrative hospital data, <strong>and</strong>assess the potential of this data source <strong>for</strong> in<strong>for</strong>ming novelsyndromic surveillance tools.MethodsSystematic literature reviewA systematic literature review was conducted to establishan evidence base of risk <strong>factors</strong> <strong>for</strong> HCA UTI. EMBASE, PubMed/MEDLINE, Web of Science <strong>and</strong> the Cochrane Database weresearched using ‘UTI’, ‘<strong>urinary</strong> <strong>tract</strong> <strong>infection</strong>’ <strong>and</strong> ‘risk’ as thesearch terms. The Cochrane Database was included to assesswhether or not a comprehensive literature review on HCA UTIrisk <strong>factors</strong> had been undertaken previously. The searchstrategy <strong>and</strong> inclusion criteria were discussed <strong>and</strong> agreedbetween the authors, <strong>and</strong> the search was conducted by a singlereviewer in April 2011.The inclusion criteria were: (1) original research papers inEnglish; (2) clear <strong>and</strong> reasonable study design; (3) demonstratedstatistical analysis, <strong>and</strong> reported odds ratios (OR), relative risksor hazard ratios, <strong>and</strong> P-values; (4) a clear definition of HCA UTIused to diagnose ‘cases’, either based on published definitions(e.g. US Centers <strong>for</strong> Disease Control <strong>and</strong> Prevention) or positivemicrobiology, antibiotic prescription <strong>and</strong> clinical data; (5)C. King et al. / Journal of Hospital Infection 82 (2012) 219e226‘controls’ clearly stated as not diagnosed with an HCA UTI; <strong>and</strong>(6) all study participants had been exposed to ‘health care’,defined as either a hospital admission <strong>for</strong> 72 h or a readmissionwith prior exposure to health care. Those studiesinvestigating risk <strong>factors</strong> <strong>for</strong> acquiring an antimicrobial-resistant<strong>infection</strong> vs an antimicrobial-susceptible <strong>infection</strong> wereexcluded as the controls did not meet the inclusion criteria.Critical Appraisal Skills Programme (CASP) tools, developed bythe British Public Health Resource Unit, <strong>for</strong> caseecontrol(available at: http://www.sph.nhs.uk/sph-files/casp-appraisaltools/Case%20Control%2011%20Questions.pdf/view)14 <strong>and</strong>cohort studies (available at: http://www.sph.nhs.uk/sph-files/casp-appraisal-tools/cohort%2012%20questions.pdf/view) 15were employed <strong>for</strong> critical appraisal of the papers in thisstudy as they were developed specifically <strong>for</strong> cohort <strong>and</strong>caseecontrol studies, <strong>and</strong> have been widely used in reviewarticles. 16 For those papers describing prevalence <strong>and</strong> surveillancestudies, an ‘adjusted CASP cohort tool’ was applied,which included all the aspects considered by the CASP cohorttool 15 with the exception of the follow-up criteria. Themaximum <strong>and</strong> minimum possible CASP scores ranged from14 to 14 <strong>for</strong> cohort studies, <strong>and</strong> from 12 to 12 <strong>for</strong>caseecontrol, prevalence <strong>and</strong> surveillance studies.Those risk <strong>factors</strong> that were <strong>associated</strong> with HCA UTI(P < 0.05) at the univariate <strong>and</strong> multivariate level wereselected <strong>for</strong> further analysis, <strong>and</strong> were defined as ‘significant’risks. An ‘independent’ risk factor was considered when its<strong>associated</strong> P-value was
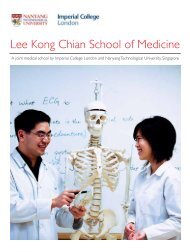
C. King et al. / Journal of Hospital Infection 82 (2012) 219e226 221review in order to address the utility of administrative hospitaldata <strong>for</strong> the development of surveillance tools.Imperial College Healthcare NHS Trust (ICHNT) is one of thelargest NHS hospital groups in the UK, consisting of five hospitalswith 1540 beds <strong>and</strong> one central laboratory. Over 750 localdatabases have been identified within ICHNT, 11 comprisinga mixture of small departmental datasets, surveillance <strong>and</strong>larger trust-wide systems. Data on patient demographics,diagnoses [International Classification of Diseases Version 10(ICD-10)], 19 operations <strong>and</strong> procedures (OPCS), <strong>and</strong> admission<strong>and</strong> discharge data are stored in the large organization-widepatient administration system (PAS). Microbiology <strong>and</strong> laboratorydata are located in the laboratory in<strong>for</strong>mation managementsystem (LIMS), <strong>and</strong> further in<strong>for</strong>mation on antimicrobialprescribing <strong>and</strong> <strong>infection</strong> prevention <strong>and</strong> control is located inlocally per<strong>for</strong>med surveillance.A comprehensive variable list <strong>and</strong> code book of the hospitaldata available <strong>for</strong> this study was created <strong>and</strong> cross-checkedagainst the list of ex<strong>tract</strong>ed risk <strong>factors</strong> <strong>for</strong> UTI. Keywordsearches of the ICD-10 codes were per<strong>for</strong>med, based on the listof HCA UTI risk <strong>factors</strong> identified during the literature review,using the World Health Organization’s online search tool(http://apps.who.int/classifications/icd10). A Microsoft Excel(2007) reference spreadsheet was generated. ICD-10 codesidentified from any included studies were also recorded on thereference spreadsheet. The process was repeated with operation<strong>and</strong> procedure codes <strong>and</strong> pathology codes using referencedatabases provided by ICHNT.In order to use hospital data <strong>for</strong> research, ethical approvalwas granted by St. Mary’s National Research Ethics Committee<strong>for</strong> the use of administrative hospital data from ICHNT in ananonymized <strong>for</strong>mat, i.e. one way anonymization <strong>and</strong> removalof all patient-identifiable fields prior to data analysis (Ref. No.:09/H0712/85).ResultsThe systematic literature search returned 4109 uniquepapers. One percent were excluded <strong>for</strong> not being in English,89% had titles that were not relevant to the study question, <strong>and</strong>6% were excluded as irrelevant after abs<strong>tract</strong> review. Theresults retrieved from the Cochrane Database returned norelevant studies. In total, 154 studies underwent full-textreview <strong>and</strong> 23 were ultimately included in the study(Figure 1). Of the 23 papers included, three papers werecaseecontrol studies, 20e22 13 papers were cohort studies, 23e35six papers were surveillance <strong>and</strong> prevalence studies, 4,36e40 <strong>and</strong>one paper used data derived from a large r<strong>and</strong>omizedcontrolled trial database (Table I). 41The majority of studies were per<strong>for</strong>med in high-incomesettings, of which two were based in the UK. 4,22 Threestudies were undertaken in the middle-income countries ofBrazil, 24 India 23 <strong>and</strong> Egypt. 39 Two studies 23,34 involved paediatricpopulations, with the remaining 21 papers addressingadult populations, including patients from generalwards, 4,20,22,26,28,36,37,39,41 patients in intensive care units(ICUs), 29e31,33,38,40 surgical patients, 35 stroke patients, 32orthopaedic patients, 27 hip fracture admissions, 21 spinalinjury patients 25 <strong>and</strong> renal transplant patients. 24The CASP scores <strong>for</strong> the three caseecontrol studies rangedfrom nine 22 to six, 20 whilst the prevalence studies, using theadjusted CASP cohort study tool, scored between five 4,37 <strong>and</strong>Title not relevant:3668Not English: 44Criteria not met: 13134 – lacking statistics60 – inappropriate cases/controls37 – not original researchInitial search: 4109Abs<strong>tract</strong> review: 441Full-text review: 154Abs<strong>tract</strong> notrelevant: 243Included:23Figure 1. Systematic literature review schematic. The numbersrepresent the number of studies at each stage (e.g. 441 studiesunderwent abs<strong>tract</strong> review).11 36 out of 12. The cohort studies scored between three 38 <strong>and</strong>13 35 out of 14. Of the 23 papers included, almost 80% hada CASP value within the score’s upper quartile, being six <strong>and</strong>above <strong>for</strong> the caseecontrol, prevalence <strong>and</strong> surveillancestudies, <strong>and</strong> seven <strong>and</strong> above <strong>for</strong> the cohort studies.Of the 143 risk <strong>factors</strong> assessed in all the studies, 96 (68%)were significant <strong>and</strong> 43 were independent risk <strong>factors</strong> <strong>for</strong> HCAUTI, with six studies not per<strong>for</strong>ming multivariate analyses. Ofthe independent risk <strong>factors</strong>, 29 were only assessed by onestudy. Among the remaining 14 risk <strong>factors</strong> that were assessedby multiple studies, half were found to be significant in morethan one of the studies in which they were included (femalesex, increasing age, diabetes mellitus, length of hospital stay,prior stroke, <strong>urinary</strong> catheter <strong>and</strong> duration of <strong>urinary</strong> catheter).Female sex was included in all the papers <strong>for</strong> analysis <strong>and</strong>was found to be significant in 65% of the studies. One-quarter ofthe independent risk <strong>factors</strong> were <strong>associated</strong> with <strong>urinary</strong>catheter use <strong>and</strong> management, including colonization of thedrainage bag, 41 having more than two catheters recorded 20 <strong>and</strong>intermittent catheterization. 22In order to assess the relative importance of the significantrisk <strong>factors</strong> <strong>for</strong> HCA UTI, PAR% values were calculated <strong>for</strong> those<strong>factors</strong> where sufficient data were reported in the correspondingstudies. Raw data (as described in the Methods) wereex<strong>tract</strong>ed directly from 14 studies, while ORs were used toobtain raw data in four studies. 25,33e35 Two studies did notpublish sufficient data to enable PAR% calculations, 27,40 <strong>and</strong>three papers were not included as these were prevalencestudies. 4,36,37 Thus, 18 of the 23 papers contributed data to thePAR% calculations. PAR% values were calculated <strong>for</strong> 35 significantrisk <strong>factors</strong> <strong>for</strong> HCA UTI, <strong>and</strong> 26 were also independent risk<strong>factors</strong>. The remaining 17 independent risk <strong>factors</strong> did not havesufficient data <strong>for</strong> PAR% calculations.
222C. King et al. / Journal of Hospital Infection 82 (2012) 219e226Table ISummary of the studies identified as a result of the systematic literature reviewStudy design Critical Appraisal Skills Patient population Country Data source (electronic) Reference (year)Programme Score (total)Caseecontrol 6 (12) General Saudi Arabia Patient records 20 (2004)Caseecontrol 8 (12) Hip Sweden Patient records 21 (1999)Caseecontrol 9 (12) General UK Study/surveillance 22 (1999)Cohort 5 (14) Paediatric India Study 23 (2011)Cohort 9 (14) Transplant Brazil Study 24 (2006)Cohort 11 (14) Spinal Spain Study 25 (2000)Cohort 12 (14) General Australia Study/patient records 26 (2007)Cohort 10 (14) Orthopaedic Spain Study 27 (2001)Cohort 10 (14) ICU Canada Linked records (e) 29 (2002)Cohort 8 (14) ICU Canada Linked records (e) 30 (2005)Cohort 9 (14) ICU France Study 31 (2003)Cohort 9 (14) Stroke USA CASPR 32 (2006)Cohort 8 (14) Paediatric USA Patient records 34 (2009)Cohort 13 (14) Surgery Spain Patient records 35 (2003)Cohort 6 (14) General USA Study 28 (1986)Cohort 12 (14) ICU France Study 33 (2001)Prevalence 5 (12) General UK Prevalence survey 4 (2008)Prevalence 11 (12) General Germany Prevalence survey 36 (1997)Prevalence 5 (12) General Israel Patient records 37 (2005)RCT 8 (14) General USA Study 41 (1986)Surveillance 3 (12) ICU USA Patient records 38 (1999)Surveillance 6 (12) General Egypt Study 39 (2010)Surveillance 12 (12) ICU France Surveillance 40 (2008)ICU, intensive care unit; CASPR, Cali<strong>for</strong>nia Acute Stroke Pilot Registry; RCT, r<strong>and</strong>omized controlled trial.For each study included in the analysis, the study design, the Critical Appraisal Skills Programme (CASP) score <strong>and</strong> the study setting aredescribed. CASP scores are presented together with the total possible score (in parentheses). The data source describes the origin of the dataused by the included study <strong>for</strong> <strong>their</strong> statistical analysis, with ‘study’ meaning either that the data was collected <strong>for</strong> the purpose of the researchpublished, or that there was no further clarification on the origin of the data. An ‘e’ in parentheses denotes that the data used were electronicor automated, instead of using paper patient records or manual searching.Of the 35 risk <strong>factors</strong> <strong>for</strong> which PAR% values were calculated,functional independence (measured as the level ofassistance required with daily living tasks) was found to havea non-significant PAR% (1.47, 95% CI 0.62 to 3.55), despitebeing identified as an independent predictor of HCA UTI. 25 Theremaining 34 significant risk <strong>factors</strong> were stratified into a hierarchy,with the risk factor with the highest PAR% (79.34%, 95%CI 78.18e80.50) being <strong>urinary</strong> catheterization (Table II). Fiverisk <strong>factors</strong> demonstrated protective properties from thecalculated PAR%: creatinine level
Table IISummary of the population-attributable risk percentage (PAR%) values <strong>for</strong> significant risk <strong>factors</strong> of <strong>healthcare</strong>-<strong>associated</strong> <strong>urinary</strong> <strong>tract</strong><strong>infection</strong>s, <strong>and</strong> <strong>their</strong> availability within local administrative hospital data<strong>Risk</strong> factor PAR% 95% ConfidenceIntervalC. King et al. / Journal of Hospital Infection 82 (2012) 219e226 223PopulationsizeNumberof studiesLevel ofsignificanceAvailable inlocal dataDatasourceUrinary catheter 79.34 78.18 to 80.50 4652 2 Independent Y ICD-10/OPCSTransurethral catheterization 52.41 48.21 to 56.60 544 1 Independent N ePositive meatal culture 36.88 33.42 to 40.34 747 1 Significant Y LIMSASA score >2 32.69 31.07 to 34.31 3229 2 Independent N eStroke 27.62 26.39 to 28.86 5028 2 Independent Y ICD-10Urine meter drainage 26.00 23.74 to 28.22 1474 1 Independent N eDisconnection of collection 25.63 23.40 to 27.86 1474 1 Significant N ejunctionBladder dysfunction 25.13 20.31 to 29.96 311 1 Independent Y ICD-10Length of stay >10 days 24.92 21.28 to 28.55 544 1 Independent Y PASUC duration >6 days 23.29 21.13 to 25.45 1474 1 Independent N eFemale sex 23.00 22.51 to 23.44 31,408 16 Independent Y PASHypertension 21.85 18.71 to 25.00 663 1 Significant Y ICD-10Dead kidney donor 19.32 13.26 to 25.38 163 1 Independent Y OPCSColonization of drainage bag 15.69 13.83 to 17.54 1474 1 Independent Y LIMSDrainage bag change 14.43 12.64 to 16.23 1474 1 Significant N eIntermittent catheterization 13.25 10.40 to 16.10 544 1 Independent Y AuditAtrial fibrillation 12.79 10.25 to 15.34 663 1 Significant N eAge >60 years 11.83 10.91 to 12.76 4674 2 Independent Y ICD-10Age >50 years 11.70 10.36 to 13.04 2221 2 Independent Y ICD-10Prior UTI in current10.37 8.82 to 11.93 1474 1 Independent Y ICD-10/LIMShospitalizationDiabetes mellitus 9.56 8.89 to 10.22 7522 6 Independent Y ICD-10ASA score >3 9.54 6.78 to 12.30 435 1 Independent N ePrior indwelling8.35 6.94 to 9.77 1470 1 Significant N ecatheterizationAge >65 years 6.42 5.12 to 7.72 1368 2 Independent Y ICD-10Bag-outlet tube error 5.72 4.54 to 6.91 1474 1 Significant N eOther malignancy 4.24 2.54 to 5.93 544 1 Significant Y ICD-10Bladder instrumentation 3.62 3.07 to 4.17 4365 1 Independent Y OPCSUnresolved spinal injury 3.54 2.99 to 4.09 4365 1 Significant Y ICD-10Central venous catheter 2.07 0.87 to 3.27 544 1 Significant Y OPCSCreatinine
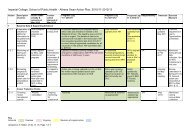
224C. King et al. / Journal of Hospital Infection 82 (2012) 219e226<strong>Risk</strong> <strong>factors</strong> assessed: 143(47 risk <strong>factors</strong> were notstatistically significant)Significant risks: 96Independent risks: 43Located in localhospital data: 39PAR% calculated: 35(one of which wasinsignificant)Located in localhospital data: 28PAR% calculated: 26(one of which wasinsignificant)PAR% <strong>and</strong> located in localhospital data: 24PAR% <strong>and</strong> located in localhospital data: 18Figure 2. Schematic of the numbers of significant <strong>and</strong> independent risk <strong>factors</strong> at different stages in the methodology. All those risk<strong>factors</strong> that are independent are also significant, whereas those risk <strong>factors</strong> that are significant but not independent may only have beenconsidered in univariate analysis or became insignificant when confounders were taken into account in multivariate analysis. Significantrisk <strong>factors</strong>, P-value of
C. King et al. / Journal of Hospital Infection 82 (2012) 219e226 225how to code conditions, <strong>and</strong> in<strong>for</strong>mation on when they are tobe recorded are provided by the NHS (available at: http://www.connecting<strong>for</strong>health.nhs.uk/codingclinic). 46 The mostrecent guidelines specify a group of comorbidities to bem<strong>and</strong>atorily coded within administrative hospital data if thereis any mention of them in the patient’s medical notes, including<strong>urinary</strong> retention, renal failure <strong>and</strong> diabetes. 46 However,despite clear guidance, poor-quality coding is still reported. 47Issues arise from variability in coders <strong>and</strong> <strong>their</strong> experience,<strong>and</strong> the detail <strong>and</strong> accuracy of the in<strong>for</strong>mation contained withinthe patient’s medical notes. In order to create surveillancetools using administrative data, these quality issues need to betaken into consideration, with an underst<strong>and</strong>ing of the potential<strong>for</strong> the under or over-recording of codes.In the absence of a real-time medical record, the applicationof surveillance <strong>for</strong> HCA UTI based on predictors at anindividual level is not plausible. The delay often encounteredwith administrative data means that data on risks, such asdiabetes mellitus, are only available electronically once thepatient has been discharged. Centres such as Salt Lake City,where electronic patient records have been implemented <strong>for</strong>20 years, have shown the potential <strong>for</strong> this technology in aidingsurveillance of HCAI. 48 Certain hospital data, such as pathology<strong>and</strong> radiology in<strong>for</strong>mation, are recorded electronically as theyare processed, suggesting that real-time syndromic surveillancecould be developed based on these data. This has beenimplemented successfully in the USA <strong>for</strong> catheter-<strong>associated</strong>bloodstream <strong>infection</strong>s. 49 However, the use of predictors todevelop surveillance at the hospital population level usingadministrative data is possible with prospective applications.This includes implementing a risk stratified framework <strong>for</strong> HCAUTI surveillance, the creation of benchmarking tools <strong>for</strong> HCAUTI which account <strong>for</strong> local patient populations, <strong>and</strong> theopportunity to monitor interventions <strong>and</strong> control measures.The use of different administrative hospital data systems todevelop novel surveillance systems is still an emerging discipline,<strong>and</strong> with over 750 individual databases located thus farwithin ICHNT, further relevant in<strong>for</strong>mation on risk <strong>factors</strong> islikely to be stored routinely within the hospital data. Electronicsurveillance represents a cost-effective, time-efficient <strong>and</strong>robust approach to surveillance, although it is subjective toclinical opinion <strong>and</strong> a changing policy l<strong>and</strong>scape. 50 In thecontext of HCA UTI, this could potentially provide a system tocomplement traditional surveillance schemes <strong>and</strong> <strong>infection</strong>prevention <strong>and</strong> control practices across <strong>healthcare</strong> settings.Despite the methodology in this paper being based upon theadministrative data found routinely within the UK NHS, theauthors believe that the principle is applicable to any healthsystem with electronic administrative data.This study has demonstrated the potential of local administrativehospital data <strong>for</strong> the development of innovativesurveillance <strong>for</strong> HCA UTI by applying the results froma systematic literature review to local administrative datausing a novel methodology, despite the various limitationsdiscussed. This work has provided the basis <strong>for</strong> a framework tofurther explore the benefits of using hospital data in thedevelopment of surveillance tools <strong>for</strong> HCA UTI. The next stepsare to investigate the utility <strong>and</strong> quality of the codes identifiedby this review in local data, apply this to developing riskprofiles <strong>and</strong> proxy indicators, <strong>and</strong> test the value of syndromicalgorithms to enhance traditional surveillance <strong>and</strong> <strong>infection</strong>control approaches.Conflict of interest statementNone declared.Funding sourcesThe UK Clinical Research Collaboration funds the NationalCentre <strong>for</strong> Infection Prevention <strong>and</strong> Management at ImperialCollege London, <strong>and</strong> also supports the UK National Institute<strong>for</strong> Health Research Biomedical Research Centre fundingscheme. The Dr Foster Unit at Imperial is largely funded bya research grant from Dr Foster Intelligence (an independenthealth service research organization) <strong>and</strong> is affiliatedwith the Centre <strong>for</strong> Patient Safety <strong>and</strong> Service Quality atImperial College Healthcare NHS Trust, funded by theNational Institute <strong>for</strong> Health Research.AcknowledgementsThe authors wish to thank the Infection Prevention <strong>and</strong>Control, Pathology <strong>and</strong> Microbiology departments <strong>and</strong> theIn<strong>for</strong>mation Technology teams within Imperial College NHSTrust <strong>for</strong> <strong>their</strong> collaboration.References1. World Health Organization. WHO guidelines on h<strong>and</strong> hygiene inhealth care: first global patient safety challenge e clean care issafer care. Geneva: WHO; 2009.2. Plowman R, Graves N, Esquivel J, Roberts JA. An economic modelto assess the cost <strong>and</strong> benefits of the routine use of silver alloycoated<strong>urinary</strong> catheters to reduce the risk of <strong>urinary</strong> <strong>tract</strong><strong>infection</strong>s in catheterized patients. J Hosp Infect 2001;48:33e42.3. Smyth ETM, McIlvenny G, Enstone JE, et al. Four country <strong>healthcare</strong><strong>associated</strong> <strong>infection</strong> prevalence survey 2006: overview of theresults. J Hosp Infect 2008;69:230e248.4. Humphreys H, Newcombe RG, Enstone J, et al. Four country<strong>healthcare</strong> <strong>associated</strong> <strong>infection</strong> prevalence survey 2006: riskfactor analysis. J Hosp Infect 2008;69:249e257.5. Haley RW, Culver DH, White JW, et al. The efficacy of <strong>infection</strong>surveillance <strong>and</strong> control programs in preventing nosocomial <strong>infection</strong>sin United States hospitals. Am J Epidemiol 1985;121:182e205.6. Brown C, Richards M, Galletly T, et al. Use of anti-infective serialprevalence studies to identify <strong>and</strong> monitor hospital-acquired<strong>infection</strong>. J Hosp Infect 2009;73:34e40.7. Berrington A, Borriello P, Brazier J, et al. National Clostridiumdifficile St<strong>and</strong>ards Group: report to the Department of Health.J Hosp Infect 2004;56(Suppl. 1):1e38.8. Department of Health. Hospitals to monitor hospital acquired<strong>infection</strong>. Press Release 2000/0584. London: Department ofHealth; 2000.9. Department of Health. Safety express: guide to programmedelivery. London: Department of Health; 2011.10. Choudhuri J, Pergamit R, Chan J, et al. An electronic catheter<strong>associated</strong><strong>urinary</strong> <strong>tract</strong> <strong>infection</strong> surveillance tool. InfectControl Hosp Epidemiol 2011;32:757e762.11. García Álvarez L, Aylin P, Tian J, et al. Data linkage betweenexisting a <strong>healthcare</strong> databases to support hospital epidemiology.J Hosp Infect 2011;79:231e235.12. Teodoro D, Choquet R, Pasche E, et al. Biomedical datamanagement: a proposal framework. Stud Health Technol In<strong>for</strong>mat2009;150:175e179.13. Jen MH, Holmes AH, Bottle A, Aylin P. Descriptive study ofselected <strong>healthcare</strong>-<strong>associated</strong> <strong>infection</strong>s using national hospitalepisode statistics data 1996e2006 <strong>and</strong> comparison with m<strong>and</strong>atoryreporting systems. J Hosp Infect 2008;70:321e327.14. Solutions <strong>for</strong> Public Health. Critical appraisal skills programme ecase control studies. UK: NHS; 2006.
226C. King et al. / Journal of Hospital Infection 82 (2012) 219e22615. Solutions <strong>for</strong> Public Health. Critical appraisal skills programme ecohort studies. UK: NHS; 2004.16. S<strong>and</strong>erson S, Tatt ID, Higgins JP. Tools <strong>for</strong> assessing quality <strong>and</strong>susceptibility to bias in observational studies in epidemiology:a systematic review <strong>and</strong> annotated bibliography. Int J Epidemiol2007;36:666e676.17. Last J. A dictionary of epidemiology. 4th ed. Ox<strong>for</strong>d: Ox<strong>for</strong>dUniversity Press; 2001.18. Pietrantojn CD. Four-fold table cell frequencies imputation inmeta analysis. Stat Med 2006;25:2299e2322.19. World Health Organization. ICD-10 classifications of mental <strong>and</strong>behavioural disorder: clinical descriptions <strong>and</strong> diagnostic guidelines.Geneva: WHO; 1992.20. Al-Helali NS, Al-Asmary SM, Abdel-Fattah MM, Al-Jabban TM, Al-Bamri AL. Epidemiologic study of nosocomial <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong>sin Saudi military hospitals. Infect Control Hosp Epidemiol2004;25:1004e1007.21. Hedstrom M, Grondal L, Ahl T. Urinary <strong>tract</strong> <strong>infection</strong> in patientswith hip fractures. Injury 1999;30:341e343.22. Nguyen-Van-Tam SE, Nguyen-Van-Tam JS, Myint S, Pearson JC. <strong>Risk</strong><strong>factors</strong> <strong>for</strong> hospital-acquired <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong> in a large Englishteaching hospital: a caseecontrol study. Infection 1999;27:192e197.23. Brindha SM, Jayashree M, Singhi S, Taneja N. Study of nosocomial<strong>urinary</strong> <strong>tract</strong> <strong>infection</strong>s in a pediatric intensive care unit. J TropPediatr 2011;57:357e362.24. Dantas SR, Kuboyama RH, Mazzali M, Moretti ML. Nosocomial<strong>infection</strong>s in renal transplant patients: risk <strong>factors</strong> <strong>and</strong> treatmentimplications <strong>associated</strong> with <strong>urinary</strong> <strong>tract</strong> <strong>and</strong> surgical site <strong>infection</strong>s.J Hosp Infect 2006;63:117e123.25. De Ruz AE, Leoni EG, Cabrera RH. Epidemiology <strong>and</strong> risk <strong>factors</strong><strong>for</strong> <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong> in patients with spinal cord injury.J Urol 2000;164:1285e1289.26. Graves N, Tong E, Morton AP, et al. Factors <strong>associated</strong> with <strong>healthcare</strong>-acquired <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong>. Am J Infect Control2007;35:387e392.27. Herruzo-Cabrera R, Lopez-Gimenez R, Cordero J, Munuera L.Urinary <strong>infection</strong> after orthopedic procedures. Int Orthopaed2001;25:55e59.28. Larsen RA, Burke JP. The epidemiology <strong>and</strong> risk <strong>factors</strong> <strong>for</strong> nosocomialcatheter-<strong>associated</strong> bacteriuria caused by coagulasenegativestaphylococci. Infect Control 1986;7:212e215.29. Laupl<strong>and</strong> KB, Zygun DA, Davies HD, Church DL, Louie TJ, Doig CJ.Incidence <strong>and</strong> risk <strong>factors</strong> <strong>for</strong> acquiring nosocomial <strong>urinary</strong> <strong>tract</strong><strong>infection</strong> in the critically ill. J Crit Care 2002;17:50e57.30. Laupl<strong>and</strong> KB, Bagshaw SM, Gregson DB, Kirkpatrick AW, Ross T,Church DL. Intensive care unit-acquired <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong>s ina regional critical care system. Crit Care 2005;9:R60eR65.31. Leone M, Albanese J, Garnier F, et al. <strong>Risk</strong> <strong>factors</strong> <strong>for</strong> nosocomialcatheter-<strong>associated</strong> <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong> in a polyvalent intensivecare unit. Intens Care Med 2003;29:1077e1080.32. Ovbiagele B, Hills NK, Saver JL, Johnston SC. Frequency <strong>and</strong>determinants of pneumonia <strong>and</strong> <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong> duringstroke hospitalization. J Stroke Cerebrovasc Dis 2006;15:209e213.33. Tissot E, Limat S, Cornette C, Capellier G. <strong>Risk</strong> <strong>factors</strong> <strong>for</strong>catheter-<strong>associated</strong> bacteriuria in a medical intensive care unit.Eur J Clin Microbiol 2001;20:260e262.34. Traxel E, DeFoor W, Reddy P, Sheldon C, Minevich E. <strong>Risk</strong><strong>factors</strong> <strong>for</strong> <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong> after dextranomer/hyaluronic acid endoscopic injection. J Urol 2009;182(Suppl.):1708e1712.35. Vazquez-Aragon P, Lizan-Garcia M, Cascales-Sanchez P, Villar-Canovas MT, Garcia-Olmo D. Nosocomial <strong>infection</strong> <strong>and</strong> related risk<strong>factors</strong> in a general surgery service: a prospective study. J Infect2003;46:17e22.36. Kampf G, Gastmeier P, Wischnewski N, et al. Analysis of risk<strong>factors</strong> <strong>for</strong> nosocomial <strong>infection</strong>s e results from the first nationalprevalence survey in Germany (NIDEP study 1). J Hosp Infect1997;37:103e112.37. Mnatzaganian G, Galai N, Sprung CL, et al. Increased risk ofbloodstream <strong>and</strong> <strong>urinary</strong> <strong>infection</strong>s in intensive care unit (ICU)patients compared with patients fitting ICU admission criteriatreated in regular wards. J Hosp Infect 2005;59:331e342.38. Rosser CJ, Bare RL, Meredith JW. Urinary <strong>tract</strong> <strong>infection</strong>s in thecritically ill patient with a <strong>urinary</strong> catheter. Am J Surg 1999;177:287e290.39. Talaat M, Hafez S, Saied T, Elfeky R, El-Shoubary W, Pimentel G.Surveillance of catheter-<strong>associated</strong> <strong>urinary</strong> <strong>tract</strong> <strong>infection</strong> in 4intensive care units at Alex<strong>and</strong>ria university hospitals in Egypt. AmJ Infect Control 2010;38:222e228.40. Vanhems P, Baratin D, Voirin N, et al. Reduction of <strong>urinary</strong> <strong>tract</strong><strong>infection</strong>s acquired in an intensive care unit during a 10-yearsurveillance program. Eur J Epidemiol 2008;23:641e645.41. Platt R, Polk BF, Murdock B, Rosner B. <strong>Risk</strong>-<strong>factors</strong> <strong>for</strong> nosocomial<strong>urinary</strong>-<strong>tract</strong> <strong>infection</strong>. Am J Epidemiol 1986;124:977e985.42. Dindo D, Muller MK, Weber M, Clavien P- A. Obesity in generalelective surgery. Lancet 2003;361:2032e2035.43. Jankovic S, Radosavljevic V. <strong>Risk</strong> <strong>factors</strong> <strong>for</strong> bladder cancer.Tumori 2007;93:4e12.44. Connor J, Norton R, Ameratunga S, et al. Driver sleepiness <strong>and</strong> riskof serious injury to car occupants: population based case controlstudy. BMJ 2002;324:1125.45. Madigan MP, Ziegler RG, Benichou J, Byrne C, Hoover RN.Proportion of breast cancer cases in the United States explainedby well-established risk <strong>factors</strong>. J Natl Cancer Inst 1995;87:1681e1685.46. National Health Service Classification Service. Coding clinic. 2011.47. Schweizer ML, Eber MR, Laxminarayan R, et al. Validity ofICD-9-CM coding <strong>for</strong> identifying incident methicillin-resistantStaphylococcus aureus (MRSA) <strong>infection</strong>s: is MRSA <strong>infection</strong>coded as a chronic disease? Infect Control Hosp Epidemiol2011;32:148e154.48. Evans RS, Burke JP, Classen DC, et al. Computerized identificationof patients at high-risk <strong>for</strong> hospital-acquired <strong>infection</strong>. Am J InfectControl 1992;20:4e10.49. Woeltje K, McMullen K, Butler AM, Goris AJ, Doherty J. Electronicsurveillance <strong>for</strong> <strong>healthcare</strong>-<strong>associated</strong> central line-<strong>associated</strong>bloodstream <strong>infection</strong>s outside the intensive care unit. Infect ContHosp Epidemiol 2011;32:1086e1090.50. Lazarus R, Kleinman K, Dashevsky I, deMaria A, Platt R. Usingautomated medical records <strong>for</strong> rapid identification of illnesssyndromes (syndromic surveillance): the example of lower respiratory<strong>infection</strong>. BMC Public Health 2001;1:9.