Resident Handbook - UC Davis Health System
Resident Handbook - UC Davis Health System
Resident Handbook - UC Davis Health System
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
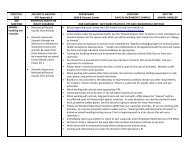
for EM occur once a month(on the third monday from 12:30 to 1:30 in conference roomAB. Periodic sessions with Dr. Rawlings as mentioned earlier. Topics will includeprocedure training. <strong>Resident</strong>s will be expected to visit PHI Aeromedical Transportheadquarters for training in Airway management. This will be arranged by Dr. Rawlings4. Self-directed learning- including self-initiative, asking for assistance and consultsappropriately, accepting criticism, and applying new information.5. Interpersonal and communication skills- including effective and appropriate communicationwith nurses, ED Attending, peers, consultants, patients, and families.6. Professionalism- relating with staff and patients in a responsible, ethical, empathic,compassionate, and trustworthy manner.7. <strong>System</strong>s based practice- uses all care resources and ancillary care providers appropriately.D. ED Organization:Patient flow: a triage nurse and Mid-level provider (Physician Assistant or Nurse Practitioner)will first see all patients arriving to the ED through the lobby entrance. This will occur in thetriage area if there are no beds available to be brought back immediately. A brief history will betaken, limited physical exam, and vitals will be done. The patient disposition may sometimes bemade directly from there, and other times the mid-level provider will start the work-up andtreatment while the patient awaits bedding in the main emergency department or the ED Annex.When a bed is available, the patients chart will then be put in the main ED rack. Seriously illpatients will be taken back immediately to a bed. The bottom left side of the rack has thepatients who have been waiting the longest. A yellow chart will indicate that the patient has notbeen seen by a physician or mid-level provider yet (they may have arrived by ambulance orbrought straight back). These are priority and should bee seen first. Before going to see thepatient, please make the attending aware you are taking the chart from the rack and will see thepatient in a timely manner. This helps to avoid confusion as to where you may be and thelocation of the medical chart. <strong>Resident</strong>s will want to see those patients who appear challengingand unusual. Many orthopedic injuries and lacerations, which may be of interest to residents, aretriaged to the ED Rapid Access Wing (RAWhide area). These patients, however, must be staffedwith the ED attending and not the mid-level providers, so please make the Attending aware andthe Midlevel provider aware of your interest.1. At SECH, color codes on the Chart: Each chart has 4 tabs: Red- nurse orders. Yellowspecimencollection. Blue- physician re-evaluation. Green- discharge patient. <strong>Resident</strong>smust review each case with the attending who will also personally evaluate the patient.2. Referral/Transfer Calls: <strong>Resident</strong>s may not accept these phone calls even if asked to do so bythe nurses (if the ED Attendings are busy). Most of the nurses know this. But if asked,residents must decline taking the call.3. Documentation: <strong>Resident</strong>s must document their findings on the paper chart and consider(discuss with attending) dictating a note, including the name of the supervising attendingphysician. Dictation will be rare, but good documentation will be expected and Dr.Rawlings will review the documentation before the rotation. <strong>Resident</strong>s, who participatein resuscitations or assist with procedures but are not primarily involved with the care ofPage 43 of 153C:\Documents and Settings\dhutak\Desktop\rshb13.doc