Health In Wandsworth - Imperial College London
Health In Wandsworth - Imperial College London
Health In Wandsworth - Imperial College London
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
06/07<strong>Health</strong> <strong>In</strong> <strong>Wandsworth</strong>The <strong>In</strong>dependent Annual Report of the Director of Public <strong>Health</strong><strong>London</strong> 2008
Published by Department of Public <strong>Health</strong><strong>Wandsworth</strong> Teaching Primary Care Trust3rd Floor Wimbledon Bridge HouseWimbledon, <strong>London</strong> SW19 3RUTel: 020 8812 7600Fax: 020 8812 7780Email: comms@wpct.nhs.ukFirst Published June 2008Copyright © <strong>Wandsworth</strong> PCT 2008The content is the responsibility of the Deputy Director of Public <strong>Health</strong>, Velena GilfillianAll rights reserved. All or part of this report may be reproduced, copied or disseminated by individuals, organisations,or reviewers provided that credit is given to <strong>Wandsworth</strong> Teaching PCT and/or the authors.Design: www.fountainhead.ccISBN 978-0-9519343-4-0
<strong>Health</strong> in <strong>Wandsworth</strong>Velena GilfillianDeputy Director of Public <strong>Health</strong>Department of Public <strong>Health</strong><strong>Wandsworth</strong> Teaching Primary Care Trust<strong>London</strong> 2008
ForewordDuring 2006/7 there was a continuation of the change process in the NHS and LocalAuthority. This has included the introduction of new polices, guidelines and performancemechanisms. These changes have brought with them opportunities to refocus work onprevention to improve health and reduce ill health. As a consequence this has enableda period of forward thinking and the creation of opportunities for health investment toobtain noticeable health gain and eventually health outcomes for those who live andwork in <strong>Wandsworth</strong>.Local strategic plans such as the Primary Care Trust Strategic Commissioning andOperational plans, the Children and Young People Plan led by the Council and theOlder Persons Strategy are important frameworks through which health improvementscan be guided. Primary prevention interventions implemented through primary care,community services, social services, education, the voluntary sector, local business andin the community are settings where healthy differences will be made. This has to beunderpinned by an effective commissioning process based on current need and anunderstanding of future need.This report intends to provide some reflection and direction on areas whereconcentrated efforts on prevention can demonstrate health gains in a relatively shorttime period. Chapter one sets the scene by briefly describing new policies impactingon public health. It also provides an update on actions taken on the recommendationsfrom the previous Public <strong>Health</strong> Report. Chapter two provides an overview of majorlifestyle risk factors as the cause of many modern day conditions that are preventable.<strong>In</strong> Chapter three, a range of issues associated with addiction are tackled. Chapter fourconcentrates on maternal health with a synopsis of a recent needs assessment and theactions required to reduce low birth weight. Chapter 5 focuses on sexual health, animportant area of Public <strong>Health</strong> concern which resonates with <strong>Wandsworth</strong>’s youngand mobile population. Chapter 6 provides a picture of primary care and the range ofpractitioners who have a role in maintaining and improving health. Chapter seven looksat issues impacting on emergency preparedness.Appendix 1 provides an outline of the nine Public <strong>Health</strong> competencies and Appendix2 gives examples of choosing health initiatives that have been produced to date. <strong>In</strong>Appendix 3 there are examples of work undertaken in the Public <strong>Health</strong> Department.Appendix 4 desccribes the work surrounding clinical effectiveness and Appendix 5describes the function of health intelligence and provides a range of indicators of healthThroughout this report local data is presented in order to give a picture of the currentstatus in line with available data. There is significant development needed in theinformation sources available, particularly in primary care, community nursing andother health determinants associated with the Local Authority.The pulling together of this report is as a result of the dedication and hard work of anumber of people. I would however like to give my particular appreciation to LaurenceGibson who has been pivotal in bringing together this report.My reflection on the last decade in the NHS is that there have been a series of positiveshifts that have brought public health closer to the centre stage, which has continuedduring the last eighteen months. I am truly excited by this and believe there are nowgreat opportunities to prevent ill health and so improve health and well-being in<strong>Wandsworth</strong>.Velena GilfillianDeputy Director of Public <strong>Health</strong><strong>Wandsworth</strong>, May 20082<strong>Wandsworth</strong> Teaching Primary Care Trust
ContentsChapter 1 <strong>In</strong>troduction41.1 New Drivers for <strong>Health</strong> Change 41.2 <strong>Health</strong> <strong>In</strong>equalities 41.3 Rising Obesity 41.4 Smoke Free England 41.5 Human Papilloma Virus 41.6 New Local Area Agreements 51.7 Financial Turnaround 51.8 World Class Commissioning 51.9 <strong>Health</strong>care for <strong>London</strong> 61.10 Joint Strategic Needs Assessment (JSNA) 61.11 Social Marketing 71.12 Recommendations 81.13 Public <strong>Health</strong> Report 2005/6Recommendations 8Chapter 2 Prevention of Disease in <strong>Wandsworth</strong> 112.1 <strong>In</strong>troduction 112.2 Risk Factors for ill-health 112.3 Preventive Programmes in <strong>Wandsworth</strong> 132.4 The Impact of <strong>In</strong>equalities 162.5 Ethnicity and <strong>In</strong>equalities 162.6 Population Wide and High Risk<strong>In</strong>dividual Prevention Approaches 162.7 Estimates of Avoidable Disease Burden 162.8 Recommendations 18Chapter 3 Addiction193.1 Definition and Scope 193.2 <strong>Health</strong> Social and EconomicImpact of Alcohol Addiction 193.3 <strong>Health</strong> Social and EconomicImpact of Drug Addiction 213.4 <strong>Health</strong> Social and EconomicImpact of Gambling 223.5 Conclusion 233.6 Recommendations 23Chapter 4 Maternal <strong>Health</strong>254.1 Births and Mortality 254.2 Tackling Mortality andLow Birth Weight 274.3 Recommendations 29Chapter 5 Sexual <strong>Health</strong>305.1 Definition and Scope 305.2 Sexual <strong>Health</strong> as a Public <strong>Health</strong> Issue 305.3 <strong>Wandsworth</strong>’s Response toThese Issues 305.4 Teenage Pregnancy 315.5 Sexually Transmitted <strong>In</strong>fections (STIs) 325.6 Improving Access to Sexual<strong>Health</strong> Services 365.7 Access to Contraception 365.8 Termination of Pregnancy 365.9 Sexual <strong>Health</strong> Promotion 375.10 Recommendations 38Chapter 6 Primary Care396.1 Defining Primary Care 396.2 Current Service Providersand Patient Profiles 396.3 Access to General Practice 456.4 Service Data Currently Availablefrom General Practice 466.5 Immunisation and Screening 466.6 Recommendations 50Chapter 7 Emergency Planning517.1 Protecting the Public 517.2 Governance and theLegislative Environment 517.3 Emergency Preparedness 517.4 Strategy to Implement EmergencyPreparedness 527.5 Achievements for 2007/08 527.6 Conclusion 527.7 Recommendations 52Appendix 1 Nine Areas of Public <strong>Health</strong> 53Appendix 2 Choosing <strong>Health</strong> 55A2.1 <strong>In</strong>troduction 55A2.2 Implementing Choosing <strong>Health</strong>in <strong>Wandsworth</strong> 55A2.3 <strong>Health</strong>y Living Programme 55A2.4 <strong>Wandsworth</strong> <strong>Health</strong> TrainerProgramme 56A2.5 Building on Firm Foundations 57A2.6 <strong>Health</strong> Improvement Projectsand <strong>In</strong>itiatives 58Appendix 3 Example of Public <strong>Health</strong> <strong>In</strong>itiatives 59Appendix 4 Clinical Effectiveness 61A4.1 Scope 61A4.2 Clinical Effectiveness Group 61Appendix 5 <strong>Health</strong> <strong>In</strong>telligence 63Staff in the Public <strong>Health</strong> Department 70Glossary 71<strong>Wandsworth</strong> Teaching Primary Care Trust 3
1.<strong>In</strong>troduction1.11.21.31.3.1New Drivers for <strong>Health</strong> ChangeSince the publication of the last public health reportthere have been significant changes, nationally andlocally. A range of new national drivers and initiativeshas been introduced with the intention of refocusingvision and energies up stream in order to prevent illhealth and promote health and well-being. Changesin the local economy have placed a re-emphasis oninvestment for improving the health of the public.<strong>Health</strong> <strong>In</strong>equalitiesThe Mayor’s draft inequalities strategy ‘Reducing<strong>Health</strong> <strong>In</strong>equalities – Issues for <strong>London</strong> and Prioritiesfor Action’ (August 07) made reference to theimportance of promoting health and well beingacross the life course. The report is underpinnedby cross cutting themes of housing, transport,education and employment, recognising importanthealth determinants for individuals, families andcommunities. This is a welcome move towardsa systematic process for planning and deliveringservices. It also provides constructive information intargeting specific age groups and communities. At alocal level, relationships with the Local Authority willbe paramount in taking forward recommendationsfrom the mayor’s inequalities strategy.Rising ObesityThe noticeable rise in obesity will over time furtherthe spectrum of health inequalities, which alsodisproportionately affects certain ethnic and socialgroups. It had been estimated that based oncurrent trends, 60%of the population in Englandwill be obese by 2050. The recent publication ofthe National Obesity Strategy (Jan 08), ‘<strong>Health</strong>yWeight <strong>Health</strong>y Lives’ sets the challenge to halt therise in the prevalence of obesity. As with most, ifnot all, modern lifestyle epidemics, effective actionwill require cross government support and multidisciplinarypartnerships at the local level (this hasalso been highlighted in the Mayor of <strong>London</strong>’s<strong>In</strong>equality Strategy). <strong>Wandsworth</strong> has alreadydeveloped and approved an obesity strategy whichwill need to be reviewed in line with national guidanceand implemented through local partnerships.Tool Kits for ActionThe publication of tool kits such as ‘lightening theload: tackling overweight and obesity’ (2007) and‘easing the pressure: tackling hypertension’ (2005)by the Facility of Public <strong>Health</strong>, demonstrate theco-morbidity of many health conditions that can1.41.5result from being overweight. They also advocate anintegrated approach to delivery of initiatives, whichsupports the approach taken locally.Smoke Free EnglandJuly 1st 2007 was a historic landmark for publichealth in England; all public places became smokefree. This now means large numbers of peopleare protected from breathing second hand smoke,known to cause a range of illness including cancer.Smoking prevention and cessation is still a significantlocal public health issue as smoking is still responsiblefor a large number of deaths. Therefore a sustainedfocus is required for health professionals and othersto support smokers to quit, also to encourage andenable young people not to begin smoking.Human Papilloma VirusThe Department of <strong>Health</strong> recently announcedthe introduction of the human papilloma virusimmunisation programme to routinely vaccinate girlsaged 12–13 years to protect against cervical cancer.Human papilloma is transmitted from skin to skinand through genital contact. Up to 80% of sexuallyactive people will be infected with human papillomaat some point in their lifetime. For most of thesepeople the body’s own immune system will clearthe virus. However in some cases infection canbecome persistent and cause abnormalities in thecells of the cervix that transform into cervical cancer.Despite the existence of the cervical cancer screeningprogramme which has reduced the number of casesof cervical cancer considerably, there remain in theUK approximately 2,800 new cases of cervical cancera year. On average 21 women die from the diseaseeach week.The Department of <strong>Health</strong> recommends that thevaccination programme should begin in September2008, followed by a two-year catch up campaignbeginning autumn 2009 for girls up to 18 years.This is a new approach to preventing cervicalcancer and will run alongside the cervical screeningprogramme in general practice. <strong>In</strong> line with nationalrecommendations, the vaccination programmewill be delivered through schools. The need for aspecialised immunisation team has been identifiedto support the work in <strong>Wandsworth</strong> schools. Aninformation campaign will be developed to informparents, students, head teachers, health careworkers and the local community. The involvementof these stakeholders and others will be instrumentalin making the programme and its uptake a success.4<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 1: <strong>In</strong>troduction<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/071.61.71.8New Local Area AgreementsThe introduction of the revised Local AreaAgreement framework provides opportunities forstatutory and voluntary sector and communitygroups to work closely together. The 198 nationaloutcome indicators are intended to match localpriorities to allow the Police, Primary Care Trusts,Councils and other partners to tackle underlying andfundamental issues affecting health, well-being andsocial cohesion, for those most vulnerable and at riskin our communities. Targets have yet to be finalised,however, chosen health indicators should be ableto demonstrate real and proxy health measurementimprovement over the life of the agreement, reducehealth inequalities, and be attributable to costeffective interventions with a sustainability plan.Again, joint work with the Local Authority and otherswill be paramount to achieving health improvements.Financial TurnaroundDuring the 2006/7 financial year <strong>Wandsworth</strong>Teaching Primary Care Trust achieved financial balanceafter some years of overspend and disinvestmentsThis new era of financial confidence puts thePrimary Care Trust in a desirable position to planand importantly invest in the future health and wellbeing of the population. Financial stability bringsan enormous responsibility to spend wisely, to havethe foresight, confidence and determination todevelop health plans that are not wholly focusedon treating ill health, but also concentrate on howto keep people in good physical and mental healththrough active engagement with those who liveand work in <strong>Wandsworth</strong>. This requires a long termand sustainable vision for ten years and beyond,rather than the traditional project based initiativewhich restricts the evaluation of longer-term healthoutcomes.World Class CommissioningThe development of a Commissioning StrategicPlan for <strong>Wandsworth</strong> Primary Care Trust has setthe landscape for the next 3–5 years. Capturedwithin the core of the document are the principlesof ill health prevention, promotion of health andwell-being, sustainability of health, equitableaccess to services and targeting health inequalities.Programme delivery is divided between five goals:1.Improving the life expectancy over and abovethe expected trends and focus on greater healthgain for those in deprived wards2.3.4.5.Enabling young people to enter adulthood in astate of health that enables them to reach theirfull potential.Improving the quality and responsiveness ofservices that address mental well-being, sexualhealth, drugs, alcohol and obesity.Improving access to, and responsiveness of GPand other primary care services.Improving the quality of services for peopleliving with complex and/or long term conditions.The diagram below demonstrates the importanceof the commissioning function, influenced throughengagement with local populations to improve healthand well-being in order to provide services that areresponsive to local need and of a high standard.The Three Functions of a PCTEngaging with its local populationto improve health and well-beingCommissioning a comprehensiveand equitable range of high qualityresponsive and efficient services,within allocated resourcesDirectly providing high qualityresponsive and efficient serviceswhere this gives best valueSource: Department of <strong>Health</strong> May 2006Front line staff have a major role in the prevention ofill health and the promotion of health and well-being.This may seem for some to be an obvious statement;however, the analysis of a pilot health promotion auditteam tool within <strong>Wandsworth</strong> Community ProviderDirectorate revealed different levels of understanding.The results showed that for some staff healthpromotion was a natural element within their role,while for others it seemed to have little relevance. <strong>In</strong>order to support and enable patients and the publicto make healthier choices, front line staff need to beencouraged to provide opportunistic advice as well asstructured health promotion support. Front line staffare our largest and greatest asset, we must supportand enable them to reach their health promotionpotential. Preventive action taken early will reduce theonset of conditions that lead to ill health.<strong>Wandsworth</strong> Teaching Primary Care Trust 5
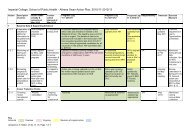
Chapter 1: <strong>In</strong>troduction<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07<strong>Wandsworth</strong> Public <strong>Health</strong> Directorate recommendsthat prevention activities should be introducedand developed within Service Level Agreementsfor 2009/10. There should be incremental changesover a period of time to allow for staff and servicedevelopments. Preventive activities should eventuallybecome a substantive element within Service LevelAgreements. The nine health improvement themeswithin the strategic commissioning plan shouldbe reflected as appropriate within commissioningintentions and Service Level Agreements.Nine delivery themes have been identifieddemonstrating a strong focus on health improvement:One of the five principles is ‘prevention is better thencure’. Public health is featured under the theme ofstaying healthy and aims to:• Tackle inequalities by ensuring equity for <strong>London</strong>’sdiverse and mobile population, for exampleimplementation of <strong>Health</strong> Impact Assessments onhealth policies. Other priorities include children andyoung people, obesity, mental health and well-being.• Develop population and individual interventionsacross the broad spectrum of public health;for example, engaging with the ‘real world’through workplaces and schools, screening andopportunistic health improvements.Table 1.1: Nine Key Commissioning StrategyPlan <strong>In</strong>itiatives<strong>In</strong>itiative• <strong>In</strong>tegrate health improvement in all health andsocial care services, with the intention of providingopportunistic and holistic approaches to preventill health.1.91 Child <strong>Health</strong>2 Stop Smoking3 <strong>Health</strong>y Living4 Mental <strong>Health</strong>5 Drug and Alcohol6 Obesity7 Sexual <strong>Health</strong>8 Access and Primary Care <strong>In</strong>frastructure9 Long Term ConditionsSource: <strong>Wandsworth</strong> PCT Commissioning Strategy Plan 2007–2012<strong>Health</strong>care for <strong>London</strong>The recent report by Lord Ara Darzi (2007) highlightedthat millions of <strong>London</strong>ers face preventable illnessesand many are at risk of stroke and heart attack forwhich they will require prompt treatment. The reportset the scene for a major <strong>London</strong> consultation led bythe 31 <strong>London</strong> Primary Care Trusts and Surrey PCT.The aim of the consultation is to develop a strategy tomeet the health and health care needs of <strong>London</strong>ers.The strategy aims to; improve health, meet theexpectations of <strong>London</strong>ers, redress inequalities inhealth and health care, refocus care from acute to thecommunity setting including better access to generalpractice, develop flexibility within the NHS workforceand achieve more efficiency for taxpayers money.1.10• Provide health protection; targeting communicabledisease such as HIV and TB which are importantpublic health issues for <strong>London</strong>. Emergencypreparedness is also included within this.• Promote corporate social responsibility withinhealth and social care. This includes economic andenvironmental impacts.The outcome of the <strong>Health</strong>care for <strong>London</strong>Consultation may have a profound effect upon thestructure of health and social care services. It willprovide a new face of service provision. It will enablethe integration between primary, secondary andsocial care. <strong>In</strong> some cases this will be partly achievedthrough the development of new health facilities andalso the creation of new and revised care pathways.Public health must be embedded within the process.Public health is able to provide health intelligence,enable critical appraisal, demonstrate the evidencebase, support the development of quality servicesand influence and facilitate health improvements.Joint Strategic Needs Assessment (JSNA)The publication of the ‘Commissioning for <strong>Health</strong>and Well-Being Framework’ (2007) is an importantstep towards joint planning, commissioning anddelivery. Primary Care Trusts and Local Authoritieshave been given a mandate to produce a JSNA.The purpose of the assessment is to use data andinformation on inequalities in order to develop ahealth and social care response.Importantly the JSNA brings together informationfrom a broad range of sources. It includes majorhealth determinants such as housing, education,6<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 1: <strong>In</strong>troduction<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07income and transport. This is important as it hasbeen widely acknowledged that a healthy societyrequires certain prerequisites which provide forbasic needs before health in its widest sense can beachieved. As such, the work of Local Authorities hasa life long and significant impact upon health andwell-being.The Public <strong>Health</strong> department and the PCT arecurrently working with colleagues at the LocalAuthority to analyse and bring together data. Animportant aspect of the assessment is also to capturelocal voices that will help to shape the findings andrecommendations. The report, when compiled, willpull together health need across all age groups.Tables 1 – 4 provide examples of key life stages(events), consequent health risks, services, andcurrent pressures. The final document will highlightpriorities for each organisation plus common healthconcerns, which need to be tackled together.Key outcomes and recommendations from thisjoint piece of work will be important in reshapingpriorities for the refresh of the Primary Care TrustCommissioning Strategy Plan for 2008/09. It shouldalso highlight any gaps and confirm strategies forchildren and young people. These will be bestdelivered though the collaborative Children andYoung People Partnership board. The findings fromthe JSNA will enable a refinement of the olderpeople strategy.Maslow’s Hierarchy of NeedsSelf-actualisation(achieving individual potential)Esteem needs(self-esteemand esteem from others)Belonging needs(love, affection, being a part of groups)Safety needs(shelter, removal from danger)Biological and physiological needs(water, food, sleep)Maslow’s hierarchy of needs demonstrates that basic and lower level needshave to be met to enable individuals to advance to the next leveland to eventually reach their full potential – including health.Abridged: A.H. Maslow, A Theory of Human Motivation, Psychological Review 50(1943):370–96Table 1.2: Application of Social Marketing at a Micro, Organisational and Macro Levels1. <strong>In</strong>dividual Consumer 2. Organisation or group 3. SocietyShort term Behaviour Change Changes in societal norms Policy changeTargeted and consistent messages Targeted and consistent messages Targeted and consistent messagesAccess to information, support and advicesuch as smoking cessation, healthy eatingand weight management<strong>In</strong>fluencing people in key positions to takeaction, for example the removal of tobaccoadvertising near schools and collegesor clear food labelling in shops, cafes,restaurants and supermarketsChanges affecting the behaviour ofpopulations, such as the compulsory ban onthe marketing and sponsoring by tobaccocompanies, the introduction of smoke freepublic places. Also prohibiting fast foodadvertising during children TV viewing timesLong term Lifestyle change Organisational change Social Cultural change and health outcomeTargeted and consistent messages Targeted and consistent messages Targeted and consistent messagesReduction in the numbers of peoplewho smokeHalt in the rise of people who becomegrossly overweightPrevent retailers from selling cigarettes tominorsOverall reduction in fat and salt content inall foodsReduction in illness associated with tobaccoor obesitySource: Adapted from Levy and Zaltman 1975<strong>Wandsworth</strong> Teaching Primary Care Trust 7
Chapter 1: <strong>In</strong>troduction<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/071.111.12Social MarketingThe re-emergence of social marketing as a publichealth tool has gathered momentum over the lastyear. <strong>London</strong> Strategic <strong>Health</strong> Authority have agreedfunding for social marketing programme to targetproblematic public health issues common to <strong>London</strong>.These include immunisation, smoking cessation, andcardiovascular disease.The application of marketing techniques has been usedfor decades to encourage consumers to buy productsand adopt behaviours in the belief particular productswill enhance their lives for the better.Many social and health problems have behaviouralcauses as a result of everyday voluntary and humanactivity. Examples of behaviours that carry ahealth risk are tobacco use, unhealthy eating andunprotected sex.Social marketing has been developed as a tool totarget specific health messages at specific groupswithin the community. Social marketing has alsobeen used successfully to introduce health policiessuch as smokefree public places and changes inhealth food labelling. Table 1.2 gives an example ofsocial marketing used across all levels of society.Local public health initiatives will benefit from the pan<strong>London</strong> approach, however, localised initiatives will needto be developed to provide for the particular needs of<strong>Wandsworth</strong> population groups.Recommendations1.Update obesity strategy in line with national guidance.2. Use the commissioning process to target widerinterventions to improve health and well-being.For example: cascading healthy eating messagesthrough appropriate services at larger groups ofthe public; enable the wider distribution of briefintervention to smokers; targeting smokers infamilies and smokers with long term conditions.1.13Public <strong>Health</strong> Report 2005/6RecommendationsReview of the recommendations from 2005/6<strong>In</strong>dependent Annual Report for the Director ofPublic <strong>Health</strong>This Annual Public <strong>Health</strong> Report maps progress inrelation to the recommendations made in the 05/06report. These include: service redesign, issues concerningchildren and young people, increased focus on mentalhealth and the development of a comprehensive healthprogramme in <strong>Wandsworth</strong> prison.The recommendations for each chapter have led to anumber of actions as specified in Table 2.References[1] Greater <strong>London</strong> Authority. Living Well in <strong>London</strong>; theMayors Draft <strong>Health</strong> <strong>In</strong>equalities Strategy for <strong>London</strong>.2008.[2] Department of <strong>Health</strong>. <strong>Health</strong>y Weight, <strong>Health</strong>y Lives: ACross Government strategy for England. TSO: <strong>London</strong>,2008.[3] Faculty of Public <strong>Health</strong>. National <strong>Health</strong> Forum.Lighting the Load: Tacking Overweight and Obesity.2007.[4] Faculty of Public <strong>Health</strong>. National <strong>Health</strong> Forum. Easingthe Pressure: Tacking Hypertension. 2005.[5] Department of <strong>Health</strong>. Commissioning for <strong>Health</strong> andWell-Being. TSO: <strong>London</strong>, 2007.[6] Lynn Mac Fadyen, Martine Stead and Gerard Hastings.Synopsis of Social Marketing.1999.[7] <strong>Wandsworth</strong> NHS Primary Care Trust. <strong>Health</strong> in<strong>Wandsworth</strong>. The <strong>In</strong>dependent Report of the Directorof Public <strong>Health</strong> 05/06. 2007.3.4.5.<strong>In</strong>tegrate public health measures into localplans developed from <strong>Health</strong>care for <strong>London</strong>Consultation recommendations.Use the outcomes of the Joint Strategic NeedsAssessment to refresh local plans.Develop segmented communication interventionsfor specific community and population groups.8<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 1: <strong>In</strong>troduction<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table 1.3: Recommendations from Public <strong>Health</strong> Report 05/06 <strong>Health</strong> in <strong>Wandsworth</strong><strong>In</strong>troductionRecommendationActions1.2.Commissioning services from a defined geography andnot merely for the GP registered populationTarget resources at deprived areas and particular atrisk groupsA key development during 2007 has been the health need assessment carried out inNorth Battersea to support service redesign and improvement.North Battersea includes two of the five highest wards of deprivation in the borough.Further RecommendationThe deprived wards of Tooting and Graveney require a similar level of health analysis toensure equitable access to services and health improvement initiatives.Chapter 1: Changing population, changing needsRecommendationActions1.2.Redesign of services such as sexual health/contraception servicesRadical review of the delivery of primary andcommunity servicesDuring the last year considerable effort has focused on the redesigning of <strong>Wandsworth</strong>contraception services. A hub and spoke model has been developed, underpinned by anincreased budget and improved skill mix of staff.Sexual health clinics for young people have extended opening hours, in addition tothe sexual health Locally Enhanced Service (LES) provided through General Practices inBattersea.Practice Based Commissioning clusters have approved and commissioned new services inareas such as obesity/weight management, sexual health, spirometry, anti-coagulation,diabetes, ECG and dermatology.24 practices are part of the PCT Extended Hours Local Enhanced Service (LES) schemeand are providing appointments outside of the core hours (8.00 – 6.30 pm Mon–Fri).The PCT is developing a Primary Care Strategy which will provide the direction for thedevelopment and commissioning of services.A series of service reviews within community service have been earmarked includinghealth visiting, school nursing and podiatry.3. Practices and services in strategic locationsSpecific attention has been given to location of new services within North <strong>Wandsworth</strong>,with discussions currently underway in Putney.4. Engage with the bulk of our population<strong>Wandsworth</strong> Primary Care Trust has earmarked new investment to develop a publicengagement strategy, with particular attention on the harder to reach groups i.e.commuters and those at work during the day.Chapter 3: Children and Young PeopleRecommendationActions1. Improve immunisation and breast feeding ratesAn immunisation action plan has been developed and presented to key strategicgroups and committees, such as the Overview and Security Committee, Primary CareTrust Management Team, Professional Executive Committee and Community ProviderManagement Team for discussion and approval. Additional funds have been madeavailable to support increased uptake.Breast feeding targets have been incorporated into Local Area Agreement priorities. Dropin clinics have been established in key geographical areas. Breast feeding and low birthweight initiatives have been explored specifically as part of wider action plans such asteenage pregnancy and smoking.<strong>Wandsworth</strong> Teaching Primary Care Trust 9
Chapter 1: <strong>In</strong>troduction<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table 1.3: Recommendations from Public <strong>Health</strong> Report 05/06 <strong>Health</strong> in <strong>Wandsworth</strong> (continued)Chapter 3: Children and Young PeopleRecommendationActions2. Tackle low birth weight rates in deprived wardsA maternity need assessment has been carried out, which included a particular focus onlow birth weight in deprived wards. As a consequence specific recommendations havebeen made for targeted action.3. Implement mental health promotion in schoolsAs part of the virtual health promotion group and the Personal, Social and <strong>Health</strong>Education agenda in schools (PSHE), schemes are being introduced to raise and tackleissues of low self-esteem. A ‘Feeling Good, Learning Well’ – Partnership ManagerConference raised the importance of ‘emotional literacy’ (mental health well being) for allthose involved in education.4. Review and strengthen school nursingA number of vacancies in school nursing are impacting on the service. The PCT ispursuing modular development courses for nurses in an effort to reach the national targetof one school nurse for each secondary school and for each cluster of primary schools.Chapter 4: Mental <strong>Health</strong>RecommendationActions1. <strong>In</strong>vest in mental health promotion staff and resources A new post is to be advertised for a specialist school nurse for adolescent mental health.<strong>In</strong> addition the funding for a mental health promotion post has been secured to workacross all services. Mental <strong>Health</strong> Graduate workers have also been appointed to work inthe primary care setting.2. Raise the importance of good mental healthWorld Mental <strong>Health</strong> day has been used as a vehicle to raise awareness in key settingssuch as schools, further education colleges, for particular Black and Minority EthnicGroups and for those with a learning disability.3.4.Improve knowledge and skills in primary carecommunity and voluntary settingsDevelop a comprehensive programme to maintain agood quality of life for mentally ill patientsMental health promotion resources have been provided to local agencies to increasecapacity to promote positive mental health. A range of training sessions has beendelivered which includes managing depression, conflict, loss and grief.Community Adolescent Mental <strong>Health</strong> and older persons needs assessments have beencompleted. An early years audit has also been undertaken to support service planningand the PCT has provided additional investment for Crisis Resolution and Home Treatmentservices.Chapter 5: Prison <strong>Health</strong>RecommendationActions1.Develop primary care, mental health and substancemisuse servicesCommissioned in reach primary care services have been put in place through theimplementation of a prison health plan.2. Improve communicable decease servicesA communicable disease committee has been established. Key achievements include:funding identified for a TB x-ray machine; flu pandemic plan; and training in place; bloodborne virus and sexual health programmes are being delivered.3. Improve data information systemThe prison has implemented a primary care data system. It is hoped this will help serviceplanning in the course of the next year.4. Establishment of a clinical governance systemA clinical governance structure has been put in place with representation from the PCT.10<strong>Wandsworth</strong> Teaching Primary Care Trust
2.Prevention of Disease in <strong>Wandsworth</strong>2.1<strong>In</strong>troductionThere have been considerable gains in the overallhealth status of the population in the UnitedKingdom. Life expectancy at birth has beenincreasing steadily and for 2003–05 was estimatedat 81.1 years for women and 76.9 years for men.<strong>In</strong>fant mortality rates have fallen to a current all timelow of 5.0 per 1000 live births. Premature mortalityfrom cardiovascular diseases and cancers has beensteadily declining in both men and women [1].Despite these improvements, significant healthchallenges remain. England has an increasingprevalence of adult and child obesity. South West<strong>London</strong> has a higher prevalence of obesity thanthe national and <strong>London</strong> average, and this isincreasing by more than double the national rates[1]. Premature mortality from chronic liver diseaseand cirrhosis is increasing, as is alcohol consumption.Even though mortality from cardiovascular diseaseand cancers is declining, these conditions are still themajor cause of morbidity and mortality.A recent <strong>London</strong> <strong>Health</strong> Observatory reportshowed that although mortality rates (Table 2.1) in<strong>Wandsworth</strong> have been decreasing, these decreasesare behind local delivery plan targets for 2005–08(except for female all age all cause mortality which isincluded here for comparison) [2].Table 2.1: Mortality Rates in <strong>Wandsworth</strong> 2003–05Age-standardised cancer mortalityrate in people
Chapter 2: Prevention of Disease in <strong>Wandsworth</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table 2.2: Economic Differences Between the Residential Wards in <strong>Wandsworth</strong>Extract from the Picture of <strong>Health</strong> (appendix 1)Latchmere Thamesfield <strong>Wandsworth</strong>Number (Measure) 1 Number (Measure) 1 Number (Measure) 1EconomicUnemployment, JSA claimant counts 2(% of resident working age population)405 (4.5%) 82 (0.8%) 4,215 (2.1%)Children
Chapter 2: Prevention of Disease in <strong>Wandsworth</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/072.32.3.1with 37% of CHD estimated to be attributable tophysical inactivity. There is also evidence that relativelyhigh levels of physical activity protect against cancers ofthe colon, breast and endometrium, and can indirectlyreduce the risk of developing other forms of cancer bymodifying weight gain and obesity.The risk factors described above are modifiable andprimary prevention through lifestyle and environmentalinterventions to reduce exposure to these risk factorsremains the main way to address them.Preventive Programmes in <strong>Wandsworth</strong>ObesityCurrently <strong>Wandsworth</strong> lacks full information onthe prevalence, distribution and health burden ofobesity for the <strong>Wandsworth</strong> population. The onlycomprehensive source is the height and weightmeasurement programme in schools, (Table 2.6);however it is known that people living in wards withthe highest number of unemployed adults withdependant children and people from black and ethnicminority groups are at greatest risk of obesity andrelated ill-health [5]. A series of activities have beenoccurring in <strong>Wandsworth</strong> over the last five years witha specific focus on the most deprived wards of theborough. The recent production of a five-year obesityprevention and management strategy has consolidatedthese activities, and will be the main driving force forfuture actions around obesity. The aim of the obesitystrategy is to halt the rise in prevalence of obesity inadults and children by 2010, and then maintain thislevel of overweight and obesity through a focus onboth prevention and management. The inclusion of anobesity initiative in the Commissioning Strategy Planreinforces the importance of these interventions for theimprovement of health.2.3.2teaching healthy eating and healthy living, establishingdiet and fitness groups, and the integration of diet andnutrition advice into other health advice sessions.• <strong>In</strong> recognition of the need to tackle this problemin young people a range of programmes has beendeveloped including baby-weight managementgroups for mothers, food and fitness policies innurseries and for childminders, helping schoolsto meet the national standards for school mealsand to have a whole school food policy, a weightmanagement service for overweight and obeseteenagers, cognitive behaviour therapy and briefmotivational advice, and a reward and recognitionscheme for grocery stores and restaurants toprovide and promote healthy foods.• To tackle obesity in adults and within the Borough,there is, in addition to the programmes mentionedabove, a weight wise programme for staff anda specialist multi-disciplinary community basedweight management service, dietician-led weightmanagement clinics and a range of physicalactivity schemes.SmokingWith an estimated adult smoking prevalence of31%, <strong>Wandsworth</strong> has a higher proportion ofsmokers than the national average, estimated at27%. Around 35% of deaths in people aged over35 are thought to be attributable to smoking, againabove the average for England.Public <strong>Health</strong> is committed to meeting the nationaltarget of reducing adult smoking rates to 21% orless by 2010, with a reduction in prevalence amongroutine and manual groups to 26% or less.The recent introduction of smoke free legislationis a significant public health advance. Locally jointwork with the Local Authority supported the smoothimplementation of the legislation, supported by stopsmoking advice for patients, employees and the public.The strategies employed in the stop smoking programmehave targeted different sections of the population:• The introduction of new drop-in clinics andincreased access to community advisors has helpedus reach younger smokers (20–44 years), who aremore mobile and are often resistant to traditionalmethods of health promotion in this field.Briefly, Public <strong>Health</strong> activities include the following:• The production and distribution of guidelines onweight management in primary care. Projects aimed at• <strong>In</strong> a recent survey 42% of <strong>Wandsworth</strong> pupilsclaimed to have tried smoking. Young peoplein the Borough have been specifically targetedby an ongoing media campaign, and a youthsmoking cessation project has provided training<strong>Wandsworth</strong> Teaching Primary Care Trust 13
Chapter 2: Prevention of Disease in <strong>Wandsworth</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table 2.5: Mental <strong>Health</strong> Service UtilisationExtract from the Picture of <strong>Health</strong> (appendix 1)Mental <strong>Health</strong>Hospital admissions under the “adult mental illness” speciality(rate per 100,000 population)People with a mental health problem helped to live at home(rate per 1,000 population)Community Mental <strong>Health</strong> Teams outpatient/community appointments(% of total appointments)Latchmere Thamesfield <strong>Wandsworth</strong>Number Measure Number Measure Number Measure56 (425.2) 9 (41.9) 661 (228.7)76 (7.25) 11 (0.92) 696 (3.02)6.0% 1.8% 100.0%Source: Clearnet activity 2005 and GL 2003 Round Population Projections: <strong>Wandsworth</strong> Borough Council: <strong>Wandsworth</strong> PCT: CMHTTable 2.6: Risk Factors for Ill <strong>Health</strong>Extract from the Picture of <strong>Health</strong> (appendix 1)Latchmere Thamesfield <strong>Wandsworth</strong>Number Number NumberObesity % Obese children in Reception 14.7% 8.1% 11.4%% Obese children in Year 6 18.8% 4.3% 19.6%Smoking Estimated prevalence of smoking in adult population 3,257 3,325 70,343LLTI % of people with Limiting Long Term Illness 17.5 9.5 13.4School height and weight programme WPCT: Smoking Epidemic in England 2004: Census 2001Figure 2.1: Ethnic Profile of Census 2001 Population, GP Population, A&E Attendances, Walk in Centre Attendances,Elective and Non Elective Admissions at St George’s Hospital100%White80%Mixed60%Asian orAsian British40%Black orBlack British20%0%Census 2001GPA&EWIC General FCE:(FY 2004/05) (July-September 2005) ElectiveGeneral FCE:Non ElectiveChinese orOther EthnicGroupNotstatedCensus 2001; Exeter 2005; local data (FCE Finished Consultant Episode)14<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 2: Prevention of Disease in <strong>Wandsworth</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07for youth workers, volunteers and peer advisors onpromoting and supporting quit attempts.• Joint working key partner support was required toensure enforcement of recent legislation prohibitingthe sale of tobacco products to under-18s.• Almost all of <strong>Wandsworth</strong>’s schools areparticipating in the National <strong>Health</strong>y Schoolsprogramme, which includes tobacco educationwithin its key themes.• Many vulnerable groups, including minority ethnicgroups, mental health patients, prisoners and thoseon low income, are known to have higher ratesof smoking and lower utilisation of mainstreamhealth services. A variety of health promotion andeducational interventions have been designed totarget the ‘hard to reach’ groups:–– Particularly high smoking prevalence ratesare seen amongst Bangladeshi (40%), Irish(30%) and Pakistani (29%) males. Examplesof interventions include ‘Stop Smoking DuringRamadan’ campaign and providing informationin a number of non-English languages.–– Mental health patients, who smoke twice asmuch as the general population, often want toquit smoking and can be successfully helped todo so. The innovative Smoke Free Minds projectprovides stop smoking support to staff andpatients within the SW <strong>London</strong> & St George’sMental <strong>Health</strong> NHS Trust.–– The Sure Start Stop Smoking Project bringsstop smoking support to low-income familiesin <strong>Wandsworth</strong> and stop smoking serviceshave been expanded in deprived wards.Prisoners at <strong>Wandsworth</strong> prison have alsobenefited from group support sessions aimedat helping them quit smoking.Partnership working is an important part of theactivities undertaken to address smoking. Localpartnerships have been formed with a variety ofsectors including local businesses, pharmacies andGPs. There has been a considerable increase in thenumber of trained pharmacists and stop smokingadvisors in GP surgeries. A new patient groupdirective has facilitated the provision of NicotineReplacement Therapy in pharmacies and more than2,100 smokers have accessed these services in thepast year with a steady increase in the number offour-week quitters.2.3.3Physical ActivityPhysical inactivity is a growing problem in theUK with serious public health consequences. The<strong>Wandsworth</strong> Public <strong>Health</strong> strategy to increasethe levels of physical activity amongst its residentsinvolves promoting the benefits of physical activityto healthcare professionals, whilst ensuring that theycan easily and confidently refer their patients forquality advice and appropriate opportunities.Medically stable patients with various conditions canparticipate in specialist gym-based sessions as partof the ‘GP Exercise on Referral Scheme’. Specialistsupport is available for patients with establishedcoronary heart disease at Cardiac Rehabilitationclasses, which is in line with recent national guidance.‘‘Staying <strong>Health</strong>y’’ is a successful project focusing onadults in the 20–44 age range, and aims to empowerthe community to adopt a healthier lifestyle and increaselevels of physical activity. There is growing evidence thatthe determinants of adult cardiovascular disease are laiddown early in life and that children with lower levelsof physical activity are more likely to have risk factorsfor cardiovascular disease. Providing opportunities foryoung people to be physically active and promotingthe benefits of physical activity is a key theme in theNational <strong>Health</strong>y Schools programme, in which nearly all<strong>Wandsworth</strong>’s schools are participating.The benefits of physical activity for older people appearto be just as strong as they are in middle age and thereis strong evidence that those who exercise have fewercardiovascular events compared with their less activecounterparts. Physical activity maintained throughoutthe lifetime may be particularly important at preventingsome forms of cancer. The Older Active Person projectoffers activity sessions targeted at the over 50s withthe aim of increasing the number of older peopleparticipating in regular exercise. The PCT has alsoworked with the housing department to train Housingofficers to lead chair based exercise classes for olderpeople in sheltered accommodation. Other activitiesaimed at older people include falls and injury preventionclasses, group walks, line-dancing classes and Tai Chi.<strong>Wandsworth</strong> Teaching Primary Care Trust 15
Chapter 2: Prevention of Disease in <strong>Wandsworth</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/072.42.5The Impact of <strong>In</strong>equalitiesReducing health inequalities is a key area of workwithin public health. Many people, although notpoor, fail to realise their full potential for betterhealth. It has recently been suggested that exposureto risk factors accumulates throughout life andincreases the risk of illness and premature death. Thisexposure is greater in more disadvantaged groupsand appears to be the main explanation for theobserved differences in health and life expectancyby socioeconomic status. Tackling these major riskfactors therefore offers an opportunity not only toincrease life expectancy in all countries but to reducethe differences between groups or regions [3, 4].The risk factors we have considered above do occurin combination. <strong>In</strong> fact the diseases of lifestyle oftenrequire the presence of more than one risk factor [3].As a result the impact of any individual risk factorcan be difficult to estimate. The multi-causal natureof these diseases means that tackling the major risksshould have an impact on several outcomes or diseases.Ethnicity and <strong>In</strong>equalities<strong>London</strong> has the largest number of people in all ethnicminority groups, except for the Pakistani group. Wealready know that there are ethnic inequalities inhealth. People from most ethnic minority groups aregenerally more deprived in terms of socio-economicstatus. The Pakistani, <strong>In</strong>dian, Bangladeshi and mixedWhite and Asian groups have higher mortality ratesdue to circulatory disease and a higher than averageproportion of admissions due to coronary heartdisease. There is a high prevalence of diabetes inthe Asian, Black Caribbean and Black ‘other’ groupsin most regions. These national patterns are alsoreflected in the <strong>Wandsworth</strong> population. <strong>In</strong> additionwe have found that young Asian women have ahigher prevalence of mental health problems thanyoung White women of the same age; and that Blackand minority ethnic groups have worse sexual healththan the general population.Some of these known differences are reflected inthe utilisation of primary and secondary servicesby ethnicity. The ethnic profile of the residents of<strong>Wandsworth</strong> from the Census in 2001, does notmatch the profile of any of the health servicesprovided to it. There are two data warnings:1.Data from secondary care (elective and nonelective)should be treated with caution due tothe high numbers of not stated ethnicity.2.62.72.The ethnicity given in the GP data is an estimate, it isbased on an application of the ethnicity given in thecensus for each postcode, which is then mappedagain the postcode as registered in primary care.Two observations are apparent:• Differences in ethnicity may be explained by theage and sex profiles of each group, for examplethe black population may be older, or more proneto illness, than the younger white population.• Differences between ethnic profiles for electiveand non-elective admissions show that a higherproportion of black and black British patients areseen as elective (pre-arranged) admissions thannon-elective (emergency) admissions. The converseis true for patients from a mixed ethnic group.Recognising these ethnic differences in health andin the prevalence of risk factors for the commonestcauses of death, Public <strong>Health</strong> has targeted theseethnic groups using particular programmes asdescribed above; including ‘Stop smoking duringRamadan’ campaigns, ‘Staying <strong>Health</strong>y’ eventsoccurring in mosques, and translation of healthpromotion material on healthy eating, diabetes andsexual health into several languages. <strong>In</strong> addition publichealth is working with local primary care clinicians andpatient groups to explore differences in prescribing andadherence to medication for cardiovascular disease.Population Wide and High Risk<strong>In</strong>dividual Prevention ApproachesMany of these health risks are widely distributed inthe population, and people are at varying levels of riskfrom these conditions. Some prevention strategiesfocus on high risk individuals who are more likely todevelop disease or complications from the risk factor.However a much larger proportion of the populationwill have low to moderate levels of risk and preventionstrategies aimed at this group have a smaller impacton the individual but a much larger effect at thepopulation level; the so called ‘prevention paradox’.There needs to be a balance between the populationwide and the high risk approaches [4].Estimates of Avoidable Disease BurdenEstimating the impact of disease preventionprogrammes on the burden of disease is difficult.Ezzati estimated that the leading risk factors indeveloped countries 1 were responsible for 35% of1 These factors for developed countries include high blood pressure, highcholesterol, high BMI, low fruit and vegetable intake, physical inactivity,tobacco, alcohol, childhood sexual abuse, indoor smoke from solid fuels,illicit drugs, occupational risk factors for injuries.16<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 2: Prevention of Disease in <strong>Wandsworth</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07the total burden of disease in Western Europe in2000; however only a portion of this attributablerisk is truly avoidable [3]. What this does show isthat even countries with high healthy life expectancycould benefit considerably from risk reduction.The World <strong>Health</strong> Report 2002 provided estimatesof the population level impact of a 25% reductionin several risk factors from their current levels [4].Table 2.8 is the estimated avoidable disease burdenattributed to these risk factors. As these estimates areat a global level, the likely avoidable disease burden inindustrialised countries is probably much higher.Table 2.8: Estimated Avoidable Global DiseaseBurden after 25% Risk Factor DistributionalTransition from 2001Risk factor2010(% total)2020(% total)Blood pressure 1.7 1.9Tobacco 1.2 1.5Cholesterol 1.1 1.2Alcohol 1.1 1.1Overweight 0.9 1.0Low fruit and vegetable intake 0.6 0.6Physical inactivity 0.4Source: World <strong>Health</strong> Report 2002There is a substantial amount of work in mentalhealth occurring in the borough. Mental disordershave been shown to be independently associatedwith a substantial excess in all-cause mortalityrisk and people with mental health disorders havebeen shown to be less likely to access the requiredcardiovascular disease treatments [6]. Mental healthis a difficult subject to accurately measure, Table 2.9illustrates the data more readily available.World Mental <strong>Health</strong> Day PromotionSeveral studies have highlighted the high prevalenceof less severe forms of mental illness and a need fora focus on mental well being. A measure that wouldbenefit local planning would simply be the numberof patients visiting a primary care professional withdepression. The European Study of the Prevalence ofMental Disorders in Europe estimated the 12 monthprevalence of mood, anxiety and alcohol disordersin six countries in Europe including the UK to be aweighted percentage of 1.2%.The Office of National Statistics Survey in 2000,‘Psychiatric morbidity among adults living in privatehouseholds’, determined the most prevalent neuroticdisorder in the population was mixed anxiety anddepressive disorder at 88 cases per 1000 population.The numbers estimated for some form of neuroticdisorder are far higher, with estimates beingapproximately 1,800 in each ward.Extremes of mental health treatment such as psychosesand admissions to hospital are easier to quantify.Table 2.9 illustrates the stark difference between theleast deprived ward and the most deprived wards inTable 2.9: Measures of Mental <strong>Health</strong> in <strong>Wandsworth</strong>Extract from the Picture of <strong>Health</strong> (appendix 1)Latchmere Thamesfield <strong>Wandsworth</strong>Number (Measure) 1 Number (Measure) 1 Number (Measure) 1Mental <strong>Health</strong> Adults (16–74) suffering from some form of neurotic disorder 1,634 1,667 35,264Hospital admissions under the “adult mental illness” speciality(rate per 100,000 population)People with a mental health problem helped to live at home (rate per1,000 population)Community Mental <strong>Health</strong> Teams outpatient/community appointments(% of total appointments)56 (425.2) 9 (41.9) 661 (228.7)76 (7.25) 11 (0.92) 696 (3.02)6.0% 1.8% 100%1 Rates per 1,000 populationSource: Clearnet activity 2005 and GL 2003 Round Population Projections, <strong>Wandsworth</strong> Borough Council, <strong>Wandsworth</strong> PCT CMHT<strong>Wandsworth</strong> Teaching Primary Care Trust 17
Chapter 2: Prevention of Disease in <strong>Wandsworth</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/072.8<strong>Wandsworth</strong>. Additionally the numbers of people witha mental health problem helped to live at home, andthe contacts made through the community mentalhealth teams, are both more heavily concentrated onthe more deprived.A range of other activities, as described in otherchapters of this report, will contribute to a reductionin cancer and cardiovascular deaths. Examplesof these include elements of the sexual healthstrategy, immunisation programmes and screeningprogrammes for cancer of the cervix and breast.Recommendations1. To continue to invest heavily in risk preventionin order to contribute substantially to futureavoidable mortality.2. A broad spectrum of activities needs to addressboth population level initiatives and moretargeted initiatives, and these componentsneed to be incorporated into all commissioningarrangements through the PCT.References[1] Department of <strong>Health</strong>. <strong>Health</strong> Improvement AnalyticalTeam – Monitoring Unit. <strong>Health</strong> Profile of England 2007.TSO: <strong>London</strong>, 2007.[2] <strong>London</strong> <strong>Health</strong> Observatory. <strong>London</strong> Public <strong>Health</strong>Performance Management Report. Quarter 12007/08. 2007.[3] Ezzati M, Vander Hoorn S, Rodgers A et al. Estimates ofglobal and regional potential health gains from reducingmultiple major risk factors. Lancet 2003; 362: 271–80.[4] World <strong>Health</strong> Organisation. World <strong>Health</strong> Report 2002.Reducing risks, promoting healthy life. 2002.[5] <strong>Wandsworth</strong> NHS Primary Care Trust. Obesity StrategyImplementation Group. Obesity prevention andmanagement strategy for <strong>Wandsworth</strong>: 2005–2010.2006.[6] Prince M, Patel V, Saxena S. No health without mentalhealth. Lancet 2007; 370: 859–77.With thanks to Anu Garrib18<strong>Wandsworth</strong> Teaching Primary Care Trust
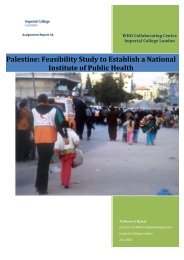
3.Addiction3.1Definition and ScopeAddiction is a term used to describe a person’sphysical and psychological dependency on anactivity, drink or drug, (seemingly) beyond consciouscontrol. Addiction is said to occur when there is: astrong desire to engage in the particular behaviour;discomfort and/or distress when the behaviour isprevented or ceased; persistence of the behaviourdespite clear evidence that it is leading to problems.Addictions can be formed to any activity orbehaviour which allows a person to escape from lifeand its problems. Examples of addictions includegambling, use of prescribed or illegal drugs, alcohol,sexual activities and food. <strong>In</strong> this chapter, alcohol,drug and gambling addictions will be discussed asthese addictions pose a major threat to the health of<strong>Wandsworth</strong>’s population.3.2<strong>Health</strong>, Social and Economic Impact ofAlcohol AddictionAlcohol consumption is responsible for increasedillness and death. Research has shown that alcohol iscausally related to more than sixty different medicalconditions. Alcohol misuse is a contributory cause toall circulatory diseases such as hypertension, strokeand heart diseases. Prolonged heavy drinking isknown to be the main cause of liver cirrhosis, chronicliver disease and acute pancreatitis. The <strong>Health</strong>Profile of England (2007) [2] shows that prematuremortality from chronic liver disease and cirrhosis hasrisen persistently in England, from the lowest in theEU in 1970 to almost the average in the EU in 2004.Alcohol has huge consequences on attendancesat accident and emergency departments, alcoholrelated admissions into hospital and ambulancecallouts. There were 26,910 alcohol relatedcallouts in <strong>In</strong>ner <strong>London</strong> (21% of all calls) and23,298 in Outer <strong>London</strong> (16% of all calls) in2001–03 [3]. <strong>In</strong> <strong>Wandsworth</strong> there were 1,642callouts related to alcohol, about 19% of allcallouts and the most common reason for calloutsapart from chest pain.Alcohol related deaths are rising nationally and in<strong>Wandsworth</strong>. The number of deaths attributable toalcohol in the period 2002–04 for <strong>Wandsworth</strong> was178 in males and 126 in females. Figure 3.1 belowshows standardised mortality ratios for chronicliver disease for <strong>Wandsworth</strong> registered patients incomparison with other boroughs which have similarsocio-economic characteristics.Source: NHS photo library<strong>In</strong>creasingly, alcohol misuse by a small minority iscausing two major and largely distinct problems;crime/anti-social behaviour and harm to health asa result of chronic and binge drinking. The PrimeMinister’s Strategy Unit (2003) [1] calculated thatalcohol related harm is costing around £20 billiona year, and that some of the harms associated withalcohol are getting worse. Following a rise in the1970s, the level of pure alcohol consumed by adultsin the United Kingdom remained relatively constantthroughout the 1980s and 1990s, but is once againrising and now exceeds the average levels of alcoholconsumed by EU countries.According to the General Household Survey [4] andthe Alcohol Needs Assessment Research Project(ANARP) [5] about 35% of men and 20% of womenwere more likely to drink above sensible limits in2005. Based on these figures, in <strong>Wandsworth</strong> weestimate that approximately 32,000 men and 22,500women drink above sensible levels.The National Centre for Social Research carried out astudy based on modelled estimates on the prevalenceof binge drinking. The study showed that <strong>Wandsworth</strong>has the highest percentage of binge drinkers (21.1%)compared to <strong>London</strong> (15.4%) and England (18.2%).These estimates are based on small numbers and mustbe interpreted with caution.The alcohol needs assessment research project (ANARP)estimated that 3.6% of people in England and 5% ofthe population of <strong>London</strong> are dependent on alcohol.Based on this it is estimated that in <strong>Wandsworth</strong> around14,000 people are dependent on alcohol.<strong>Wandsworth</strong> Teaching Primary Care Trust 19
Chapter 3: Addiction<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table 3.1: Alcohol UnitsAlcohol drinkUnitsOne pint of ordinary strength lager 2One pint of strong lager 3One pint of ordinary strength bitter 2175ml glass of red or white wine – small glass 2Source: NHS photo libraryUpdated Government advice is based on recommendeddaily rather than weekly amounts of alcohol intake. Therecommendations are that men should not regularlydrink more than 3–4 units of alcohol per day, andwomen should not regularly drink more than 2–3 unitsof alcohol per day. After an episode of heavy drinkingit is advisable to refrain from drinking for 48 hoursto allow your body to recover. By the end of 2008the government expects all alcoholic drinks labels toinclude alcohol unit information. The Department of<strong>Health</strong> also advises that pregnant women or womentrying to conceive should avoid drinking alcohol. If theydo choose to drink, to minimise the risk to the babythey should not drink more than one to two units ofalcohol once or twice a week. A description of whatconstitutes a unit of alcohol is shown in Table 3.1.An alcopop 1.5A pub measure of spirits 1Source: Department of <strong>Health</strong> 2007Recent information on consumption of alcoholin <strong>Wandsworth</strong> school-aged children is currentlyunavailable. However the “<strong>Wandsworth</strong> surveyof smoking, drinking and drug use amongschoolchildren, 2004” found that the prevalenceof frequent drinking, that is pupils drinking at leastonce a week, is substantially lower in <strong>Wandsworth</strong>(7%) than the prevalence reported at national level(18%). This survey is due to be repeated this year.It is well established that there is a strong correlationbetween alcohol misuse and crime. It is associatedwith different types of offences, including domesticand other forms of violence, sexual assault anddrink driving. The local alcohol profiles for Englandproduced by the North West Public <strong>Health</strong>Figure 3.1: Standardised mortality ratios for chronic liver disease including cirrhosis:<strong>Wandsworth</strong> and comparator boroughs, 2004–2006.200Standardised mortality ratios15010050FemalesMales0<strong>Wandsworth</strong>CroydonEalingEnfieldHammersmithand FulhamHounslowLambethLewishamSource: Compendium of Clinical and <strong>Health</strong> <strong>In</strong>dicators, 2007Boroughs20<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 3: Addiction<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Observatory (NWPHO) [6] estimated that 3,444 casesof crime in <strong>Wandsworth</strong> were attributable to alcoholin 2005/6. Alcohol misuse is associated with manytypes of violence. <strong>In</strong> 2005/6 there were 6,139 cases ofviolence against the person in <strong>Wandsworth</strong> (Source:British Crime Survey). 2,271 cases of violence againstthe person were attributable to alcohol accordingto the local alcohol profiles. <strong>In</strong> the same period, 507incidences of domestic violence were reported to thepolice in <strong>Wandsworth</strong> (Source: P78 Police Service).Anti-social behaviour can be described as any activityby an individual that impacts on other people ina negative way. The risk of anti-social behaviouris increased by the use and availability of alcoholand drugs. Anti Social Behaviour Orders (ASBOs)are being handed out to tackle this problem and in<strong>Wandsworth</strong> so far 81 have been issued.Drink driving occurs when an individual drives underthe influence of alcohol. <strong>In</strong> the United Kingdom, thepresent limit for driving whilst under the influenceof alcohol is 80mg/100ml blood. <strong>In</strong> <strong>Wandsworth</strong>in 2005/6 there were 520 arrests for being unfit todrive due to alcohol, testing positive for excessivealcohol or refusing to take a breath test, a slightdecrease from 540 in 2004/5.risks from taking cocaine include increased bloodpressure, irregular heartbeats and increases in bodytemperature. Long-term use of cocaine can lead toextreme paranoia, depression, insomnia, weight lossand impotence in men. As well as having immediatehealth risks, some drugs can be addictive and leadto long-term damage to the body. Heavy or longtermuse of some illegal drugs may cause the user tooverdose, which may cause permanent damage to thebody and can be fatal. The injection of drugs presentsanother set of risks. Sharing needles increases the riskof contracting serious diseases such as Hepatitis B,Hepatitis C and HIV. Long-term injecting of opiatesmay cause collapsed veins, appetite loss and severeconstipation.Table 3.2: Number of <strong>In</strong>jecting drug users newlydiagnosed with HIV, resident in <strong>Wandsworth</strong>,2003-3005Year Males Females Total2003 14 6 202004 11 5 162005 11 6 173.3<strong>Health</strong>, Social and Economic Impact ofDrug AddictionThe social and economic costs of drug misuse in theUK are estimated at between £10 billion and £18billion a year, 99% of which is due to problematicdrug users. Around four million people use at leastone illicit drug each year and around one millionpeople use at least one of the most dangerous orClass A drugs such as ecstasy, heroin and cocaine. Itis the problematic drug users, usually those whosedrug use consists of, “illicit opiates, crack-cocaine orbenzodiazepines,” who cause considerable harm tothemselves and others. We must therefore continueto work with our most damaged communities,particularly those living within our deprived wards,concentrating on preventing and treating problematicdrug use, if we are to be successful in reducing theharm caused by drug use.Taking illegal drugs carries many serious health risks.Many illegal drugs may have been imported fromdifferent countries around the world, resulting in thembeing processed and handled by a number of differentpeople and potentially mixed with other unknownsubstances to increase quantities. Different drugshave different health risks which can be immediateand long term. For example, the immediate healthSource: <strong>Health</strong> Protection Agency, 2004–2006Drug abuse, like alcohol, has consequenceson attendances at Accident and Emergencydepartments and ambulance callouts. During theperiod 2002–04 there were 1,070 ambulancecallouts for drug overdoses in <strong>Wandsworth</strong>. Datafrom the <strong>London</strong> <strong>Health</strong> Observatory shows thatthe number of drug misuse deaths in <strong>London</strong>[7] has declined from a peak of 303 in 1998 to150 in 2003, a reduction of just over 50%. <strong>In</strong><strong>Wandsworth</strong>, the data reflects this declining trend.There was a statistically significant decline in agestandardised drug misuse death rates betweensix time periods. The rate was 3.4 for the period1994–1998 and 1.9 for the period 1999–2003. <strong>In</strong>England, the number of deaths due to drug misuseincreased from 1993 until 2000 (from 821 to 1,565)and then decreased in 2001 to 1,528, continuingto decrease in the following two years to 1,181in 2003.<strong>Wandsworth</strong> Teaching Primary Care Trust 21
Chapter 3: Addiction<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Source: acc.tv.comNo accurate local data is available regarding illegalbehaviour relating to drug abuse. However, theprevalence of common forms of drug use can beobtained from population surveys, such as the BritishCrime Survey carried out by the Home Office in 2000[8]. Table 3.3 illustrates the estimated number of16–29 year olds in <strong>Wandsworth</strong> who had used anydrug, Class A drug, Cocaine, Heroin or Hallucinatesin the last year and last month.Table 3‐3: Estimated Number of 16–29 year oldsin <strong>Wandsworth</strong> Using Various Drugs in the LastYear and Last Month (as reported in 2000)Last yearLast monthAny drug 22,466 15,943Class A 10,146 4,348Cocaine 8,696 2,899Heroin
Chapter 3: Addiction<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/073.5problems, and gambling was correlated withdepression.The Gambling Act 2005 [16] has been designedto control all forms of gambling. It will transferauthority for licensing gambling from magistrates’courts to local authorities. The objectives of the Actare as follows:• Preventing gambling from being a source ofcrime or disorder, being associated with crime ordisorder or being used to support crime• Ensuring that gambling is conducted in a fair andopen way• Protecting children and other vulnerable personsfrom being harmed or exploited by gambling.ConclusionThis chapter has highlighted some of the problemsour population faces with regard to alcohol, drugsand gambling. The alcohol health needs assessment,which was carried out in 2007 by the public healthdepartment in partnership with the council, producedan effective strategy to tackle the problem of alcoholmisuse. This encompassed all the different types ofdrinkers, binge, harmful/hazardous and dependent.This strategy must be implemented in order to protectpeople from the harms of alcohol and prevent themfrom becoming dependent. Our population must beeducated on what constitutes sensible drinking andharm reduction, in order to reduce adverse healthconsequences from alcohol misuse. Delivering briefinterventions in the community or in a primary caresetting may help us to achieve this. Further workand needs assessments should be carried out aroundgambling and drug abuse in our population. This workwill enable us to implement additional strategies,targeting individuals who have been affected by theseaddictions and prevent those who are at risk frombecoming addicts.3.6Recommendations1. To develop alcohol awareness programmes forvulnerable groups such as pregnant women, youngpeople and for particular groups of binge drinkers.2.3.4.To raise awareness of sensible drinking limits withkey partner organisations.Develop health promotion initiatives to addressmental health problems associated with gambling.<strong>Health</strong>care Partnership Group to assess the effectof the changes in gambling legislation.5. Continue to work with vulnerable groups to raiseawareness of the seriousness of illegal drugs,their danger to health, and as a cause of death.6. Action plan by the harm reduction group toincrease awareness and co-ordinate services forthose with addiction problems.7.<strong>Health</strong>y schools programme to increaseawareness of addiction issues amongst children.With thanks to Melissa Cottington<strong>Wandsworth</strong> Teaching Primary Care Trust 23
Chapter 3: Addiction<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07References[1] Prime Minister’s Strategy Unit. Alcohol HarmReduction Strategy for England. 2004.[2] <strong>Health</strong> Profile of England 2007, Department of<strong>Health</strong>. 2007.[3] <strong>London</strong> <strong>Health</strong> Observatory. Ambulance call-outs2001–2003. 2004.[4] Office for National Statistics. General Household survey:smoking and drinking among adults. 2005.[5] Department of <strong>Health</strong>. Alcohol Needs AssessmentResearch Project (ANARP): The 2004 national alcoholneeds assessment for England. TSO: <strong>London</strong>, 2005.[6] North West Public <strong>Health</strong> Observatory. Local AlcoholProfiles for England. 2006.[7] Deaths Due to Drug Misuse in <strong>London</strong>: Data fromthe Office of National Statistics up to 2003, Reportprepared by Peter Madden and Charlotte Fellows,January 2006. Available at: http://www.lho.org.uk/viewResource.aspx?id=10128[8] Home Office. British Crime Survey. 2000.[9] Hickman M, Stimson G, Howe S, Farrell M, Taylor C, CoxS et al. Estimating the prevalence of problem drug usein <strong>In</strong>ner <strong>London</strong>: a discussion of three capture-recapturestudies. Addiction, 1999, 94(11): 1653–62[10] Home Office Drugs Strategy Directorate. National DrugStrategy. 2002.[11] Middleton, J., Latif, F. Gambling with the nation’shealth, British Medical Journal, 2007, 334(7598), 828[12] Stitt BG, Nicholas M, Giacopassi D., Does the presenceof casinos increase crime? Crime and Delinquency,2003, 49(2): 253–284[13] Topp J, Sawka E, Room R, Poulin C, Single E, ThompsonH. Policy discussion paper in problem gambling.Ottawa: Canadian Centre on Substance Abuse, 1998.[14] Rodda, S, Brown, S,L & Phillips, J,G., The relationshipbetween anxiety, smoking, and gambling in electronicgaming machine players, Journal of Gambling Studies,2004, 20 (1): 71–81[15] Stuhldreher, W,L, Stuhldreher, T,J & Forrest, Y–Z, K.,Gambling as an emerging health problem on campus,Journal of American <strong>College</strong> <strong>Health</strong>, 2007, 56 (1):75–88[16] Department of Culture, Media and Sport. GamblingAct. TSO: <strong>London</strong>, 2005.24<strong>Wandsworth</strong> Teaching Primary Care Trust
4.Maternal <strong>Health</strong>4.1Births and Mortality.Maternal health typically relates to the femalepopulation aged between 15 and 44, and includesinfant mortality and low birth weight. Over thelast three years, the impact of an increasing femalepopulation has resulted in rising numbers of birthswithin the Borough of <strong>Wandsworth</strong> as a whole andat residential ward level.During 2004, 4102 births were recorded to residentsof <strong>Wandsworth</strong> and by 2006 this had increased to4687. <strong>Wandsworth</strong> PCT is responsible for servicesdelivered to those children that are registered with a<strong>Wandsworth</strong> GP, this represents a slightly differentpopulation which in 2007 was 4,108. The highestproportions of births occurred mainly within ourmost affluent communities but also within two ofour least affluent communities. These two differingcommunities have specific needs, experiencedifferent birth outcomes and make differentdemands on services.The fertility rate varies considerably within the borough.During 2006, this ranged from 23.62 live births per1,000 females aged 15–44 years in Tooting to 78.83live births per 1,000 females aged 15–44 years inNorthcote during 2006. This means that in the periodof one year when compared to Tooting, three timesmore births occurred in the ward of Northcote.<strong>In</strong>fant mortality has shown a substantial decreasein England and Wales over the last quarter of thetwentieth century, largely as a result of fallingneonatal mortality over the period. Improvementsin the general health of women, general medicaladvances, reduction in the number of illegal abortionstogether with improvements in standards of obstetricand anaesthetics care have all contributed to a majordecline in maternal and infant mortality. However,unacceptable inequalities in infant mortality stillremain. A key proxy indicator for infant mortality isthe number of Low Birth Weight babies (LBW). During2004–2006 the proportion of LBW in the boroughwas 6.9%. <strong>Wandsworth</strong> reports one of the lowestLBW proportions in <strong>London</strong> (LHO). <strong>In</strong>equalities havebeen shown to exist in birth outcomes related to lowbirth weight, associated with socio-economic position,age and ethnicity characteristics in <strong>Wandsworth</strong>.Figure 4.2 demonstrates that the least affluentwards in the borough experience higher proportionsof LBW births. For Latchmere and Tooting, duringthe period of 2004–2006, this was at a statisticallysignificant level.There is evidence that local efforts which havefocused on families from our most economicallydisadvantaged areas have had an impact and haveprevented a higher overall increase in the numbers.Whilst the recording of birth weight is mandatory,recording of ethnicity is still very poor. This needs toimprove so that inequalities related to ethnicity canbe more effectively monitored and addressed.All stakeholders who work to improve maternaland infant health within the NHS have a centralpart to play in addressing these inequalities. Table4.1 demonstrates what a significant contributionall these stakeholders make to addressing a largenumber of the Department of <strong>Health</strong>’s Public ServiceAgreement (PSA) targets by improving and targetingservices to those pregnant women most in need.Figure 4.1: Number of Births by Ward, 2004–06BalhamBedfordEarlsfieldEast PutneyFairfieldFurzedownGraveneyLatchmereNightingaleNorthcoteQueenstownRoehamptonShaftesburySouthfieldsSt Mary’s ParkThamesfieldTooting<strong>Wandsworth</strong>CommonWest HillWest Putney0 50 100 150 200 250 300 3502004Source: Office for National Statistics20052006<strong>Wandsworth</strong> Teaching Primary Care Trust 25
Chapter 4: Maternal <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table 4.1: Contribution Maternity Services can make to Public Service Agreement TargetsPSA TargetContribution from maternity careSubstantially Reduce Mortality Rates:…from heart disease and stroke…from cancer…from suicideGood maternity care promotes and sustains breastfeeding. Breastfed infants are at reduced risk ofcoronary heart disease throughout life and have lower average blood pressure in later life. Babies bornat low birth weight (
Chapter 4: Maternal <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/074.2Tackling Mortality and Low Birth Weight<strong>In</strong>fant mortality rates can most successfully betackled by addressing the influencing factors andaddressing child poverty.The most vulnerable groups are defined as thoseexpectant and new mothers:• Who are under 20 or over 40 years old,• Who do not speak English as their first languageor who have a an ethnic background which is notwhite British,• Who live in areas considered to the most deprivedin the Borough.Actions which will have the most impact onreducing the <strong>In</strong>fant Mortality Rate (IMR) further in<strong>Wandsworth</strong> are those that focus on addressing theinequalities in health outcomes in the following areas:• Targeting the reduction in the number of LowBirth Weight (LBW) births in vulnerable groups.• Supporting pregnant mothers and fathers invulnerable groups to stop smoking.• Reducing the number of pregnant women invulnerable groups booking late for maternity care(>12 weeks).• <strong>In</strong>creasing the number of women from vulnerablegroups who breastfeed at birth and for up to 6–8weeks after.During the period of 2003–2005, the IMR for<strong>Wandsworth</strong> was 4.5 per 1,000 live births which isless than the reported rates for England and <strong>London</strong>.However, a recent maternity needs assessment,conducted by the Public <strong>Health</strong> Department,identified that inequalities do exist in <strong>Wandsworth</strong>in relation to those factors that influence IMR. Table4.2 illustrates the differences between Thamesfieldward, and Latchmere ward in the number of birthsto mothers under the age of twenty, and the numberof births where the weight was under 2.5 kilograms.Table 4.2: Maternity Patterns between Least andMost Deprived Wards in <strong>Wandsworth</strong>Children (number)Latchmere Thamesfield(most deprived) (least deprived) <strong>Wandsworth</strong>Total Births, 2007 248 193 4,108Births to women
Chapter 4: Maternal <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/074.2.14.2.2SmokingYounger women and those who belong to lowersocio-economic groups were more likely to besmokers before pregnancy and were less likely togive up when they are pregnant.The current proportion of pregnant women who smokein <strong>Wandsworth</strong> is 6.8%. To support effective targetingof services, recording and monitoring of smoking statusneeds to be improved to include variables such as socioeconomic,age and ethnicity status.Fertility data indicates that Latchmere ward has oneof the highest fertility and teenage conception ratesin the borough. It could therefore be prudent forpregnant women in this ward to be targeted to makemost progress in reaching the LDP target.Late Access to Maternity ServicesLate access to services after 12 weeks gestation canbe an important indicator of poor accessibility ofservices and can result in health inequalities in birthoutcomes. It is important that women access servicesearly to ensure full maternal care is provided toimprove health outcomes for both mother and child.A person who accesses maternity services after 12weeks is considered a late booker.Figure 4.3: Proportion of Young MothersWho Book Late72%book lateSource: St George’s Hospital, January – November 200728%book early• Treatable health problems in the mother that canaffect the baby’s health, such as Blood Borne Viruses• Characteristics of the baby, including size, sex, age,and placement in the uterus• The chance that a baby has certain congenital,genetic, or chromosomal problems (screening)• Certain types of foetal abnormalities, includingheart problems (diagnostic)It has been suggested that there are four reasons forvariations in access to health care:1. Availability: health services may not beavailable to some population groups2. Quality: quality of services may vary betweenpopulation groups3. Costs: health services may impose personalcosts which vary between population groups,such as time off work for an appointment, orpublic transport4. <strong>In</strong>formation: for some population groups,there may be lack of clarity of what healthservices are on offer.Some categories of women and families areunlikely to get the maternal care they require unlessservices adapt to meet their needs, such as use ofinterpreters, access to advocates, and/or healthprofessionals proactively directing women to thecare on offer.Although late booking data is collected by serviceproviders there is no current requirement forthis to be reported, although the local authorityis recommending this becomes a Local AreaAgreement target in the future.To demonstrate if there is any evidence ofinequalities locally, a small study analysed bookingdates for expectant mothers less than 20 yearsold. This analysis found that of those 46 expectantteenagers booked to deliver at St Georges duringJanuary and November 2007, 72% booked after 12weeks gestation and were found to have an averagegestation of 15 weeks at time of booking. (Figure 4.3).It is important for women to access services atan early stage of their pregnancy to ensure thatimportant screening can take place and advice canbe given.Prenatal tests normally are conducted between10–14 weeks gestation and can identify a number ofcharacteristics about the unborn child:28<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 4: Maternal <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/074.2.3Breastfeeding4.3RecommendationsEvidence shows that breastfeeding is the bestmethod for feeding babies. Breast milk providesall the energy, liquid and nutrients the baby needsfor growth and development. At birth and at 6–8weeks, breastfeeding rates in <strong>Wandsworth</strong> are 79%and 62% respectively and have passed the targetsset for the PCT.1. It is important that women access services early(ideally before 12 weeks gestation) to ensurefull maternal care is provided to improve healthoutcomes for both mother and child.2. To decrease the number of LBW births at anindividual level, smoking cessation should bestrongly promoted by all health professionals andservices made easily accessible to provide support.Source: heelpress.com, painted by Liz Smith3.4.5.6.7.Useful information is collected by <strong>Health</strong> Visitors.If the return rate of the eight-week assessmentform to the Child <strong>Health</strong> records department wasimproved which included a record of smokingin the home status, the child health recorddepartment could begin to analyse and report onthis data.Breastfeeding rates at 6–8 weeks after birth arecollected by <strong>Health</strong> Visitors but the return rateof these forms to the PCT is currently poor. Itis important that the response rate using thisestablished reporting mechanism is improved toenable correct reporting, effective monitoringand targeting of services.Routine local analysis on breastfeeding is collated,but the age of a breastfeeding or bottle feedingmother needs to be added to the data set.<strong>Health</strong> promotion services for which there isevidence of effectiveness should be providedand agreed in Service Level Agreement with allproviders.It is recommended that the Maternity Servicesself assessment tool is used to direct the PCTto annually review maternal data to addressinequalities segmented by age, gender, ethnicityand location.With thanks to Jo-Anne Alner<strong>Wandsworth</strong> Teaching Primary Care Trust 29
5.5.1Sexual <strong>Health</strong>We cannot afford not to invest in sexual healthDefinition and ScopeSexual health is an important part of physicaland mental health. It impacts upon our identityas human beings together with the fundamentalhuman rights to privacy, a family life and living freeof discrimination and prejudice. Essential elementsof good sexual health are equitable relationshipsand sexual fulfilment with access to information andservices to avoid the risk of unintended pregnancy,illness or disease (The National Strategy for Sexual<strong>Health</strong> and HIV: 2001).Sexual health includes a number of important elements:• Prevention and treatment of sexually transmittedinfections (STIs)• Preventing unintended pregnancy and unsafe abortionassociated with preventable infertility and pelvicinflammatory disease.Sexual ill health is an important public health issuelinked to poverty, poor housing, unemployment andsocial exclusion. With sexual risk taking behaviour onthe increase, consequences of poor sexual health are:• Social costs – significant social costs arise fromthe growth in sexual health need. The burden ofsexual ill health is not equally distributed amongthe population but concentrated amongst themost vulnerable segments of society includingwomen, gay men, teenagers, young adults, blackand ethnic minority groups. Young people aredisproportionately affected by STI and Africancommunities and gay men continue to bedisproportionately affected by HIV.5.2• Preventing sexual enslavement or persuasion• Sexual well-being• <strong>In</strong>fertility• Supporting teenage parents• Safeguarding young people and vulnerable adults• Addressing risk taking behaviour• Aspects of mental health.Sexual <strong>Health</strong> as a Public <strong>Health</strong> IssueThe consequences of poor sexual health can beserious and costly for both the individual and society.It is estimated that the average lifetime costs fora HIV (human immunodeficiency virus) positiveindividual is between £135,000 and £181,000with the monetary value of preventing just a singleonward transmission to be somewhere between£500 thousand to £1 million. [1]Teenage pregnancy and its cost to the NHS aloneare estimated at £63 million per year. [2] <strong>In</strong> October2006 National <strong>In</strong>stitute for <strong>Health</strong> and ClinicalExcellence (NICE) guidelines on Long ActingReversible Contraception (LARC) suggested thatsimply an 8% shift from oral contraceptive use toLARC methods would result in net savings of morethan £102 million. [3]Preventive services in sexual health not onlypromote well-being but also positively impact uponfinancial costs. It is suggested that the preventionof unplanned pregnancy by the NHS contraceptionservices saves the NHS over £2.5 billion a year [4],and through activities such as chlamydia screeningthere is the potential to dramatically reduce costs5.3• Human costs – the human costs of unplannedpregnancy, STIs and HIV are substantial. Theadverse psychological and life changing impactof unplanned pregnancy (especially amongteenagers) and sexual ill health is avoidable.• Economic costs – there are considerable economicconsequences as a result of increased sexual healthneeds. Acute hospital capacity is taken up by HIVrelated illnesses which can be prevented with earlydiagnosis and treatment. Savings in expenditure canbe made by prevention of unplanned pregnancy andreduction in the termination of pregnancy rate.Clinical consequences of poor sexual health:• Unpleasant symptoms• Onward spread of disease• Unintended pregnancy and terminations• HIV• Pelvic inflammatory disease which may be linked tofuture infertility and ectopic pregnancy• Genital cancers• Hepatitis• Psychological ill health.<strong>Wandsworth</strong>’s Response to These IssuesThe 2005/06 Public <strong>Health</strong> Annual Report raised thepriority of sexual health. The need to improve sexualhealth is also reflected as a local key issue in thePrimary Care Trust’s Local Delivery Plan (LDP). The<strong>Wandsworth</strong> PCT Strategy for Sexual <strong>Health</strong> and HIV(January 2005) highlights inequalities in sexual health30<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 5: Sexual <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07and sets a blueprint for the development of sexualhealth services in the borough.<strong>Wandsworth</strong> Teaching Primary Care Trust has onePublic Service Agreement target relating to sexualhealth: reducing teenage conceptions by 50%from the 1998 baseline by 2010. Additionally,<strong>Wandsworth</strong> Public <strong>Health</strong> Department supportsthese areas of need:• Improve sexual health services for young people• Prevention, diagnosis and treatment of HIV and STIs• <strong>In</strong>crease access to contraception/CommunitySexual <strong>Health</strong> Services, providing better healthcare closer to home• Ensure all new patients access GUM (GenitoUrinary Medicine) services within 48 hours• Screening of 15–24 year olds for Chlamydiainfection• Provide free condom distribution.young parents. Figure 5.1 shows the downward trendobserved across <strong>Wandsworth</strong>, <strong>London</strong> and England,and highlights the relatively high rate observedin <strong>Wandsworth</strong>. As an inner city Borough the<strong>Wandsworth</strong> rates can be expected to be higher thanEngland, but the lower <strong>London</strong> rate illustrates theneed for concerted effort in <strong>Wandsworth</strong>.Consequences of teenage pregnancy: [5]• Rates of infant mortality for babies born tomothers aged under-20 are around 60% higherthan rates for children born to mothers aged20–39 years• Children of teenage parents are more likely toexperience the risk factors of early parenthood andso become teenage parents themselves, creating acycle of deprivation that is difficult to break• By age 30 teenage mothers are 22% more likelyto be living in poverty, 20% more likely to have noqualifications and much less likely to be employed orliving with a partner.5.4Teenage PregnancyTeenage pregnancy is a key issue which <strong>Wandsworth</strong>continues to tackle, to both improve health andaddress inequalities and social exclusion. Economic,social and cultural influences all impact on sexualwell-being and often give rise to inequalities. It isvital to reduce the rate of under-18 conceptions andensure information and support to those who become• Young fathers are more likely to live in deprived areas,to be unemployed and to be in receipt of benefits• It is estimated that three quarters of under-18conceptions are unplannedRisk factors for teenage pregnancy: [6].• Early onset of sexual activity• Poor contraceptive useFigure 5.1: Teenage Conception Rates for Under-18 year olds across <strong>Wandsworth</strong> in Comparison to National Ratesfor England (dotted lines are projected targets).Under 18 conception rate per 1,00075706560555045403530252019981999200020012002 2003 2004 2005 2006 2007 2008 2009 2010<strong>Wandsworth</strong><strong>London</strong>EnglandSource: Office for National Statistics<strong>Wandsworth</strong> Teaching Primary Care Trust 31
Chapter 5: Sexual <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07• Mental health/conduct disorder/involvement in crime• Alcohol and substance misuse• Low educational attainment• Disengagement from school• Leaving school at 16 with no qualifications• Living in care• Daughter of a teenage mother• Parental aspirations for their daughter.5.5Sexually Transmitted <strong>In</strong>fections (STIs)5.4.1The Local Picture for Teenage PregnancyONS (Office for National Statistics) for 2006 showa slight increase in teenage pregnancy rates for<strong>Wandsworth</strong>. The rate of conceptions measured asper 1000 of the female population aged 15–17 hasincreased from 52.2 to 57.8 (ONS 2006). Althoughincreasing slightly this is still an 18.7% reductionsince the baseline of 1998 according to figuresby the Teenage Pregnancy Unit. This 18.7% is agreater improvement on the 2004 interim target of15%, the national reduction for England and Walesof 13.7% and the inner <strong>London</strong> reduction targetof 16.6%. However, for the borough to meet its2010 target of a 55% reduction in the under-18conception rate challenges remain. To tackle thistrend teenage pregnancy must remain high on<strong>Wandsworth</strong>’s agenda so that work achieved so farcan be sustained and enhanced.Teenage pregnancy rates vary widely across theborough and are closely associated with levels ofdeprivation. Based on the assumption that eachteenager only conceives once, analysis of the ratesof teenage conceptions between 2001–2003 showsthat, approximately one in ten young womenbetween the ages of 15–17 years who live in thewards of St Mary’s Park, Queenstown, Latchmere andNightingale conceive before they reach 18 years old.Three of these wards are considered to be deprivedcommunities. The ward of Nightingale is one of themost affluent, but based within it is a large temporaryaccommodation unit for homeless people. Manyyoung pregnant women are housed here, resulting inmore births being registered in this ward.5.5.1Source: Department of <strong>Health</strong>Sexually transmitted infections are a major publichealth concern. <strong>In</strong> 2005, more than 790,000diagnoses of STIs were made in GUM Clinics. [7]Young people aged 15 to 24 are most vulnerable.Certain ethnic groups and men who have sex withmen (MSM) are also disproportionately at risk.Use of imaginative local media campaigns hasmeant sexually active teenagers are getting themessage about contraception. Condom distributionin local nightclubs, a local website, and creativeartwork by South Thames <strong>College</strong> students hasled to innovative sexual health messages by youngpeople for young people.Human Immunodeficiency Virus (HIV)Based on HPA (<strong>Health</strong> Protection Agency) figures, in2006 there were approximately 63,500 adults livingwith HIV in the UK and this number is increasingby about 5,000 each year. [8] Likewise, prevalenceof HIV infection in <strong>Wandsworth</strong> is increasing as aresult of both rising numbers of new HIV diagnosesand decreasing number of AIDS-related deaths sincethe introduction and effectiveness of highly activeantiretroviral therapy (HAART).32<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 5: Sexual <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Figure 5.2: Trends in HIV Prevalence in <strong>Wandsworth</strong>, South West <strong>London</strong> and England350300Rate per 100,00025020015010050200520060CroydonKingstonMertonRichmondSutton<strong>Wandsworth</strong>SWL<strong>London</strong>EnglandSource: SOPHID dataFigure 5.3: Percentage <strong>In</strong>crease of HIV <strong>In</strong>cidence in <strong>Wandsworth</strong> and South West <strong>London</strong>2520152004 – 2005102005 – 200650CroydonKingstonMertonRichmondSutton<strong>Wandsworth</strong>Source: SOPHID data<strong>Wandsworth</strong> Teaching Primary Care Trust 33
Chapter 5: Sexual <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Key Points• Despite the introduction of effective therapies,HIV infection still causes appreciable morbidityand mortality and imposes a significant burden onresources. Preventing onward infection of one casecould save £0.5 million in health care costs andindividual health gains. [9].• The prevalence rate of HIV in South West <strong>London</strong>(SWL) is more than double the rate of England.<strong>In</strong> 2006, there were 330.5 people per 100,000(see Figure 5.2) living with HIV in <strong>Wandsworth</strong>,a 8.4% increase (see Figure 5.3) from the 304.9per 100,000 diagnosed in 2005, and represents arate higher than South West <strong>London</strong> and <strong>London</strong>as a whole. (Survey Of Prevalent diagnosed HIV<strong>In</strong>fection Data – SOPHID)• <strong>In</strong> 2005, most heterosexual cases in SWL werethought to have been infected abroad (83%) and ofthese, the majority were infected in Africa (72%). <strong>In</strong>2005, more than half of newly diagnosed cases ofHIV infection were in Black Africans. [10]• Transmission of HIV continues at a high level in MSM,Black Africans and injecting drug users. [10] <strong>Health</strong>promotion campaigns should target these groups. Toprevent STIs in general, addressing young people’ssexual health needs should be priority.5.5.25.5.3ChlamydiaChlamydia is the most common sexuallytransmitted infection in South West <strong>London</strong>. Oftenasymptomatic, it affects an estimated one in tensexually active young people.The number of chlamydia diagnoses has risen yearon year and remains the most commonly diagnosedSTI in GUM clinics with the highest rates of infectionoccurring in 15 to 24 year olds. Untreated infectioncan lead to serious health problems including Pelvic<strong>In</strong>flammatory Disease (PID), ectopic pregnancy andinfertility in both men and women.The borough now offers free opportunistic testingand treatment to males and females under 25 yearsof age (including partner notification) in a variety ofprimary care settings across <strong>Wandsworth</strong> includingsome community pharmacies. To meet the LDPtarget of 17% of the 15–24 year old population,<strong>Wandsworth</strong> needs to screen approximately 5,400young people per year.GonorrhoeaGonorrhoea is the second most common bacterialsexually transmitted infection. <strong>In</strong>fection rates tend to behigher among MSM, young women and some ethnicminority groups. Untreated it can lead to serious healthproblems, particularly in women. As with chlamydia,complications include PID, ectopic pregnancy andinfertility. Within South West <strong>London</strong> the highestnumber of chlamydia and gonorrhoea cases werediagnosed at St George’s hospital. [10]Table 5.3: Percent change in the number of gonorrhœaand chlamydia cases in 2006 compared to 2002 and 2005GonorrhœaChlamydiaSWLHospital% changesince 2002% changesince 2005% changesince 2002% changesince 2005Kingston -21.3% -13.9% -12.0% -22.8%Mayday -41.8% -16.1% 94.2% 11.8%Queen Mary’s 3.7% 1.8% -24.4% 5.4%St George’s -40.5% -7.0% -7.4% -5.8%St Helier -67.8% -48.1% -19.2% -25.6%Source: South West <strong>London</strong> <strong>Health</strong> Protection Unit 2006 Annual Review34<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 5: Sexual <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Figure 5.4: Patient Access to Sexual <strong>Health</strong> Service within 48 hours in 2006 by PCT90%<strong>London</strong>80%SWL<strong>Wandsworth</strong>70%Sutton & MertonRichmond60%Kingston50%Croydon10 February 200610 May 200610 August 200610 November 2006Source: Gettingiton.org.ukFigure 5.5: Patient Access to Sexual <strong>Health</strong> Service within 48 hours in 2006 by Clinic100%England90%<strong>London</strong>80%St HelierRoehampton70%Mayday60%St Georges50%Kingston10 February 200610 May 200610 August 200610 November 2006Source: Gettingiton.org.uk<strong>Wandsworth</strong> Teaching Primary Care Trust 35
Chapter 5: Sexual <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/075.6Improving Access to Sexual <strong>Health</strong> ServicesImproving access to sexual health services is key to STIcontrol. Identified as a national priority, GUM clinicsare required to work to reduce waiting times of newpatients contacting the services to 48 hours. The datacollection methodology has changed, and is nowavailable on a monthly basis. Full year data is not yetavailable. However, in December 2007 89% of peoplewere offered an appointment to be seen within 48hours of contacting a service, and this rose to 97% inJanuary 2008.IF YOU HAVE CONCERNSABOUT YOURSEXUAL HEALTHYOU SHOULDN’T KEEP THEMBOTTLED UP!GUM is an open access service, residents from anyPCT are free to use the service at Queen Mary’sHospital Roehampton or St George’s Hospital inTooting. At the end of 2006, 89% of patients in<strong>Wandsworth</strong> were offered an appointment within 48hours. This is higher than the <strong>London</strong> average (82%).[11] Figure 5.4 shows the proportion of patientsoffered an appointment at a sexual health servicewithin 48 hours in 2006 by PCT. This comparativedata is only available for 2006 (as at January 2008).HELP IS AT HAND...www.gettingiton.org.uk5.7<strong>In</strong>dividual GUM clinics across <strong>Wandsworth</strong> have alsoimproved access. Between February–November 2006,St George’s and Queen Mary’s Hospitals improvedtheir access from 79% to 95% and 80% to 81%respectively, both at or above the <strong>London</strong> average of81%. [11] Figure 5.5 shows the proportion of patientsoffered an appointment at a sexual health servicewithin 48 hours in 2006 by clinic of attendance. Themost recent audit from a snapshot in February 2008indicates attendees offered an appointment within48 hours as 97% and 95% for Queen Mary’s and StGeorge’s respectively.Access to ContraceptionKey to reducing the number of unplannedpregnancies and sexually transmitted infections in<strong>Wandsworth</strong> is improved access to contraceptiveservices. Both men and women requestingcontraceptives should be given information aboutall methods, including long-acting reversiblecontraceptives (LARCs). The National <strong>In</strong>stitute for<strong>Health</strong> and Clinical Excellence (NICE) estimates suchchoice would be less costly to the NHS and reducethe number of unplanned pregnancies by 70,000each year.Key points5.8Source : Gettingiton.org.uk• Nationally LARCs (including implants, injections,and coils) were used by only 8% of women aged16–49. [13] LARC are less susceptible to incorrectusage, highly effective and fit well with thelifestyle of modern women. However their uptakeis far lower than women who took the Pill (25%)and women who relied on condoms (23%).• All currently available LARC methods are more costeffective than the combined oral contraceptive pilleven after one year of use. [13]Termination of Pregnancy<strong>Wandsworth</strong> has achieved a big fall in the numberof abortions. Between 1998 and 2005 the numberof terminations per 1,000 girls aged 15–17 fell from139 to 85. [14]Key points• <strong>In</strong> 2006, the total number of abortions (England& Wales) was 193,700 compared with 186,400 in2005, an increase of 3.9%. [14]• Nationally three quarters of women aged 16–49use at least one form of contraception. [12].36<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 5: Sexual <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07• <strong>In</strong> 2005, the highest abortion rates were in womenaged 20–24 years. Table 5.2 shows the rate in<strong>Wandsworth</strong> at 38.6 in comparison to rates forEngland at 31.7. [14]Table 5.2: Abortions in Women aged 20–24 in 2005PCT Number Rate*Croydon 616 54.7Kingston 199 31.3Richmond 127 22.4Sutton & Merton 422 39.7<strong>Wandsworth</strong> 456 38.6<strong>London</strong> 13,971 49.0England 50,983 31.7have a significant influence on sexual health.Through information, sexual health promotionhelps reduce inequalities and challenges stigma anddiscrimination across all services in <strong>Wandsworth</strong>.World Aids Day 2007To mark the twentieth annual World AIDS Day,<strong>Wandsworth</strong> PCT held a special Staying <strong>Health</strong>yevent in December 2007. Closely linked with thevoluntary sector, seven local African communitygroups in <strong>Wandsworth</strong> including Brook & Menattended this year. Building on the theme of‘leadership’, the day was a success in tackling stigmaand increased awareness of AIDS and HIV.Public health colleagues along with partners fromthe local authority, Total <strong>Health</strong> @ <strong>Wandsworth</strong>and the Terence Higgins Trust organised a fun,educational event highlighting the serious issue ofHIV/Aids to students at South Thames <strong>College</strong>.*per 1,000 20–24 year old womenSource: Department of <strong>Health</strong>• <strong>In</strong> 2005, there were 39,593 conceptions in England(in those aged under 18, ONS 2005) of these,nearly half ended in abortion.5.8.1Emergency Hormonal ContraceptionA network of <strong>Wandsworth</strong> Community Pharmaciescurrently provides Emergency HormonalContraception (EHC) to young women, free ofcharge. Access to EHC via pharmacies will be furtherdeveloped through a local enhanced service. From 1stApril 2006 to March 2007 there were 198 suppliers.5.9Sexual <strong>Health</strong> PromotionSexual health promotion is an important publichealth issue. Deprivation, social exclusion,discrimination and levels of educational attainmentTake the LeadWorld leaders have pledged to provide universal access to HIVprevention, treatment, care and support by 2010. Despite theirpromises, more people are becoming infected with HIV than everbefore and only a fraction who need treatment receive it. Our leadersmust be held accountable. Take the lead – demand action.Stop AIDS. Keep the Promise.Visit www.worldaidscampaign.orgSource: Department of <strong>Health</strong><strong>Wandsworth</strong> Teaching Primary Care Trust 37
Chapter 5: Sexual <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/075.10Recommendations1. Use of public health intelligence to increaseeffective commissioning of sexual healthservices to address health needs of the<strong>Wandsworth</strong> population2.3.4.5.Target sexual health initiatives and servicesdirectly towards adolescents and young peopleEncourage an integrated approach to sexualhealth services<strong>In</strong>crease activity to support young parentsImprove engagement with young people toenable appropriate service development6. Ensure education strategies develop youngpeople’s skills (for example, negotiation inrelationships)7.Develop efficient, consistent and timely sexualhealth data reporting for <strong>Wandsworth</strong> PCT8. Strengthen evaluation, and intelligencegathering procedures9.Work with key primary care services to extendsexual health services for the local community.References[1] British Medical Association’s written submission to the<strong>Health</strong> Select Committee inquiry – new developmentsin HIV/AIDS and sexual health policy. 2005.[2] Teenage Pregnancy Strategy Evaluation Team. Annualreport synthesis 2002, page 7. <strong>London</strong>: TeenagePregnancy Unit, 2003.[3] NICE National cost-impact report. Implementingthe NICE clinical guideline on long-acting reversiblecontraception. December 2005.[4] House of Commons. Select Committee on <strong>Health</strong>, ThirdReport, Sexual <strong>Health</strong>. TSO: <strong>London</strong>. 2003.[5] Department of <strong>Health</strong> & Department for Children,Schools and Families. Teenage Parents Next Steps:Guidance for Local Authorities and Primary Care Trusts.2007.[6] Department of <strong>Health</strong> & Department for Children,Schools and Families. Teenage Pregnancy: workingtowards 2010. 2007.[7] <strong>Health</strong> Protection Agency. A complex picture: HIV andother sexually transmitted infections in the UnitedKingdom: 2006. 2006.[8] <strong>In</strong>dependent Advisory Group on Sexual <strong>Health</strong> andHIV. Public <strong>Health</strong> Policy and HIV/AIDS, an IAG SeminarReport. December 2007.[9] Armstrong, N., Donaldson C. The Economics of Sexual<strong>Health</strong>. FPA 2005.[10] South West <strong>London</strong> <strong>Health</strong> Protection Unit. AnnualReview. <strong>London</strong>: <strong>Health</strong> Protection Agency, 2006.[11] <strong>Health</strong> Protection Agency. GUM Waiting Times Audit:National Results. 2007[12] Department of <strong>Health</strong>. Contraception: Factsheet,patterns of use. TSO: <strong>London</strong> 2007. Available atwww.fpa.org.uk.[13] National Collaborating Centre for Women’s & Children’s<strong>Health</strong>. Long-acting reversible contraception: theeffective and appropriate use of long-acting reversiblecontraception. NICE. 2005.[14] Department of <strong>Health</strong>. Abortion Statistics, England &Wales: 2006 Bulletin 2007/01. TSO: <strong>London</strong>, 2007.With thanks to Elizabeth Dubois38<strong>Wandsworth</strong> Teaching Primary Care Trust
6.Primary CareFor most people, Primary Care is the first point ofcontact with health services. It is through PrimaryCare that early and basic diagnoses are made andtreatment plans delivered. Services are based in thecommunity and so are easily accessed by the localpopulation. They are also more likely to be openin the evenings and at weekends. Primary carepractitioners are networked into local communitiesand so are able to refer and signpost people toa range of services from community through tosecondary care.As most contacts are initiated by the well, PrimaryCare services provide an excellent opportunity topromote health and to give a range of preventiveinterventions and influence positive health behaviour.Primary Care provides quick access to professionalswho can give one to one expert advice and support.6.1Defining Primary Care‘The health services that play a central role in thelocal community, such as family doctors (GPs),pharmacists, dentists and ophthalmologists. Everycitizen should have the best possible access to theseprimary care services’ (DH 2007).<strong>Wandsworth</strong> Primary Care Trust is responsible forcommissioning primary care services for the localresident population. This chapter describes primary careservice providers within <strong>Wandsworth</strong>, who uses theseservices, and the role the services play in protectinghealth.6.2Current Service Providers andPatient ProfilesThe age profile of service users can be comparedwith the profile of the resident population from thelast census (2001) to highlight which services attractwhich age groups. Knowing these profiles helpsidentify any inequity in service provision. Age relatedservice data is limited to the Tooting Walk in Centre,dentistry, and General Practice.<strong>Wandsworth</strong> Teaching Primary Care Trust 39
Chapter 6: Primary Care<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Walk <strong>In</strong> Centre at St GeorgesThe Tooting Walk in Centre (WIC) is‘open access’, offering health careadvice, information, and treatment forminor injuries.A comparison of people who attendedthe Tooting WIC (Figure 6.1) over aperiod of one year with the population of<strong>Wandsworth</strong> highlights the following:• <strong>In</strong> the 17–25 year age band, there are alarger proportion of people attendingthe walk in centre compared to thegeneral population of <strong>Wandsworth</strong>.<strong>In</strong> addition the ‘white’ population is theethnic group that has the largest numberof Walk <strong>In</strong> Centre contacts, however theyrepresent only 64% of the attendances,despite being 78% of the generalpopulation. Most other ethnicities aretherefore over represented at the Walkin centre. This may be due to a lack ofknowledge or understanding about thehealth care system or appropriate access toprimary care services within <strong>Wandsworth</strong>.• <strong>In</strong> the 36–45 year age band, fewer malesare attending the WIC compared to thegeneral population of <strong>Wandsworth</strong>.• <strong>In</strong> the 56+ year age band, a considerablygreater number of males attend the WICcompared to the general population of<strong>Wandsworth</strong>.Walk <strong>In</strong> Centre ConclusionBy analysing the user profilesof the WIC, healthcare issues inline with age and ethnicity areidentified and allow services tobe developed accordingly.Figure 6.1: Population Pyramid for Tooting Walk <strong>In</strong> Centre for consultations 1 April 2006 – 31 March 2007>8066 to 79Age bands (years)56 to 6546 to 5536 to 4526 to 3517 to 255 to 161 to 4
Chapter 6: Primary Care<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Primary Care Dental ServicesThe PCT has 53 general/personal dentalservice contracts covering 45 dentalsurgeries spread across <strong>Wandsworth</strong>.(Figure 6.2). The PCT is encouragingdentists to take an increased role inpromoting health such as smokingcessation and healthy eating.The largest proportion of people accessingdental services in <strong>Wandsworth</strong> is in the 25to 44 year age group (38%). Almost half ofthe <strong>Wandsworth</strong> population (48%) is agedbetween 25 and 44 years. This indicatesthat further work is needed to ensuredentistry services are accessed by the 25-44year old group of people in <strong>Wandsworth</strong>.The PCT has contracted with Harmoni totriage all dental emergencies during theout of hours periods in order to improveaccess for the whole population.Table 6.1: Number of <strong>Wandsworth</strong> ResidentsAttending Local DentistsAgeRange(years)Number ofpatients% of peopleattendinga dentist% of peoplein <strong>Wandsworth</strong>0–2 1,560 2 43–5 4,567 5 46–12 11,724 13 613–17 6,061 7 418–24 6,342 7 925–34 19,060 21 3035–44 15,521 17 1845–54 10,092 11 955–64 7,695 8 765–74 5,514 6 575+ 3,222 4 4Dental Services ConclusionBetter use should be made ofdental services data to determineif those vulnerable have accessto NHS dental services. Acomprehensive review of dentalcaries by area would help totarget particular initiatives.Total 91,358 100 100Source: Business Support Agency, 2006/07 data<strong>Wandsworth</strong> Teaching Primary Care Trust 41
Chapter 6: Primary Care<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Community Optometric ServicesThere are 28 optometrists in <strong>Wandsworth</strong>with a further ten optometristscommissioned by the PCT to providedomiciliary services. Optometrists alsosupport the prevention of ill-health, forexample by providing cataract referralschemes and making referrals for a numberof other conditions to the Hospital EyeService. Developments in these areas canhelp in assisting the shift of resources fromsecondary to primary care.Optometric ServicesConclusionBetter use should be made ofoptometric services data to drawup user profiles, and thereforeidentify those groups notaccessing the service.Figure 6.2: Dentists and Optometrists in <strong>Wandsworth</strong> and Levels of Deprivation by WardScores for the Wards of <strong>Wandsworth</strong>1 Most deprived2345 Least deprivedOptometrists in <strong>Wandsworth</strong>Dentists in <strong>Wandsworth</strong>42<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 6: Primary Care<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Community PharmaciesThere are 64 community pharmacies in<strong>Wandsworth</strong>, which all draw staff fromthe local community and can thereforeeffectively identify and respond to changingpopulation needs. The current network ofcommunity pharmacies (Figure 6.3) withextensive opening hours provides the publicwith ready access to a health professional,medication, and opportunistic health advicefor minor ailments. The pharmacies providesome of the services which people need toaccess quickly – for example, emergencyhormonal contraception, or frequently – forexample, anti-coagulation monitoring. Thesespecial characteristics of local pharmacistscan be utilised to provide structured healthpromotion programmes.Community pharmacy is an existinginterface between health and social careworking with district nurses, carers andother professionals that support peopleliving at home. This diverse nature ofthe community pharmacy is one that canbe called upon in a short space of timeand used in times of emergency, such aspandemic flu.The Pharmacy Contractural Framework,which was launched in April 2005, providesthe means for more accessible Preventiveand health improvement interventions. Theframework offers a range of services forall ages, such as services to drug mis-users,smoking cessation, emergency hormonalcontraception, as well as the dispensing ofmedicines, and medicines management.Figure 6.3: Community Pharmacies in <strong>Wandsworth</strong>Pharmacy ConclusionThe accessibility ofpharmacists to their localpopulations should be utilisedto a greater extent to providea basis for opportunistic andstructured health promotion,and as a resource to monitorlocal health need.<strong>Wandsworth</strong> Teaching Primary Care Trust 43
Chapter 6: Primary Care<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07General PracticeThe PCT has contracts with 55 GP surgeriesacross <strong>Wandsworth</strong>. Every UK practice mustprovide essential services covering the dayto-daywork of general practice which cover:• The management of patients whoare ill, or believe themselves to be ill,with conditions from which recovery isgenerally expected.• The general management ofchronic disease.• The non-specialist care of patients whoare terminally ill.<strong>In</strong> addition practices may offer thefollowing additional services:• Cervical screening;• Contraceptive services;• Vaccinations and immunisations;• Child health surveillance;• Maternity medical services;• Minor surgery.There are further Enhanced services whichmay be offered which are ‘essential’ or‘additional’ services as above but deliveredto a specified standard; they are also morespecialised services, for example, anticoagulationmonitoring, or services forviolent patients.Data from General Practice is limited to acensus of people registered with a GP andis not available for subsequent use of a GP.When comparing the GP registeredpopulation (Figure 6.4) with the generalresident population (Figure 6.5), it isobvious that the number of peopleregistered with a GP is more than thenumber resident (2001 census). Withinthis there exist some under and overrepresentationsof population groups:• <strong>In</strong> the 15 to 19 year age band, more femalesare registered with a GP than males.However the number of residents is equal.• <strong>In</strong> the 35 to 59 year age bands aconsiderably larger proportion of malesattend a GP practice compared with theresident population of <strong>Wandsworth</strong>.Figure 6.4: <strong>Wandsworth</strong> GP registered population (GP) Figure 6.5: <strong>Wandsworth</strong> resident population (Census 2001)Age groups (years)90+85-8980-8475-7970-7465-6960-6455-5950-5445-4940-4435-3930-3425-2920-2415-1910-1405-090-420 16 12 8 4 0 4 8 12 16 2090+85-8980-8475-7970-7465-6960-6455-5950-5445-4940-4435-3930-3425-2920-2415-1910-1405-090-420 15 10 5 0 5 10 15 20Age groups (years)Source: Exeter 2007Source: Census 2001MaleFemale44<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 6: Primary care <strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/076.3Access to General PracticeGeneral Practice Conclusions• Knowing the extent of theGP registered population incomparison to the residentpopulation of the Boroughwill enable the PCT throughPractice Based Commissionersto better understand, developand target services.Access to primary care services is a national and localpriority. The NHS Plan aimed to ensure that patientswere able to access a GP within 48 hours and aPrimary Care Practitioner within 24 hours. Alongsidethis is the increasing pressure to provide patientswith access that fits in with their lives. <strong>In</strong> order toaid this, a Direct Enhanced Service (DES) for accesswas developed. The aims of this were to look at thefollowing key areas:• Access to a GP within 48 hours• Ease of telephone access to the practice• Ability to book appointments in advance• Ability to book an appointment with a specific GP.<strong>In</strong> order to assess if practices were achieving theabove elements, the government commissioned aNational Patient Survey. The survey was conductedlocally during 2006–7. At a national and local level,the greatest area of dissatisfaction was lack of lateevening and Saturday opening hours.• By analysing the userprofiles of general practice,healthcare issues areidentified and allow servicesto be developed accordingly.<strong>Wandsworth</strong> teaching Primary Care Trust45
Chapter 6: Primary Care<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/076.4Service Data Currently Available fromGeneral PracticeThe Quality and Outcomes Framework (QOF) is theannual reward and incentive programme detailingGP practice achievement results. QOF, a voluntaryprocess for all surgeries, was introduced as part of theGP contract in 2004. QOF includes a register of mostcommon chronic diseases – for example, asthma, anddiabetes. The register is crude and does not containage, sex, or ethnicity details. Completion of the registercannot be used solely as a measure of quality.Using a postcode based mapping process, the resultsavailable from QOF based on GP have been allocatedto residential ward. There are some caveats to thisapproach, most notably that people registered topractices outside of <strong>Wandsworth</strong> but live within<strong>Wandsworth</strong> fall outside of the analysis.Comparing the most deprived ward and theleast deprived ward reveals a common theme,registrations for long term conditions, cancer, andhealth risks (obesity, hypertension) seem to behigher in the most deprived wards compared to theleast deprived wards. This theme is also commonthroughout the wards of residence for StandardisedMortality Ratios (SMR) as in Table 6.2.<strong>In</strong>terestingly the prevalence rates for long termconditions in Latchmere are higher than forThamesfield but frequently lower than the averagerate for <strong>Wandsworth</strong> as a whole. This is not the casewhen looking at the Standardised Mortality Ratios(SMR) between wards of residence where mortality6.56.5.1outcomes in Latchmere are higher than expectedwhen compared to Thamesfield and <strong>Wandsworth</strong>as a whole. These observations suggest that whilstmortality may be more closely correlated with levelsof residential deprivation, other factors influencethe potential association between deprivation andregistration for long term conditions, cancer andhealth risk. These other factors could be patientprofiles (age, sex, ethnicity), or differences inregistration approach between practices.Immunisation and ScreeningPreventive services such as immunisation andscreening are additional services that can beprovided by primary care. The arrangements forthe provision of these services are subject to localnegotiation, and data flowing between GeneralPractice and the PCT is often a limitation to formingfirm conclusions and recommendations.ImmunisationThe uptake rates for almost all childhoodimmunisations were lower in <strong>Wandsworth</strong> comparedto <strong>London</strong> and England in 2007/08 (Table 6.3). Sofar the rate for childhood immunisation at two yearsof age has improved, due primarily to concertedefforts to capture all paper based immunisationnotifications from GPs and community clinics.Measles was rare in the UK because MMRvaccination protected against it. However, there hasrecently been a growing number of cases of measlesTable 6.2: Prevalence Rates and Standard Mortality Ratios (Extract from the Picture of <strong>Health</strong>) (Appendix 5)Latchmere Thamesfield <strong>Wandsworth</strong>Number (Rate*) Number (Rate*) Number (Rate*)GP Register CHD 166 (12.78) 192 (9.91) 5,305 (16.26)COPD 85 (6.54) 77 (3.98) 2,695 (8.26)Hypertension 1,072 (82.54) 1,013 (52.29) 28,003 (85.85)Diabetes 387 (29.80) 266 (13.73) 9,630 (29.52)Stroke 93 (7.16) 89 (4.59) 2,662 (8.16)Cancer 63 (4.85) 115 (5.94) 2,441 (7.48)Obesity 752 (57.90) 513 (26.48) 16,129 (49.45)Mental <strong>Health</strong> (schizophrenia, bipolar disorder, & other psychoses) 112 (8.62) 91 (4.70) 2,773 (8.50)SMR All cause mortality Men under 75 165.4 70.8 105.8All cause mortality Women under 75 152.2 79.6 106.3All cause mortality, Males, All Ages 146.5 76.6 104.8All cause mortality, Females, All Ages 120.4 79.7 106.1CHD, under 75 175.3 ** 99.4Cancer, under 75 153.9 78.0 99.4Cardiovascular disease, under 75 191.7 71.5 114.5*Rate per 1,000 GP registered populationSource: QMAS 2007, Clearnet activity 2007 and GLA 2006 Round Population Projections, SARs from HES 2005/06, analysed by the LHO, SMR’s 2001–2005 LHO,**where the observedvalue is under 20, the corresponding SMR has been suppressed.For SAR and SMR, England = 10046<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 6: Primary Care<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07in <strong>Wandsworth</strong> which has heightened concernregarding the relatively low level of vaccine coverage(section 6.5.3 notifiable disease). A strategy toimprove MMR coverage rates in <strong>Wandsworth</strong> hasbeen developed and is being implemented.From September 2006 children aged two monthshave been receiving the pneumococal conjugatevaccine (PCV). <strong>In</strong> <strong>Wandsworth</strong> all children bornbetween 05/09/04 – 03/07/06 were offered eitherone or two PCV as part of the catch-up campaignprogramme.Since March 2006, BCG vaccination programmetargeting 0-5 year olds at risk of exposure to TBhas been operating within <strong>Wandsworth</strong>. Four BCGcommunity clinics offer a service in <strong>Wandsworth</strong>.Further immunisation activities planned include aproposed BCG ‘catch up’ programme to commencein spring 2008.The recording of immunisation uptake is a knownproblem in <strong>London</strong>, and especially within ahighly mobile population like <strong>Wandsworth</strong>. Theintroduction of a new community health system hasgiven <strong>Wandsworth</strong> PCT the opportunity to reassessall those children due immunisations and removethose from the system that are no longer eligible.Flu<strong>In</strong>fluenza or ‘flu’ is a respiratory illness caused bythe influenza virus. Severity of illness ranges fromminor symptoms through to pneumonia and death.Vaccination against flu can protect individuals fromthe illness.Table 6.3: Percentage of Children Immunised by TheirSecond Birthday, 20076.5.2DTaP/IPV/Hib* Meningitis C MMR% Q1 Q2 Q1 Q2 Q1 Q2England 93 94 93 94 85 84<strong>London</strong> 83 85 83 84 73 73<strong>Wandsworth</strong> 74 78 82 83 75 71Q1 April to June 2007, Q2 July to September 2007.* Diphtheria, tetanus, pertussis, polio and Haemophilus influenzae type bSource: <strong>Health</strong> Protection AgencyIt was estimated that 70.4% of South West <strong>London</strong>(SWL) residents aged 65 and over had received the2006/07 influenza vaccine by January 2007. (Figure6.6). This was the same as the <strong>London</strong> uptake butslightly lower than the national uptake (73.5%).Compared with last year, only <strong>Wandsworth</strong> PCTrecorded an improved influenza vaccine uptake for2006/7 within SWL PCTs. The <strong>Health</strong> Protection Unithas yet to release the figures for 2007/8.ScreeningCervical ScreeningThe National Cervical Screening Programme aims toreduce the risk of cervical cancer and targets womenaged 25 to 64. <strong>Wandsworth</strong> Teaching Primary CareTrust is responsible for ensuring that this service isprovided to these groups of women with targetcoverage of 80%. It is most generally providedthrough General Practice.Figure 6.6: Recorded <strong>In</strong>fluenza Vaccine Uptake Rate in People Aged Over 65 for 2006/7Vaccine uptake100%90%80%70%60%50%40%30%20%10%0%70.4% 68.6% 75.4% 67.1% 74.6% 72.4% 72.9% 71.7% 70.7% 72.0%CroydonKingstonRichmond Sutton & Merton <strong>Wandsworth</strong>2006–20072005–2006Source: <strong>Health</strong> Protection Agency 2007PCT<strong>Wandsworth</strong> Teaching Primary Care Trust 47
Chapter 6: Primary Care<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07During 2005–2006, around 26,000 women in<strong>Wandsworth</strong> aged 25–64 years were invited for acervical smear. The coverage rate for the target agegroup was 72.9% which compares against 74.2%achieved across <strong>London</strong> as a whole.General Practice coverage shows that around twothirdsof the practices in <strong>Wandsworth</strong> were achievingthe national target of 80% coverage.Recent <strong>Wandsworth</strong> PCT Screening Serviceimprovements include the appointment of a nurseadvisor who will be visiting under-performing GPpractices and providing advice and support forimprovements.Breast ScreeningThe South West <strong>London</strong> Breast Screening Service(SWLBSS) is based at St George’s Hospital, withsatellite screening units located throughout the area.It offers a National <strong>Health</strong> Service Breast ScreeningProgramme (NHSBSP) to women between the agesof 50 and 70 within SW <strong>London</strong>.There are 14,151 women eligible for NHSBSP screeningin <strong>Wandsworth</strong>. During 2006–7, 11,439 women wereinvited and 6,440 women attended from <strong>Wandsworth</strong>in whom 82 cancers were diagnosed. The provisionalfigures for 2006-7 show coverage of 62.5% (target70%). Coverage in inner city areas is recognised to below, especially in <strong>London</strong>.The SWLBSS is currently looking at how serviceprovision will change in the light of the recentlypublished Cancer Reform Strategy.Bowel ScreeningBowel cancer is the UK’s second largest cause of deathfrom cancer. One in 20 people will develop bowelcancer. Bowel cancer kills around 16,000 people a year.Regular bowel screening has shown to reduce deathsfrom bowel cancer by 16%.The bowel screening programme was introduced in<strong>Wandsworth</strong> in October 2006. All those betweenthe age of 60–69 registered with a GP will be senta simple-to-use test kit over the first two years ofthe programme and then every two years untilthey reach 70. The test is also available to thoseover 70 years old on request. Pharmacists across<strong>Wandsworth</strong> are supporting the bowel screeningprogramme by raising awareness and discussingsymptoms with clients. The Cancer Screening Nurseis also meeting with Primary Care staff and usergroups to promote the programme.It is estimated that about 98% of the tests will benegative. Further consultation and investigation will6.5.3be offered to those with a positive test. Of the 2%receiving a positive result only about 10% will havebowel cancer. If detected early 90% of those peoplewith bowel cancer will survive.<strong>Health</strong> Protection Through Primary CareTable 6.4 highlights the number of infectiousdiseases that were notified to the <strong>Health</strong> ProtectionUnit in South West <strong>London</strong> in 2006 and in 2007. Thedata for 2007 is provisional and will change.Measles, Mumps and RubellaThere was a significant rise in measles from 2005to 2006, which seems to have reduced slightlyinto 2007. The number of mumps notifications hasdropped from the outbreak in 2005, and across thesector seems to have dropped to a similar level tothat in 2004, but these levels are still far higher thanthe number of cases being notified in 2001–2003.The number of rubella cases notified has continuedto drop across the sector, and within <strong>Wandsworth</strong>.Whooping Cough (Pertussis)A total of 12 formal notifications of whooping cough inSWL residents were made in 2006, two of which werein <strong>Wandsworth</strong>. <strong>In</strong> 2007 there were 13 notificationsand three confirmed cases. The number of notificationshas varied over the last ten years, and there appearsto be little obvious trend. There was one case oftetanus reported in SWL in 2006, and provisionallynone in 2007. There were no reported cases of polio ordiphtheria in the sector in 2006 or 2007.TuberculosisThe number of tuberculosis cases notified hasdeclined in the sector over the last three years butthe overall numbers are approximately 100 morethan the numbers notified in 2000. The <strong>Wandsworth</strong>rate fell to just over 30 per 100,000 in 2006, but theprovisional figures for 2007 show a marked increaseover 2006, which may give a final rate above the40 per 100,000 figure, a threshold below whichselective BCG is given in contrast to universal BCG.Following advice from the Joint Committee onVaccination and Immunisation (JCVI) the universalBCG vaccination programme delivered throughschools has been replaced with a targeted programmefor those individuals who are at greatest risk.48<strong>Wandsworth</strong> Teaching Primary Care Trust
Chapter 6: Primary Care<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07A system for monitoring Hepatitis B immunisationshas been established by working in partnership withSt. George’s Hospital to follow up all babies whoare born to Hepatitis B mothers in order to completetheir vaccination programme. It is hoped to extendthis service to other maternity units serving the<strong>Wandsworth</strong> population.Source: Cavendish laboratoriesThe new programme will identify and vaccinate babiesand older people who are most likely to catch thedisease, especially those living in areas with a highrate of TB or whose parents or grandparents wereborn in a TB high prevalence country. <strong>In</strong> <strong>Wandsworth</strong>this has resulted in the setting up of four neonatalBCG clinics, in Tooting, Doddington, Westmoor andthe Walk <strong>In</strong> Centre, in 2007 these clinics vaccinated562 infants. It is not exactly known how manychildren in <strong>Wandsworth</strong> would qualify for BCG,and it is therefore not possible to present these 562vaccinations as a coverage rate.Hepatitis BThe prevalence of Hepatitis B virus (HBV) amongstwomen tested antenatally in 2006 was 0.63%representing a fall from 2005. <strong>In</strong> 2006, theprevalence of previous or current HBV infection ininjecting drug users was 29.2%, a rise from 2005.SWLHPU also worked to improve vaccine uptake inbabies born to HBV positive mothers. Unfortunately,despite this, the reported coverage remains poorwith only 68% of babies receiving three vaccinationsby their first birthday.Gastrointestinal <strong>In</strong>fectionsFood poisoning includes reported cases ofSalmonella and Campylobacter bacteria. Salmonellacauses food poisoning, and can also cause typhoidfever and paratyphoid fever. Campylobacter is thecommonest reported bacterial cause of infectiousintestinal disease in England and Wales. The numberof food poisoning outbreaks in SWL in 2006remained similar to 2005, and provisionally thenumber in 2007 dropped slightly to 1798. This trendwas the same for <strong>Wandsworth</strong>, with a slight dropfrom 513 to 508 cases in <strong>Wandsworth</strong>.Scarlet FeverScarlet fever usually occurs after a throat or skininfection with streptococcus bacteria usually passedon from coughs and sneezes. It usually affectschildren, most commonly between the ages of fourand eight years, but people of any age can catch it. Itis quite rare in the UK because of the regular use ofantibiotics for streptococcus infections. <strong>In</strong> 2006 therewere 83 cases within the South West <strong>London</strong> sector,the provisional data for 2007 indicates a similarquantity. Within <strong>Wandsworth</strong> the number of casesso far notified is half that of 2006, and it does notpresent a pressing concern for any additional action.Table 6.4: Notifications of <strong>In</strong>fectious Disease (NOIDs), SWL by Local Authority and Disease Type, 2006 and 2007*CroydonKingstonupon ThamesSutton & MertonRichmondupon Thames <strong>Wandsworth</strong> SW <strong>London</strong>Disease 2006 2007* 2006 2007* 2006 2007* 2006 2007* 2006 2007* 2006 2007*Measles 22 26 10 7 26 25 9 9 25 16 92 83Mumps 77 27 31 14 79 27 78 15 81 36 346 119Rubella 9 – – – – 9 – – 9 7 – –Scarlet Fever 33 18 3 12 20 29 2 7 25 12 83 78Tuberculosis 117 121 21 18 90 66 16 9 70 105 314 319Food Poisoning 326 397 120 105 697 642 193 146 513 508 1,849 1,798Data source: HPA <strong>London</strong> NOIDS Database* 2007 data is provisional<strong>Wandsworth</strong> Teaching Primary Care Trust 49
Chapter 6: Primary Care<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/076.6Recommendations1. To involve the young population of <strong>Wandsworth</strong>(20–44 year olds) in primary care service redesignand also to raise awareness about access to thefull range of local services available.2.3.4.5.Develop an information strategy that maximisesthe effective use of primary and community caredata to enhance available information for healthcare planning. <strong>In</strong> particular to target ‘at risk’groups and increase life expectancy.To improve the data capture between communityhealth systems and primary care to accuratelyreport immunisation coverage.To improve actual immunisation uptake bysharing best practice with other Boroughs in<strong>London</strong> that face similar challenges.Through Practice Based Commissioning and thePrimary Care Strategy develop integrated servicesthat support the reduction of health inequalities.With thanks to Asmat Nisa50<strong>Wandsworth</strong> Teaching Primary Care Trust
7.Emergency Planning7.1Protecting the Public7.2<strong>Wandsworth</strong> PCT has a duty to protect and promotethe health of the community, including at timesof emergency. The PCT is required to plan for andrespond to any incident with major consequencesfor health or health services in partnership with theacute and non-acute trusts, emergency services andlocal authorities. The Chief Executive, through theDirector of Public <strong>Health</strong> and a senior manager foremergency preparedness, is responsible for ensuringthat the PCT has an emergency plan in placethat is based on the principles of risk assessment,co-operation with partners, emergency planning,communicating with the public and informationsharing. <strong>In</strong> addition <strong>Wandsworth</strong> PCT supports andassists emergency planning and preparedness forNHS organisations in the South West <strong>London</strong> LocalResilience Forum (LRF).Governance and the LegislativeEnvironmentThe field of emergency preparedness has becomemore complex with changing threats such asglobal terrorism and the rising flu pandemic risk,and at the same time more challenging with theneed for business continuity planning and effectiveengagement with borough partners under theCivil Contingencies Act 2004. The PCT is meetingthese emergency preparedness challenges througheffective governance by the Emergency PlanningCommittee which oversees compliance with theDepartment of <strong>Health</strong>’s Emergency PlanningGuidance 2005 and accompanying NHS guidance,the Civil Contingencies Act 2004, and meeting the<strong>Health</strong>care Commission performance standards C24.The Emergency Planning Committee ensures thatthe board receives regular reports, at least annually,regarding emergency preparedness. These includereports on exercises, training and testing undertakenby the staff and services and demonstrate thatadequate resources are made available to allowdischarge of these responsibilities.7.3Source: www.epcollege.gov.ukEmergency Preparedness<strong>Health</strong>care Commission performance standardC24 states that <strong>Health</strong>care organisations protectthe public by having a planned, prepared and,where possible, practised response to incidentsand emergency situations which could affectthe provision of normal services. The PCT hasrobust command and control mechanisms toplan for, and respond to, major incidents linkedwith the command and control arrangementsof the NHS <strong>London</strong> Strategic <strong>Health</strong> Authority(SHA). The PCT has an emergency plan in placethat is reviewed twice annually by the emergencyplanning committee. The plan links into the PCT’sarrangements for ensuring business continuitythrough the business continuity plan.The PCT:• Has up to date plans to deal with major incidentsand emergency situations that are compliant andtested in accordance with national guidance• Has included key partner organisations in thepreparation and testing of the PCT emergency plan• Can mobilise staff to respond to incidents andemergency situations that could affect theprovision of normal services.<strong>Wandsworth</strong> Teaching Primary Care Trust 51
Chapter 6: Emergency Planning<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/077.4Strategy to Implement EmergencyPreparednessThe most effective vehicle for ensuring emergencypreparedness is training and exercising. Theemergency planning committee ensures thatmanagers and staff are prepared for and haveconfidence in mobilising the resources of the PCT inthe event of a major incident through an intensivetraining and exercise schedule which simulatesincidents and gives an opportunity for managers andstaff to increase their competence in managing amajor incident. As a minimum requirement, the PCTis required to undertake a live exercise every threeyears; a table top exercise every year and a test ofcommunications cascades every six months.7.67.7ConclusionGood progress in training staff in emergencypreparedness has been achieved. But the risksand threats continue to change. Emergency plans,systems and staff competencies need to constantlyreviewed and refined to ensure that the PCTmaintains its obligations to protect the public.Recommendations1. Implementation of specialist training courses,especially in emergency management supportingroles and log taking.2.Training in emergency preparedness to be givento all managers whether on a rota or not.7.5Achievements for 2007/08Areas where significant progress in emergencypreparedness has been made are:3.4.To operationalise flu pandemic planningTo hold a live exercise independently or inpartnership with other agencies.• The training and exercising programme has beenimproved and significant progress towards raisingstaff skills in this field has been made.With thanks to Ed Checkley• Communications exercises have been held at sixmonthly intervals• The requirement to hold one table top exercise peryear has been exceeded• Close partnership working with <strong>Wandsworth</strong>Council has been achieved through sharing theCouncil’s full time emergency centre for alertingthe PCT and using each other’s incident controlroom as a back-up facility.• The on call rota system has been reinforced with arobust pager system linked with mobile phone textmessaging and e mail.• The PCT’s business continuity plan is updatedfollowing the re-structuringSource:www.chelmsford.gov.uk52<strong>Wandsworth</strong> Teaching Primary Care Trust
Appendix 1Nine areas of public healthThe Public <strong>Health</strong> Directorate is part of themultidisciplinary Primary Care Trust and Boroughwide resources. It is committed to improving thehealth and well being of people living and workingin <strong>Wandsworth</strong> by:• Working in partnership other directorates, the<strong>London</strong> Borough of <strong>Wandsworth</strong>, the voluntarysector and other agencies including the third sector.• Providing leadership for health improvement.• Raising professional and public awareness ofhealth related issues.The overall aim of the Public <strong>Health</strong> Directorate isto ensure that the health needs of <strong>Wandsworth</strong>’spopulation are met through effective commissioningof services and delivery of sustainable programmesof health improvement. This is achieved throughthe integration of the high level expertise fromPublic <strong>Health</strong> in clinical practice, health promotion,Preventive programmes and data analysis.The Faculty of Public <strong>Health</strong> have outlined nine coreareas of practice, which form a template for thetraining curriculum and for developing standards ofpractice in public health (Box A1.1). Each core area ishighlighted and briefly explained within the contextof the <strong>Wandsworth</strong> Directorate of Public <strong>Health</strong>(Table A1.1).Box A1.1: Nine Core Areas of Public <strong>Health</strong>1 Surveillance and assessment of the population’s health and wellbeing2 Assessing the evidence of effectiveness of health and healthcare interventions, programmes and services3 Policy and strategy development and implementation4 Strategic leadership and collaborative working for health5 <strong>Health</strong> Improvement6 <strong>Health</strong> Protection7 <strong>Health</strong> and Social Service Quality8 Public <strong>Health</strong> <strong>In</strong>telligence9 Academic Public <strong>Health</strong>Source: Faculty of Public <strong>Health</strong>, 2006<strong>Wandsworth</strong> Teaching Primary Care Trust 53
Appendix 1: Nine Areas of Public <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table A1.1 Examples of Public <strong>Health</strong> Core CompetenciesPublic health core area Definition <strong>In</strong>itiativesSurveillance and assessment of thepopulation’s health and well beingAssessing the evidence of effectivenessof health and healthcare interventions,programmes and servicesQualitative assessments from the public andstakeholders concerning well being and need.<strong>In</strong>cludes the wider determinants of health,housing, environment and transport.Ensuring that all commissioned interventions areevidence based as effective and best practiceTeams of community development workersare based in deprived communities and aim toempower local people to articulate their healthneeds, act as advocates, and help local people maketheir concerns heard in order to influence and shapelocal decisions and service development.The Public <strong>Health</strong> Clinical Effectiveness Groupreviews evidence of the effectiveness of existingand new health technologies. It advises on theappropriateness of investment or disinvestmentand likely service and financial implications.Members of the group are also involved in thedevelopment of sector-wide guidance.Strategic leadership and collaborativeworking for healthLong-term perspective, through strategic andoperational partnerships.Membership of groups such as the LocalStrategic Partnership, <strong>Health</strong> Partnership Board,Sexual <strong>Health</strong> Implementation group and SectorCommissioning group.Policy and strategy development andimplementationIdentification of particular health issues,through to the development of policies andimplementation of actions to address them.Strategies to promote health and well beingsuch as sexual health, obesity, and physicalactivity underpinning commissioning andprovider functions.<strong>Health</strong> improvementImplementation of initiatives in appropriatesettings and through partnership withstakeholders.Implementation of health and well beingprogrammes such as mental health, stop smokingand Staying <strong>Health</strong>y. Collaborative work withkey partners on Drugs, Alcohol and teenagePregnancy.<strong>Health</strong> protectionAdvice and action against communicablediseases, major incidents and hazards includingchemical and biological.Surveillance of communicable diseases and noninfectiousenvironment hazards through the SouthWest <strong>London</strong> <strong>Health</strong> Protection Unit. Co-ordinationof screening programmes such as breast, cervical,chlamydia and immunisation. Provision of an up todate emergency plan and training.<strong>Health</strong> and social service qualityReview and evaluation of service provisionand quality.Audit work with the Early <strong>In</strong>tervention in Psychosisteam and also leading in the evaluation of a newstroke care pathway across South West <strong>London</strong>.Public health intelligenceCollation, analysis and interpretation ofepidemiological information to support healthand social well being interventions.<strong>Health</strong> needs assessments in sexual health,primary care, prison services, and contributingto a Joint Strategic Needs Assessment with<strong>Wandsworth</strong> Borough Council. A survey of thedeterminants of health is planned for 2008.Academic public health Research and teaching to support trainees. The department supports a number of publichealth trainees. It also runs educational sessionson a range of topics and is an accredited WHOCollaboration centre.54<strong>Wandsworth</strong> Teaching Primary Care Trust
Appendix 2Choosing healthA2.1<strong>In</strong>troductionA2.3<strong>Health</strong>y Living ProgrammeA2.2The government’s white paper on Public <strong>Health</strong>(Choosing <strong>Health</strong> 2004) sets out a strategy forhealth improvement. It recognises that smallchanges in the choices people make can make bigdifferences; preventing many major lifestyle illnessesand also assisting in the management of associatedconditions. The Choosing <strong>Health</strong> policy includesrecommendations that local health plans shouldhave strategies and programmes which focus onimproving and sustaining healthy communities byenabling individuals to take more control of theirhealth and well being.Implementing Choosing <strong>Health</strong> in<strong>Wandsworth</strong>The <strong>Health</strong>y Living Programme has been designed tocomplement work that has already been established,is successful and has a proven evidence base. Theprogramme is intended to add value to work alreadybeing undertaken. It also supports local prioritiesto improve health and well being and reduceinequalities such as:• Enabling healthier individuals and communities• Supporting the reduction of long term unavoidablechronic conditions• Supporting improvements to increase lifeexpectancy particularly in deprived wards.The programme consists of three elements:During 06/07 plans to implement the preliminaryphase in the delivery of Choosing <strong>Health</strong> objectiveswere approved and funded. The criteria for selectinginitiatives included:<strong>Health</strong>y Living Programme• Being in line with Choosing <strong>Health</strong> priorities1. Develop <strong>Health</strong> Promotion Capacity• Implementing recommendations from the previousPublic <strong>Health</strong> report (2004)Development of knowledge, skills and expertise• Working towards reducing morbidity or mortality• Reduces inequalities2. <strong>In</strong>crease Access to <strong>Health</strong>y Living Advice• Supports the achievement of national targets orlocal objectives.Choosing health plans were developed in three phases:Supporting behaviour change1. <strong>Health</strong>y Living programme, whichmainstreamed aspects of two healthy livingnetworks, previously funded from NewOpportunities monies.2. <strong>Health</strong> Trainer programme in order toprovide personal and practical support in theimplementation of individual health plans.3. A series of prevention and early interventionservices developed through consultation thatincluded the Council and other stakeholders.3. Support Positive LifestylesMaintaining behaviour changeSupportive local services<strong>Health</strong> promotion capacity focusing on thedevelopment of skills in the local communityto improve health through informed choices byempowering individuals and community leadershipto advocate health action.<strong>In</strong>crease access to healthy living advice by putting inplace service infrastructure which enables better access.Support positive lifestyles through theestablishment and development of partnershipswith key stakeholders in the statutory and voluntarysector to ensure initiatives are in place to sustainpositive health changes.<strong>Wandsworth</strong> Teaching Primary Care Trust 55
Appendix 2: Choosing <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07A2.4<strong>Wandsworth</strong> <strong>Health</strong> Trainer ProgrammeThe <strong>Wandsworth</strong> <strong>Health</strong> Trainers Programme iscomplementary to the <strong>Health</strong>y Living Programme,having been developed upon the same principlesoutlined above. <strong>Health</strong> trainers are facilitatorsand sign posters to better health and socialcare. Importantly they are a workforce, madeup of non-health professionals from a variety ofbackgrounds, who have a good knowledge of theirlocal communities. This approach seeks to useapproachable people ‘from next door’ rather thanprofessionals ‘from on high’ to facilitate positivehealth changes.<strong>Health</strong> trainers are employed, trained and accreditedby the NHS. They have various roles determined bythe local need of the community from which theyare drawn and work.As they are from the communities in which theywork as health trainers they:• Are more in touch with daily realities of people intheir community• Are aware of local resources and services• Have a shared stake in improving the health oftheir communityA2.4.1• Helping individuals tackle wider issues that mightbe impacting on their ability to live healthily suchas access to other health and social care facilities.Positive Behaviour ChangeAn important aspect of the health trainer role isthe engagement with individuals with the aim ofempowering them to take control of their healthbefore significant and irreversible damage is done.<strong>Health</strong> trainers give personal health advice throughone to one sessions or in group settings. Thisadvice is based on an evidence base of a systematicapproach to advice and support. An example ofthis is the theoretical and working knowledge ofthe stages of behaviour change. (See figure A2.1)By understanding an individual’s position within thecycle of change, health trainers can provide tailoredadvice and information. Clients of health trainershave personalised health plans, which includepractical actions to apply and sustain positive healthchanges. This consists of preparing for change,setting goals, recognising barriers and monitoringprogress. Importantly health trainers provideencouragement and support as and when needed.The Stages of Change(Transtheoretical) ModelFigure A2.1 The Stages of Change(Transtheoretical) Model• May have more access to hard to reach anddisadvantaged groups.<strong>Wandsworth</strong> teaching Primary Care Trust issupporting the implementation of the NHS nationalstrategy for <strong>Health</strong> Trainers and has agreedprogramme funding. The programme builds on thePrimary Care Trust’s role as a teaching organisationand the Public <strong>Health</strong> Department reputation as anaccredited training unit.The Public <strong>Health</strong> department aims to recruit sevenhealth trainers from the community to assist thosewho are vulnerable and who are at risk for damagingtheir health in the long term. The key tasks for<strong>Wandsworth</strong>’s health trainers include:• <strong>In</strong>creasing service access in areas such as screeningand immunisation, smoking cessation, weightmanagement, physical activity and mental healthpromotion• Supporting the delivery of the obesity and physicalactivity strategiesStartPrecontemplation:Client sees noproblem butothers disapproveRelapse:Return topreviouspattern ofbehaviourMaintenance:ActivelymaintainingchangeContemplation:Weighing uppros and conson changingOptimal recoveryChange consolidatedSource: Prochaska and DiClemente (1984)Active changes:Putting decisioninto practicePrematureway out• Encouraging and supporting people to maintainpositive health changes56<strong>Wandsworth</strong> Teaching Primary Care Trust
Appendix 2: Choosing <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07A2.5Building on Firm FoundationsA2.5.3Support Positive LifestylesA2.5.1Developing <strong>Health</strong> Promotion CapacityMaintaining Behaviour ChangeA2.5.2Development of Knowledge, Skills and Expertise<strong>Health</strong> Trainers from the Community.The Public <strong>Health</strong> community developmentprogramme has a proven track record of workingwith local communities to build health promotioncapacity. For a number of years the public healthdepartment has run a serious of successfulcommunity development and health courses. Thesecourses are University accredited and provide anexcellent springboard for community members todevelop advocacy skills in health. These courseshave enabled local people to gain knowledge andskills, which they have used for the benefit of theircommunities, families, and friends. Successfulparticipants have been involved in stop smokingevents, helped with local research, supported healthsessions and have run social prescribing sessions ingeneral practice.The community development and health course isa building block for the <strong>Wandsworth</strong> health trainerframework. It acts as a first step and catalyst forparticipants who may wish to become candidates forthe <strong>Wandsworth</strong> <strong>Health</strong> Trainer programme whenfully developed.<strong>In</strong>crease Access to <strong>Health</strong>y Living AdviceSupporting Behaviour Change<strong>Health</strong> Trainers Supporting <strong>Health</strong>y LivingThe implementation of a ‘Footsteps’ lifestyle‘taster’ referral scheme through general practice iscurrently being cascaded across the borough. GPreferred patients are offered advice and support onstopping smoking, becoming physically active, eatinghealthily and stress management. The health trainerprogramme when fully operational will enhancethe co-ordination of this initiative by supplementingaccess to community health advice and support.Supporting Structure for <strong>Health</strong> TrainersThe success of the <strong>Health</strong>y Living programmes inTooting and Battersea has left an infrastructure thathas supported local capacity building through anextensive network of local community and voluntarygroups. Both programmes targeted the harder to reachcommunities focusing on lifestyle interventions forhealth and well being. The relationship with voluntaryand community groups built over many years hasbeen maintained and local venues could act as a basefrom which health trainers can function. Work is alsounderway to create a health promoting network withsupport from the voluntary sector. Combined, theserelationships and networks will provide support andsustain the work of health trainers and their clients.<strong>In</strong> addition these networks will also act as recruitinggrounds for local health trainers.<strong>Health</strong> Trainers in the PrisonPublic <strong>Health</strong> has worked with <strong>Wandsworth</strong> Prisonto take forward the health trainer programme incollaboration with the prison’s physical educationdepartment, CSIP, and NHS <strong>London</strong>. The initiativeforms part of prisoner rehabilitation and releaseprogrammes. Nine prisoners have completed thepilot and were awarded certificates by the Mayor of<strong>Wandsworth</strong> at a celebration, joined by their families.<strong>In</strong> 2006 the Secretary of State, Patricia Hewitt, visiteda stress management session. A DVD has beendeveloped by NHS <strong>London</strong> showcasing the healthtrainer initiative as a national example for goodpractice in prisons. The health trainer course hasbeen accredited through the Open <strong>College</strong> Network.Following national evaluation 2007/08 the PhysicalEducation Department at H.M.P <strong>Wandsworth</strong> hasbeen funded to deliver three further courses.The Public <strong>Health</strong> department has run a series ofsuccessful ‘staying healthy’ MOT events, across theborough. These events have screened and givenadvice on cholesterol and blood pressure to a rangeof public groups. Advice is also given on stoppingsmoking, increasing physical activity and weightmanagement. Once established <strong>Wandsworth</strong> healthtrainers will run a series of events throughout theyear in community settings.<strong>Wandsworth</strong> Teaching Primary Care Trust 57
Appendix 2: Choosing <strong>Health</strong><strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07A2.6<strong>Health</strong> Improvement Projectsand <strong>In</strong>itiativesA range of health improvement projects has beenresourced covering alcohol, young people, andmental health. Evaluation measures for each initiativehave been drawn up and implementation has begun.1.2.To reduce the negative effects of alcohol abuseon the individual and the community––––Safe drinking Co-ordinatorTo co-ordinate and deliver harm reductionand sensible drinking initiativesBrief <strong>In</strong>terventions workerTo offer brief interventions to people fromthe criminal justice system and/or the localaccident and emergency services.To support young people to make healthychoices for their lifestyle4.To promote mental well-being and prevent anissue from developing into a problem that couldrequire treatment.––––––Developing Mental <strong>Health</strong> courseTo cover Personal Social and <strong>Health</strong> Education(PSHE) in schools for children and youngpeople. Training staff to become ‘experts’,and offering postgraduate qualifications tocover the areas of alcohol, suicide, self harm,bereavement, young carers, and safeguardingchildrenPostnatal depression training for staffTo set up a self sustaining postnataldepression course for health visitorsMental <strong>Health</strong> Promotion co-ordinatorTo revise the mental health strategies, torun events, provide education, consultancyand advice.––Obesity in schoolsTo work with key schools to develop,implement and evaluate a school nutritionpolicy. To assist and advise schools oneffective promotions–– Total <strong>Health</strong> @ <strong>Wandsworth</strong> (THAW) projectextensionTo extend the health and well-being outreachand awareness service for young people.5.To support initiatives that specifically targetvulnerable and at risk groups––––Women’s <strong>Health</strong> Drop in RoehamptonTo launch a drop in service for womenconcerning all aspects of well beingBCG Catch Up CampaignTo help launch the immunisation campaign inschools to capture those at risk.3.To support early diagnosis and treatment foraspects of sexual health–– Community sexual health clinics for YoungPeopleTo increase the opening hours at three sexualhealth clinics and to enhance the service inone family planning clinic to include sexuallytransmitted infection (STI) screening.58<strong>Wandsworth</strong> Teaching Primary Care Trust
Appendix 3Examples of Public <strong>Health</strong> <strong>In</strong>itiativesThe following table illustrates broad areas of general public health work programmes captured within the CommissioningStrategy Plan. The table demonstrates the focus of these areas across life stage events. The delivery of these programmes willrequire input and the support of key stakeholders such as the Local Authority, voluntary and community groups.Life StagesArea ofWork Title AimPregnancy/Pre-School(0–5)8% popSchool/Adolescent(6–16)11% popYoungpeople(17–25)13% popAdulthood(26–64)59% popElders(65+)9% popChild healthImplementation of HPVimmunisationImplement a vaccination programme for girls’12–13-year eligible in <strong>Wandsworth</strong> from Sept 08.YoungpeopleAlcohol anddrugsSexual<strong>Health</strong>PhysicalactivityImplementation ofMMR action plan<strong>College</strong> <strong>Health</strong>Improvement StrategyCommunity SmokingAdvisers<strong>Health</strong>y LivingOutreach ServiceBlood Borne Virus(BBV) ServiceHIV/STI’s healthpromotionTotal <strong>Health</strong> @<strong>Wandsworth</strong>Brook and Men (BAM)Condom DistributionSchemeChlamydia ScreeningBattersea WalkingProgramme“Train Thyself!”Physical Activity CarePathway PilotNetwork of PhysicalActivity Clinics.Promotion of ActiveTransportPedometers in SchoolsLoan Scheme“Smart Links”Falls and <strong>In</strong>juriesPrevention ExerciseWalk and Ride: AHome Exercise PilotOsteoporosis ExerciseClinicsChair based exercise.Survey of provision ofexercise services.To increase childhood immunisation rates in<strong>Wandsworth</strong>.To build health promotion capacity within SouthThames <strong>College</strong>.Reduce smoking uptake in young people throughusing Youth and Key Workers.Targeted at young people in Roehampton andBattersea.To increase numbers of service users who arescreened and successfully treated for BBVs.Reduction in the incidence of HIV infection withinAfrican communities.Outreach sexual health service for young people.Aimed at improving health outcomes for youngmen in some of the most deprived wards.To promote safer sex and reduce the incidence ofsexually transmitted infections.To reduce the incidence of sexually transmittedinfections.To establish a series of volunteer led walkinggroups in Battersea.Helping participants to build more physical activityinto their daily activities.Practice nurses have been trained to deliver briefinterventions on physical activity.To extend network of Physical Activity Clinics(PACs) across <strong>Wandsworth</strong>.<strong>In</strong>crease the number of people using activetransport (walking and cycling).Using pedometers to increase physical activity insedentary children.Improving access of obese patients or patients withmental health issues to physical activity services.Targeted exercise in those at risk of having a fall ispart of NICE guidelines on Falls Prevention.To increase the number of people using publictransport.Monthly exercise classes for independently livingpatients with diagnosed osteoporosis.To increase the level of physical activity inresidents of sheltered housing schemes.To establish the prevalence of falls in nursinghomes and residential care centres.<strong>Wandsworth</strong> Teaching Primary Care Trust 59
Appendix 3: Example of Public <strong>Health</strong> <strong>In</strong>itiatives<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Life StagesArea ofWork Title AimPregnancy/Pre-School(0–5)8% popSchool/Adolescent(6–16)11% popYoungpeople(17–25)13% popAdulthood(26–64)59% popElders(65+)9% popObesityObesity – Children andYoung PeopleReducing the increase in obesity rates in childrenunder 11 years.CommunityDevelopmentObesity – Adults andPublic <strong>Health</strong>CommunityDevelopment‘Heart of Roehampton’Raising Awareness ofDomestic AbuseBattersea SocialPrescribing projectA healthier workforce and improved managementof morbid obesity.Course to develop health skills and knowledge inorder to become community health advocates.Older People Outreach to reduce isolation andbuild capacity to address health and social issues.Working with women to develop a communityresource.Finding alternative non-medical solutions viainterest groups and self-help initiatives.Mental<strong>Health</strong>Smoking<strong>Health</strong>yLivingMental health steppedcare modelGraduate primary caremental health workersBooks on prescriptionLiving and learningBME Mental healthneedsMental healthpromotion postCare pathwaysCo-creating healthprogrammeMidwife smokingcessation trainingComputer AssistedBrief <strong>In</strong>terventionExtension of service toDental PracticesExtension of service toMental <strong>Health</strong> UnitsLow <strong>In</strong>come GroupsSmoking ProgrammeSmoke-free workplacesprojectExtension of service toGP’s and PharmaciesSmoking cessation inHMP <strong>Wandsworth</strong>.Footsteps lifestylereferral programme<strong>Health</strong> promotion andhealth trainerTB commissioningrecommendationsImproving Access to Psychological Therapies(IAPT) in Putney and Roehampton.Aimed at helping progress the primary carestepped care model.Providing a range of carefully selected self helpmaterials in cooperation with <strong>Wandsworth</strong> libraries.Offering stress management courses, aimed atpersonal development.Scoping exercises to document mental healthneeds of black and minority ethnic communities.To develop the implementation of the 10:10mental health promotion strategy.Provision of care pathways from primary care to afull range of evidence based interventions.Enable more people with chronic or recurrentdepression to take back control over their illness.Reducing smoking during pregnancy.To design and pilot a new computer based tool(CABI) for use in quit-smoking support.To train up and include dental practicioners ascommunity advisors with the Stop SmokingService.To offer a tailored, quit smoking support service toin-patient units at Springfield Hospital.To achieve four-week quits in deprived wards.Highlighting second hand smoke risks and reducingsmoking uptake among young employees.<strong>In</strong>crease the number of GP practices andpharmacies with improved levels of participation.Establishing smoking cessation as a core service.Lifestyle support to reduce risk factors related tocardiovascular disease, cancers and well-being.Put in place and evaluate a borough wide healthimprovement training programme.Implementation of recommendations to deliver onthe 1–9 <strong>London</strong> TB good practice targets.60<strong>Wandsworth</strong> Teaching Primary Care Trust
Appendix 4Clinical EffectivenessA4.1ScopeClinical effectiveness is an important aspect ofcommissioning health care for the population.This brief appendix outlines the role of clinicaleffectiveness in underpinning safe, cost effectiveand clinically effective healthcare. It explains theparticular contribution that the Clinical EffectivenessGroup within Public <strong>Health</strong> has made.<strong>Wandsworth</strong> PCT pays for just about all NHSservices for people living in <strong>Wandsworth</strong> and peopleregistered with <strong>Wandsworth</strong> GPs using taxpayers’money, although patients themselves make extracontributions for some elements of health care atthe time they need them, including prescriptions,dentistry and optometry. The PCT has to fund allhospital services (for example, all operations, tests,outpatients and accident and emergency), GeneralPractices, screening services and community services,for example, family planning and health visitors.New ways of treating, preventing and testing fordisease are being invented all the time. Just inthe last few years, there have been hundreds andhundreds of new developments (Box A4.1).Box A4.1: Some exciting new developments in health careA4.2Excellence (NICE), the National Screening Committeeand the Joint Committee for Vaccination andImmunisation. But sometimes this guidance is slowto be published, and, for most new developments,central committees never produce any firm guidanceand PCTs are left to decide what to fund dependingon their local circumstances. Yet PCTs are specificallyrequired to make decisions on whether or not tofund new developments based on an assessment ofneed, effectiveness and cost-effectiveness.Clinical Effectiveness GroupAdvising the PCT on what to pay for and what not topay for is a key role of the Public <strong>Health</strong> Department,and, in particular, of the Clinical Effectiveness Group.The advice requires an analysis of effectiveness,cost-effectiveness, safety and need for differentnew developments that health professionals andpatients may request (often with pressure frompharmaceutical companies), which often involvesinterpretation of complex scientific research.Sometimes the Public <strong>Health</strong> Department will advisethat the PCT does not fund a new development untilbetter evidence is available, because the evidencethat it will really benefit the people of <strong>Wandsworth</strong>is uncertain, or if there are concerns about safety.• Screening for bowel cancer• Vaccine against human papilloma virusThe Public <strong>Health</strong> Department Clinical EffectivenessGroup also assesses all Clinical Guidelines producedby the PCT, ensuring that they are based on a carefulassessment of the evidence and do not pose a risk topatients or other members of the population (Box A4.2).• New drugs for eye disease and cancers• Techniques for unblocking arteries at the time of a heartattack (primary angioplasty).Box A4.2: Examples of recent guidelines assessedby the Clinical Effectiveness Group• Guidelines for the management of depressionThe Department of Public <strong>Health</strong> believes that peopleeligible for NHS care should have access to newdevelopments that are likely to improve their healthand well being significantly. We believe that one ofthe richest countries in the world should be able toprovide a first class service for its population – basedon ability to benefit, and not on ability to pay.• Weight management guidelines• Guidelines for the management of hypertension, angina andhyperlipidaemia in primary care• Guidelines for the primary prevention of cardiovasculardisease in primary careNew treatments, services, prevention programmesand tests are often very expensive and PCTs haveto keep within budget. So how does <strong>Wandsworth</strong>PCT decide whether to fund them for the people of<strong>Wandsworth</strong>? And what not to fund? The NHS andother government agencies produce some guidancefor PCTs on what they should pay for – for example,in National Service Frameworks, and guidancefrom the National <strong>In</strong>stitute for <strong>Health</strong> and Clinical• Guidelines on beta-blockers in heart failure• Guidelines on antiplatelet treatments in primary careThe Clinical Effectiveness Group also providesevidence reviews for the south west <strong>London</strong> EffectiveCommissioning <strong>In</strong>itiative, which aims to promote<strong>Wandsworth</strong> Teaching Primary Care Trust 61
Appendix 4: Clinical Effectiveness<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07clinical quality and equity of access, helping toensure that local health services are appropriate, safeand effective (Box A4.3)Box A4.3 The south west <strong>London</strong>effective commissioning initiative• Sets criteria that patients should meet before they areoffered certain procedures, based on a careful assessmentof the evidence, so that:–– Procedures are available to those who are likely to benefit–– People are not exposed to risk of unnecessary procedures–– Transparent guidelines are applied – across the whole ofSouth West <strong>London</strong> – consistently.• Procedures covered so far:–– Cosmetic surgery–– Surgery for carpal tunnel syndrome–– Surgery for varicose veins–– Hysterectomy for heavy menstrual bleeding–– Surgery for minor skin lesions• More information is available on the PCT website (http://www.wandsworth-pct.nhs.uk/work/GPReferral/Referral/effectivecommissioning.aspMuch of the work of the Clinical Effectiveness Group isavailable on the PCT website: http://www.wandsworthpct.nhs.uk/Public<strong>Health</strong>/CEG/default.asp#62<strong>Wandsworth</strong> Teaching Primary Care Trust
Appendix 5<strong>Health</strong> <strong>In</strong>telligenceThe <strong>Health</strong> <strong>In</strong>telligence Unit within Public <strong>Health</strong> hasthe following core functions:1.2.3.4.<strong>In</strong>novation (new developments in sourcing,presenting and directing the decision makingprocess)Modelling (applying statistical, economic andepidemiological techniques to predict and planthe health economy)Research (scanning current literature fordevelopments in health/health care deliveryincluding the impact of new technologies andclinical practices).Monitoringa. Establishing a routine mechanism forinforming all stakeholders of health statusand health utilisation of the health economyb. Evaluating the impact of targetedinterventions within the health economy5.Co-ordinating the input of staff from<strong>Wandsworth</strong> PCT, St George’s Hospital NHSTrust, and <strong>Wandsworth</strong> Local Authority into thework of the <strong>Health</strong> <strong>In</strong>telligence Unit.Table A5.1 demonstrates the source of a number ofhealth indicators that are commonly available. Thestructure of the analyses concerns demography,measures of deprivation, risk factors for health,utilization of health services, and mortality. TableA5.2 gives these indicators for each of the twentywards in <strong>Wandsworth</strong>.<strong>Wandsworth</strong> Teaching Primary Care Trust 63
Appendix 5: <strong>Health</strong> <strong>In</strong>telligence<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table A5.1 Framework for Picture of <strong>Health</strong> <strong>In</strong>dicators 2007Data <strong>In</strong>dicator Source Definition DetailsPopulationGP RegisterHospitalAdmissions/AttendancesPopulation in 2007 GLA 2006 Round population mid-year estimatesNo of people one ward, cases are divided bythe proportion from each ward.SAR= 100 indicates that the ward hasan average admissions rate, > 100indicates a higher than average rate, 100 indicatesa higher than average mortality,
Appendix 5: <strong>Health</strong> <strong>In</strong>telligence<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table A5.1 Framework for Picture of <strong>Health</strong> <strong>In</strong>dicators 2007 (continued)Data <strong>In</strong>dicator Source Definition Details% of singleton live births < 2500 g ONS Low birth weight is defined by theWHO as a birth weight < 2500 gMMR 2nd year cohort for FY 2006/7Children on child protection register (as% of total on register)Children in need (as % of total)COMWISECommunitysystemChildren’sServices,<strong>Wandsworth</strong>Local Authority,as at 31/3/07The child protection register is aconfidential list of names of childrenwithin <strong>Wandsworth</strong> who are believedto be at risk of significant harm. Thismay be from physical abuse, emotionalabuse, sexual abuse or neglect.Children in need are defined as childrenaged under 18 years who need localauthority services to achieve/maintaina reasonable standard of healthor development and/or to preventsignificant or further harm to health ordevelopment and/or are disabled.Emergency admissions – children < 16 Vital Signs 2007 Emergency hospital admissions rate forchildren aged 16 years and underTeenage conceptions (females aged 15–17)Child and Adolescent Mental <strong>Health</strong>Services (CAMHS) utilisationTeenagePregnancy Unit2002–04SWL & StGeorge’s NHSTrust, RioConception rate per 1,000 femalesaged 15–17 yearsReferral rate to <strong>Wandsworth</strong> CAMHSElderly % population over the age of 65 GLA 2006 Round population mid-year estimatesSexual <strong>Health</strong>Obesity% population over the age of 75 GLA 2006 Round population mid-year estimatesLone pensioner households (Numberand % of all households )Number of Over 65’s with LLTI (% of allover 65s)Census 2001Census 2001Emergency Admissions in population 65+ Vital Signs 2007Number of Family Planning ClinicAttendances (Number of sessions),April–August 2006% Obese children in Reception% Obese children in Year 6Family Planning<strong>Wandsworth</strong> PCT2007Data collected for school height andweight measurements. Used age andgender-specific body mass index (BMI)cut-offsBirth weight-specific infant mortalitybegins to rise rapidly below 2500 g(Kramer, 1987)*Ward level data for females aged13–15 is not reliableData based on pupil’s ward ofresidence (home address). 55 Primaryschools participated.Population (continued)*Kramer, M. S. (1987). Determinants of low birth weight: methodological assessment and meta-analysis. Bulletin of the World <strong>Health</strong> Organization 65: 663–737.**Twigg L, Moon G, Walker S. The Smoking Epidemic. <strong>London</strong>: <strong>Health</strong> Development Agency, 2004.<strong>Wandsworth</strong> Teaching Primary Care Trust 65
Appendix 5: <strong>Health</strong> <strong>In</strong>telligence<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table A5.1 Framework for Picture of <strong>Health</strong> <strong>In</strong>dicators 2007 (continued)Data <strong>In</strong>dicator Source Definition DetailsSmokingLLTIMental <strong>Health</strong>CervicalScreeningEstimated number of smokers in adultpopulation% of people with Limiting Long TermIllnessAdults (16–74) suffering from someform of neurotic disorderHospital admissions under the “adultmental illness” speciality (rate per100,000 population)People with a learning disability helpedto live at homePeople with a mental health problemhelped to live at homeCommunity Mental <strong>Health</strong> Teamsoutpatient/community appointmentsAmbulance call outs for drug overdose,2006/07Percent of patients aged 25–64 whohave had smear in past 3–5 years<strong>Health</strong>DevelopmentAgency**Census 2001Psychiatricmorbidity surveySUS 2007<strong>Wandsworth</strong>Local Authority,social careservicesMental <strong>Health</strong>Disability RegisterSWL &St George’s NHSTrust, Rio<strong>London</strong>AmbulanceService, as at31/1/08PCSS, December2007Primary Care No of GP practices QMAS, October2007No of patients registered with a GP(within <strong>Wandsworth</strong> wards)% of <strong>Wandsworth</strong> registeredpopulationExeter systemExeter systemPharmacy Data No of Pharmacies <strong>Wandsworth</strong> PCT2005Economic and Social CareTotal no of prescription items dispensedin one year<strong>Wandsworth</strong> PCT2008Economic Unemployment, JSA claimant counts Nomis September2007Social ServicesChildren < 16 living in householdsdependent upon income supportLone parent claimantsYounger physically disabled peoplehelped to live at homeDWP tables, April2006Nomis February2007<strong>Wandsworth</strong>Local Authority,social careservicesNumbers from literature based PCTestimate crudely applied to wardpopulation.Secondary user serviceNumber of residents (< 65) on theLearning Disability Register, rate per1,000 populationNumber of residents (< 65) on theMental <strong>Health</strong> Disability Register, rateper 1,000 populationNumber of appointments from eachward as a percent of the total numberof appointments in <strong>Wandsworth</strong>Based on first responses where anarrive at scene time is recorded andPRF illness code is recorded as 21(drug overdose) or information givenat time of call indicates drug overdoseJobseeker’s Allowance claimant countsas percent of resident working agepopulationRate per 1,000 children aged < 16yearsLone parent claimant counts aspercent of total number of residentclaimantsNumber of residents (< 65) on thePhysical Disability Register, rate per1,000 populationOlder people helped to live at home Social Services Number of residents (65+) on register,rate per 1,000 population 65+*Kramer, M. S. (1987). Determinants of low birth weight: methodological assessment and meta-analysis. Bulletin of the World <strong>Health</strong> Organization 65: 663–737.**Twigg L, Moon G, Walker S. The Smoking Epidemic. <strong>London</strong>: <strong>Health</strong> Development Agency, 2004.66<strong>Wandsworth</strong> Teaching Primary Care Trust
Appendix 5: <strong>Health</strong> <strong>In</strong>telligence <strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table A5.2 Picture of <strong>Health</strong>, January 2008Population Latchmere Roehampton Queenstown Tooting Graveney FurzedownSt Mary’sPark West Hill Shaftesbury Bedford Earlsfield West Putney Fairfield Nightingale Balham East Putney<strong>Wandsworth</strong>Common Southfields Northcote Thamesfield <strong>Wandsworth</strong>Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number NumberPopulation in 2007 13,840 14,899 15,619 15,076 14,819 14,696 15,624 15,474 13,305 14,354 14,192 13,641 13,660 14,426 13,951 14,462 14,470 15,636 13,912 14,439 290,495No of people
Appendix 5: <strong>Health</strong> <strong>In</strong>telligence <strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table A5.2 Picture of <strong>Health</strong>, January 2008 (continued)Population (continued)Latchmere Roehampton Queenstown Tooting Graveney FurzedownSt Mary’s<strong>Wandsworth</strong>Park West Hill Shaftesbury Bedford Earlsfield West Putney Fairfield Nightingale Balham East Putney Common Southfields Northcote Thamesfield <strong>Wandsworth</strong>Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*) Number (Rate*)Children Total Births, 2007 248 189 203 103 176 176 224 197 225 140 235 127 247 250 208 174 235 288 270 193 4108Births to women
Appendix 5: <strong>Health</strong> <strong>In</strong>telligence <strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Table A5.2 Picture of <strong>Health</strong>, January 2008 (continued)Primary Care Latchmere Roehampton Queenstown Tooting Graveney FurzedownSt Mary’s<strong>Wandsworth</strong>Park West Hill Shaftesbury Bedford Earlsfield West Putney Fairfield Nightingale Balham East Putney Common Southfields Northcote Thamesfield <strong>Wandsworth</strong>Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number NumberGP data No of GP practices 1 4 1 0 4 3 2 4 2 3 2 3 1 5 3 2 0 5 3 2 51No of patients registered with a GP(within <strong>Wandsworth</strong> wards)12,987 20,616 17,043 3,257 18,347 14,120 23,876 13,435 14,330 14,712 24,422 13,503 2,718 34,212 13,750 14,687 2,256 33,264 15,291 19,371 326,196% of <strong>Wandsworth</strong> registered population 3.98 6.32 5.22 1.00 5.62 4.33 7.32 4.12 4.39 4.51 7.49 4.14 0.83 10.49 4.22 4.50 0.69 10.20 4.69 5.94PharmacyDataNo of Pharmacies 3 5 2 4 4 4 2 3 2 2 3 3 2 5 2 2 0 7 6 3 64Total no of prescription items dispensed inone year149,532 243,376 123,312 167,808 203,560 185,872 164,244 161,308 81,256 127,528 218,920 105,356 44,984 187,368 66,564 153,260 N/A 281,264 187,588 80,436 2,933,536Source: A Pharmaceutical Needs Assessment for <strong>Wandsworth</strong>, 2005WPCT Community Pharmacy Lead, Jan 2008Economic and Social Care Latchmere Roehampton Queenstown Tooting Graveney FurzedownSt Mary’s<strong>Wandsworth</strong>Park West Hill Shaftesbury Bedford Earlsfield West Putney Fairfield Nightingale Balham East Putney Common Southfields Northcote Thamesfield <strong>Wandsworth</strong>Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number Number NumberEconomic Unemployment, JSA claimant counts ‡(% of resident working age population)405(4.5%)Children
<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Staff in the Public <strong>Health</strong> Departmentat 20 February 2008Public <strong>Health</strong> DepartmentOrganisational Chart20 February 2008Serena GebbelsPA to DPH0.5 WTEJane RoderickPA to DPHProfessor Salman RawafDirector of Public <strong>Health</strong>Director of <strong>Wandsworth</strong>World <strong>Health</strong> OrganisationCollaboration CentreElizabeth DuboisAssociate DirectorEconomist<strong>Health</strong> <strong>In</strong>telligence UnitEdmund CheckleyEmergency PlanningLiaison OfficerNick KendallDental PH ConsultantEmployed byCroydon PCTHugo Van WoerdenCPHMMental <strong>Health</strong>VACANTCPHMMaternity &Child <strong>Health</strong>Ros LoboAssociate Director/PH Specialist<strong>Health</strong> PromotionMary GomezPA/Team SecretaryVelena GilfillianDeputy Directorof Public <strong>Health</strong>ProvidersJohn ThomasCPHMSexual <strong>Health</strong>Helen DrainPA to Consultats in PHVACANTCPHMAcute Services & ClinicalEffectivenessLaurence GibsonAssociate DirectorEpidemiologist<strong>Health</strong> <strong>In</strong>telligence UnitNick BeavonChief PharmacistWPCTRosie SmithCommunity PharmacyServices PharmacistEmployed by KHTVACANTMental <strong>Health</strong>Promotion Specialist<strong>Wandsworth</strong>Isaac OjoStop SmokingService ManagerVACANT<strong>Health</strong>y LivingManagerSamara HammondImprovementManagerSexual <strong>Health</strong> & HIVTed PoulterOlder People &Physical ActivityLeadAnupam GarribPublic <strong>Health</strong>StrategistMichelle WuPublic <strong>Health</strong>StatisticianPam ShepherdOffice ManagerSita PatelPrescribingAdvisorVACANTCommunity DevelopmentCoordinator Putney &Roehampton0.5 WTEAnna D‘ArcyPublic <strong>Health</strong>DieticianVACANTPublic <strong>Health</strong>Resource UnitManagerMaureen VidalAdministratorLisa McNallyTobacco ControlManagerVACANTFemale SexProject WorkerEmily De NobregaSpecialist ExercisePractitionerChildren, YP & LTCAlistair JohnstonPublic <strong>Health</strong>KnowledgeManagerSally BahriPublic <strong>Health</strong>Research OfficerCarol EllisTeam SecretaryStella Oluwole OjoGP PrescribingSupport PharmacistBrenda HerbertCommunity DevelopmentCoordinator Putney &Roehampton0.5 WTEGraeme Markwell<strong>Health</strong> ImprovementCoordinator/Young PeopleRobin AustinPublic <strong>Health</strong>CampaignsOfficerAbiolaBankole-AdekunleBattersea Cluster StopSmoking CoordinatorKate SaxtonSmoking Cessation Advisorfor Low <strong>In</strong>come Groups0.5 WTERose LaguSexual <strong>Health</strong>/HIVBlack AfricanOutreach WorkerKaren GrayCervical ScreeningNurseMelissa CottingtonPublic <strong>Health</strong>Research OfficerAndy ElmerTravel PlanCoordinator0.5 WTEMary BoucherGP PrescribingSupport Pharmacist(starts 17 Dec)Elaine CurleyCommunity DevelopmentCoordinatorAnne-LouiseMiddletonBlood BorneVirus NurseVACANTPrison WorkerVACANTPutney & RoehamptonCluster Stop SmokingCoordinatorMichael NayagamAdvocacy ServiceCoordinator0.8 WTEAnne PattersonTeenage PregnancyCoordinator0.7 WTEAseel HergaziPublic <strong>Health</strong> DoctorChild <strong>Health</strong>Department(6.3 wte)Gary BradleyGP PrescribingSupport TechnicianAsmat NisaCommunity DevelopmentCoordinator <strong>Wandsworth</strong>Christine YenPublic <strong>Health</strong>NutritionistVACANTAlcoholCoordinatorVACANT<strong>Wandsworth</strong> South ClusterStop Smoking Coordinator0.5 WTEMatthew Robinson<strong>Health</strong>y LivingTeam Project Office0.5 WTEKate MilstedTeenage PregnancyAdvisorSilvana UnigwePublic <strong>Health</strong> Doctor(starts 3 Dec)Betty AtipoeImmunization NurseLeadVACANTHeart of RoehamptonOlder Persons CoordinatorMaxine RhodesStop SmokingServices FacilitatorVACANT<strong>Health</strong>y LivingTeam Project Officer0.5 WTEJanine RailtonSWAGNET Manager(Employed by WPCT)Kate HaireSpecialist RegistrarPost Funding:WPCTWPCT Vacant PostsLeanne BobbSWAGNET Administrator(Employed by WPCT)Azhar HafeezSTI GPSWL PCTsLAADEANERYPBC ClustersTeenage Pregnancy70<strong>Wandsworth</strong> Teaching Primary Care Trust
GlossaryTerm Abbreviation ExplanationAccident and Emergency A&E The part of the hospital concerned with the immediate treatment of patientswho have had an accident or who require medical or surgical emergency care.Age-specific rate ASR An age-specific rate is the rate measured in a particular age group. Thenumerator and the denominator for this rate refer to the same age group,that is, both have the same age distribution.Asylum SeekersAsylum seekers are people who have made a claim for asylum, but whosecase has not been decided.Body Mass <strong>In</strong>dex BMI A measurement of the relative percentages of fat and muscle mass in thehuman body, in which weight in kilograms is divided by height in metres andthe result used as an index of obesity.Cardiovascular disease CVD Diseases of the heart or blood vessels, also called circulatory diseases.CensusEvery ten years the nation has set aside one day for the Census – a count of allpeople and households. It is the most complete source of information about thepopulation that we have. The latest Census was held on Sunday 29 April 2001.Chief Medical Officer CMO The Chief Medical Officer (CMO) is the Government’s principal medicaladviser and the professional head of all medical staff in England. The annualreport of the Chief Medical Officer provides an important survey of thenation’s health and reports the main challenges faced by the Government intackling public health problems.Chronic diseaseCirculatory diseaseA disease, condition or health problem which persists over a long period oftime. The illness may recur frequently and in some cases may lead to partial orpermanent disabilities. Examples include, arthritis, diabetes and hypertension.Diseases affecting the circulation of blood in the heart, arteries, capillaries or veins.Clostridium Difficile C-diff C. diff is a bacteria present in the gut of some people. Some types ofantibiotics can cause C. diff bacteria to multiply and cause symptoms such asdiarrhoea and fever.CommissioningCommissioning is the strategic planning and resource allocation functionof the NHS, mostly done by Primary Care Trusts (PCTs). It involves buyingin services from a range of health service providers (including GPs, dentists,and community pharmacists, NHS and private hospitals, and voluntary sectororganisations) to meet the health needs of local people, and monitoring howwell they are being delivered.Commissioning Strategy Plan CSP The CSP establishes the PCT’s direction and priorities for at least the next fiveyears. PCTs develop the plan at least every three years and update it annually.The PCT is also part of a sector wide collaborative commissioning groupwhich has produced a supplementary Collaborative Commissioning <strong>In</strong>itiatives(CCI) document according to the same timetable.Communicable diseaseConceptionConfidence <strong>In</strong>tervalsIllness capable of being transmitted from person to person or from an animalto a human – i.e. infectious diseases such as measles and chicken pox.The number of pregnancies leading either to a live or stillbirth, or to atermination of pregnancy.Confidence intervals or limits are used to give a range of values within whichthere is a degree of certainty that the values are correct, and to assess ifvalues are significantly different from that of the reference population. Thisrange is required as there is likely to be some variation that occurs by chance.<strong>Wandsworth</strong> Teaching Primary Care Trust 71
Glossary<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Term Abbreviation ExplanationCoronary heart disease CHD Disease of the heart that occurs when the walls of the coronary arteriesbecome narrowed by a gradual build up of fatty material (atheroma).Examples of CHD include heart attack and angina.Crude RateA crude rate is a rate that applies to the population as a whole, and that hasnot been adjusted to account for differences in population structures such asage and sex. It is calculated using this formula:Crude Rate = Number of Events/Total Number of People in a PopulationDirect StandardisationElective admissionEthnic groupFertility RateDirectly standardised rates give an indication of the number of events thatwould occur in a standard population, if the population had the sameage-specific rates of the local area. The standard population that is mostcommonly used is the European Standard population. The rates are calculatedper 100,000 and because rates are applied to the same population, ratesacross areas can be compared.An admission from a waiting list (including booked admissions), or a plannedadmission.Defined in Census 2001 as ‘one’s perceived ethnic background or culturalidentity’.The number of children an average women would have assuming that shelives her full reproductive lifetime. The numerator is the number of live birthsin a year, the denominator is the number of females of child-bearing age,usually defined as ages 15–44.General Medical Services GMS General medical services are services provided by family doctors (GPs) andtheir staff, as provided for in Section 29 of the 1997 Act, and framed in theGeneral Medical Services Regulation 1992.Genito Urinary Medicine GUM The main work of genitourinary medicine (GUM) is the diagnosis andtreatment of sexually transmitted infections (STI), including HIV. Screeningand vaccination for sexually transmissible hepatitis viruses (A and B) andhepatitis C virus screening are also routinely offered.<strong>Health</strong> inequalitiesThe gap in health status, and in access to health services, between differentsocial classes and ethnic groups and between populations in differentgeographical areas.<strong>Health</strong> needs assessment HNA The process of exploring the relationship between health problems in acommunity and the resources available to address those problems in order toachieve a desired outcome.South West <strong>London</strong> <strong>Health</strong>Protection UnitSWL HPUResponsible for communicable disease control, infection control, chemicalincidents and environmental hazards and health protection aspects ofemergency planning.Human Immunodeficiency Virus HIV HIV prevents the immune system from working properly. Normally, thebody’s immune system would fight off infection, but HIV is able to infect keycells (called CD4 cells) which co-ordinate the immune system’s fight againstinfection. Many are actually destroyed by being infected. Others, includingCD4 cells which are not themselves infected, no longer work properly.Human Papilloma Virus HPV An infection that is strongly linked to the development of cervical cancer.The vaccine which protects against this infection will be introduced in<strong>Wandsworth</strong> from September 2008.72<strong>Wandsworth</strong> Teaching Primary Care Trust
Glossary<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Term Abbreviation ExplanationHyperglycemiaHypertensionImmunisation CoverageImmunisation Uptake<strong>In</strong>cidenceHyperglycemia is a condition that causes blood sugar level to dropdangerously low. It mostly shows up in diabetic patients who take insulin.Blood pressure greater than or equal to 140/90mmHg.The proportion of individuals in the eligible population (for example, of agiven age/sex) who have been immunised.The number of individuals who have been immunised as a proportion of allthose in the population who are eligible for immunisation.The rate at which new events occur in a population, i.e. the number of newcases of a disease in a specific period of time, divided by the total populationat risk of getting the disease during that period. It is often expressed as ratesper million population.<strong>In</strong>dex of multiple deprivation IMD An aggregate score based on a number of domains that could affect healthand well being. Last calculated 2004.<strong>In</strong>dicator<strong>In</strong>direct Standardisation<strong>In</strong>ternational Classification ofDiseases, version 10ICD10A statistic or marker that has been chosen to monitor health or service activity.For example the number of women attending for breast cancer screening orthe number of deaths from coronary heart disease in a defined population.<strong>In</strong>direct standardisation compares actual numbers of deaths to expectednumbers, adjusting for age and sex. This produces a ratio which is commonlycalled a standardised mortality ratio, or an SMR. The expected number ofdeaths is taken from the number of deaths in a larger reference population.For example, if the analysis is looking at death rates in wards, the referencepopulation could be England and Wales.The <strong>In</strong>ternational Classification of Diseases (ICD) is a diagnosis coding structureused to promote international comparability in morbidity and mortality.Joint Strategic Needs Assessment JSNA A key strategic document which aims to ensure that PCTS and LocalAuthorities look at the joint needs of the populations they represent, andtherefore ensure that common priorities can be tackled together.Life expectancyThe theoretical time an average person born today would live if he or she hadthe same rate of death at each age as people who are alive at the moment.Limiting long term illness LLTI A health problem or disability which limits your daily activities or the workyou can do. <strong>In</strong>cluding problems due to old age.Local Area Agreement LAA LAA’s set out the priorities for a local area agreed between centralgovernment and a local area (the local authority and Local StrategicPartnership) and other key partners at the local level. LAAs simplify somecentral funding, help join up public services more effectively and allow greaterflexibility for local solutions to local circumstances.Local Delivery Plan LDP All PCTs were required to produce Local Delivery Plans (LDP) for the period2003–06 setting out how they intend to achieve key targets set out in theNHS Plan, and identifying how annual funding allocations were to be used toachieve that delivery.LocalityAn area within a PCT with similar community and neighbourhood needs.Low birth-weight LBW A baby born weighing less than 2,500 grams.Measles Mumps & Rubella MMR MMR is the combined vaccine against measles, mumps and rubella. It is thesafest way to protect your children against these diseases.<strong>Wandsworth</strong> Teaching Primary Care Trust 73
Glossary<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Term Abbreviation ExplanationMethicillin-ResistantStaphylococcus AureusMorbidityMortalityNon-elective admissionsNational <strong>Health</strong> ServiceMRSANHSMRSA (sometimes referred to as the superbug) stands for methicillin-resistantStaphylococcus aureus (SA). About one in three of us carries SA on the surface ofour skin, or in our nose, without developing an infection. This is known as beingcolonised by the bacteria. However, if SA bacteria get into the body through abreak in the skin they can cause infections such as boils, abscesses, or impetigo. Ifthey get into the bloodstream they can cause more serious infections.Morbidity rates are the number of cases of an illness, injury or conditionwithin a given time, usually one year. It is also the ratio of sick persons to wellpersons in a defined population.The proportion of deaths in a defined population.Emergency admissions to hospital.National Service Framework NSF National Service Frameworks (NSFs) establish a set of minimum nationalstandards for clinical quality and access to services for the major care anddisease groups. Their aim is to improve performance and reduce localvariations in care standards.ObesityOccupationOlder peopleDescription of an individual with a Body Mass <strong>In</strong>dex of equal to or greaterthan 30kg/m².Defined in the Census 2001 as being the full title of the main job coded usingthe Standard Occupational Classification (SOC) 2000.Usually regarded as anyone aged ≥65 years.Operating Plan OP This document sets out how the PCT plans to achieve the health outcomeand financial goals for the year listed in its Commissioning Strategy Plan.It includes targets, financial and activity schedules and action plans. It isdeveloped annually. <strong>Wandsworth</strong> Teaching PCT’s Operating Plan 2007/08was submitted to NHS <strong>London</strong> in March 2007.OutbreakOutpatient AttendanceParticipatory needs assessmentWhere people are exposed to a common harmful influence, such as aninfectious agent or toxin. The exposure may be brief, or people may beexposed over a period of days, weeks or longer, with the exposure beingeither intermittent or continuous.An outpatient attendance is the occasion of a patient attending a consultantor other medical clinic or meeting with a consultant or senior member of theteam during a clinic session.Uses qualitative material, gathered locally to define need.Practice Based Commissioning PBC Under practice based commissioning, GP practices will take on responsibilityfrom their PCTs for commissioning services that meet the health needs oftheir local population.PrevalencePrimary careThe number of people with a disease at a given time, or at any time in aspecified period, divided by the number of people at risk from the disease.The frontline of the NHS is officially called primary care. The initial contact formany people when they develop a health problem is with a member of theprimary care team, usually their GP. Many other health professionals workas part of this frontline team – nurses, health visitors, dentists, opticians,pharmacists and a range of specialist therapists.74<strong>Wandsworth</strong> Teaching Primary Care Trust
Glossary<strong>Health</strong> in <strong>Wandsworth</strong> The Annual <strong>In</strong>dependent Report of the Director of Public <strong>Health</strong> 06/07Term Abbreviation ExplanationPrimary Care Trust PCT Primary Care Trusts are responsible for planning and commissioning healthservices for their local population.Public healthThe science and art of preventing disease, prolonging life and promotinghealth through the organised efforts of society. (Faculty of Public <strong>Health</strong>).Sexually transmitted infection STI Sexually transmitted infections, or STIs, are infections that can be transferredfrom one person to another through sexual contact.ScreeningSouth West <strong>London</strong>SW <strong>London</strong>SWLScreening tests sort out apparently well persons who probably have a disease fromthose who probably do not. Screening is usually concerned with chronic illnessand aims to detect disease not yet under medical care. Screening may identify riskfactors, genetic predisposition, and precursors, or early evidence of disease.<strong>Wandsworth</strong>, Croydon, Kingston, Sutton & Merton and Richmond &Twickenham are the PCTs in the South West <strong>London</strong> sector.Standardised mortality ratio SMR Death rate calculated to enable fair comparison with another area allowingfor the difference in age (or age and sex) composition of the population.Expressed as a ratio to the average value – in this case England and Waleswhose SMR is set to 100. Values greater than 100 indicate higher thanaverage mortality. Values less than 100 indicate lower than average mortality.Walk in centresWards (Electoral)NHS Walk-in Centres offer fast and convenient access to a range of NHS services,including health information, advice and treatment for a range of minor illnesses(coughs, colds, infections) and minor injuries (strains, sprains, cuts).An area within a local authority for electoral purposes. <strong>Wandsworth</strong> has 20 wards.<strong>Wandsworth</strong> PCT WPCT <strong>Wandsworth</strong> Teaching Primary Care NHS Trust.World <strong>Health</strong> Organization WHO The World <strong>Health</strong> Organization is the United Nations specialised agency forhealth. WHO’s objective, as set out in its Constitution, is the attainment byall peoples of the highest possible level of health. <strong>Health</strong> is defined in WHO’sConstitution as a state of complete physical, mental and social well-being andnot merely the absence of disease or infirmity.<strong>Wandsworth</strong> Teaching Primary Care Trust 75
Published by Department of Public <strong>Health</strong><strong>Wandsworth</strong> Teaching Primary Care Trust3rd Floor Wimbledon Bridge HouseWimbledon, <strong>London</strong> SW19 3RUTel: 020 8812 7600Fax: 020 8812 7780Email: comms@wpct.nhs.ukFirst Published June 2008Copyright © <strong>Wandsworth</strong> PCT 2008The content is the responsibility of the Deputy Director of Public <strong>Health</strong>, Velena GilfillianAll rights reserved. All or part of this report may be reproduced, copied or disseminated by individuals, organisations,or reviewers provided that credit is given to <strong>Wandsworth</strong> Teaching PCT and/or the authors.Design: www.fountainhead.ccISBN 978-0-9519343-4-0
The <strong>In</strong>dependent AnnualReport of the Director ofPublic <strong>Health</strong>The <strong>Wandsworth</strong> Annual Public <strong>Health</strong> Report:Improving <strong>Health</strong> in <strong>Wandsworth</strong> 06/07, providesan updated picture of health. It contains a seriesof fast facts available at geographical level. Thisreport is aimed at all organisations: statutory,voluntary and private, as a base for improvinghealth, providing high quality services, reducingill health and inequalities. It is also meant tobe of relevance to those who live and work in<strong>Wandsworth</strong> by highlighting current key andemerging health issues.Published by the Department of Public <strong>Health</strong><strong>Wandsworth</strong> Teaching Primary Care Trust3rd Floor, Wimbledon Bridge HouseWimbledon, <strong>London</strong> SW19 3RUTel: 020 8812 7600Fax: 020 8812 7780Email: comms@wpct.nhs.ukWeb: www.wandsworth-pct.nhs.uk/publichealth