Neonatal Presentations of CHARGE Syndrome and VATER
Neonatal Presentations of CHARGE Syndrome and VATER
Neonatal Presentations of CHARGE Syndrome and VATER
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
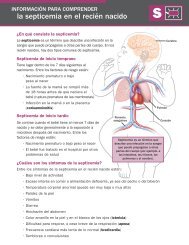
genetics<strong>CHARGE</strong> <strong>and</strong> <strong>VATER</strong>/VACTERLClinical FindingsColobomas are present in 80% to 90% <strong>of</strong> patients whohave <strong>CHARGE</strong> syndrome, <strong>and</strong> retinal colobomas aremore common than iris colobomas (Fig. 1). Retinalinvolvement can affect the optic nerve or macula, leadingto impaired visual acuity. Severe chorioretinal colobomascan be associated with microphthalmia. Newborns inwhom <strong>CHARGE</strong> syndrome is suspected should receivean ophthalmologic evaluation for retinal colobomas <strong>and</strong>be monitored by ophthalmology with an eye examinationevery 6 months.Heart defects are <strong>of</strong>ten complex <strong>and</strong> found in 75% to85% <strong>of</strong> those who have <strong>CHARGE</strong> syndrome. Althoughcardiac defects can vary substantially, conotruncal anomalies(tetralogy <strong>of</strong> Fallot, double-outlet right ventricle,truncus arteriosus, <strong>and</strong> perimembranous ventricular septaldefect) <strong>and</strong> aortic arch anomalies (interrupted aorticarch, vascular ring, <strong>and</strong> aberrant subclavian artery) comprise38% to 40% <strong>of</strong> the defects seen in <strong>CHARGE</strong> syndrome.Other common defects include atrioventricularcanal defects, atrial septal defects, ventricular septal defects,<strong>and</strong> patent ductus arteriosus.Choanal atresia is a blockage in the passages betweenthe nasal cavity <strong>and</strong> the nasopharynx. Affected individualsmay have a complete blockage (choanal atresia) or apartial blockage (choanal stenosis), <strong>and</strong> the blockage maybe unilateral or bilateral. Whereas bilateral choanal atresiacauses significant respiratory distress in the newborn,unilateral choanal atresia or choanal stenosis may not bedetected in the newborn period; the older child who haschoanal stenosis or unilateral choanal atresia may presentwith persistent rhinorrhea or infections. Choanal atresiaor stenosis is present in 50% to 60% <strong>of</strong> patients who have<strong>CHARGE</strong> syndrome <strong>and</strong> should focus the clinician’sattention on involvement <strong>of</strong> other organ systems, such asthe eye <strong>and</strong> heart. Individuals who have bilateral posteriorchoanal atresia <strong>of</strong>ten have a prenatal history <strong>of</strong> polyhydramnios,believed to be due to an insufficient swallowingmechanism. The inability to pass a nasogastrictube should alert the clinician to the possibility <strong>of</strong> choanalatresia, but computed tomography (CT) scan <strong>of</strong> thenasopharynx <strong>and</strong> nasal cavity is necessary to evaluate thequality <strong>of</strong> the blockage. Bilateral choanal atresia is amedical emergency that should be corrected surgically assoon as possible. Chronic otitis media <strong>and</strong> deafness arepotential complications <strong>of</strong> choanal atresia.Infants affected with <strong>CHARGE</strong> syndrome typicallyhave normal growth parameters at birth, but their lineargrowth tends to decline by late infancy. Some childrenhave been found to have growth hormone deficiency,but growth deceleration frequently is due to cardiac,Figure 1. Retinal coloboma.respiratory, or feeding problems. Early intervention forfeeding difficulties is important.Most children who have <strong>CHARGE</strong> syndrome showmarked delays in motor development. Such delays can bedue to prolonged hospitalizations, truncal hypotoniawith ligamentous laxity, decreased visual acuity, or vestibulardisturbances. Language development <strong>of</strong>ten is delayedas well due to hearing loss. Other individuals mayhave central nervous system abnormalities that can includearrhinencephaly; holoprosencephaly; hypoplasia <strong>of</strong>the cerebellum, inferior cerebellar vermis, <strong>and</strong> brainstem;cerebellar heterotopias; <strong>and</strong> absence <strong>of</strong> the septum pellucidum.Due to the variable nature <strong>of</strong> the developmentaldelay, the extent <strong>of</strong> the delay should not be used topredict cognitive function. Cognitive function may rangefrom learning disabilities to pr<strong>of</strong>ound mental retardation.Genital hypoplasia is present in about 50% to 60% <strong>of</strong>males who have <strong>CHARGE</strong> syndrome <strong>and</strong> can manifest asmicrophallus, hypospadias, cryptorchidism, chordee, <strong>and</strong>bifid scrotum. Female genital hypoplasia may be moredifficult to recognize externally, but hypoplastic labia <strong>and</strong>clitoris <strong>and</strong> atresia <strong>of</strong> the uterus, cervix, <strong>and</strong> vagina havebeen reported. Renal anomalies have been reported in25% to 40% <strong>of</strong> individuals <strong>and</strong> include unilateral renalagenesis, hydronephrosis, renal hypoplasia, duplex kidneys,<strong>and</strong> vesicoureteral reflux. Hypogonadotropic hypogonadismcan occur in males <strong>and</strong> females <strong>and</strong> is associatedwith delays in puberty <strong>and</strong> low concentrations <strong>of</strong>luteinizing hormone <strong>and</strong> follicle-stimulating hormone.Ear anomalies occur in approximately 90% <strong>of</strong> children<strong>and</strong> can involve the outer, middle, or inner ear. Thetypical “<strong>CHARGE</strong> ear” is protuberant, short, <strong>and</strong> wide,with a hypoplastic lobule, prominent antihelix, <strong>and</strong> tri-e300 NeoReviews Vol.9 No.7 July 2008Downloaded from http://neoreviews.aappublications.org by J Michael Coleman on August 12, 2010