Chronicle - March 08.pdf - DHCS Digital Library
Chronicle - March 08.pdf - DHCS Digital Library
Chronicle - March 08.pdf - DHCS Digital Library
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Publication ofThe Chronic Diseases NetworkWelcomeHappy New Year andwelcome to the firstedition of the <strong>Chronicle</strong>for 2008Marie HodsdonChronic Diseases NetworkCoordinator2008I am please to be the acting NetworkCoordinator for the next few monthsuntil the formal appointment of theNew CDN coordinator in <strong>March</strong>.Firstly I would like to wish a warmBon voyage and formal thank youto Rachael McGuin, former CDNcoordinator. Rachael provided anexceptional key role in bringingtogether the CDN committees,researching and writing articles in the<strong>Chronicle</strong> and establishing a workingframework for the 2008 Conference.I would like to wish Rachael the verybest in her future prospects and willpersonally miss her smiling face andeasygoing approach in all areas ofher achievements.Most of you will be familiarwith who I am having workedwith the Preventable ChronicDisease program since 2004 inan administration capacity andcoordinating the 11 th annual CDNconference in Darwin, Sept 2007.Proposed deadlinesand dates for 2008AprilContributors deadlineFriday 7 <strong>March</strong>JuneContributors deadlineFriday 9 MayAugustContributors deadlineFriday 11 JulyOctoberContributors deadlineFriday 5 SeptemberDecemberContributors deadlineFriday 7 NovemberThe <strong>Chronicle</strong> <strong>March</strong> 2008I am honoured to fulfil this roletemporarily and look forward to thechallenges the position may offer.This edition of the <strong>Chronicle</strong> featurestopics around new staff and futureplans for 2008.In forthcoming editions of the 2008<strong>Chronicle</strong> we will continue with theregular topic areas for Mens health,Women’s health and Resourcesincluding a new section aroundScreening. Each consecutive editionof the <strong>Chronicle</strong> will follow a theme(to be announced in the next edition)as they did last year.Thank you for your ongoing supportand I look forward to receiving yourstories for future editions of the<strong>Chronicle</strong>. For those wishing to jointhe CDN email list for informationon job vacancies, workshops andthe like please send an email tochronicdiseasesnetwork@nt.gov.au
The <strong>Chronicle</strong>New FacesIntroducing:Preventable Chronic Disease(PCD)DarwinBeth AmegaPublic Health Nurse (PHN)With a back ground of remote practice both in theTerritory and overseas and a recent few years in renalnursing, being a PHN on the PCD team is the ideal jobfor me. I love the remote work and I’m passionate aboutbeing proactive and working on preventative care to limitcomplications in CD patients. As part of the expandedPHN team in the Top End I’m looking forward to workingwith Wadeye, Palumpa, Peppimenarti and Warruwi healthcentres and their communities to enhance CD recalls andwork on a community and individual level in promoting selfcare strategies.L-R Beth Amega, Gaynor Garstone and Hilary BloomfieldAsthma Foundation NTWe wish to welcome Alexis Allen to the educationteam at Asthma Foundation NT. Alexis is aRegistered Nurse who has an interest in respiratoryeducation. She came to the Territory in May 2007after having worked in Sydney Children’s Hospitalin Randwick where she gained experience inworking with acute respiratory diseases includingasthma. Her knowledge in this area will beinvaluable and will add an extra dimension to oureducation sessions with health professionals.Hilary BloomfieldPublic Health NursePrior to this position I worked at Minyerri (HodgsonDowns) out of Katherine, a place very special to me, andbefore that worked on the Tiwi Islands on a renal researchproject and have previously spent time at Lajamanu.TheTerritory is my home having grown up and completed mynursing degree here. I look forward to working very hardwith the communities of Maningrida, Oenpelli, Jabiru andBelyuen and their staff and patients in a chronic diseaseand renal case management capacity. Outside work I canbe found competing in athletics, camping whenever I canor pottering in the garden.Gaynor GarstonePublic Health NurseI have worked as a RAN in both Queensland andNorthern Territory and have huge interest in Diabetes.Being apart of the extended PCD team is such a greatopportunity to work with both RN and Health workers toimprove outcomes for clients with chronic disease and beproactive in promoting self-management strategies. I lookforward to working with the health staff and communitiesof the Tiwi Islands, Borroloola and Minjilang to increasetheir knowledge and understanding the PCD program.TheAlexis Allen<strong>Chronicle</strong> <strong>March</strong> 2008
Publication ofThe Chronic Diseases NetworkSharon JohnsonPublic Health NurseMy name is Sharon Johnson, I moved to the NorthernTerritory from Victoria over 2 years ago to work inindigenous health. I worked with an NGO in Tennant Creekas a public health nurse for 2 years prior to commencingmy work with <strong>DHCS</strong>. I have a varied nursing career havingworked in research for a University, with Divisions ofGeneral Practice as a project manager, nursing educationin TAFE and quality management in rural settings. Myformal study post nursing registration has been in publichealth, health promotion, women’s health and mostrecently - diabetes education.Preventable Chronic Disease(PCD)Alice SpringsSharon JohnsonShirley Ann BaileyPublic Health NurseI lived and worked in the centre many years ago. I workedas a RN with the mobile health team, worked at Areyonga,Yuendumu and also worked in the Sexual Health Clinic(now known as Clinic 34). The last position I had beforeI moved back to Western Australia was the HIV/AIDSCoordinator for Central Australia.Since leaving in 1987, I have returned many times for shortperiods of time to spend time with very close friends and tobe in Central Australia.This visit has been a little different. I decided to dosome work and stay around for awhile. My professionalbackground is Primary Health Care, Women’s Health/Sexual Health and I have a passion for communitydevelopment.Shirley Ann BaileyFor the first 2 months I worked with Sandy McElligott(Women’s Health) providing additional Women’s Healthservices for some of the remote communities. The positionI have now is a temporary PHN position working withcommunities in the Eastern Alyawarra-Anmatjere area. I willalso provide services to the Hermannsburg community. It’sgreat to be back.continued next page ...The <strong>Chronicle</strong> <strong>March</strong> 2008
The <strong>Chronicle</strong>... continued from previos pageNutrition & Physical ActivityProgramTop EndRita ApeltAlison Lorraine, Acting Program Coordinator- Top Endwould like to Welcome three new additionsto their Top End Nutrition and PhysicalActivity team.• Linda Lay will commence as ourAdministration Officer on the 4th of Feb• Jessica Taylor will be the new Child HealthNutritionist also commencing on the 4th ofFeb• Jacqui Brown will be the new Top End WestPublic Health Nutritionist commencing onthe 18th of Feb.Rita ApeltMSOAP MidwifeHi, my name is Rita Apelt. I took over from CarolynCasserley in Nov 07 as Medical Specialist OutreachProgram (MSOP) Midwife. The lovely Carolyn has returnedto maternity at Alice Springs Hospital (ASH) and left somebig shoes to fill. I came to Alice Springs in 2002 primarilyto get remote experience in Midwifery so I could workwith Medecins Sans Frontieres (MSF). Here I am 5 yearslater. I’ve worked as a Remote Area Nurse (RAN) and alsoat ASH. The MSOP position provides the best of bothworlds. It’s a great opportunity to see most of CentralAustralia and meet many interesting and varied people.Also I feel a deep commitment to Indigenous health,especially Women’s health. The four Obstetrics andGynecology Specialists I work with all great to work with.My goals for 2008 - assist MSOP to see as many womenas possible, assist the clinics with their Pap recalls andget a more useful and meaningful database happening.I’m also studying through James Cook University (JCU) soplan to complete two subjects of Masters of Public Healthand Tropical Medicine (MPHTM). So should be a busy andproductive year.Tania CookeAdministration OfficerI started with PCD on the 3rd of January as AdministrationAssistant. Before that I was working for Dept. PrimaryIndustry, Fisheries and Mines as the Information manager.I have lived in Central Australia for almost five years now,and plan on hanging around for quite a few years yet! Ioriginally come from Mt Gambier in South-east S.A, buthave not lived there for many years now, preferring totravel Australia and the world in all its glory.I love the Territory, and enjoy living here; it really is anamazing place. My plans for this year are to save hard,see my family and friends as much as I can and stick to allmy NYE resolutions.... no I wont tell you what they are???I look forward to meeting the rest of the PCD Darwin teamin August.Linda LayThe<strong>Chronicle</strong> <strong>March</strong> 2008
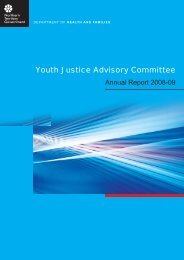
Publication ofThe Chronic Diseases NetworkI’m OK project updatePatient journeymodellingBhavini PatelNICS-HCF Foundation Fellow and Director of Pharmacy, Royal Darwin HospitalPatient journey modelling is an innovative patient-centric technique thatanalyses a patient’s movement through a given healthcare service from amulti-dimensional perspective. Two workshops were facilitated by Jo Curryfrom University Western Sydney in November last year to map the journey ofpatients living with stage 4 and 5 Chronic Kidney Disease through the current NThealth system. The sessions were run over two mornings and participants weresplit into service delivery groups for example NT renal staff, remote health staff,palliative care, preventable chronic disease programme, urban community healthstaff and surgeons. During the discussions a patient journey model graduallyevolved over time (see diagram 1). This allowed for the first time each group tohave a clear idea of steps a patient needs to take to access a particular part ofthe CKD treatment process and highlighted the complexity of the system. Thiswas particularly challenging for the public health nurses for the care coordinationprocess as this has not been done before but provided a good opportunity tocreate an ideal patient journey. Suggestions on improvements were discussedon the second day and an action plan detailing implementation of identifiedimprovements and responsibilities is currently being undertaken with each group.Meet the some of themembers of the “I’m OK”Top End care coordinationteamThe <strong>Chronicle</strong> <strong>March</strong> 2008The I’m OK project is aiming toimplement and evaluate a carecoordination model which usesquality improvement interventionsto provide sustainable solutions tothe management of chronic kidneydisease (CKD) which will result indelaying the progression of CKD and“soften” the transition to dialysis.It has been a busy first six monthsof the project, which has involveda lot of behind the scenes work.Bhavini and the team have travelledacross the Northern Territory (NT)holding consultations with the keystakeholders and establishing goodrelationships with both managersand clinicians in the NT Departmentof Community Services and in thefour urban based Aboriginal MedicalServices. A series of workshopslooking at mapping the journeya patient has to take to accessservices once they have stage 4 CKDwere held in November. NT fundingin 2007 allowed an increase in thepublic health nurses in PCD programand Australian Government fundingfor new positions in the AboriginalMedical Services to assist inimplementation of this process, hasallowed the scope of the project tobe broadened to include Aboriginalpatients living in urban areas.>>>
Patient Journey Modelling flowchartPA T IEN TMOVE ME NTST AF FRO LE SGP /Nurs e/AH W/DMOCa reC o-ordGP /DMO/S pecOR PP R OC E SSESSC R EEN ING ORMONIT ORI NG /R EVI EW *140.ST AG ING *2INF OR MAT IONC R EAT ION/UP DAT EPatient F ile*1One-off S creening -2 nd &sub cycles monitoring/review*2One-off C are C oord a s partof AuditBrief Inter ventionPA T IEN TNE E DS /PR AC T IC EGUIDEL INES /P OLIC IE SSN APEMEASU R E -ME NT SC areC oordP 2>Car eC o-ordGP /Nurse/AH W/DMOCar eCo-ordGP /DMO/S pecO/R /PCa reC o-ordGP /DMOCar eC o-ord30-60ml41.EN S UR ENOTI FI C ATI ON TOC K N UR SE & C DPR OGR AM *2CK D Nur seS pecialis t T eameG F R LE VE L?
Publication ofThe Chronic Diseases Network
The <strong>Chronicle</strong>Top End Tobacco ProjectNHMRC Project Grant 436012Project TeamIntervention Strategies:• Engage whole community• Employ local research assistants• Provide tobacco cessation training for clinic workers• Develop locally appropriate health promotionresources and strategies• Improve access to Nicotine Replacement TherapyJan Robertson Alan Clough Anil RaichurNicotine Replacement gum, lozenges and patchStudy communitiesProject Aims:To implement a multiple component, community-actionintervention to reduce tobacco smoking in remoteAboriginal communities over five years.Evaluation will include:• self-reported tobacco use measured at baselineand smoking status followed up on 2 occasions• tobacco sales monitored in each community forduration of projectVisiting HomelandsSchool mural10The<strong>Chronicle</strong> <strong>March</strong> 2008
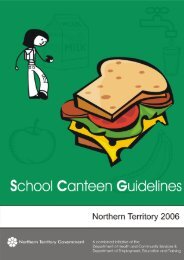
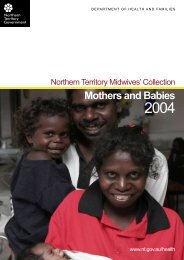
Publication ofThe Chronic Diseases NetworkQuarterly Tobacco Sales: Study Communities & Regional EnvironmentTOBACCO (tailor made cigarettes)TOBACCO (roll-your-own)Number2,500,0002,000,0001,500,0001,000,000500,0002,022,4351,648,255Grams250,000200,000150,000100,000201,960188,860050,00030 September 2007Quarter EndingRegional EnvironmentStudy Communities030 September 2007Quarter EndingRegional EnvironmentStudy CommunitiesPROJECT PROGRESSCommunity Engagement:• Visited Galiwin’ku, Ngukurr andKunbarllanjnja communities twice.• Wadeye has postponed its decision toparticipate.• Formal support received from councils.• Support of local health services, women’scentres, stores, schools and other communityagencies.• Some homelands/outstations want toparticipate.• Local endorsement of project team’s widecommunity engagement to date.• Involved local linguists to assist with projectnaming and identification of key concepts.PROJECT PROCESS (cont)Issues identified:• Need to overcome discouragement or shamedue to first relapse in smokers trying to quit.• Address community concerns regardingpassive smoking by children.• Increase awareness of harmful effects ofsmoking other than respiratory disease.• Lack of resources appropriate to eachcommunity (ie local languages, literacy level).• Chewing of tobacco (particularly by women).Data collection:• Monthly data from 6 tobacco retail outlets in 3communities. Fourth community ready toprovide relevant data.• Tobacco sales data from other stores in theregion have been obtained for comparison.• Community lists received from localgovernment & health services for selectingpeople for interview.Source:Queensland Health SmokecheckNEXT……• Provide feedback to communities and otherstakeholders of project progress.• Commence baseline interviews incommunities beginning February/<strong>March</strong> 2008.• Prepare for intervention launches in eachcommunity at staged intervals commencingJune 2008For more information contact:Jan RobertsonPhone: 07 40421635 Fax: 07 40421675Email: Jan.Robertson@jcu.edu.auJames Cook UniversitySchool of Public HealthPO Box 6811Cairns QLD 4870The <strong>Chronicle</strong> <strong>March</strong> 200811
The <strong>Chronicle</strong>Jo Watts,Palliative Care Network CoordinatorTerritory Palliative Care (TPC) service has two specialistteams, one based in Darwin, (TPC – Top End) and theother based in Alice Springs (TPC – Central), and aHospice which is located in Darwin on the RDH Campus.Although these are specialist teams they are not the onlypalliative care providers, there are a wide range of healthcare workers and organisations that provide palliative careacross the Territory.Many health staff realise that palliative care, even if notdirectly, is a part of their day-to-day work. This knowledgeand the support that is required when working withpalliative care clients/patients, their families and carershave encouraged many to join the Palliative Care Network.The Palliative Care Network is about ensuring a structureis in place to connect health professional, communitiesand organisations for the benefit of those living with a lifelimiting illness and their families/carers.The Palliative Care Network is maintained by:• A twice yearly newsletter that contains; articles/stories from those with an interest in or work inpalliative care, updates on what is happening inpalliative care in the Territory, important dates toremember as well as lists of websites, texts andresources available.• Meetings, which are held in Alice Springs,Darwin, Katherine, Nhulunbuy and TennantCreek. These meetings are held 4 times a yearin Alice Springs and Darwin and 2 times a yearin the other centres. An education session isoften incorporated into these meetings.• In conjunction with PEPA, an annual fullyfunded Network day/conference.• An electronic members list to disseminatedinformation.The Palliative Care Network aims to:• Enhance the coordination and communicationbetween services• Improve communication between serviceproviders• Reduce professional isolation• Increase knowledge through the sharing ofinformationThe next Network meeting in Darwin is onTuesday 4 <strong>March</strong> at 3pm at the auditorium at RDH,everyone is very welcome.For any information about the network, meetingdates or if you are interested in joining the PalliativeCare Network contact:Jo Wattson 8922 6915 orEmail: joanne.watts@nt.gov.au• Sharing of resources12The<strong>Chronicle</strong> <strong>March</strong> 2008
The <strong>Chronicle</strong>Program of Experience in the Palliative Approach (PEPA)PEPA is a program providing primary health providers an opportunity to develop knowledgeand skills in the palliative approach, by undertaking a supervised clinical attachment with aspecialist palliative care service and engaging in networks of support. The program is open toa wide range of health disciplines.PEPA will offer you:• an opportunity to pursue your own learning objectives• a clinical workplace attachment with a palliative care specialist•post-placement support to assist implementing learning experiencesClinical placements commenced in 2004 and will continue until 2010. Workplace placements of up to 2weeks (4 days for Doctors) are offered at a time to suit you, at Territory Palliative Care with thespecialist teams in Darwin or Alice Springs or a combination of both.To be eligible to participate in PEPA you must be currently employed in a health care service, whichcares for people with palliative care or end of life care needs. You must have a currentqualification/registration in the associated discipline and must have the approval of your currentemployer to participate.Those working with chronic disease clients are likely to benefit greatly from anenhanced understanding of the palliative approach.For 2007 – 2010 those working in remote and rural settings,including Aboriginal Health Workers, are encouraged to apply.Full costs of travel, accommodation are included in for eligible applicants.Employers are compensated for costs associated with back fill or overtime for staffparticipating in PEPA.For more information visit www.pepaeducation.comNT Information kit and Application Forms at: www.nt.gov.au/health/comm_health/palliative/pepa.shtmlTerritory Hospice, Royal DarwinHospital campus. Opened 2005or contactPEPA Project ManagerJohn CarsonTerritory Palliative CarePh: 08 892 27679 Fax: 08 89226775john.carson@nt.gov.auThis program is an initiative of and funded by the Australian Government, Department of Health andAgeing, under the National Palliative Care Program14The<strong>Chronicle</strong> <strong>March</strong> 2008
Publication ofThe Chronic Diseases NetworkMaximisinginfluenza vaccinationBeth Amega,Public Health Nurse,<strong>DHCS</strong>, Preventable Chronic DiseasesOver 2,500 Australians die each year from complicationscaused by influenza. Less than half the people most at riskof developing life threatening complications from influenzaare being vaccinated annually.The Audit & Best Practice For Chronic Disease (ABCD)audit in diabetics in NT remote communities showed fluimmunisation rates averaged around 58% with someareas as low as 37% in 2007. (ABCD, 2008 unpublished).Focused effort can increase the vaccine coverage.The 2008 influenza vaccine will be available in midFebruary so start planning strategies to maximise influenzavaccine coverage in your community now.Those who should be vaccinated include:• Indigenous people over 50 years,• Non-Indigenous people >65 years• Health care workers• Indigenous people aged 15-49 years old with chronicdisease such as:»»»»»»»»Chronic lung diseaseChronic liver diseaseChronic heart diseaseChronic renal failure (stages 3-5)DiabetesWeakened immune systemsHIVSevere Asthma(CARPA standard treatment manual 4 th ed. p.294)Health care workers(nurses, Aboriginal health workersand doctors) are at an increased risk of both getting andspreading influenza so should be vaccinated to protectthemselves and their patients.Some ideas to increase vaccination in yourcommunity are:• Generate a list of people in your communitywho should be vaccinated by age and bydisease - this is your target population• Ensure computerised records have targetpatients on an annual fluvax recall• Health promotion activities such as posters,word of mouth, community radio• Organise flu vaccination days• Organise immunisation booths on specificdays out side the clinicThe Preventable Chronic Disease team (PCD) can providein-services on flu vaccination and assist with strategies topromote flu vaccination in your community.Contact:Beth Amega: beth.amega@nt.gov.au orPhone: 8922 6913Centre for Disease Control (CDC) can provide informationabout immunisation and the flu vaccine.Contact:Rosalind Webby: Rosalind.webby@nt.gov.auPhone: 08 892 28825Fax: 08 892 28310All flu vaccines should be recorded on either the adultvaccination record forms or population lists with details ofthe vaccine, date given, name and date of birth and faxedto the Centre for Disease Control.Resources can be sourced from PCD/CDC or found at thefollowing websiteswww.flushots.com.auwww.fightflu.gov.auhttp://www.nt.gov.au/health/cdc/immunisationhttp://www.immunise.health.gov.au/The <strong>Chronicle</strong> <strong>March</strong> 200815
The <strong>Chronicle</strong>Healthy Living NTGerard WongNutrition EducatorHealthy Living NTHealthy Living NT (HLNT) provides group andindividual diabetes education and cardiacrehabilitation services to clients and healthprofessionals in Darwin and Alice Springs. Manyhealth professionals are unaware our diabetes nurseeducators, dietitians and cardiac nurse educatorsare available to provide information and support byphone, email or in groups as part of an in-service.In 2008 we are starting a regular four-week groupeducation program for people with Type 2 diabetesfacilitated by a multidisciplinary team consistingof an exercise physiologist, dietitian and diabeteseducator. The group ‘Taking Charge of Diabetes’focus is to increase physical activity levels andknowledge about food and nutrition and selfmanagement.The group is a new Medicare initiativeavailable as part of the Enhanced Primary CareProgram (EPC).>>>16The<strong>Chronicle</strong> <strong>March</strong> 2008
Publication ofThe Chronic Diseases Network
The <strong>Chronicle</strong>Work Opportunities>>>with a new Chronic Diseases services improvement projectCentral Australian Division ofPrimary Health Care”Are you interested in serviceintegration and coordinated care forpeople with chronic diseases?Do you have experience in healthsystems reform and improvement?Part-time project work will soon beavailable on an exciting new ChronicDiseases activityAs many of you will be well aware, the delivery ofcoordinated care to urban residents can be challenging.This is said to be due to a number of factors includingthe diversity of Primary Health Care (PHC) providers,(eg General Practitioners, Community Controlled HealthOrganisations, Hospital Emergency Departments, privateAllied Health Professionals, NT Government CommunityHealth Centres and Non-Government Organisations), theextreme shortages of Allied Health Professionals and alack of Practice Nurses in General Practice with clear rolesin early intervention and care processes.To tackle these challenges, a new project is to commencethis year through funding from the Australian Governmentunder the Australian Better Health Initiative (ABHI) andthe NT Department of Health and Community Services(<strong>DHCS</strong>). The funding is for three years. Aims of the NTproject are to:1.2.3.Facilitate the delivery of integrated and coordinated care topeople with Type 2 Diabetes and heart disease living in theDarwin/Palmerston and Alice Springs regions;Increase the ability to work in effective partnerships toreform and integrate urban PHC services according tobest practice, in order to better meet client needs; andDevelop or promote health promotion activities andresources for use by Practices and/or PHC providers.18The<strong>Chronicle</strong> <strong>March</strong> 2008
Publication ofThe Chronic Diseases Networkwork opportunities
The <strong>Chronicle</strong>Some of what wehave planned forPhysical Activity2008 …Community Engagement andParticipationIn 2008 the Heart Foundation will be a key player in thePhysical Activity arena. Heart Foundation objectives willbe integrated into the GoNT strategy and the staff willbe increasing networking opportunities and support forthose working across the physical activity field particularlyin indigenous communities. Mid year forums will beconducted bringing together interested parties to facilitatea shared events calendar and documentation of andsolutions to barriers to participation.20TheRegister your interest by calling 89811966Active By DesignActive By Design is an area that the Heart Foundationwill continue to be involved in at both the Territory andNational level. After the interest developed by the HealthyBy Design seminar in Palmerston in November, the HeartFoundation is determining whether there is interest tohost something similar in Central Australia. In addition itis hoped to involve the Northern Territory in consultativeworkshops relating to the Healthy Spaces, Healthy Placesproject that is a joint initiative between the National HeartFoundation, the Planning Institute of Australia and theAustralia Local Government Association. We also lookforward to disseminating the outcomes from the propertydevelopment sector-scoping project that is currently underway. All in all it’s a busy and growing area of work. Forfurther information please contact Joanne Blayney orLisa Fox.Heart Foundation WalkingHeart Foundation Walking is Australia’s largest networkof free community based walking groups led byvolunteer walk organisers. The Heart Foundation worksHeart Foundation walking – kicking off to a good startin partnership with Area coordinators to set up groups inthe local community. Area Coordinators may come fromhealth or community centres, councils or workplaces andwork with the Heart Foundation to assist volunteer walkorganisers to recruit walkers and establish groups.Community based volunteer Walk Organisers leadthese groups in their local area. They are provided withresources, training and support to begin and maintain theirgroup. Walkers will all be connected to a national database offering regular newsletters, a walker’s recognitionscheme, access to all Heart Foundation resourcesincluding the website, telephone information serviceand hard copy resources assisting participants to makehealthier lifestyle choices.In 2008 in the Northern Territory, Heart FoundationWalking will be piloted in remote communities. Interesthas already been registered and we hope to have aminimum of one community in the Top End and one fromCentral Australia. Contact the Darwin office on 89822703to register your interest, join a walking group or for furtherinformation.>>><strong>Chronicle</strong> <strong>March</strong> 2008
Publication ofThe Chronic Diseases NetworkAusPAnetIn an Australian first there is now a community networkproviding access to timely, accurate information about“Physical Activity”, from developments in the area toevents and conferences. The network is called AusPAnetand is for anyone in Australia who sees physical activity aspart of their role, or interest, and who would like to accessaccurate and timely information.The network is a joint initiative of the National HeartFoundation of Australia and the centre for Physical Activityand Health, University of Sydney.To become a member, register your details athttp://auspanet.heartfoundation.org.auOnce you register you will receive a fortnightly e News witheasy ‘click-through options that link you to the website andother relevant information sources. There is also the optionto post information and articles on the site.In 2008 we hope to attract new members from the Territoryalong with local articles.Local Government AwardsEach year the Heart Foundation facilitates a recognition program acknowledging and rewarding Local Government andtheir partners conducting heart health initiatives. The awards provide an opportunity for communities to celebrate theirachievements and seek recognition for their valued contribution to creating healthy communities; they include cash, plaquesand certificates across four categories at national and state levels.In 2007 the Kunbarllanjnja community store was awarded a national category win along with cash prizes and plaques. In2008 we would like to see more entries from Northern Territory councils and their partners. Entry will be posted to all councilsby April and will be available on the Heart Foundation website www.heartfoundation.org.au Contact the Darwin Office forfurther information on 89811966.The 2008 four award categories are:• Implementation of Plans and Policies to Support Heart HealthThe Heart Foundation recognises Local Governments’ development and effective implementation of plans andpolicies that support people to be heart healthy.• Provision and Use of Facilities to Improve Heart HealthThe Heart Foundation recognises Local Governments that develop and implement programs to encourage the use oftheir facilities to improve heart health.• Programs that Improve Heart Health in Priority GroupsThe Heart Foundation recognises Local Governments that develop and implement programs in collaboration with thecommunity to improve the heart health of priority groups.Key priority groups for heart disease include: Aboriginal and Torres Strait Islander peoples, people from low socioeconomicareas and culturally and linguistically diverse backgrounds, groups from rural areas, socially isolatedindividuals, the older population, overweight individuals and people with risk factors for heart disease. If you believeyour program addresses the needs of a priority group not listed here please contact your state coordinator.• Programs that Promote Healthy WeightThe Heart Foundation recognises Local Governments that are running programs to address the increasing levels ofoverweight and obesity in our communities.>>>The <strong>Chronicle</strong> <strong>March</strong> 200821
The <strong>Chronicle</strong>World Record AttemptJump Rope for Heart is 25 years old in 2008!We will be celebrating with an attempt to break the Guinness World Record for the most number of people skipping atone time all around the country. We look forward to more schools than ever joining in with the fun and activity.22TheMilingimbi Community Education Centre “Jumping Off” in 2007<strong>Chronicle</strong> <strong>March</strong> 2008
Publication ofThe Chronic Diseases Network
The <strong>Chronicle</strong>Obesity in AdultsTammy Devine,<strong>DHCS</strong>, Nutrition & Physical ActivityThe latest stats are out!The Australian Bureau of Statistics has just releasedOverweight and Obesity in Adults, Australia, 2004-05,which shows that 54% of Australian adults are overweightor obese and the numbers are increasing. In this report,overweight and obesity are classified as those adultshaving a Body Mass Index (BMI) of 25 or above. The cutoff points for classification are outlined in Table 1.To calculate BMI, use the following formula:For example, if my weight is 85kg and my height is 1.7m,my BMI is 29. I am in the overweight category.Table 1*. Body Mass Index CutpointsUnderweight Less than 18.5Normal range 18.5 to less than 25.0Overweight 25.0 to less than 30.0Obese30.0 and greater* BMI cut off points in Table 1 are only for adults. BMIcalculations for children or adolescents must becompared with age and gender percentile charts.Sedentary behavior (low levels of activity) is one of the riskfactors associated with being overweight or obese.Full copies of Overweight and Obesity in Adults,Australia, 2004-05 are available athttp://www.abs.gov.au/ausstats/abs@.nsf/mf/4719.0?OpenDocument.ReferencesWeight (kg)Height (m) 2http://www.canadian-health-network.cahttp://www.beactive.com.au/workplace.htmlhttp://www.beactive.com.au/tips.htmTake the opportunity now to make ‘increasingyour physical activity levels’ a New Year’sresolution. Some helpful tips to keep youmoving and motivated:• Choose activities that are fun.• Try a unique activity (wall climbing, poledancing, laser tag, or drum dancing,for example) – you could even findsomething unique to do at home likeusing soup cans as weights, dancingto music on the radio or using an activevideo dance game.• Exercise with other people – exercisecan be fun and socially rewarding.• Keep a diary of your physical activity– this can be a great motivating tool.• Set specific, realistic goals – if you needto, seek advice from your GP.• Join a team or club – you’ll get to workout and meet new people.• Find activities that fit into your dailyroutine – if you’re in an office, take thestairs, walk to a co-worker’s office togive him or her a message or take anactive break (go walking, stretch at yourdesk) instead of a coffee break.If you need some more tips and ideas, visithttp://www.beactive.com.au/tips.htm24The<strong>Chronicle</strong> <strong>March</strong> 2008
Publication ofThe Chronic Diseases NetworkGood Tucker - Good HealthThe <strong>Chronicle</strong> <strong>March</strong> 2008Alison Lorraine,<strong>DHCS</strong>, Nutrition andPhysical ActivityThis conference will be the firstNational Nutrition NetworksConference since the last one heldin Cairns in 1999. Throughout the1990’s Nutrition Networks was avalued forum for Aboriginal andTorres Strait Islander people (andothers) working in a wide range ofnutrition programs and activitiesto share good practice and learnfrom each other. National NutritionNetworks 08 (NNN08) will be agathering of people working in manydifferent settings and approachesto improve the nutrition, health andwellbeing of Aboriginal and TorresStrait Islander people. NNN08 aimsto provide an environment thatenables Aboriginal and Torres StraitIslander people to share thoughts,knowledge and experiences infood and nutrition, and be inspiredby the good practice shared andnetworks formed. It will also bea great opportunity to advocatefor nutrition and the NationalAboriginal and Torres Strait IslanderNutrition Strategy and Action Plan(NATSINSAP) to be at the forefrontof the Aboriginal and Torres StraitIslander health agenda, as well asto consider future directions for theNATSINSAP.NNN08 will have opportunitiesfor all, from keynote speakers topapers, workshops, sharing storiesvia ‘yarning sessions’, posters anddisplays. We will have the opportunityto hear from some prominentAboriginal and Torres Strait Islanderspeakers, as well as many of youfrom rural, remote and urban areaswho are doing exciting work that ismaking a difference, so check theconference website regularly forupdates on keynote speakers andthe conference program.11-14 <strong>March</strong> 2008The conference themes also covera broad range of nutrition issues forAboriginal and Torres Strait Islanderpeople, including the supply ofhealthy foods to remote and ruralcommunities, nutrition issues inurban areas, Aboriginal and TorresStrait Islander nutrition workforce,family focused nutrition programsto improve nutrition and growth formothers and babies, and programsthat promote good nutrition andhealthy weight at other life stages forAboriginal and Torres Strait Islanderpeople. ‘Good practice’ programsthat help build healthier individualsand communities will also behighlighted.Most importantly, the conferencewill be an opportunity to meetold friends, make new ones, andbe inspired with new ideas andenergy to continue improving policy,knowledge, skills, and supportiveenvironments that will enablehealthy food choices to be easy andaffordable choices for Aboriginal andTorres Strait Islander people.For further information:The National Nutrition NetworksConferencePO Box 280DEAKIN WEST ACT 2600P: 02 6285 4660F: 02 6285 4670E: conference@ruralhealth.org.auor register@ruralhealth.org.auWebsite www.ruralhealth.org.au25
The <strong>Chronicle</strong>Healthy For Life hitsOenpelliHealthy for LifeBanner outside theYouth & RecreationCentre - painted bythe Oenpelli PrimarySchool childrenJonathan Jauncey<strong>DHCS</strong>, Preventable Chronic DiseaseOenpelli community came together with Kakadu Health Services and NTDepartment of Health and Community Services on Thursday 1 st November toLaunch the Healthy for Life program. With the key focus of the Oenpelli programaiming to educate the community on the importance of good overall health(Healthy inside, Healthy outside, Healthy upstairs, Healthy Environment)The Launch for the program took place on Thursday 1st November 2007andhad great participation from both the community and all the key stakeholders.A Family BBQ was held at the youth centre with activities for all the family:• Healthy for life poster competition forSchool children• Sporting activities: basketball andfootball• Line dancing exhibition from theGroovy Grans• Concert by community band26The• Healthy Food BBQ (meat providedby Oenpelli Abattoir)• Health display and expo withinformation on Health Promotion,Male Health, Chronic disease, MentalHealth• Children’s face paintingDinner prepared by theMale Health Team at theYouth & Recreation Centrecontinued next page ...<strong>Chronicle</strong> <strong>March</strong> 2008
Publication ofThe Chronic Diseases Network... continued from previos pageJonathan Jaunceywith resourcesoutside Oenpelli storeMale Health Team– Chadwick Koimala,Leon James, MarkHansen, RichardGarling, Jason Bonson,Christopher Galaminda& Jonathan JaunceyOenpelli clinic staff Heather Keighley,Dr Heggie and Joan Tuppack,supported by Darwin based <strong>DHCS</strong>staff Hillary Bloomfield, JasonBonson and Jonathan Jauncey dida marvellous job in planning andfacilitating the launch. The resultswere evident with a packed houseand lots of smiles on the eveningThe week also set the stage for aHealthy for Life Male health week.The combined Male health teamof Oenpelli Clinic staff (Dr Heggie,Chadwick Koimala, ChristopherGalaminda, Grant Nayinggul, MarkHanson) Jabiru based AOD Staff(Leon James) Darwin based PCDstaff (Jason Bonson, JonathanJauncey) Mental Health Staff(Richard Garling) and Department ofJustice (Charlie King) set out to talkthe men of the area in several keyareas:• Educating Oenpelli men aboutAboriginal Male health statistics andthe importance of good overall health• Empowering Oenpelli men to takecontrol of the method in which malehealth services are delivered with inthe region• Strengthening relationship betweenthe community and Health Services• Promoting the strong need for moreCommunity based AHWOver the period of the week thecombined male health teamfacilitated:• Men’s Health and Health Promotioneducation sessions at Local Council,Demed, Injalak Arts centre and theAbattoir.• Men’s health promotion displaysheld at the Store and single men’squarters.• Domestic violence talk presented byCharlie King• Mental Health talk by Richard GarlingThe results of the team’s hard workand good planning were evidentwith 116 men attending over theweek. Through the consultationprocess and feedback provided bythe men it was clear that the weekwas a great success with the menof Oenpelli confirming they wouldlike to start a male health programwithin the community in 2008. Theprogram will start in February 2008and will run recurrent fortnightly malehealth days with sessions covering:Health Education, Sport, Screening,Nutrition, Male Health Camps andCultural Activities.Special Thanks to Traditionalowners, community stakeholders,Oenpelli Clinic staff, <strong>DHCS</strong> staff,Kakadu health staff, specialguests Charlie King, Dotty Daby,and above all, special thanks tothe people of Oenpelli for gettingbehind the Health for Life programand making the week a greatsuccess.The <strong>Chronicle</strong> <strong>March</strong> 200827
The <strong>Chronicle</strong>Screening CornerWhat is a Screening Program?Dr Madhumati Chatterji,HD&OH, Public Health Physician, Screening AdviserScreening is a public health service in which members of a defined population, who do not necessarily perceive theyare at risk of a disease or its complications, are asked a question or offered a test to identify those individuals who aremore likely to be helped than harmed by further tests or treatment to reduce the risk of disease or its complications(Gray, 2001 Evidence-based Healthcare).The aim of screening is to detect disease before the usual time of diagnosis. Three fundamental principles govern thedecision to screen:1.2.3.The disease/health condition should be serious, well understood (natural history of the disease known), and thereshould be an effective treatment or intervention that will improve the outcome for the individual.There should be an appropriate (valid & accurate) and acceptable (simple, affordable) screening test to detectthe disease/health condition in time for effective treatment or intervention, with prior appropriate diagnostic andconfirmatory tests.Health gains in terms of cost-effectiveness, yield (numbers needed to screen to detect one likely case), socio-culturaland ethical appropriateness, quality care and client satisfaction.What is a ScreeningProgram?Decision to launch a screeningprogram is made based on acomprehensive appraisal of allavailable evidence, global, nationaland local. The term ‘screeningprogram’ implies that health servicesundertake to deliver services inscreening for the disease/healthcondition, follow up and treatment.The screening services are offeredto populations, where an individualis invited to participate in thescreening program, applied thescreening test, and if found to be‘screen positive’ is followed upthrough confirmatory diagnosisand treatment. This is contrary to‘opportunistic’ screening where testsare delivered opportunistically whenthe client accesses health care foranother reason (such as screening28Thefor high blood pressure, blood sugar,pre-employment health checks, etc).Any ongoing population based healthscreening initiative or ‘program’needs to be ‘organised’.What are therequirements to set upan organised screeningprogram?To undertake the specific activitiesand deliver quality services, ascreening program requires thefollowing structures and processesin place:1. A clearly defined screening policyon:• Population to be screened– region, gender, age-group,risk/exposure• Screening test delivery• Screening interval• Call, recall to be screened• Screening pathway – screening,diagnosis, treatment, follow up,rescreening• Targets, Guidelines, Standardsand Monitoring Indicators• Appropriate and timely follow upand treatment• Rescreening (individuals returningto screening after treatment)• Informed consent/choice2. Register on the enrolled screeningpopulation – recruitment andfollow up3. Ongoing Monitoring andEvaluation system4. A quality improvement system5. Dedicated funding and staffcontinued next page ...<strong>Chronicle</strong> <strong>March</strong> 2008
Publication ofThe Chronic Diseases Network... continued from previos pageScreening programs can be targetedat the general population (massscreening), or targeted at sectionsof the population (targeted orselective screening). Sometimesmultiple diseases/health conditionsare screened for through multiplescreening tests (multiphasicscreening), commonly seen inemployment scenarios or HealthMaintenance Organisations.What are the ethicalaspects of an organisedscreening program?For the symptomatic distressedpatient seeking help, the cliniciandoes what s/he can; for the healthyperson invited to participate in thescreening program, only the bestpossible service will suffice. As thehealth service initiates and invitesthe asymptomatic individual to thescreening program, there is an ethicalobligation on the health service thatscreening services delivered arebeneficial to the individual. That is,the screening picks up the disease/health condition truly (and the testis ‘true positive’ not ‘false positive’),and when the test results arenegative, the individual is truly freefrom the disease/health condition(and the test is ‘true negative’ not‘false negative’).Access to appropriate and completeinformation on the benefits andharms of the screening program/test is a fundamental right of theindividual who is invited to screen.Based on the information, theindividual makes the ‘informedchoice’ to accept the screening testand be enrolled in the screeningprogram.What are the potentialharms from a screeningprogram?Balancing the benefits and harms isan eternal challenge for a screeningprogram. Given that apparentlyhealthy and asymptomatic peopleare ‘invited’ to the program, it isobligatory on the part of the healthservice that harm to the individuals isminimised and benefits maximised.Potential harms or negative effects ofa screening program can be physical,psychological or financial, rangingfrom complications and pain from thescreening test, through to anxiety inthe wait for the result, anxiety in thewait for the diagnostic result if thescreening test result is positive, costs,and the trauma of ‘wrong’ test results(false positive or false negative)ConclusionScreening programs save lives,improve quality of life, reduce theburden of disease in the populationand minimise costs of treatment(through early diagnosis). Whendelivered, managed and monitoredappropriately, screening programslead to significant population andindividual health gains. However, thechallenges and complexities of ascreening program are not small.For further information, contactDr Madhumati Chatterji,Medical Advisor Screening HealthDevelopment & Oral Health, Dept. ofHealth & Community Services;madhumati.chatterji@nt.gov.auNext in the series: Complexities of ascreening test – 1The following interesting‘aphorisms’ by Muir-Gray(Evidence-based Healthcare,2001) provide ‘food forthought’:• A stitch in time does notalways save nine (withinherent issues with thedisease progress, thescreening test, timelinessof follow up, etc)• All screening programmesdo harm; some can dogood as well• The harm from a screeningprogramme startsimmediately; the goodtakes longer to appear• Screening programmesshould be run withfirm management. Ifquality falls, a screeningprogramme that wasdoing more good thanharm may then do moreharm than good• A screening programwithout false positives willmiss too many cases tobe effective• A screening programwithout false negatives willcause unnecessary harmto many healthy people• Though insignificant tothe population, a singlefalse positive can be ofdevastating significance tothe individual• If a quality assuranceprogramme is notgenerating at least onemajor public enquiry every3 years, it is ineffective• At best, screening is azero-gratitude business.The <strong>Chronicle</strong> <strong>March</strong> 200829
The <strong>Chronicle</strong>R E S O U R C E SRecent Research reports>>>ON LINE ARTICLES1. Assessing ‘fun foods’: nutritional contentand analysis of supermarket foods targeted atchildrenThis article provides a nutritional profile of foods targetedspecifically at children in the Canadian supermarket.Excluding confectionery, soft drinks and bakery items, 367products were assessed for their nutritional composition.The article examines the relationship between ‘funfood’ images/messages, product claims and actualproduct nutrition. Among other findings, it concludesthat approximately 89% of the products analysed couldbe classified as of poor nutritional quality owing to highlevels of sugar, fat and/or sodium. Policy considerationsneed to be made in light of the fact that ‘fun food’ is aunique category that poses special challenges; as such,recommendations regarding food labelling and packagingare presented.http://www.blackwell-synergy.com/doi/abs/10.1111/j.1467-789X.2007.00418.x2. Effects of Tai Chi on glucosehomeostasis and insulin sensitivity in older adultswith type 2 diabetes: a randomised double-blindsham-exercise-controlled trialBackground:Large proportion of adults with type 2 diabetes remainsedentary despite evidence of benefits from exercise fortype 2 diabetes. Simplified Yang Tai Chi has been shownin one study to have no effect on insulin sensitivity inolder adults. However, a modified Tai Chi form, Tai Chi forDiabetes (TCD) has recently been composed, claiming toimprove diabetes control.Methods:Subjects were randomised to Tai Chi or sham exercise,twice a week for 16 weeks. Primary outcomes were insulinresistance 72 h post-exercise (HOMA2-IR), and long-termglucose control (HbA1c).Results:Thirty-eight subjects (65 ± 7.8 years, 79% women) wereenrolled. Baseline BMI was 32.2 ± 6.3 kg/m2, 84% hadosteoarthritis, 76% hypertension, and 34% cardiacdisease. There was one dropout, no adverse events, andmedian compliance was 100 (0 – 100)%. There were noeffects of time or group assignment on insulin resistance orHbA1c ( –0.07 ± 0.4% Tai Chi versus 0.12 ± 0.3% Sham; P= 0.13) at 16 weeks. Improvement in HbA1c was related todecreased body fat (r = 0.484, P = 0.004) and improvement30Thein insulin resistance was related to decreased body fat (r =0.37, P = 0.03) and central adiposity (r = 0.38, P = 0.02), aswell as increased fat-free mass (r = –0.46, P = 0.005).Conclusions:TCD did not improve glucose homeostasis or insulinsensitivity measured 72 h after the last bout of exercise.More intense forms of Tai Chi may be required to producethe body composition changes associated with metabolicbenefits in type 2 diabetes.http://ageing.oxfordjournals.org/cgi/content/abstract/afm127v13. Challenges in health and health care forAustralia (Abstract)The next Australian Government will confront majorchallenges in the funding and delivery of health care.These challenges derive from:• Changes in demography and disease patterns as thepopulation ages, and the burden of chronic illnessgrows;• Increasing costs of medical advances and the needto ensure that there are comprehensive, efficientand transparent processes for assessing healthtechnologies;• Problems with health workforce supply and distribution;• Persistent concerns about the quality and safety ofhealth services;• Uncertainty about how best to balance public andprivate sectors in the provision and funding of healthservices;• Recognition that we must invest more in the health ofour children;• The role of urban planning in creating healthy andsustainable communities; and• Understanding that achieving equity in health, especiallyfor Indigenous Australians, requires more than justproviding health care services.The search for effective and lasting solutions will requirea consultative approach to deciding the nation’s priorityhealth problems and to designing the health system thatwill best address them; issues of bureaucratic and fiscalresponsibility can then follow.http://www.mja.com.au/public/issues/187_09_051107/arm11047_fm.html<strong>Chronicle</strong> <strong>March</strong> 2008
R E S O U R C E SPublication ofThe Chronic Diseases NetworkHealth promotionActivitiesNational Youth Tobacco Free Day:National Youth Tobacco Free Day is on Wednesday 19<strong>March</strong>, 2008. The theme for 2008 is‘Smoking in Movies’There will be a national competition with stacks of greatprizes and lots of ideas about how you can get involvedwith the day. To receive a free information pack includingposters please email bianca.crosling@cancervic.org.auKeep checking the OxyGen website (www.oxygen.org.au)for more information about National Youth Tobacco FreeDay 2008!Conferences, Trainingand Courses for 2008Clinical Learning calendarnow availableClinical Learning is focused on providing continuingeducation for Nurses, Midwives and where possible toother health professionals across the diverse practicesettings in the Northern Territory.The main focus for 2008 is to provide continuingeducation that holds national endorsement, orprofessional accreditation.General enquiries about scheduled courses within thecalendar should be directed to:Darwin(For enquires relating to courses in Darwin, Katherine andNhulunbuy)Phone: (08) 892 28747Facsimile: (08) 892 28010Alice Springs(For enquiries relating to courses in Alice Springs andTennant Creek)Phone: (08) 895 17724Facsimile: (08) 895 17733Practical PaediatricsDarwin, June 2-6This five-day course will develop the knowledge andskills required to prevent, identify and treat illnesses andpromote the physical, social and emotional well being ofchildrenSuitable for Registered Nurses and Aboriginal HealthWorkers practising in a remote settingFor more information contact:Brad Palmer:brad.palmer@nt.gov.au orPhone 89227816Aboriginal HealthResearch HealthConference 2008Strong Foundations …Strong FutureSydney, 29-30 April 2008DOCKSIDE Cockle Bay WharfSpeakers:Ms Sandra BaileyCEO, Aboriginal Health and Medical Research Council ofNSWProfessor Sandra EadesDirector Aboriginal Programs, The Sax InstituteProfessor Bruce ArmstrongProfessor of Public Health and Medical Foundation Fellow,Sydney Cancer CentreProfessor Kerin O’Dea AOProfessorial Fellow, University of Melbourne and Baker HeartResearch InstituteProfessor Fiona Stanley ACDirector, Telethon Institute for Child Health ResearchFor further information http://www.saxinstitute.org.au/newsevents/EventItem.cfm?objid=754The <strong>Chronicle</strong> <strong>March</strong> 200831
The <strong>Chronicle</strong>R E S O U R C E SRural and RemoteAboriginal and TorresStrait Islander ChronicDisease ConferenceBetter by a Country Mile:Solutions to AboriginalChronic Disease in Rural andRemote AustraliaGreater Western Area Health Service, Maari MaHealth Aboriginal Corporation, University of SydneyDepartment of Remote Health, Broken Hill, RoyalFlying Doctor Service, NSW Health will host a Ruraland Remote Aboriginal and Torres Strait IslanderChronic Disease Conference in partnership withAboriginal Community Controlled Health Services.When: Thursday 15 and Friday 16 May 2008provide an opportunity for health professionals toshowcase success and share best practice.Where: Broken Hill Entertainment CentreWe are seeking keynote speakers, plenaryspeakers and abstracts, which describesuccessful and innovative approaches tochronic disease among Aboriginal peopleliving in rural and remote areasFor further information about the conference contactLynne Lambell, Conference Coordinator on (02)63638027 or email lynne.lambell@gwahs.health.nsw.gov.au .For registration or attendance inquiries contact theevent manager, Bradley Hayden at CountrywideConference & Event Management on (02) 6023 6300 orbradley@ccem.com.auWhat: The Conference will focus on the successesin managing the challenges of Chronic Disease forAboriginal people in remote and rural settings, andThe National Nutrition Networks ConferenceAlice Springs Convention Centre,11-14 <strong>March</strong> 2008REGISTRATION NOW OPEN PROGRAM AVAILABLEInformation available on the website throughwww.ruralhealth.org.auhttp://www.ruralhealth.org.au/conferences/nnnc2008/home.html32The<strong>Chronicle</strong> <strong>March</strong> 2008
Publication ofThe Chronic Diseases NetworkThe four D’sDelayfor at least five minutes, the urge will passDeep breathebreathe slowly and deeplyDo something elsekeep your hands busyDrink Watertake time out to sip it slowlyCounsellors are available to supportsmokers to Quit.Benefits of Quitting ...• Reduced risk of heart attack and stroke• Quicker healing after an operation• Better anaesthetic outcome• Cleaner lungs - reduce risk of cancer4 ways to avoid a cigaretteCall the Quitline137 848To refer patients/clients to the NT Quitline for help to Quit a simple referralform is available. To obtain a pad of referral forms call theNT Tobacco Hotline on 1800 588 564.Department of Health and Community Services nt.gov.au/healthThe <strong>Chronicle</strong> <strong>March</strong> 200833
Health at the Heart ofAustralia ConferenceAlice Springs, 13 - 15th August 2008The <strong>Chronicle</strong>12th Annual Conference of the Chronic Diseases Network of the NT18th Annual Scientific Meeting and Exhibition of theAustralian Cardiovascular Health and Rehabilitation AssociationThe 12th Annual Chronic Diseases Network Conference promises to promises to be one of the mostexciting and memorable of the CDN conferences! This is the first time the conference will be heldin Alice Springs, which will provide a great opportunity for participants from Central Australia to jointhe conference, as well as some fantastic social events, including dinner at the Desert Park, tours toremote clinics and a Welcome Reception with the Western Desert Renal Choir. The 2008 conferencewill also be a joint event with the Australian Cardiovascular Health and Rehabilitation Association,(ACRA), a national association representing multidisciplinary health professionals who are involved inprimary and secondary prevention of cardiac disease.The theme of the conference: ‘Health at the Heart of Australia’ focuses on cardiovascular healthwithin the context of chronic disease. Cardiovascular disease is the leading cause of death inAustralia, and is one of the most prevalent, costly, and preventable of all chronic diseases. Challengesfor Indigenous health and remote health service delivery will also be core-underlying themes of theconference, with a range of other areas covered within the program.Keynote speakers and topics that will be on the Program include:Professor Garry JenningsDirector, Baker Heart Institute, Professorof Medicine, Monash University, Chair,World Health Organisation CollaboratingCentre for Research and Training inCardiovascular Diseases.TOPIC: Cardiovascular Risk FactorsDr Alex BrownDirector, Centre for Indigenous VascularResearch, Baker Heart Institute, AliceSprings.TOPIC: Disparities in Qualityand Outcomes of Care in AcuteCoronary Syndrome in the NTDr Marcus IltonCardiologist, NT Cardiac ServicesTOPIC: Rheumatic Heart Disease– NT and national issuesProfessor Melanie WakefieldDirector of the Centre for BehaviouralResearch, Cancer Council Victoria.TOPIC: The Impact of TobaccoPolicy and Research in Australiaand InternationallyDr Robyn ClarkResearch Assistant, ClinicalPharmacology Royal Adelaide Hospital,National Institute of Clinical StudiesFellowship.TOPIC: Rural and UrbanDifferentials in Primary and TertiaryHeart Failure ManagementDr Sepehr ShakibDirector of Clinical Pharmacology, RoyalAdelaide Hospital, National Institute ofClinical Studies and SA Department ofHealth Fellowship.TOPIC: Chronic DiseaseManagement in an Acute ServiceInstitutionDr Nancy HuangCoordinator, National Clinical Guidelines,Heart Foundation.TOPIC: The Application ofGuidelines within Primary Care,with reference to Absolute RiskProfessor Robert NewtonFoundation Professor, Exercise and SportScience, Edith Cowan University.TOPIC: Exercise and ChronicDiseaseRegistrations Open NOW! Go to:www.nt.gov.au/health/cdc/preventable/chronicdisease.shtmlFor further information:PHONE:(08) 89228280;Email:chronicdiseasesnetwork@nt.gov.au34The<strong>Chronicle</strong> <strong>March</strong> 2008
Call for Abstracts / PostersPublication ofThe Chronic Diseases Network“Health at the Heart of Australia”Alice Springs Convention Centre 13- 15th August 200818th Annual Scientific Meeting and Exhibition of the Australian Cardiovascular Health and RehabilitationWe invite you to submit anAbstract or Poster for thisexciting conference!&12th Annual Conference of the Chronic Diseases Network of the NTThe Australian Cardiovascular Health and RehabilitationAssociation and the Chronic Diseases Network of theNT represent two groups of multidisciplinary healthprofessionals dedicated to the support, education andnetworking of people working in the fields of cardiovascularhealth and chronic diseaseAbstracts and Posters need to address the theme of theconference ‘Health at the Heart of Australia’ and focus oncardiovascular health within the context of chronic disease.Challenges for Indigenous health and remote health servicedelivery will also be a preference theme.There will be three conference streamsincluding:1.2.3.Models of Care (primary, tertiary, multi-disciplinary,rehabilitation, palliative care);Prevention and Population Health (community, individuals,health professionals);Workforce (recruitment / retention / quality improvement /training).To submit an abstract or poster, please followthese steps:1.2.3.4.Prepare a 250 word summary of your proposed presentation& include the title of presentation;Prepare a short biography of the presenter’s details (approx250 words);Go to www.thebestevents.com.au click on “CurrentEvents” and scroll to “Australian Cardiovascular Health &Rehabilitation Association & Chronic Diseases NetworkConference”;Click on the link tinyurl.com/369f8a and follow theinstructions to submit your abstract.Deadline for submission is 31st <strong>March</strong> 2008If you require assistance with on-line submission or for any further queries please contact:The Chronic Diseases NetworkT: (08) 892 28280E: chronicdiseasesnetwork@nt.gov.auThe <strong>Chronicle</strong> <strong>March</strong> 2008Chrissie Inglis, ACRA (NT Rep)T: 0409 697 32435
The <strong>Chronicle</strong>The Chronic Diseases Network acknowledges the participationand support of members of the CDN Steering Committee, fromthe following organisations:foundationCentral Australian Division ofPrimary Health Care”36The<strong>Chronicle</strong> <strong>March</strong> 2008