Fatih Durmuşoğlu_Menopausal Hormon Therapy Update.ppt ...
Fatih Durmuşoğlu_Menopausal Hormon Therapy Update.ppt ...
Fatih Durmuşoğlu_Menopausal Hormon Therapy Update.ppt ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
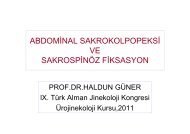
Estrogen Deprivation Related ProblemsShort-term SymptomsLong-term DiseasesDevelopmentof subclinicaldiseaseEstrogen SecretionHot flushesMood, sleep, and/oracute cognitive changesUrogenital symptomsCardiovascular diseaseOsteoporosisCognitive decline(Alzheimer’s disease)40 45 50 55 60 65 70 ‡75Age (years)
<strong>Menopausal</strong> <strong>Hormon</strong> Treatment• Mid 1970’s Endometrial cancer was related withunooposed estrogen.• 1980’s progesterone addition after estrogenpriming was accepted as protective issue onendometrium.• Long term treatment was thought as goodprotection for atherosklerozis, osteoporozis andmight have decreasing effect on postmenopausalmortality.
<strong>Hormon</strong> Tedavisi-Klinik Çalışmalar1985 NHS; HT decrease risk for MI 50%1993 Start of WHI for evaluating kardioprotection of HT.1995 PEPI; HT good for cholesterol profile1998 HERS; HT increases existing cardiovascular risk2002 WHI ended / HT ↑risk for CVD2003 WHI; ended E arm for increases in Stroke risk.2006 NHS; timing for HT is important for CVD risk.2007 WHI; early start of HT in women at perimenopausal periodnot increasing CVD risk.
Menon et al. Menopause, 2007
WHI çalışmasındaki sorunlar§ Yaş ortalaması 63§ % 34 ü obez§ % 36 sı hipertansif§ % 45 inde sigarakullanımı öyküsü8
WHI – 10.000 kadın/yılE+P ile E karşılaştırılmasıE+P50-59 yE50-59 yE+P70-79 yE70-79 yToplam FraktürlerKalça-30-2?+3-61-15?-20Kolon Ca -1 -5 -14 +17KKH +5 -10 +23 +4İnme +4 0 +13 +14DVT +9 +2 +35 +12Meme Ca +5 -8 +13 -2
Postmenopozal hormon kullanımı ve KVH<strong>Hormon</strong> başlama zamanının yaşla ilişkisi (NHS)50-59 yaş(KVH olan PM kadınlar hariç tutulmuştur)RR (%95 CI)RR = 0.7260 + yaş0 0.2 0.4 0.6 0.8 1.0 1.2 1.4Yaş, BMI, hiperkolesterolemi, hipertansiyon, ailesel KKH, diabet, sigara kullanımı, diyeterveriler, alkol alımı, fiziksel aktivite, vitamin E veya multivitamin suplementasyonu, aspirinkullanımı parametreleri ayarlanmıştır.Grodstein F et al. J Womens Health 2006
WHI; combined analysis• HT before age 60– CVD risk probably decreases– Stroke risk neither increase or decrease with startingage• HT may have protective effect but no indication forCVD• If there is health benefit this will be for youngstarters“Window of opportunity”Rossouw et al. JAMA 2007
EMAS 2011 Position Statement• Cardiovascular disease is the main cause of death in women.• Postmenopausal status is associated with a higher prevalence of coronary heartdisease.• Randomized controlled trial data show that HT does not have a role in theprimary prevention of CHD in women over 50, but most information is limited toconjugated equine estrogens and medroxyprogesterone acetate.• HT does not have a role in the secondary prevention of CHD; but the number ofpatients involved in randomized controlled trials is small.• The lowest effective estrogen dose should be used for menopausal symptoms(17beta-estradiol 0.5–1mg orally daily, conjugated equine estrogen 0.3–0.625mgdaily orally, or 25–50g 17betaestradiol transdermally).• Transdermal HT should be the first choice in women either at increased risk of CHDor with pre-existing disease because of itslesser effects on coagulation.• Regular follow up by a specialist service is recommended
WHI – İnvaziv Meme CaYıllar E+P Plasebo HazardRatio(vaka sayıları)1 12 19 0,60 (0,29-1,23)2 26 32 0,77 (0,46-1,30)3 29 22 1,26 (0,73-2,20)4 44 27 1,54 (0,95-2,49)5 43 21 1,99 (1,18-3,35)6 ve üstü 45 29 1,35 (0,85-2,16)Genel 199 150 1,24 (1,01-1,54)Ölüm 4 4Chlebowski et al. JAMA , 2003
Invaziv Meme Ca –WHI verileriHTn (yıllık oran)Plasebon (yıllık oran)HR(%95 CI)50-79 yaşE+P199 (0,41) 150 (0,33) 1,24 (1,01-1,54)+8/10.000/yıl50-79 yaşE94 (0,26) 124 (0,33) 0,77 (0,57-1,06)-7/10.000/yılChlebowski et al. JAMA, 2003WHI steering committee JAMA, 2004
TANIMLAR
Conclusions with Level of Evidence AHot flashes• “Standard-dose” estrogen with or without a progestogenmarkedly lowers the frequency and severity of hotflashes, and lower doses of estrogen are also effective inmany women.• Tibolone (a hormonal alternative widely availableworldwide but not in the United States) alleviatespostmenopausalvasomotor symptoms.
Conclusions with Level of Evidence AUrogenital system• Very low doses of vaginal estradiol relieve symptomsand normalize vaginal atrophy.• Estrogen used vaginally or systemically reduces thesymptoms of overactive bladder.• Vaginal estrogen reduces the incidence of recurrent urinarytract infections.• Tibolone improves urogenital atrophy.
Conclusions with Level of Evidence ABone• Estrogen with or without a progestogen prevents earlypostmenopausal bone loss and augments bone mass inlate postmenopause as effectively as the bisphosphonates.• Estrogen alone and estrogen plus a progestogen preventhip and vertebral fractures.• Tibolone significantly reduces vertebral and nonvertebralfractures in osteoporotic women over the age of 60 yr.• Raloxifene, a selective estrogen receptor modulator,improves bone mineral density and reduces vertebralbut not hip fractures.
Conclusions with Level of Evidence AColon cancer• MHT with estrogen plus a progestogen decreases coloncancer risk.Breast• Raloxifene decreases breast cancer risk.• Estrogen and estrogen plus a progestogen increasemammographic density.• Tibolone increases risk of breast cancer recurrence.
Conclusions with Level of Evidence ASexual function• Physiological amounts of transdermal testosterone increasethe number of self-reported, sexually satisfying events permonth as well as desire, arousal, responsiveness,and orgasm.• DHEA does not significantly improve sexual function.Venothrombotic episodes• MHT increases the risk of venothrombotic episodesapproximately 2-fold and is multiplicative with baselinerisk factors including age, higher body mass index,thrombophilias, surgery, and immobilization.• Raloxifene increases the incidence of venothromboticepisodes.
Conclusions with Level of Evidence AStroke• Tibolone increases risk of stroke in older but not inyounger women.• No increase in stroke occurs with raloxifene.• <strong>Hormon</strong>e use does not reduce stroke incidence in olderwomen with preexisting vascular disease.Endometrium• Estrogen alone without a progestogen causes an increasein endometrial cancer.• Continuous estrogen plus a progestogen does not causeendometrial cancer.• Tibolone does not induce endometrial hyperplasia orcarcinoma
Conclusions with Level of Evidence AGallbladder• Estrogen alone and estrogen plus a progestogenincrease the risk of gallbladder disease.Cognition• MHT initiated after age 60 yr does not improvememory
Selected Conclusions with Level ofEvidence BMetabolism• Use of estrogen alone and estrogen plus a progestogenin theWHIwas associated with a decrease in the risk fortype 2 diabetes.• Initiation of MHTis associated with lesser accumulationof weight, fat mass, and/or centrally located fat mass.Joints• Estrogen exerts a protective effect on osteoarthritis.• Estrogen alone reduces total arthroplasty rate.• Addition of a progestogen to estrogen appears to counteractthe beneficial effects of estrogen on arthroplasty rate.
Selected Conclusions with Level ofEvidence BQuality of life• MHTproduces an improvement in health-related qualityof life through decreased symptoms, sleep enhancement,and, possibly, mood enhancement.Sexual function• Tibolone improves sexual well-being in postmenopausalwomen presenting with low libido, with greaterimprovements in desire, arousal, satisfaction, andreceptiveness than seen with transdermal estrogenprogestogentherapy.
Selected Conclusions with Level ofEndometriumEvidence B• Sequential estrogen plus a progestogen reduces therisk of endometrial carcinoma compared to estrogenbut not as effectively as continuous estrogen plus aprogestogen.• Vaginal estrogen in doses of 7.5 to 25 g twice weeklydoes not stimulate the endometrium.• Raloxifene reduces the incidence of endometrialcarcinoma.
Selected Conclusions with Level ofEvidence BPremature menopause• Women with bilateral oophorectomy prior to age 45are at increased risk of negative effects on the cardiovascularsystem, bone, cognition, mood, and sexuality.Overall mortality• MHT was associated with a 40% reduction in mortalityin women in trials in which participants had a mean agebelow 60 yr or were within 10 yr of menopause onset.
Selected Conclusions with Level ofEvidence BCoronary heart disease (CHD)• Basic science, animal models, and observational studiessupport the hypothesis that MHT may prevent atherosclerosisand reduce CHD events.• Subgroup analyses suggest that the lack of benefit orincrease in CHD risk observed in the overall analysis ofthe WHIresulted from harmful effects of MHT in olderwomen starting therapy many years after onset ofmenopause.• Tibolone does not increase the risk of CHD events.
Selected Conclusions with Level ofEvidence B• Use of estrogen alone for less than 5 yr may reduce therisk of breast cancer in patients starting therapy manyyears after the onset of menopause.• Tibolone reduces the risk of developing breast cancer.• Estrogens increase the risk of breast cancer after morethan 5 yr of use, particularly in recently menopausalwomen.• Combined estrogen and progestogen therapy increasesthe risk of invasive breast cancer, which may occurwithin 3 to 5 yr of initiation and rises progressively beyond thattime.
Important points for future• Disseminate literature to practitioners and postmenopausal womenregarding the levels of benefit and risk associated with MHT asprescribed in currently used doses, in women close to menopause,and for periods of less than 3–5 yr.• Continue research on lowest doses, optimal administration routes,and optimal products.• Conduct research to identify women who may specifically benefit orbe at risk from MHT.• Develop new approaches to maximize benefit and minimize risk.• Conduct randomized trials to examine rate of cardiovascularevents, stroke, breast cancer, and carbohydrate intolerance asprimary endpoints in women starting MHT for the first time betweenthe ages of 50 and 55 yr.
Conclusions•The major conclusions related to the overall benefits and risks of MHTexpressed as the number of women per1000 taking MHTfor 5yr whowould experience benefit or harm.•Primary areas of benefit included relief of hot flashes andsymptoms of urogenital atrophy and prevention of fractures anddiabetes.•Risks included venothrombotic episodes, stroke, andcholecystitis.•In the subgroup of women starting MHT between ages 50 and59 or less than 10 yr after onset of menopause, trendssuggested additional benefit including reduction of overallmortality and coronary artery disease.(J Clin Endocrinol Metab 95: S7–S66, 2010)
Conclusions cont.•In this subgroup, estrogen plus some progestogens increasedthe risk of breast cancer, whereas estrogen alone did not.•Beneficial effects on colorectal and endometrial cancer andharmful effects on ovarian cancer occurred but affected only asmall number of women.•Data from the various studies, which involved women ofaverage age 63, cannot be appropriately applied to calculaterisks and benefits of MHT in women starting shortly aftermenopause.•At the present time, assessments of benefit and risk in theseyounger women are based on lower levels of evidence.(J Clin Endocrinol Metab 95: S7–S66, 2010)
![Engin Oral_Konjenital uterus anomalileri.ppt [Uyumluluk Modu]](https://img.yumpu.com/51729800/1/190x146/engin-oral-konjenital-uterus-anomalilerippt-uyumluluk-modu.jpg?quality=85)