Freedom of Information and Protection of Privacy Act - Ontario ...
Freedom of Information and Protection of Privacy Act - Ontario ...
Freedom of Information and Protection of Privacy Act - Ontario ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
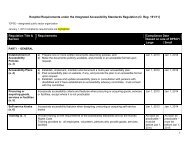
March 2011Frequently Asked Questions:<strong>Freedom</strong> <strong>of</strong> <strong>Information</strong> <strong>and</strong><strong>Protection</strong> <strong>of</strong> <strong>Privacy</strong> <strong>Act</strong>BACKGROUND/CONTEXTThe Broader Public Sector Accountability <strong>Act</strong> contains amendments to the <strong>Freedom</strong> <strong>of</strong><strong>Information</strong> <strong>and</strong> <strong>Protection</strong> <strong>of</strong> <strong>Privacy</strong> <strong>Act</strong> (FIPPA or <strong>Act</strong>) that brings hospitals under the<strong>Freedom</strong> <strong>of</strong> <strong>Information</strong> (FOI) regime beginning January 1, 2012. These Questions <strong>and</strong>Answers were prepared by the <strong>Ontario</strong> Hospital Association (OHA) in consultation with theMinistry <strong>of</strong> Government Services, the Ministry <strong>of</strong> Health <strong>and</strong> Long-Term Care (MOHLTC), <strong>and</strong>the Office <strong>of</strong> the <strong>Information</strong> <strong>and</strong> <strong>Privacy</strong> Commissioner <strong>of</strong> <strong>Ontario</strong> (IPC). The answers set outbelow are intended to help hospitals underst<strong>and</strong> FIPPA in order to support its effectiveimplementation.This document is intended for general informational purposes only <strong>and</strong> should not be construedas legal advice. For detailed information regarding specific situations, hospitals may wish toconsult independent legal counsel.GENERAL INFORMATION/APPLICATION1. What information/records does the <strong>Act</strong> apply to?FIPPA will apply to “records” that have been in the “custody or control” <strong>of</strong> a hospital sinceJanuary 1, 2007, unless the record is subject to an express exclusion under the <strong>Act</strong>. “Record”means any record <strong>of</strong> information however recorded, whether in printed form, on file, byelectronic means or otherwise. The public will have a right to hospital records in the form thatthey are stored; however, in response to a particular request, the hospital may have anobligation to produce a single electronic record that combines information from variousindependent records. Sometimes, compiling information or calculating a statistic is a convenient<strong>and</strong> sensible means <strong>of</strong> answering an access request.A hospital does not have the duty to create a record, but it does have a duty to provide anelectronic record in a requested format if producing it does not unreasonably interfere with theoperations <strong>of</strong> the hospital. Costs can be passed on to the requester in certain circumstances.
2. How do we determine if a record is under the custody or control <strong>of</strong> the hospital?In general, custody means the keeping, care, watch, preservation or security <strong>of</strong> the record for alegitimate business purpose. While physical possession <strong>of</strong> a record may not be sufficient toconstitute custody, it is the best evidence <strong>of</strong> custody. An institution must have some right to dealwith the records; “bare possession” with no right to do anything with the record is not consideredcustody.In general, control <strong>of</strong> a record does not mean having actual physical possession <strong>of</strong> the record,but rather the power or authority to make a decision about the use or disclosure <strong>of</strong> the record.Based on past decisions <strong>of</strong> the courts <strong>and</strong> the IPC, a “broad <strong>and</strong> liberal” approach is normallytaken to determine custody or control. For further information, see IPC Order MO-1251.Thequestion <strong>of</strong> whether FIPPA’s purpose <strong>of</strong> institutional accountability may also be relevant indetermining whether the hospital has custody or control <strong>of</strong> a record.The IPC has developed a list <strong>of</strong> factors to consider in determining whether or not a record is inthe custody or control <strong>of</strong> an institution. These factors include:Was the record created by an <strong>of</strong>ficer or employee <strong>of</strong> the institution?What use did the creator intend to make <strong>of</strong> the record?Does the institution have statutory power or the duty to carry out the activity thatresulted in the creation <strong>of</strong> the record?Is the activity in question a “core”, “central” or “basic” function <strong>of</strong> the institution?Does the content <strong>of</strong> the record relate to the institution’s m<strong>and</strong>ate <strong>and</strong> functions?Does the institution have physical possession <strong>of</strong> the record, either because it hasbeen voluntarily provided by the creator or pursuant to a m<strong>and</strong>atory statutory oremployment requirement?If the institution does not have possession <strong>of</strong> the record, is it being held by an <strong>of</strong>ficeror employee <strong>of</strong> the institution for the purposes <strong>of</strong> his or her duties as an <strong>of</strong>ficer oremployee?Does the institution have a right to possession <strong>of</strong> the record?Does the institution have the authority to regulate the record’s content, use<strong>and</strong> disposal?Are there any limits on the use to which the institution may put the record, what arethose limits, <strong>and</strong> why do they apply to the record?To what extent has the institution relied upon the record?How closely is the record integrated with other records held by the institution?What is the customary practice <strong>of</strong> the institution, as well as similar institutions, inrelation to possession or control <strong>of</strong> records <strong>of</strong> this nature, in similar circumstances?2
If the record is not in the institution’s possession, some additional factors the IPC considersinclude the following: Who owns the record? Who paid for the creation <strong>of</strong> the record? Are there any provisions in any contracts between the institution <strong>and</strong> the person whocreated the record that give the institution the right to possess or otherwise controlthe record? Was the person who created the record an agent <strong>of</strong> the institution for the purposes <strong>of</strong>the activity in question? What is the customary practice about control over records <strong>of</strong> this nature in theindustry?IPC Orders P-120, P-239 <strong>and</strong> MO-1251 should be reviewed for a more comprehensive list <strong>of</strong>factors the IPC has considered in past decisions.3. Does FIPPA apply to records from a long-term care facility that is owned <strong>and</strong>operated by a hospital?Generally speaking, FIPPA does not currently apply to the long-term care (LTC) sector. (FIPPAhas been extended to only include the hospital sector at this time). As such, on an individualFIPPA request basis, the hospital would need to determine if it has “custody or control” <strong>of</strong> theLTC home record to determine whether the record is responsive to the specific FIPPA request.For greater clarity, if a hospital has custody or control <strong>of</strong> a LTC home record, then that record issubject to FOI even though generally the LTC sector is not. See question #2 for furtherinformation on how to determine custody or control <strong>of</strong> a record.4. What records are not covered by the <strong>Act</strong>?Records that are subject to express exclusions under the <strong>Act</strong> are not covered by the <strong>Act</strong>. Forexample, records that relate to: employment, labour relations, the appointments or privileges <strong>of</strong>health pr<strong>of</strong>essionals, regulated health pr<strong>of</strong>essionals’ private practice records, as well asresearch <strong>and</strong> teaching records, hospital foundation <strong>and</strong> charitable donation records, <strong>and</strong>records relating to the provision <strong>of</strong> abortion services are excluded from the <strong>Act</strong>. It is alsoimportant to note that FIPPA does not apply to “personal health information” that is subject tothe Personal Health <strong>Information</strong> <strong>Protection</strong> <strong>Act</strong> (PHIPA).As a result <strong>of</strong> an amendment to the Quality <strong>of</strong> Care <strong>Information</strong> <strong>Protection</strong> <strong>Act</strong> (QCIPA), FIPPAdoes not apply to “quality <strong>of</strong> care information” prepared by or for a designated quality <strong>of</strong> carecommittee under QCIPA. Section 1 <strong>of</strong> QCIPA defines “quality <strong>of</strong> care information” as information3
that: (a) is collected by or prepared for a quality <strong>of</strong> care committee for the sole or primarypurpose <strong>of</strong> assisting the committee in carrying out its functions, or (b) relates solely or primarilyto any activity that a quality <strong>of</strong> care committee carries on as part <strong>of</strong> its functions.It should be noted, however, that this exclusion does not extend to quality <strong>of</strong> care information<strong>and</strong> records generated outside <strong>of</strong> QCIPA, such as root cause analysis, failure mode <strong>and</strong> effectsanalysis, self-assessment activities or chart reviews. Other records that relate primarily topatient safety <strong>and</strong> risk management may qualify for an exemption from disclosure under otherprovisions <strong>of</strong> the <strong>Act</strong>.5. When does the <strong>Act</strong> apply to hospitals?The <strong>Act</strong> applies to hospitals as <strong>of</strong> January 1, 2012, but is retrospective to January 1, 2007. As aresult, records that came into a hospital’s custody <strong>and</strong>/or control on or after January 1, 2007 aresubject to the <strong>Act</strong>.6. Does the <strong>Act</strong> apply to other health care organizations/providers?FIPPA was amended by Bill 122, the Broader Public Sector Accountability <strong>Act</strong>, passed inDecember 2010 to bring hospitals under <strong>Ontario</strong>’s freedom <strong>of</strong> information <strong>and</strong> privacy regime.No other health care organizations were added at that time. However, many health-relatedorganizations <strong>and</strong> agencies have been made subject to the <strong>Act</strong> through designation as“institutions” under the FIPPA regulation. For example, Local Health Integration Networks(LHINs) were added as an institution in 2005, <strong>and</strong> Cancer Care <strong>Ontario</strong> was added in 2010. TheMOHLTC <strong>and</strong> other provincial <strong>and</strong> municipal institutions involved in the delivery <strong>of</strong> health careare also subject to FIPPA.7. Does the <strong>Act</strong> apply to email/text messages?Yes, e-mail <strong>and</strong> text messages are “records” for the purposes <strong>of</strong> FIPPA <strong>and</strong>, in general, aresubject to the right <strong>of</strong> access. However, there is significant ongoing litigation relating to whetheremployees’ “personal communications” that are stored in an organization’s network informationsystems are records under the “custody or control” <strong>of</strong> a FIPPA institution.A recent judicial review by the <strong>Ontario</strong> Superior Court <strong>of</strong> Justice <strong>of</strong> an IPC decision found thatpersonal emails unrelated to work that were sent <strong>and</strong> received from a workplace email addresswere not subject to the Municipal <strong>Freedom</strong> <strong>of</strong> <strong>Information</strong> <strong>and</strong> <strong>Protection</strong> <strong>of</strong> <strong>Privacy</strong> <strong>Act</strong>(MFIPPA) 1 . MFIPPA is the municipal equivalent <strong>of</strong> FIPPA <strong>and</strong> contains the same “custody or1 City <strong>of</strong> Ottawa v. <strong>Ontario</strong>, 2010 ONSC 6835. The IPC is requesting leave to appeal the decision to theCourt <strong>of</strong> Appeal <strong>of</strong> <strong>Ontario</strong>.4
control” provisions. Specifically, the employee’s personal emails were not considered to bewithin the “custody or control” <strong>of</strong> the institution. The Court held that the IPC Adjudicator failed toconsider the purpose <strong>and</strong> intent <strong>of</strong> FOI legislation in determining the <strong>Act</strong> applied to theserecords. The IPC has requested leave to appeal the Divisional Court’s decision to the <strong>Ontario</strong>Court <strong>of</strong> Appeal.The outcome <strong>of</strong> this litigation may affect how hospitals respond to specific requests, but doesnot warrant any change in approach to the management <strong>of</strong> electronic communications. Asalways, hospitals should require responsible use <strong>of</strong> hospital communication systems <strong>and</strong> shouldreserve a broad right <strong>of</strong> access to all communications stored on their systems. Individualsshould underst<strong>and</strong> that all emails sent <strong>and</strong> received via hospital-administered systems are notprivate vis-à-vis the hospital, <strong>and</strong> beginning on January 1, 2012, may be required to be retrieved<strong>and</strong> examined for the purpose <strong>of</strong> complying with FIPPA.8. What is the role <strong>of</strong> the <strong>Information</strong> & <strong>Privacy</strong> Commissioner under FIPPA?The Commissioner is appointed by <strong>and</strong> reports to the Legislative Assembly <strong>of</strong> <strong>Ontario</strong> <strong>and</strong> isindependent <strong>of</strong> the government <strong>of</strong> the day. The IPC provides an independent review <strong>of</strong> thedecisions <strong>and</strong> practices <strong>of</strong> institutions covered by the <strong>Act</strong> concerning access <strong>and</strong> privacy. Tosafeguard the rights established under the <strong>Act</strong>, the IPC has the following key roles:Resolving appeals when institutions refuse to grant access to information;Investigating privacy complaints related to information held by institutions;Ensuring that institutions comply with the <strong>Act</strong>s;Conducting research on access <strong>and</strong> privacy issues <strong>and</strong> providing advice onproposed government legislation <strong>and</strong> programs; <strong>and</strong>Educating the public about <strong>Ontario</strong>’s access, privacy <strong>and</strong> personal healthinformation laws <strong>and</strong> access <strong>and</strong> privacy issues.In resolving access to information appeals, the IPC has the ability to issue orders to resolveissues raised during the appeal, including requiring institutions subject to the <strong>Act</strong> to discloserecords. <strong>Privacy</strong> complaints may be resolved either informally or formally. Formal resolutionmay result in the IPC issuing a public investigation report containing recommendations foraction by the institution that is the subject <strong>of</strong> the investigation.5
9. What is the role <strong>of</strong> the “head” under FIPPA?The <strong>Act</strong> refers to the “head <strong>of</strong> the institution” as the person responsible for making decisions inrespect <strong>of</strong> access requests. The head is responsible for the <strong>Act</strong>’s day-to-day administration <strong>and</strong>decision-making <strong>and</strong> for ensuring that personal information held by the hospital is accurate, upto-date<strong>and</strong> collected, used <strong>and</strong> disclosed only as authorized.FIPPA identifies the chair <strong>of</strong> the board <strong>of</strong> a public hospital, the superintendent <strong>of</strong> a privatehospital <strong>and</strong> the chair <strong>of</strong> the board <strong>of</strong> the Ottawa Heart Institute as the “head”. The <strong>Act</strong> permitsthe head to delegate in writing some or all <strong>of</strong> his/her powers <strong>and</strong> duties under the <strong>Act</strong> to an<strong>of</strong>ficer(s) <strong>of</strong> the hospital. It is essential that the delegated <strong>of</strong>ficer(s) have expert knowledge aboutthe <strong>Act</strong> <strong>and</strong> the hospital, <strong>and</strong> have the authority to make decisions independently. The head,however, ultimately remains accountable for all actions taken <strong>and</strong> any decisions made under the<strong>Act</strong>. The head may also place limitations, restrictions, conditions or requirements on thedelegation <strong>of</strong> powers (Section 62). The <strong>Act</strong> specifies circumstances where the head must denyaccess to information, may exercise his/her discretion to deny access, or grant access.A summary <strong>of</strong> the head’s responsibilities are as follows: Adhering to time limits <strong>and</strong> notification requirements; Considering representations from third parties; Responding to access requests; Determining the method <strong>of</strong> disclosure; Responding to requests for correction <strong>of</strong> personal information; Obligation/ discretion to refuse access based on exemptions; Calculating <strong>and</strong> collecting fees; Providing access to the public by preparing manuals <strong>and</strong> guidelines <strong>of</strong> records; Include in a personal information bank all personal information under the institution'scontrol, (that is not personal health information); Responding to access appeals; <strong>and</strong> Administering the privacy protection provisions <strong>of</strong> the <strong>Act</strong>.10. What are the reporting obligations <strong>of</strong> hospitals under FIPPA?Hospitals must submit an annual report to the IPC. The report must set out:The number <strong>of</strong> access requests received;The number <strong>of</strong> requests refused, the provisions <strong>of</strong> the <strong>Act</strong> relied upon for refusal, <strong>and</strong>the number <strong>of</strong> times each provision was invoked;For each provision <strong>of</strong> the <strong>Act</strong>, the number <strong>of</strong> appeals commenced;6
The number <strong>of</strong> times personal information was used or disclosed for a purpose which isnot included in the statements <strong>of</strong> uses <strong>and</strong> purposes set forth under section 45paragraphs (d) <strong>and</strong> (e) <strong>of</strong> the <strong>Act</strong> (relating to the use <strong>of</strong> personal information banks);The amount <strong>of</strong> fees collected under section 57 <strong>of</strong> the <strong>Act</strong>, <strong>and</strong>Any other information indicating an effort by the institution to put into practice thepurposes <strong>of</strong> the <strong>Act</strong>.These are in addition to the existing reporting requirements under PHIPA.DEALING WITH ACCESS REQUESTS11. Who can request records?Any person can make a request for access to records. A “person” includes individuals <strong>and</strong>organizations such as corporations, partnerships <strong>and</strong> sole proprietorships. The right <strong>of</strong> access isnot limited by citizenship or place <strong>of</strong> residence. It is important to note that there may besituations where one person represents another individual (e.g., substitute decision maker). Therights <strong>and</strong> powers which an individual may exercise on behalf <strong>of</strong> another include the right tomake access requests.12. How does the request process begin?Under the <strong>Act</strong>, an access request must be made in writing, be accompanied by the $5.00application fee, <strong>and</strong> provide sufficient detail to enable an experienced hospital employee toidentify the record(s) requested. If an individual is seeking access to his/her own personalinformation, the request must also identify the personal information bank or the location <strong>of</strong> thepersonal information being requested. If after a thorough search, the institution cannot locatethe requested personal information, <strong>and</strong> the requester cannot provide any credible evidence tosupport the existence <strong>of</strong> records, the head may conclude that the institution does not have therecords.There is a prescribed form available on the IPC website <strong>and</strong> the Ministry <strong>of</strong> GovernmentServices website for access requests. A letter (not on the prescribed form) that makes referenceto the <strong>Act</strong> is also considered a request if accompanied by the required application fee. If aninstitution is in doubt about whether or not a requester wishes a letter <strong>of</strong> inquiry to be treated asa request under the <strong>Act</strong>, the requester should be contacted <strong>and</strong> clarification <strong>of</strong> the inquiryobtained.FIPPA does not require a freedom <strong>of</strong> information request to access hospital records. If a formalaccess request can be better h<strong>and</strong>led by the hospital on an informal basis, the hospital should7
contact the requester to determine whether he/she is agreeable to this change. An agreement torequest a record on an informal basis generally results in quicker access to the records, butremoves the opportunity to appeal the hospital’s decision at a later date.13. How long do we have to respond to a request?The <strong>Act</strong> requires the institution to respond to access requests within 30 calendar days from thedate a request is received. The 30-day time period starts to run the day the institution receives acomplete request. A complete request is one which has been clarified, or one which providessufficient detail to allow the institution to underst<strong>and</strong> what information is being requested. The$5.00 application fee must also have been received.The institution may extend the 30-day time limit in two situations:i. The request is for a large number <strong>of</strong> records or necessitates a search through a largenumber <strong>of</strong> records <strong>and</strong> meeting the time limit would unreasonably interfere with theoperations <strong>of</strong> the institution; orii. Consultations with a person outside the institution are necessary to comply with therequest <strong>and</strong> cannot reasonably be completed within the time limit.The time limit for responding to a request is automatically extended where notice is given to athird-party.For example: An institution that receives an access request for records whose disclosuremay affect a third-party must notify the third-party within 30 days <strong>of</strong> receiving the request.This initial time period allows the institution time to gather the records, make a determinationthat a third-party must be consulted <strong>and</strong> define exactly what the-third party must beconsulted about. The third-party is allowed 20 days to respond to this notice. Upon receipt <strong>of</strong>the third-party's response, the institution has a further 10 days to make its final decisionabout the requested records. Under normal circumstances then, an institution would have upto 60 days to respond to an access request that involves third-party notification.14. How long do we have to respond to a request that has been forwarded or transferredto another institution?A hospital has 15 calendar days from the date a request is received to forward or transfer therequest. The 30-day time limit begins when the request is received at the first institution. Thesecond institution that receives the request has the remainder <strong>of</strong> the 30-day period to respond.For more information on forwarding or transferring a request see question # 23.8
15. Do we need to have a formal FIPPA request before we can release information?No. Hospitals may continue to respond to informal requests for information. The access toinformation regime established by FIPPA is only one avenue through which hospitals are able torelease information. Because <strong>of</strong> the resources involved in the formal FOI process, it should bereserved for requests where information will not be released, or where there is some questionas to the hospital’s ability to disclose records. Hospitals are encouraged to consider theproactive disclosure <strong>of</strong> information to the public on a routine basis to minimize the volume <strong>of</strong>requests.16. Does the request have to be in writing?Yes, under the <strong>Act</strong> a formal access request must be made in writing. Only a formal requestprovides the requester with the opportunity to appeal the hospital’s decision to the IPC at a laterdate. For more information on formal vs. informal requests see question # 12.17. What is the fee structure under FIPPA?FIPPA adopts a user pay principle; a person making an access request must pay some <strong>of</strong> thecosts the hospital incurs in processing the request. A fee schedule is contained in the regulationto FIPPA. Under FIPPA, different fees are applied depending on whether the request is forgeneral records or the requester's own personal information. Fees must be charged unless theyare waived by the institution.A $5.00 m<strong>and</strong>atory application fee must accompany a request for either personal information orgeneral records under FIPPA. Once the application fee is received, the head is required toprovide a requester with access to records <strong>and</strong>/or a decision letter within 30 days. Thisrequirement does not apply if the m<strong>and</strong>atory application fee has not been received by theinstitution. The onus is on the institution to collect this application fee before processing therequest if it decides to proceed.A request for personal information under FIPPA is a request made by an individual (or anotherperson acting on his/her behalf) for the individual's own information. No fees are charged forsearch or preparation time, but there are fees for photocopying ($0.20 per page) <strong>and</strong> computercosts as specified in the regulations.All other (general record) requests under FIPPA may be subject to the following charges: Photocopies <strong>and</strong> computer printouts; The amount <strong>of</strong> time required to search for records; Personnel time involved in physically preparing the record for disclosure;9
Computer costs; <strong>and</strong> Shipping costs.Refer to Regulation 460 under FIPPA for further details on charges.18. Do we have to provide an estimate <strong>of</strong> the expected fee?Unlike PHIPA, a fee estimate is only required under FIPPA where it appears that the cost <strong>of</strong>processing the request will be over $25.00. Further, where the cost estimate is $100.00 or more,the head may require the requester to pay a deposit equal to 50 per cent <strong>of</strong> the estimate beforetaking any further steps to respond to the request.19. Can we waive the fees?Yes, under FIPPA a head must waive the payment <strong>of</strong> all or part <strong>of</strong> the fee where the head is <strong>of</strong>the opinion that it is fair <strong>and</strong> equitable to do so. This decision is made only after the head hasconsidered specific factors provided in the <strong>Act</strong>. Under FIPPA, it is the requester's responsibilityto ask the institution for a fee waiver. A request for a waiver need not be explicit, it may beimplied. The party seeking a fee waiver also bears the responsibility <strong>of</strong> establishing his/hercase.20. Are there costs associated with appealing a decision under FIPPA?Yes, under FIPPA there are m<strong>and</strong>atory fees for a requester appealing a decision to the IPC. A$10.00 fee applies to personal information request appeals <strong>and</strong> a $25.00 fee applies for generalrecords request appeals. There is no fee for a third-party to appeal an institution's decision todisclose information.21. Can we refuse a request for access to a record? What happens then?Yes, a request for a record can be refused where: (1) the record or part <strong>of</strong> the record falls withinone <strong>of</strong> the enumerated exemptions, or (2) the head is <strong>of</strong> the opinion that the request is frivolousor vexatious. (Subsection 10(1))Once the decision to refuse access to the record, in whole or in part, has been made, writtennotice <strong>of</strong> the decision (a “decision letter”) must be provided to the requester <strong>and</strong> any affectedthird-parties. The decision letter must be provided to the requester within the 30-day time period(or within the period <strong>of</strong> extended time, if any).10
However, if third-party notices have been given, the decision letter cannot be issued until the20-day period in which a third-party can respond to a third-party notice has elapsed, or sooner ifthe third-party responds before the 20 days expire.The decision letter must contain the following information:A statement that the record does not exist; orWhere the record exists, the specific provision <strong>of</strong> the <strong>Act</strong> under which access is refused<strong>and</strong> the reason the provision permits the head to deny access;The name <strong>and</strong> position <strong>of</strong> the person responsible for the decision; <strong>and</strong>That the requester may appeal the decision to the Commissioner.The head is also required to provide the requester with a clear description <strong>of</strong> the recordsresponsive to the request. The decision letter should be accompanied by a detailed index <strong>of</strong>records at issue which describes the subject matter <strong>of</strong> the withheld record(s) in general terms.This can be done by providing at least a summary <strong>of</strong> the categories <strong>of</strong> the responsive records inenough detail that the requester should be in the position to make a reasonably informeddecision on whether to seek a review <strong>of</strong> the head's decision with the IPC.If a head does not give the requester notice <strong>of</strong> his/her decision within the 30 days (or within thetime frames extended under the extension <strong>of</strong> time, for third-party notice procedures) the head isdeemed to have refused access to the record, <strong>and</strong> this refusal can be appealed to the IPC bythe requester.22. Are we allowed to ask the reason/purpose for the request? If so, can this be used as ajustification to deny access to a record?A hospital is permitted to ask for the purpose <strong>of</strong> a request if this will assist the hospital inidentifying the specific records that the requester is looking for. Obtaining this information canhelp you determine what types or categories <strong>of</strong> records to search for. However, care must betaken to properly word the question when you are seeking reasons for the request because therequester has no obligation to provide reasons. When asking “why” it is important to explain tothe requester that knowing the purpose <strong>of</strong> the request will assist you in finding the exactdocument they are looking for. Note: the purpose <strong>of</strong> the request is irrelevant to FIPPA <strong>and</strong>cannot be used as a reason to refuse disclosure.23. Where a request for access to records from ‘Hospital A’ is made to ‘Hospital B’, whichhospital is responsible for h<strong>and</strong>ling the request?Forwarding a request – Occurs when “Hospital A” does not have the record in its custody orunder its control11
Where “Hospital A” receives a request for access to a record that is not in the hospital’s custodyor under its control, the head is required to make inquiries to determine whether “Hospital B”has the record in their custody or control. Where the head determines that “Hospital B” doeshave custody or control <strong>of</strong> the record, the head (<strong>of</strong> “Hospital A”) has 15 days after the originalaccess request was received to (a) forward the request to “Hospital B”; <strong>and</strong> (b) provide writtennotice to the requester that the request has been forwarded to “Hospital B.”Transferring a request – Occurs when “Hospital A” may or may not have the record but“Hospital B” has a greater interest in the record.Where “Hospital A” receives a request for access to a record that the head believes “Hospital B”has a greater interest in, the head may transfer the request to “Hospital B”. In this situation“Hospital A” may also be required to transfer the record where “Hospital B” does not have therecord despite its greater interest. The head must provide written notice <strong>of</strong> the transfer to therequester, <strong>and</strong> complete the transfer within 15 days after receiving the access request. Whatconstitutes a “greater interest” is described in subsection 25(3) <strong>of</strong> the <strong>Act</strong>. Two essential factorsdetermine greater interest:i. A record was originally produced in or for an institution; orii.A record was not produced in or for an institution, but it was the first to receive acopy <strong>of</strong> itA request from “Hospital A” is deemed to be forwarded or transferred to “Hospital B” on the day“Hospital A” received the request. (Subsection 24(4))24. How are hospitals to deal with requests for access to records that contain third-partypersonal information?If the “third-party information” is personal health information, the request cannot be processedunder FIPPA.Records sometimes contain information concerning a person other than the requester. Beforegranting access to a record affecting a third-party, a head must give written notice to the thirdpartyto whom the information relates. The information is considered to affect a third-party if:The head has reason to believe that the record contains third-party information,proprietary, commercial or labour relation information described in section 17(1) <strong>of</strong>the <strong>Act</strong>; or12
The record contains personal information (not personal health information) that thehead has reason to believe might, if released, constitute an unjustified invasion <strong>of</strong>personal privacy.25. What is the notice requirement for access to records that contain third-party personalinformation?If the head intends to release the records, then the affected party must be given notice. Noticeto an affected party gives that party an opportunity to make representations to the hospital abouthow the proposed disclosure <strong>of</strong> records will affect him/her.The notice must contain:A statement that the head intends to disclose a record or part <strong>of</strong> a record that may affectthe interests <strong>of</strong> the person or organization;A description <strong>of</strong> the contents <strong>of</strong> the record or the part that relates to the third-party; <strong>and</strong>A statement that the person may, within 20 days after the notice is given, makerepresentations to the head as to why the record in whole or in part should not bereleased.The notice must be given within the initial 30-day period after a complete request is received or,if there has been an extension <strong>of</strong> time, within the extended time period. The third-party then has20 days after the notice is given to make representations to the head. Representations are to bein writing unless the head permits them to be made orally. After the representations arereceived, or after the 20-day period for representations has elapsed (whichever time is shorter),the head must decide within 10 days whether to disclose the record.If affected third-parties have been notified, this will delay the processing <strong>of</strong> a request. Therefore,the head must notify the requester <strong>of</strong> the delay. It is advisable to do this at the same time thatthe affected third-party is notified. The notice to the requester must state that the:Disclosure <strong>of</strong> the record or part may affect the interests <strong>of</strong> a third-party;Third-party has an opportunity to make representations concerning the disclosure; <strong>and</strong>The head will decide within 30 days if the record or part will be released.13
If a head decides to release a record in whole or in part that affects a third-party <strong>and</strong> has heardrepresentations from the third-party, or the time period for making representations has expired,the head must notify the requester <strong>and</strong> the affected third-party that:The affected person may appeal the decision to the IPC within 30 days; <strong>and</strong>The requester will be given access to the record or part unless such an appeal is filedwithin the 30 days after the notice is given.26. How are hospitals to deal with requests for access to records that contain third-partyinformation <strong>of</strong> a commercial party?Hospitals <strong>of</strong>ten acquire information about the activities <strong>of</strong> private sector organizations. Some <strong>of</strong>this information may constitute a valuable asset to the organization, <strong>and</strong> disclosure would impairits ability to compete effectively. FIPPA provides a m<strong>and</strong>atory exemption from disclosure forcertain third-party information where disclosure could reasonably be expected to cause certainharms. This exemption is not limited to commercial third-parties, but can also be applied to anysupplier or institution (including another hospital) which meets all three <strong>of</strong> the following thresholdtests:1. The information must fit within one <strong>of</strong> the specified categories <strong>of</strong> third-partyinformation;2. The information must have been "supplied" by the third-party "in confidence",implicitly or explicitly; <strong>and</strong>3. The disclosure <strong>of</strong> the information could reasonably be expected to cause certainharms as specified in the (third-party) exemption.The threshold test has been the subject <strong>of</strong> significant IPC jurisprudence <strong>and</strong> interpretation bythe courts. For example, in general, contracts with suppliers <strong>of</strong> goods <strong>and</strong> services arenegotiated, not “supplied” <strong>and</strong> therefore do not qualify for this exemption.27. What is the notice requirement for access to records that contain third- partyinformation <strong>of</strong> a commercial party?FIPPA provides that before access is granted to a record that might contain information referredto in the third-party exemption, that party must be notified <strong>and</strong> given the opportunity to makerepresentations before a final access decision is made. If a third-party claims in itsrepresentations that the record is exempt, the burden <strong>of</strong> establishing that the record falls withinthe exemption rests with that third-party. Similarly, where an institution asserts that this14
provision applies, the burden <strong>of</strong> pro<strong>of</strong> is on the institution. It should be noted that the finaldecision on whether the record should be disclosed rests with the institution, not the third-party.28. Can a hospital publicly post who is making access requests <strong>and</strong> the costs <strong>of</strong> h<strong>and</strong>lingthe request?No, a hospital is not able to publicly identify/ post the names <strong>of</strong> individuals who make accessrequests. In fact, the identity <strong>of</strong> a requester should only be shared with the hospital staff whorequire the information in order to respond to the request. The costs <strong>of</strong> h<strong>and</strong>ling a particularrequest can only be published as long as the requester cannot be identified in anyway. Forexample, linking a particular “requester” to multiple access requests may result in the requesterbeing identified.EXEMPTIONS/EXCLUSIONS FOR HOSPITAL RECORDS29. Do we have to provide access to all hospital records?Hospitals must provide access to only those records that are in their custody or control. Thegeneral right to access hospital records is limited by the retrospective application provision,such that a person’s right <strong>of</strong> access applies only to records that came into the custody or undercontrol <strong>of</strong> the hospital on or after January 1, 2007.30. Do I have to give the requester the entire record?Not necessarily. Portions <strong>of</strong> the record may be severed prior to disclosing the record. Wheninformation falls within an exemption <strong>and</strong> can reasonably be severed from the record, FIPPAprovides the requester with a right <strong>of</strong> access to the remainder <strong>of</strong> the record.One method <strong>of</strong> severing is to blank out the exempt information from a photocopy <strong>of</strong> the recordusing a black marker, <strong>and</strong> releasing a copy <strong>of</strong> the severed photocopy to the requester.Generally, the smallest unit <strong>of</strong> information to be disclosed after severing is a sentence. But evenwhere only a sentence remains, some information, such as a name, might be removed <strong>and</strong> theremainder released.When information is severed from a record, the notification to the requester must specify thesection(s) <strong>of</strong> the <strong>Act</strong> under which access to the severed information is refused. As well, whereinformation must be severed from a record, it is not feasible to allow a requester the option <strong>of</strong>viewing the original. It is not necessary to disclose “disconnected” snippets <strong>of</strong> information.15
Severing does not apply where the <strong>Act</strong> specifically exempts from disclosure an entire class <strong>of</strong>records such as qualified in-camera meeting records that discuss litigation or drafts <strong>of</strong> by-lawsor resolutions. In all cases, the information in a record must be assessed to determine whetherportions are severable.31. What is the difference between an exemption <strong>and</strong> an exclusion?The primary difference is that excluded records are not subject to the <strong>Act</strong>. As a result, thehospital is not required to process requests for records that fall within section 65 <strong>of</strong> the <strong>Act</strong>.However, the hospital must still respond to the requests, indicate the exclusion claimed <strong>and</strong> thatthe requester has the right to appeal this decision to the IPC. Similarly, the IPC will review thematter to determine if the exclusion has been properly claimed, The IPC reserves the right torequire the production <strong>of</strong> records for which an exclusion has been claimed as part <strong>of</strong> such anappeal. It should also be noted that records that are excluded from the <strong>Act</strong> may still bedisclosed. The exclusion simply means that the records are not available through the formal FOIprocess.By contrast, exempted records are subject to the <strong>Act</strong> <strong>and</strong> must be processed under the <strong>Act</strong> todetermine how <strong>and</strong> to what extent an exemption applies. As a result, the hospital may havegrounds to refuse to disclose information that falls within the description <strong>of</strong> one <strong>of</strong> theexemptions in the <strong>Act</strong>, but nonetheless review the request <strong>and</strong> determine what other informationin the record can “reasonably be severed” <strong>and</strong> disclosed to the requestor. See question #30 forinformation on severing.32. What is the difference between m<strong>and</strong>atory <strong>and</strong> discretionary exemptions?M<strong>and</strong>atory exemptions impose a duty on the head <strong>of</strong> an institution to refuse to disclose arecord. In the case <strong>of</strong> m<strong>and</strong>atory exemptions, the head must determine whether the actualcontents <strong>of</strong> the requested record(s) fall within the exemption. Only two m<strong>and</strong>atory exemptionsmay apply to hospital records: section 17 (third-party proprietary confidential information) <strong>and</strong>section 21 (personal information). All other exemptions are discretionary exemptions. Theypermit the head to disclose a record despite the application <strong>of</strong> the exemption to the requestedrecord. A decision by a head to disclose, or not disclose information falling within an exemptionis an exercise <strong>of</strong> discretion, <strong>and</strong> must be based on appropriate <strong>and</strong> relevant grounds. Anexample <strong>of</strong> a proper exercise <strong>of</strong> discretion occurs when the hospital first determines if anexemption applies, <strong>and</strong> after that considers if there are circumstances which require theinformation to be withheld. Hospitals should only exercise a discretionary exemption wherethere is a compelling reason to do so.16
33. What changes were made to FIPPA to reflect the kinds <strong>of</strong> records kept by hospitals?The BPSAA provided new exemptions <strong>and</strong> exclusions to FIPPA for a broad range <strong>of</strong> hospitalrecords. These include records relating to credentialing, teaching <strong>and</strong> research, provision <strong>of</strong>abortion services, charitable donations, foundations <strong>and</strong> ecclesiastical records. Amendmentswere also made to QCIPA to clarify that FIPPA does not apply to quality <strong>of</strong> care information asdefined under QCIPA. More information on protection for funding <strong>and</strong> planning records <strong>of</strong> ahospital will follow in additional guidance documents including the OHA FIPPA Toolkit <strong>and</strong>related material.34. Are records from employment <strong>and</strong> labour relations negotiations at the hospitalsubject to disclosure under FIPPA?Exclusions set out in subsections 65(6) <strong>and</strong> 65(7) provide that most employment <strong>and</strong> labourrelations records collected, maintained, prepared or used by, or on behalf <strong>of</strong> a hospital areexcluded from FIPPA. Exclusions relevant to the hospital sector include:Proceedings or anticipated proceedings before a court, tribunal, or other entity (relatingto labour relations/ employment <strong>of</strong> a person by the hospital);Negotiations or anticipated negations regarding hospital labour relations/ employment <strong>of</strong>a person;Meetings, consultations, discussions or communications about labour relations/employment-related matters in which the hospital has an interest; <strong>and</strong>Meetings, consultations, discussions or communications about applications for hospitalappointments, the appointments or privileges <strong>of</strong> persons who have hospital privileges,<strong>and</strong> anything that forms part <strong>of</strong> the personnel files <strong>of</strong> those persons.However, subject to an exemption, FIPPA does apply to:An agreement between a hospital <strong>and</strong> a union;An agreement between a hospital <strong>and</strong> at least one employee that concludes a labourrelations/ employment-related proceeding;An agreement between a hospital <strong>and</strong> at least one employee resulting from employmentrelated negotiations; <strong>and</strong>17
An expense account submitted to the hospital by an employee (for expenses incurredduring employment).Unless the person to whom the information relates consents to disclosure, the third-partyinformation exemption must be applied to hospitals’ labour relations/employment records(subsection 17(1)) to exempt the following from disclosure:A record that reveals labour relations information that was supplied in confidence (eitherimplicitly or explicitly) must not be disclosed where disclosure could reasonably beexpected to:ooooSignificantly prejudice the competitive position or interfere significantly withnegotiations;Result in similar information (that is in the public’s interest to be supplied) to nolonger be supplied;Result in undue loss or gain; orReveal information supplied to, or the report <strong>of</strong> a conciliation <strong>of</strong>ficer, mediator,labour relations <strong>of</strong>ficer or other person appointed to resolve a labour relationsdispute.FIPPA AND OTHER ACTS35. What is the relationship between FIPPA <strong>and</strong> PHIPA?FIPPA does not apply to records <strong>of</strong> personal health information in the custody or control <strong>of</strong>health information custodians unless PHIPA provides otherwise. Section 8 <strong>of</strong> PHIPA providesthat only sections 11, 12, 15, 16, 17, 33 <strong>and</strong> 34, subsection 35 (2) <strong>and</strong> sections 3 <strong>and</strong> 44 <strong>of</strong>FIPPA apply to personal health information held by the health information custodian (i.e.hospital).Personal health information is defined in PHIPA as identifying information about an individual inoral or recorded form, if the information, (a) relates to the physical or mental health <strong>of</strong> theindividual, including information that consists <strong>of</strong> the health history <strong>of</strong> the individual’s family, (b)relates to the provision <strong>of</strong> health care to the individual, including the identification <strong>of</strong> a person asa provider <strong>of</strong> health care to the individual, (c) is a plan <strong>of</strong> service within the meaning <strong>of</strong> theHome Care <strong>and</strong> Community Services <strong>Act</strong>, 1994 for the individual, (d) relates to payments or18
eligibility for health care, or eligibility for coverage for health care, in respect <strong>of</strong> the individual, (e)relates to the donation by the individual <strong>of</strong> any body part or bodily substance <strong>of</strong> the individual oris derived from the testing or examination <strong>of</strong> any such body part or bodily substance, (f) is theindividual’s health number, or (g) identifies an individual’s substitute decision-maker. PHIPAdoes not limit the right <strong>of</strong> access to the records if personal health information is reasonablysevered from the document(s).Therefore, the public does not have a right <strong>of</strong> access under FIPPA to records <strong>of</strong> personal healthinformation under the custody or control <strong>of</strong> a hospital. However, if a hospital record containsboth personal health information <strong>and</strong> non-personal, administrative information, the latterremains subject to FIPPA (<strong>and</strong> access requests), if the former can be “reasonably severed” fromthe record.36. How does the amendment to QCIPA protect all quality <strong>of</strong> care information fromdisclosure?The amendment to QCIPA does not necessarily protect all quality <strong>of</strong> care information fromdisclosure. As a result <strong>of</strong> the amendment to QCIPA, FIPPA does not apply to quality <strong>of</strong> careinformation prepared by or for a designated quality <strong>of</strong> care committee under QCIPA. Section 1<strong>of</strong> QCIPA defines “quality <strong>of</strong> care information” as information that: (a) is collected by or preparedfor a quality <strong>of</strong> care committee for the sole or primary purpose <strong>of</strong> assisting the committee incarrying out its functions, or (b) relates solely or primarily to any activity that a quality <strong>of</strong> carecommittee carries on as part <strong>of</strong> its functions. As such, this exclusion from FIPPA does notextend to quality <strong>of</strong> care information <strong>and</strong> records generated outside <strong>of</strong> QCIPA, such as rootcause analysis, failure mode <strong>and</strong> effects analysis, self-assessment activities or chart reviews.Note: Section 2 <strong>of</strong> QCIPA provides that QCIPA <strong>and</strong> its regulations prevail (over any other act orits regulations) unless otherwise specifically provided.37. How do we deal with a request that is made jointly under PHIPA <strong>and</strong> FIPPA?All information that can be disclosed under PHIPA should be disclosed under that <strong>Act</strong>. A requestfor an individual’s own health information (or about an individual for whom the requester isacting as a substitute decision maker) can only be made under PHIPA. There are some limitedexemptions under PHIPA that may prevent all requested records from being disclosed. Thehospital should decide whether or not to deal with the outst<strong>and</strong>ing records via a FIPPA request.Before this is done the hospital should explain to the requester that some <strong>of</strong> the records fallunder FIPPA, not PHIPA, <strong>and</strong> therefore an access request for those records must be madeunder FIPPA. The requester must also be made aware <strong>of</strong> the fee that comes with requests foraccess to records under the <strong>Act</strong>.19
Exceptions to the exemptions should be considered for every request regardless <strong>of</strong> what act therequest falls under.38. Does access to a record fall under FIPPA or PHIPA after personal health informationhas been deleted from a record?After personal health information has been deleted from the record, the rest <strong>of</strong> the record issubject to FIPPA - unless a FIPPA exclusion applies to it.DISCLOSURE39. How can we protect personal health information received for the purpose <strong>of</strong> aninvestigation from disclosure?It is necessary to consider who is asking for the information. If the patient is making the requestfor their own personal health information, then this falls under PHIPA. However, subsection52(1)(d) <strong>of</strong> PHIPA exempts records related to an ongoing investigation. Specifically, anindividual does not have a right <strong>of</strong> access to a record <strong>of</strong> personal health information where:i. The information was collected or created in the course <strong>of</strong> an inspection,investigation or similar procedure authorized by law… <strong>and</strong>ii. The inspection, investigation … has not been concluded.When the media is asking for a record containing personal health information, the record maybe subject to FIPPA, if all health information is removed <strong>and</strong> the patient cannot be identified (forexample, treatment methods). The hospital can then consider if the remaining information fallsunder an exemption. For example, subsection 14(1)(b) <strong>of</strong> FIPPA permits a head to refuse todisclose a record where the disclosure could reasonably be expected to “interfere with aninvestigation undertaken with a view to a law enforcement proceeding or from which a lawenforcement proceeding is likely to result.” Note: A record that may identify an individual despiteall personal health information having been removed is dealt with under FIPPA.RECORD RETENTION40. Can hospitals dispose <strong>of</strong> any existing records?Records must be kept for the prescribed period as set out in relevant statutes. For furtherinformation on how long specific types <strong>of</strong> records need to be kept see the OHA RecordsRetention Toolkit: A Guide to Maintenance <strong>and</strong> Disposal <strong>of</strong> Hospital Records (2006). This guideassists members in underst<strong>and</strong>ing the legal retention periods for hospital records. The20
implementation <strong>of</strong> FIPPA within the hospital sector provides an excellent opportunity forhospitals to consider when reviewing records, the length <strong>of</strong> time a specific record must be keptin order to abide by legislative requirements.The head must authorize the destruction <strong>of</strong> all hospital records that contain personalinformation. Reasonable steps must be taken to ensure that records containing personalinformation are destroyed in such a way that it cannot be reconstructed or retrieved. Alldisposed records are to be recorded on a “disposal record.” The disposal record documentswhat personal information was disposed, the date <strong>of</strong> disposal, <strong>and</strong> the manner by which therecords were disposed.This process is not to be confused with subsection 13(1) <strong>of</strong> PHIPA which requires a healthinformation custodian to dispose <strong>of</strong> personal health information in a secure manner inaccordance with the prescribed requirements (if any) as set out in the <strong>Act</strong>.41. Are backup files <strong>of</strong> deleted emails subject to disclosure?This issue has not yet been definitively decided. This may depend on whether the deletedemails have been retained by the institution on backup tapes <strong>and</strong> how difficult the retrievalprocess would be. Generally speaking, if providing access to requested information is so difficultthat it interferes with the operations <strong>of</strong> an institution, then the requested document is notconsidered to be a record under the <strong>Act</strong>.42. Will OHA be updating its Records Retention Toolkit?As FIPPA has not changed the legal retention periods for hospital records, an update at thispoint is not needed. As part <strong>of</strong> the OHA’s strategy to support the implementation <strong>of</strong> FIPPA inhospitals, a practical toolkit to implementing FOI will be developed. This toolkit will provide abrief summary <strong>of</strong> the retention periods <strong>of</strong> some common hospital documents. In the interim, it isrecommended that hospitals review the OHA Records Retention Toolkit: A Guide toMaintenance <strong>and</strong> Disposal <strong>of</strong> Hospital Records (2006) for a more thorough examination <strong>of</strong>document retention requirements.GETTING READY FOR IMPLEMENTATION43. Is each hospital required to have a dedicated staff person or <strong>of</strong>fice to deal withFIPPA?The person ultimately accountable for meeting a wide range <strong>of</strong> duties under FIPPA is called the“head” – a position assigned under FIPPA to chairs <strong>of</strong> boards for public hospitals. However, this21
duty may be delegated to one or more other individuals – usually a senior manager. The duties<strong>of</strong> the head may be undertaken by exp<strong>and</strong>ing the duties <strong>of</strong> an existing <strong>of</strong>fice – e.g. the Chief<strong>Privacy</strong> Officer or PHIPA Coordinator. Or, if appropriate, hospitals may delegate privacy-related<strong>and</strong> access-related duties to two separate <strong>of</strong>fices. Alternatively hospitals may consider sharingresources <strong>and</strong> delegating responsibilities for a joint <strong>of</strong>fice. Additional information on variousmodels or structures will be provided in the OHA FOI Toolkit.44. What policies or practices should hospitals be putting in place now?Although the <strong>Act</strong> does not apply to hospitals until January 2012, there are a number <strong>of</strong> practicalimplementation issues that you will need to consider in the year ahead. These include suchthings as identifying needed resources, reviewing records management <strong>and</strong> privacy policies,establishing issues management protocols, <strong>and</strong> developing new access procedures, to name afew.45. How should we respond to FOI requests before the implementation date <strong>of</strong> January 1,2012?As the <strong>Act</strong> does not yet apply to hospitals, you are not required to respond to requests forinformation. Nonetheless, hospitals are always encouraged to make publicly available generalcorporate information (e.g., accountability agreements, annual reports, board agendas, etc.).This is consistent with the need to be transparent <strong>and</strong> accountable to the community <strong>and</strong> mayalso ultimately reduce the time <strong>and</strong> expense <strong>of</strong> responding to individual access requests. Withrespect to other information (i.e. that is not routinely made publicly available), to avert potentialdisclosure <strong>of</strong> information that is not permitted to be released pursuant to the <strong>Act</strong> it isrecommended that hospitals not process requests before January 2012 unless the keyobligations <strong>of</strong> FIPPA are well understood <strong>and</strong> hospital policies <strong>and</strong> procedures are aligned withthe requirements <strong>of</strong> the <strong>Act</strong>.46. Is there any way to anticipate the magnitude <strong>of</strong> requests for access to records?Access requests will be the source <strong>of</strong> the greatest dem<strong>and</strong> on resources in connection withFIPPA. Unfortunately, there is no way to anticipate the number <strong>of</strong> requests for access torecords. Experiences in other sectors suggest that volume depends on a variety <strong>of</strong> factors,notably the level <strong>of</strong> media interest <strong>and</strong> community advocacy.Likely sources <strong>of</strong> requests include: media (minutes, proposals), politicians (minutes, proposals,plans), patients (complaints about members <strong>of</strong> pr<strong>of</strong>essional staff), members <strong>of</strong> pr<strong>of</strong>essional staff<strong>and</strong> ex-employees (their information <strong>and</strong> that <strong>of</strong> other staff members), advocacy groups(minutes), unions (minutes, employee information), <strong>and</strong> vendors.22
It is important to create a contingency plan in case the volume <strong>of</strong> requests exceedsexpectations/ available resources.As indicated earlier, hospitals are encouraged to consider the proactive disclosure <strong>of</strong>information to the public on a routine basis to minimize the volume <strong>of</strong> requests.AVAILABLE RESOURCES/EDUCATION47. What will the OHA be providing by way <strong>of</strong> guidance <strong>and</strong>/or tools <strong>and</strong> templates?To ensure that any new administrative <strong>and</strong> cost burdens are minimized, the OHA is currentlydeveloping a comprehensive <strong>and</strong> effective implementation strategy. The OHA is working withgovernment <strong>and</strong> the IPC to create <strong>and</strong> build on existing FOI resources. In the coming months,the OHA will be developing an FOI toolkit tailored to the needs <strong>of</strong> hospitals, as well as anextensive number <strong>of</strong> educational opportunities. An OHA FOI Implementation Advisory Groupwith representatives from hospitals <strong>of</strong> varying types <strong>and</strong> sizes has been established to oversee<strong>and</strong> provide guidance on this work.48. What educational supports can I expect to receive?The OHA will be providing regional training workshops to assist FOI leads in hospitals;developing on-line modules for in-house training on specific issues; <strong>and</strong> hosting a series <strong>of</strong>webcasts <strong>and</strong> conferences. These resources will be tailored to the varying needs <strong>of</strong> all thoseinvolved in developing <strong>and</strong> overseeing FIPPA implementation - FIPPA leads, senior staff,CEOs <strong>and</strong> Boards. The educational tools <strong>and</strong> events are currently being developed <strong>and</strong> willbegin within the next four to six months. Additional details respecting these educational eventswill be provided in the short time ahead.49. Where can I go to get more information?As noted above, over the next few months the OHA will be producing an FOI toolkit formembers. Hospitals wishing to gain additional background information on FIPPA in the shorttime ahead are encouraged to consult the IPC’s website, as well as the Ministry <strong>of</strong> GovernmentServices general guidance manual.For additional information on FIPPA, please contact Alissa Raphael, Legislative Advisor ataraphael@oha.com or 416-205-1356, or Elizabeth Carlton, Director, Policy <strong>and</strong>Legislative/Legal Affairs at ecarlton@oha.com or 416-205-1429. For information respectingupcoming FIPPA educational <strong>of</strong>ferings, contact Sara Simone at ssimone@oha.com or 416-205-1463.23