Empanelment of Dental Clinic - ECHS
Empanelment of Dental Clinic - ECHS
Empanelment of Dental Clinic - ECHS
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
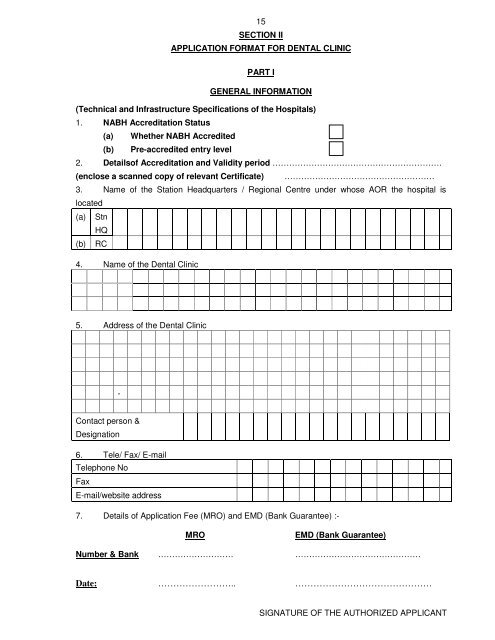
15SECTION IIAPPLICATION FORMAT FOR DENTAL CLINICPART IGENERAL INFORMATION(Technical and Infrastructure Specifications <strong>of</strong> the Hospitals)1. NABH Accreditation Status(a) Whether NABH Accredited(b) Pre-accredited entry level2. Details<strong>of</strong> Accreditation and Validity period …………………………………………………….(enclose a scanned copy <strong>of</strong> relevant Certificate) ………………………………………………3. Name <strong>of</strong> the Station Headquarters / Regional Centre under whose AOR the hospital islocated(a) StnHQ(b) RC4. Name <strong>of</strong> the <strong>Dental</strong> <strong>Clinic</strong>5. Address <strong>of</strong> the <strong>Dental</strong> <strong>Clinic</strong>-Contact person &Designation6. Tele/ Fax/ E-mailTelephone NoFaxE-mail/website address7. Details <strong>of</strong> Application Fee (MRO) and EMD (Bank Guarantee) :-MROEMD (Bank Guarantee)Number & Bank ……………………… ………………………………………Date: …………………….. ………………………………………SIGNATURE OF THE AUTHORIZED APPLICANT