LCP Medial Proximal Tibial Plate 4.5/5.0
LCP Medial Proximal Tibial Plate 4.5/5.0
LCP Medial Proximal Tibial Plate 4.5/5.0

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
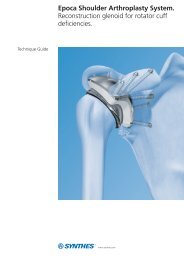
Technique Guide<strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong><strong>4.5</strong>/<strong>5.0</strong>. Part of the Synthes <strong>LCP</strong>periarticular plating system.
Table of ContentsIntroduction<strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> 2AO Principles 4Indications 5Surgical Technique 6Product InformationInstruments for Minimally Invasive Osteosynthesis 22<strong>Plate</strong>s 23Screws 24Drill and Wire Guides 26Sets 27Image intensifier controlWarningThis description is not sufficient for immediate application ofthe instrumentation. Instruction by a surgeon experienced inhandling this instrumentation is highly recommended.Synthes 1
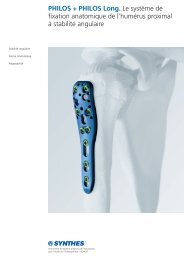
<strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong><strong>4.5</strong>/<strong>5.0</strong>. Part of the Synthes <strong>LCP</strong>periarticular plating system.The <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> is part of theSynthes <strong>LCP</strong> periarticular plating system, which merges lockingscrew technology with conventional plating techniques.<strong>LCP</strong> Periarticular Plating SystemThe <strong>LCP</strong> periarticular plating system is capable of addressing:– complex fractures of the proximal tibia with the <strong>LCP</strong> <strong>Proximal</strong><strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> or the <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong><strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong>.– complex fractures of the distal femur with the <strong>LCP</strong> Condylar<strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong>.– complex fractures of the proximal femur with the <strong>LCP</strong><strong>Proximal</strong> Femoral <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> or the <strong>LCP</strong> <strong>Proximal</strong> FemoralHook <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong>.Locking Compression <strong>Plate</strong>The Locking Compression <strong>Plate</strong> (<strong>LCP</strong>) has combi-holes in theplate shaft that combine a dynamic compression unit (DCU)hole with a locking screw hole. The combi-hole provides theflexibility of axial compression and locking capabilitythroughout the length of the plate shaft.Note: More detailed information on conventional and lockedplating principles can be found in the Synthes Locking Compression<strong>Plate</strong> (<strong>LCP</strong>) Technique Guide (Art. No. 036.000.019).2 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
<strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong>The <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> is available instainless steel and titanium and has a limited-contact shaftprofile. The head and neck portions of the plate accept <strong>5.0</strong>mm cannulated locking screws and <strong>5.0</strong> mm cannulated conicalscrews. The screw hole pattern allows a raft of subchondrallocking screws to buttress and maintain reduction of thearticular surface. This provides fixed-angle support to thetibial plateau.<strong>Plate</strong> head– Anatomically contoured to approximate the anteromedialproximal tibia.– Three convergent threaded screw holes accept cannulatedlocking screws <strong>5.0</strong> mm or cannulated conical screws <strong>5.0</strong> mm.– Two 2.0 mm holes for preliminary fixation with Kirschnerwires, or meniscal repair with sutures.<strong>Plate</strong> shaft– The two angled locking holes distal to the plate headaccept cannulated locking screws <strong>5.0</strong> mm or cannulatedconical screws <strong>5.0</strong> mm to secure the plate position. Thehole angles allow the locking screws to converge with twoof the three screws in the plate head.– Combi-holes, distal to the angled locking holes, combine aDCU hole with a threaded locking hole. The combi-holesaccept locking screws <strong>5.0</strong> mm in the threaded portionof the hole and cortex screws <strong>4.5</strong> mm in the DCU portionof the hole.– Available with 4, 6, 8, 10, 12, 14, or 16 combi-holes in theplate shaft.– Limited-contact profile.Two 2.0 mm holes for Kirschner wires and suturesThree locking screw holesaccept cannulated lockingscrews <strong>5.0</strong> mm orcannulated conical screws <strong>5.0</strong> mm.Angled locking holes acceptcannulated locking screws <strong>5.0</strong> mm or cannulatedconical screws <strong>5.0</strong> mmand support the proximalscrewsCombi-holes combine aDCU hole with a threadedlocking holeFor articulatedtension deviceAvailable in left and right platesSynthes 3
AO PrinciplesIn 1958, the AO formulated four basic principles which havebecome the guidelines for internal fixation. 1 Those principles,as applied to the <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong>,are:Anatomic reductionFacilitates restoration of the articular surface by exact screwplacement using guide wires for reduction and insertion ofcannulated screws.Stable fixationLocking screws create a fixed-angle construct, providingangular stability.Preservation of blood supplyTapered end simplifies submuscular plate insertion. Limitedcontactshaft profile reduces plate-to-bone contact and vasculartrauma.Early, active mobilization<strong>Plate</strong> features combined with AO technique create an environmentfor bone healing, expediting a return to optimalfunction.1M.E. Müller, M. Allgöwer, R. Schneider, and H. Willenegger (1991) AO Manual ofInternal Fixation, 3rd Edition. Berlin: Springer.4 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
IndicationsThe <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong>s <strong>4.5</strong>/<strong>5.0</strong> are intended tobuttress metaphyseal fractures of the medial tibial plateau,split-type fractures of the medial tibial plateau, medial splitfractures with associated depressions and split or depressionfractures of the medial tibial plateau. The plates may also beused for fixation of the proximal quarter (lateral and medial)of the tibia, as well as segmental fractures of the proximaltibia.The <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong>s <strong>4.5</strong>/<strong>5.0</strong> may also beused for fixation of nonunions and malunions of the medialproximal tibia and tibia shaft, as well as opening and closingwedge tibial osteotomies.Synthes 5
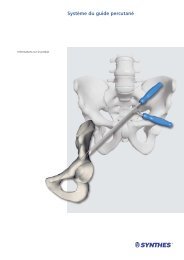
Surgical Technique1Preparation and preoperative planning Required sets<strong>Plate</strong> Set <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong>s <strong>4.5</strong>/<strong>5.0</strong>Periarticular <strong>LCP</strong> Plating System Instrument SetCannulated Conical and Cannulated Locking Screw Set <strong>5.0</strong> and 7.3 mm<strong>LCP</strong> Large Fragment Instrument Set 1 <strong>LCP</strong> Large Fragment Screw SetComplete the preoperative radiographic assessment andprepare the preoperative plan. Determine plate length andinstruments to be used.X-ray template for right <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong>s<strong>4.5</strong>/<strong>5.0</strong> (Art. No. 034.000.497) Important: Determine proximal screw placement and screwlengths to ensure proper screw placement in the metaphysis.Position the patient supine on a radiolucent operating table.Visualization of the proximal tibia under fluoroscopy in boththe lateral and AP views is necessary. 1 60 X-ray template for left <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong>s<strong>4.5</strong>/<strong>5.0</strong> (Art. No. 034.000.500)6 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
2Reduce articular surfaceOptional instruments117.700 Instrument Set for Large Distractor inSterilization Tray01.301.000 Large External Fixator in Vario Case394.350 Large DistractorTechnique Tip: Prior to reduction, application of an externalfixator or large distractor may facilitate visualization and reductionof the joint.Reduce the fracture fragments and confirm reduction usingimage intensification. Fragments may be reduced using independentKirschner wires; however, Kirschner wire holes arealso provided on the plate to help achieve provisional reduction,plate position, or fixation.The locking screws do not provide interfragmentary or plateto-bonecompression; therefore, any desired compressionmust be achieved with traditional lag screws or cannulatedconical screws <strong>5.0</strong> mm. The articular fragments must bereduced and compression must be obtained prior to applyingthe <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> with locking screws.Technique Tip: To verify that independent lag screws willnot interfere with plate placement, hold the plate to thebone.Apply the distractor to assist in the visualization andreduction of the joint.Synthes 7
Surgical Technique3Determine plate positionUsing anatomic landmarks and fluoroscopy, mount the plateon the intact or reconstructed plateau without attempting toreduce the distal portion of the fracture.8 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
Mount the plateInstruments324.174 Wire Guide <strong>5.0</strong>, for Guide Wire 2.5 mm292.210 Kirschner Wire 2.0 mm with trocar tipAttach a wire guide to the central hole in the head of theplate. Insert a Kirschner wire 2.0 mm through a Kirschnerwire hole.Readjust the plate position, if necessary. Place a second wirein the other Kirschner wire hole to prevent rotation of theplate and to secure provisional fixation of the plate to thetibial plateau.Synthes 9
Surgical Technique4Insert proximal provisional (conical) screwInstruments310.243 Guide Wire 2.5 mm, with drill tip319.701 Measuring Device for Cannulated LockingScrews and Cannulated Conical Screws <strong>5.0</strong> and 7.3 mmFor predrilling in dense bone310.634 Drill Bit 4.3 mm, cannulated, withQuick CouplingInsert guide wireWhile the plate is placed against the bone, insert the guidewire 2.5 mm through the wire guide in the central screwhole in the plate head. It is imperative to drill using fluoroscopyto ensure proper screw trajectory and screw placement.Advance the guide wire through to the lateral cortexor to the desired screw tip location.Determine proper screw trajectory by using clinical examinationand fluoroscopy to confirm:– Guide wire trajectory in the proximal locking hole is parallelto the joint and the reduction is maintained.– The screw and plate placement will be consistent with thepreoperative plan.– Alignment of the plate to the shaft of the tibia is correct inboth the AP and lateral views. Placement of the plate atthis point will determine final flexion/extension.Measure screw lengthMeasure for screw length using the measuring device forcannulated screws.Note: The measuring device must contact the end of thewire guide for an accurate measurement.Predrilling in dense boneThe self-drilling, self-tapping flutes of the cannulated conicalscrews <strong>5.0</strong> mm make predrilling and pretapping unnecessaryin most cases. If necessary, in dense bone, the lateralcortex can be predrilled with the cannulated drill bit 4.3 mm.10 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
Insert proximal cannulated (conical) screwInstruments314.050 Screwdriver, hexagonal, cannulated338.490 Quick Coupling314.230 Screwdriver Shaft, hexagonal, cannulatedUse the cannulated hexagonal screwdriver to remove thewire guide.Insert the appropriate length cannulated conical screw <strong>5.0</strong> mm in the central hole in the plate head to pull theplate to the bone and gain interfragmentary compressionthrough the plate by using a power tool with the quick couplingand the cannulated screwdriver shaft.Perform final tightening by hand using the hexagonal cannulatedscrewdriver.Notes– Insert a screw that is approximately 5 mm shorter than themeasurement from the measuring device.– When interfragmentary compression is desired, usecannulated conical screws <strong>5.0</strong> mm. Locking screws arenot lag screws.Synthes 11
Surgical Technique5Secure plate to plateauInstruments324.174 Wire Guide <strong>5.0</strong>, for Guide Wire 2.5 mm310.243 Guide Wire 2.5 mm, with drill tip319.701 Measuring Device for Cannulated LockingScrews and Cannulated Conical Screws <strong>5.0</strong> and 7.3 mm314.050 Screwdriver, hexagonal, cannulatedAttach wire guides to the anterior and posterior holes in thehead of the plate. Insert guide wires 2.5 mm throughthese wire guides to the desired screw tip location.Use the measuring device to measure for screw length. Usethe hexagonal cannulated screwdriver to remove the wireguides.Remove the Kirschner wires.12 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
Insert cannulated locking screwsInstruments511.771 Torque Limiter, 4 Nm or511.774 Torque Limiter, 4 Nm, for AO/ASIF QuickCoupling for Reamers338.490 Quick Coupling314.230 Screwdriver Shaft, hexagonal, cannulatedFor final tightening and locking397.705 Handle for Torque Limiter Nos. 511.770and 511.771 or397.706 Handle for Torque Limiter No. 511.774For predrilling in dense bone310.634 Drill Bit 4.3 mm, cannulated, withQuick CouplingInsert the appropriate length cannulated locking screws <strong>5.0</strong> mm into the bone with a power tool using the torquelimiter, the quick coupling and the hexagonal cannulatedscrewdriver shaft.Perform final tightening by hand using the hexagonal cannulatedscrewdriver shaft together with the quick coupling, thetorque limiter and the handle for torque limiter. After oneclick, the optimum torque is reached.Warning: If the torque limiter is unavailable, do not tightenthe screws to the plate using a power tool. Perform finaltightening by hand.Predrilling in dense boneThe self-drilling, self-tapping flutes of the cannulated lockingscrews <strong>5.0</strong> mm make predrilling and pretapping unnecessaryin most cases. If necessary, in dense bone, the lateralcortex can be predrilled with the cannulated drill bit 4.3 mm.Once both the anterior and posterior locking screws are securelylocked to the plate, the central cannulated conicalscrew <strong>5.0</strong> mm may be removed and replaced with a thirdcannulated locking screw <strong>5.0</strong> mm.Synthes 13
Surgical Technique6Reduce shaft to tibial plateauInstruments398.810 Bone Holding Forceps, self-centering,speed lock or398.813 <strong>Plate</strong> Holding Forceps, with Swivel Foot321.120 Tension Device, articulatedReduce the tibial plateau to the shaft of the tibia, usingindirect reduction techniques whenever possible. Usingatraumatic technique, secure the plate to the tibial shaft withbone holding forceps.Confirm rotational alignment of the extremity by clinicalexamination.Once reduction is satisfactory, and if it is appropriate basedon the fracture morphology, the plate should be loaded intension using the tension device.Note: With multifragmentary fractures, it may not always bepossible or desirable to achieve anatomic reduction of thefracture. However, in simple fracture patterns, the tensiondevice may facilitate anatomic reduction. This device may beused to generate either compression or distraction.14 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
7Insert screws in plate shaft1 2 2 1In addition to having threaded locking holes, the plate functionssimilarly to DCP plates which offer the ability to axiallycompress fracture fragments. Therefore, a combination ofcortex screws and locking screws may be used.CorrectImportant: If a combination of cortex (1) and locking screws(2) is used, a cortex screw should be inserted first to pull theplate to the bone.2 1 1 2Note: If locking screws (1) have been used to fix the plate toa fragment, subsequent insertion of a cortex screw (2) in thesame fragment without loosening and retightening thelocking screw is not recommended.IncorrectSynthes 15
Surgical Technique7aInsert cortex screwsInstruments323.460 Universal Drill Guide <strong>4.5</strong>/3.2310.290 Drill Bit 3.2 mm, 2-flute, forQuick Coupling319.100 Depth Gauge for Screws <strong>4.5</strong> to 6.5 mm03.400.102 Screwdriver Shaft 3.5, hexagonal,Stardrive T2503.400.112 Handle for Screwdriver Shaft 3.5,hexagonal, Stardrive T25Insert as many self-tapping cortex screws <strong>4.5</strong> mm asnecessary into the distal portion of the plate.Important: All of the cortex screws <strong>4.5</strong> mm must beinserted prior to insertion of locking screws <strong>5.0</strong> mm.Use the universal drill guide to predrill for the cortex screwsand drill through both cortices with the drill bit 3.2 mm.For the neutral position, press the drill guide down in thenonthreaded hole. To obtain compression, place the drillguide at the end of the nonthreaded hole away from thefracture. Do not apply downward pressure on the drillguide’s spring-loaded tip.Measure for screw length using the depth gauge.Select and insert the appropriate length cortex screw <strong>4.5</strong>mm. Perform final tightening by hand using the screwdrivershaft together with the handle for the screwdriver shaft.16 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
7bInsert locking screwsInstruments323.042 <strong>LCP</strong> Drill Sleeve <strong>5.0</strong>, for Drill Bits 4.3 mm310.430 <strong>LCP</strong> Drill Bit 4.3 mm with Stop319.100 Depth Gauge for Screws <strong>4.5</strong> to 6.5 mm314.119 Screwdriver Shaft Stardrive <strong>4.5</strong>/<strong>5.0</strong>, T25 or314.150 Screwdriver Shaft, hexagonal, 3.5 mm511.771 Torque Limiter, 4 Nm or511.774 Torque Limiter, 4 Nm, for AO/ASIFQuick Coupling for ReamersFor final tightening and locking397.705 Handle for Torque Limiter Nos. 511.770and 511.771 or397.706 Handle for Torque Limiter No. 511.774Attach the <strong>LCP</strong> drill sleeve to the locking hole in the plateshaft. Drill a hole using the <strong>LCP</strong> drill bit 4.3 mm.Note: Use of the drill sleeve is mandatory for screws to lockto the plate properly.Synthes 17
Surgical TechniqueRemove the drill sleeve and determine the screw length withthe depth gauge. Alternatively, read the drilled depth directlyfrom the laser mark on the drill bit by shoving the stop ringdown to the drill sleeve to make reading easier.Insert the appropriate length locking screw <strong>5.0</strong> mm byusing a power tool with the torque limiter and the screwdrivershaft.Perform final tightening by hand using the screwdriver shafttogether with the torque limiter and the handle for torquelimiter. After one click, the optimum torque is reached.Repeat as necessary to insert additional locking screws.Warning: If the torque limiter is unavailable, do not tightenthe screws to the plate using power. Perform final tighteningby hand.Examine the limb clinically and radiographically. It is importantthat the tibial plateau is in proper orientation to thetibial shaft.Important: Securely tighten all locking screws again.18 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
8Insert cannulated locking screws in angled holesInstruments324.174 Wire Guide <strong>5.0</strong>, for Guide Wire 2.5 mm310.243 Guide Wire 2.5 mm, with drill tip319.701 Measuring Device for Cannulated LockingScrews and Cannulated Conical Screws <strong>5.0</strong> and 7.3 mm314.050 Screwdriver, hexagonal, cannulated511.771 Torque Limiter, 4 Nm or511.774 Torque Limiter, 4 Nm, for AO/ASIF QuickCoupling for Reamers338.490 Quick Coupling314.230 Screwdriver Shaft, hexagonal, cannulatedNote: Use the oblique locking positions to buttress a medialfragment.If not already done, thread a wire guide into an angledlocking hole. Insert a guide wire 2.5 mm through the wireguide. Advance the guide wire until it reaches the desiredscrew tip location.Measure for screw length using the measuring device. Thecorrect length measurement will place the screw tip at thetip of the guide wire. Use the hexagonal, cannulated screwdriverto remove the wire guide.Note: The measuring device must contact the end of thewire guide for an accurate measurement.For final tightening and locking397.705 Handle for Torque Limiter Nos. 511.770and 511.771 or397.706 Handle for Torque Limiter No. 511.774For predrilling in dense bone310.634 Drill Bit 4.3 mm, cannulated, withQuick CouplingSynthes 19
Surgical TechniqueInsert the appropriate length cannulated locking screws <strong>5.0</strong> mm by using a power tool with the torque limiter,quick coupling and the hexagonal, cannulated screwdrivershaft.Perform final tightening by hand using the hexagonal cannulatedscrewdriver shaft together with the quick coupling, thetorque limiter and the handle for torque limiter. After oneclick, the optimum torque is reached.Repeat steps for locking screw insertion for the remainingangled hole.Warning: If the torque limiter is unavailable, do not tightenthe screws to the plate using power. Perform final tighteningby handPredrilling in dense boneThe self-drilling, self-tapping flutes of the cannulated lockingscrews <strong>5.0</strong> mm make predrilling and pretapping unnecessaryin most cases. If necessary, in dense bone, the lateralcortex can be predrilled with the cannulated drill bit 4.3 mm.20 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
Screw length considerationsWhen using the appropriate length screws in the angledlocking holes, the screw tips should meet the proximallocking screws.70 mm65 mm65 mmSuggested screw lengths to achieve desired screw convergenceNote: Securely tighten all locking screws to lock them to theplate.Synthes 21
Instruments for Minimally InvasiveOsteosynthesisHohmann Retractor HolderThe Hohmann retractor holder was developed to supportminimally invasive, percutaneous plate osteosynthesis. Itsunique design enables the easy and reliable percutaneous insertionof plates. These characteristics make the Hohmannretractor holder the ideal instrument for use in combinationwith modern implant systems such as <strong>LCP</strong> and LISS.− The Hohmann retractor holder allows better visualizationof the inserted plate.− Serves as a guide for the inserted plate.− Ensures that the inserted plate is centered on the bone.For additional information see the separate Synthespublication on the Hohmann retractor holder(Art. No. 036.000.219).Soft Tissue RetractorThe offset blade facilitates an easy preparation of theepipereosteal cavity for percutaneous plate insertion.− Adjustable blade for free choice of insertion angle andblade length− Available in two sizes: for small and large fragment platesFor additional information see the separate Synthes publicationon the Soft tissue retractor (Art. No. 036.000.127).22 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
<strong>Plate</strong>s<strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong>s <strong>4.5</strong>/<strong>5.0</strong>Steel Titanium Holes (shaft) Length (mm)239.984 439.984 4 106 right239.986 439.986 6 142 right239.988 439.988 8 178 right239.990 439.990 10 214 right239.992 439.992 12 250 right239.994 439.994 14 286 right239.996 439.996 16 322 right239.985 439.985 4 106 left239.987 439.987 6 142 left239.989 439.989 8 178 left239.991 439.991 10 214 left239.993 439.993 12 250 left239.995 439.995 14 286 left239.997 439.997 16 322 leftAll plates are available nonsterile and sterile packed. For sterile implants addsuffix S to article number.Synthes 23
ScrewsCannulated Locking Screw <strong>5.0</strong> mm(0X.20<strong>5.0</strong>25 – 0X.205.145)Creates a locked, fixed-angle screw-plate construct– Threaded conical head– Fully threaded shaft– Self-drilling, self-tapping tipCannulated Conical Screw <strong>5.0</strong> mm(0X.205.240 – 0X.205.295)Compresses the plate to the lateral femoral condyle andprovides interfragmentary compression– Smooth conical head– Partially threaded shaft– Self-drilling, self-tapping tipScrew Nut <strong>5.0</strong> mm (X22.578)Offers additional fixation and compression options forcomplex fractures– Self-cutting, serrated tip– Inserted from the lateral aspect of the proximal tibia– Internal threads mate with the <strong>5.0</strong> mm cannulated conicalscrewsSee the <strong>LCP</strong> Condylar <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide (Art.No. 036.000.727) for more information on use of the screwnut.Locking Screw <strong>5.0</strong> mm( X13.314 – X13.390 / X12.201–X12.227)Creates a locked, fixed-angle screw-plate construct– Threaded conical head– Fully threaded shaft– Self-tapping tipCortex Screw <strong>4.5</strong> mm (X14.814 – X14.940)– May be used in the DCU portion of the combi-holes in theplate shaft– Compresses the plate to the bone or creates axialcompression– Self-tapping tipX = 2: Stainless steelX = 4: Titanium and titanium alloy (TAN)24 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
Cannulated Locking and Cannulated Conical Screws <strong>5.0</strong> mmThe screw design enhances fixation and facilitates thesurgical procedure.Screw headThe conical head simplifies alignment in the plate hole. Thisis of particular importance when using locking screws. Thethreaded screw head must align with the plate hole threadsto provide a secure screw-plate construct. To ensure properalignment and prevent cross-threading, the appropriatethreaded wire guide or drill guide must always be used.Large diameter screw coreThe large diameter screw core improves bending and shearstrength, and distributes the load over a larger area in thebone.Thread profileThe shallow thread profile of the locking screws is necessaryto provide a larger core. This is appropriate since lockingscrews do not rely on compression between the plate andthe bone to maintain stability. When required, interfragmentarycompression can be achieved with the partially threadedcannulated conical screws, especially when near the articularsurface.Synthes 25
Drill and Wire Guides324.174 Wire Guide <strong>5.0</strong>, for Guide Wire 2.5 mmFits the screw holes in the plate head323.042 <strong>LCP</strong> Drill Sleeve <strong>5.0</strong>, for Drill Bits 4.3 mmFits the threaded part of the combi-holesin the plate shaft323.460 Universal Drill Guide <strong>4.5</strong>/3.2Fits the nonthreaded part of the combiholesin the plate shaft26 Synthes <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong> <strong>4.5</strong>/<strong>5.0</strong> Technique Guide
Sets<strong>Plate</strong> Set <strong>LCP</strong> <strong>Medial</strong> <strong>Proximal</strong> <strong>Tibial</strong> <strong>Plate</strong>s <strong>4.5</strong>/<strong>5.0</strong> inVario Case01.120.430 Stainless steel01.120.431 Titanium689.508 Vario Case68.120.430 Insert689.507 Lid01.120.021 Periarticular <strong>LCP</strong> PlatingSystem Instrument Set in Vario Case68.120.447 Vario Case68.120.445 Insert689.507 LidCannulated Conical and Cannulated Locking Screws <strong>5.0</strong> and 7.3 mm in Sterilization Tray01.120.022 Stainless steel01.120.445 Titanium68.120.450 Sterilization TrayAdditionally required01.120.457 <strong>LCP</strong> Large Fragment Instrument Set68.120.457 Vario Case<strong>LCP</strong> Screw Set <strong>4.5</strong>/<strong>5.0</strong> mmHexagonal Stardriverecess recessStainless steel 01.200.011 01.200.013Titanium 01.200.012 01.200.014300.610 Sterilization TraySynthes 27
Synthes GmbHEimattstrasse 3CH-4436 Oberdorfwww.synthes.com Presented by:0123036.000.360 SE_128407 AA 30070077 © Synthes 2007 <strong>LCP</strong>, Stardrive and Vario Case are trademarks of Synthes Subject to modifications