S.W.A.S.H. clinical manual - Allard International
S.W.A.S.H. clinical manual - Allard International
S.W.A.S.H. clinical manual - Allard International

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
History OF DEVELOPMENTIn 1984, a four-year old girl with dystonic cerebral palsydeveloped subluxation of her left hip. She had been ableto sit, stand and walk with support (albeit with scissoring).A fixed abduction brace was recommended to stabilize herhip, but her father was concerned about the negative sideeffects such a device could impart on ”normal” function.He researched medical literature published on use of hiporthotic devices, and concluded the ”ideal” brace for hisdaughter must permit:• Independent hip flexion• Maximum abduction during hip flexion• Minimum abduction - just enough to prevent scissoringduring hip extension and weight-bearing• Normal anatomical movement as the orthosis movesfrom minimum abduction with hip extension tomaximum abduction with hip flexionBased on the findings in available literature, the father concludeda device was required that:• Would allow the child to pursue a more normal rangeof activites with reduced risk of hip dislocation• Would further enhance acetabular modeling andand development of the hip joint complex.With this in mind, he set about to design his daughter abrace that uses the rotation of leg bars about an inclinedpivot to achieve abduction which was continuously variableaccording to the degree of hip flexion. The result of thiseffort is the SWASH ® (Sitting, Walking And Standing Hip)Orthosis.The first commercial use of the SWASH ® began in 1992.Since then, thousands of children and some adults worldwidewith varying degrees of disabilities have been able torealize the functional and psychological benefits offered bythe assistance of this innovative orthotic intervention.Primary development goals of the SWASH ®1. Increase abduction and stretch hip adductors to improvehip alignment2. Prevent excessive adduction during sitting, standingand walking3. Optimize sitting and standing posture4. Achieve the above goals with an automatic transitionfrom neutral (walking, standing) to abduction (sitting)4
BIOMECHANICS OF SWASH ®A Major BiomechanicalEngineering AccomplishmentThe SWASH ® appears to be a relatively simple device, butlooks can be deceiving. From the distal tip of one uprightto the distal tip of the other, there are a combination oftwenty-one (21) joints and angles in the SWASH ® . Changingone angle affects the function of the other twenty.Anatomic vs. Orthotic Pathways of MotionAt first glance, it appears that the orthosis should causesignificant ”pistoning” of the thigh cuffs on the thighs, asthe wearer moves from standing to sitting. The orthotichip joints do not approximate the location of the anatomicalhip joints. The orthotic joints are actually positioned closerto the sacroiliac joints than they are to the hip joints.20°Center of GravityUpon seeing the SWASH ® orthosis, one would expect thatthe center of gravity would be posterior to the trunk. Thejoints are posterior, leading to the expectation that thecenter of gravity would also be posterior.In fact, however, the tri-plane engineering again utilizes allthe angles described previously to bring the center of gravityjust anterior to L2, through the center of the trunk. Ofmost significance is the 20° angle in the transverse planedesigned into the posterior section of the pelvic band. Thisangle moves the center of gravity from posterior to midtrunkalignment.AnatomicalOrthoticBut in fact, the pathways of motion of the SWASH ® thighcuffs do mimic the pathways of motion of the femurs.This is designed into the orthosis through a combinationof the angle of the pelvic band in the sagittal plane, and theangle of the hip joint assemblies in the transverse plane.Also contributing are the angles of the uprights throughthe hip joints, and the planes on which the angles on theuprights themselves are shaped.The result of this tri-plane engineering is that ”pistoning”of the cuff on the thigh is minimized.Proximal Transfer of Adductor ToneHigh adductor tone affects posture of the entire body. Itdrives the feet into pronation, internally rotates the lowerlimbs, and has a flexion influence on both the knees andthe hips. This lower extremity reaction to adductor toneinfluences the trunk into a slouched posture.It is theorized that as SWASH ® overcomesadductor tone, two thingshappen. First, the biomechanicaleffect of the tone is reversed.It exerts an external rotaryinfluence on the lower limbs(without twister cables), theknees and hips are influencedmore towards extension, andthe trunk stands more erect.Second, as the SWASH ® reachesits limit for adduction, it transfersadductor force proximally,assisting anterior rotation of thepelvis to help achieve a more erect posturalposition.NOTE: Preliminary results of a 10- patient study reportsthere is no increase in adductor tone associated with theuse of a SWASH ® .5
HIP STABILIZATIONThe most visible benefits of the SWASH ® are improvementsin sitting and standing posture and stability, and for theambulatory user, improvement in gait. The benefits can beimmediate and are often dramatic. Continued improvementsmay be seen after the wearer has become acclimatized tothe orthosis.Excessive adduction with internal rotation causes a posteriordislocating force, which is opposed by the SWASH ®variable abduction brace. Although this may be expectedto reduce the risk of hip dislocation, ongoing studies todocument this benefit have not yet been been completed.Given the visible benefits, perhaps the most importantbenefit the SWASH ® offers is its influence on hip stability.The very nature of high adductor tone places dislocatingforces on the hips. The internal rotation and adductionforces leave hips at risk. Data shows that ambulatory childrenwith CP have a 30% incidence, and non-ambulatorychildren have a 60% incidence of hip subluxation requiringmedical intervention.ADductionInternal RotationUnstable AlignmentABductionExternal RotationBetter AlignmentThis case example offers some insight into the effects of SWASH ® to help prevent hip displacement over an extendedperiod of time.In this before fitting x-ray, pelvic obliquity and (R)hip subluxation are readily evident. The acetabulumis shallow and does not cover the femoral head.At year two post fitting shows further improvementof the femoral head within the acetabulum.One year post fitting shows improvement in pelvicangle and hip subluxation. Approximately 80% ofthe femoral head is now covered.Three years post fitting shows normal pelvicangles and closer to normal hip development.6
Functional influenceSitting Posture & StabilityMany individuals with neuromuscular disorders are veryunstable during sitting due to spastic adduction leading toa narrow base of support. This is demonstrated by a typicalslouched posture during sitting, along with the need forexternal assistance or the use of hands for ”touch balance”.While it is common to refer to one’s ”envelope of function”,this type of sitting instability might be described as limitingone to a ”cocoon of function”, as hands are functionallytied down to the sitting surface.When in the sitting position, SWASH ® abducts the hipsto create a wider tripod base for sitting stability. This widerbase of support, combined with the spinal and pelvic supportof the pelvic band, often provides sufficient posturalassistance to open a whole new world for the userwho otherwise is unable to sit without external assistance.Harnesses, wedges, and bolsters may often be considerablyreduced if not eliminated.The less involved child, who may be able to sit withoutexternal assist but requires use of the upper extremitiesfor touch balance, may be able to sit independently whenwearing the SWASH ® - freeing the hands for eating, interactingwith others, for more active participation in therapyprograms, and for playing.From the mild to the severely involved, the stable base forsitting will result in a more upright sitting posture - certainlya significant benefit for hip and spine alignment. The opportunityfor enhanced upper extremity function may alsoimprove trunk strength and control.Standing Posture & StabilityWith a successful fitting, SWASH ® may offer significantimprovements in standing posture. Non-ambulatory wearerswill often be better able to stand more upright in theirstanding frames with reduced external assistance. For theambulatory wearer, there will often be improvements intrunk posture, reduced scissoring and a wider base ofsupport for standing.As a result of overcoming adductor tone and its biomechanicalconsequences, standing frames or walkers will generallyneed to be adjusted higher to accommodate the moreerect posture.Proprioceptive ImplicationsWhile the biomechanical aspects of the SWASH ® may berelatively well understood, it is more difficult to understandthe proprioceptive implications. In almost every instance,fitting the SWASH ® will result in a decrease in spasticityand improved reach targeting of the upper extremities.The mechanism for this common outcome is not entirelyunderstood.7
Functional influenceGait DynamicsSWASH ® is the only hip orthosis that is designed to offervariable hip abduction - requiring no ”unlocking” or otheradjustments by the wearer or the caregiver.For the ambulatory patient, this can offer significant functionalbenefits. With a successful fitting SWASH ® can provideenough abduction to prevent scissoring during standingand gait. As the hips are flexed to the sitting position,the SWASH ® uprights guide the femurs to further abductthe hips to create a tripod base for sitting stability and tostretch the hip adductors.Respiratory and Speech FunctionsThe improved posture reduces the compromising of breathingcapacity which can be a side affect of slouched posture.Many therapists have reported this improved posturecan also have a positive impact on speech as a result of theimproved breathing control and since the user can nowbring the head and neck (less constriction of the vocalcords) into a more upright position.Control of scissoring gait, more upright posture, and abilityto shift from standing to sitting and sitting to standing withminimal, if any, external assistance can offer numerous benefitsfor ambulatory candidate:• They may ambulate with greater independence. Manychildren who have never taken more than a few stepswithout someone having to untangle their feet can nowwalk to the limits of their endurance without scissoring.• SWASH ® may help conserve energy. Without the energyconsumed in attempting to stabilize the trunk and untanglescissoring feet, the child is often able to walk more fluidlyfor greater distances.• With the ability to walk better and more independently,they will want to walk more, and their distance/walkingmay improve. Walking now becomes a means of gettingfrom here to there instead of an exercise to be enduredduring supervised therapy sessions. With better gait biomechanicsand greater gait capacity, they will be betterable to participate in physical therapy protocols to increasemuscle length and reduce tone in the hamstrings and calfgroup.8
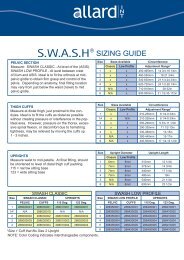
CANDIDATE SELECTIONSince its introduction, physicians have prescribed thousandsof SWASH ® for patients from infants to adults, ambulatoryand non-ambulatory, from mild to severe involvement - toprotect hip alignment, improve the ability to sit independentlyor at least with reduced external assistance, improvesitting and standing posture, and for improvement ofstepping for patients with scissoring postures.The following are guidelines presented bysubject area.AgeThe following age discussions are intended as a guide only,based on fitting experiences. However, it is important toremember every candidate and level of development variesat different ages, so there will definitely be exceptions ineach age category:Early Intervention (9 months - 2 years):Both SWASH ® and SWASH ® Low profile will fit an infantas young as 9-10 months. SWASH ® has been widely prescribedfor infants at risk for spastic hip displacement. Whenproperly fitted, SWASH ® will not interfere with crawling.For the child that may be able to learn to walk, SWASH ®can often help them to better stabilize as they pull themselvesup on furniture. For the child who may only be able tosit, the wide abduction base may help them achieve a morestable position.2 - 6 yearsThis age group will generally adapt to the SWASH ® veryquickly. They tend to accept quite readily the correctionit offers and, with guidance from the physical therapist andcaregiver, develop new skills. They usually accept the sittingstability it offers and quite freely start using their upperextremities for function instead of for sitting balance.13 - AdultThe pelvic band of the Classic SWASH ® will fit a waistcircumference up to 72 cm (28 1/4 inches). SWASH ® hasbeen successfully fitted on small adults who fit within thisrange. Again, due to the increased strength of the uprights,the SWASH ® Low Profile may be required to control theadductor tone. A larger size SWASH ® Low Profile withlonger uprights and larger cuffs is now available.Acclimatization TimeAge, cooperation, and the degree of functional involvementall affect the length of time for the wearer to become accustomedto the orthosis. As a general rule, the younger thecandidate, the quicker they accommodate to the orthosis. Eventhose that acclimate quickly, will continue to improve infunction as they continue to wear the orthosis. If immediateresults are not seen, it is encouraged to allow the candidateto continue to wear the orthosis at least an additional30 minutes to one hour as it has been observed that giventime to relax in the orthosis - they start to realize howthey can use its support to sit, stand, or walk better. If noimprovement is seen after one hour, it is unlikely SWASH ®will be of benefit.Sometimes improved posture is evident immediately uponapplication, but then he or she tends to return to the originalslouched posture. This is usually indicative that the orthosiswill work, but physical therapy and re-training may berequired to establish new movement patterns.Especially children who have always had to use their handsfor balance, are scared to ”let go” for fear they will toppleover. A little ”diversion therapy”, such as trying to get themto clap their hands or reach for a ball will help them overcomethe fear.6 - 12 yearsAround this age the child can be slower to adapt. By thetime a child reaches 9 or 10, there may also be musclelength issues (contracture), muscle strength issues, andlong-standing neuromotor patterns that can be very difficultto overcome. For the child in this age group withstrong adductor tone, the SWASH ® Low Profile is generallyrecommended as the uprights in this model are stronger.10
PRODUCT SELECTIONLow profileClassicSWASH ® ClassicThe original design of SWASH ® uses a plastic anterior overlappelvic band to secure the orthosis around the waist andmaintain its position, resting over the ASIS, just below thenavel. In the back, the pelvic section extends from L2/L3 tothe distal margin of the sacrum, providing maximum pelvicsupport. Children with low trunk tone and/or very limitedtrunk control strength may benefit from the increasedposterior and lateral support this design offers. The thighcuff closure is a double-lock strapping system to reducethe chances of unwanted removalv by children. Pelvic bandand thigh cuff padding are removable for laundering.The uprights are 6mm (size1) and 7mm (sizes 2-4) diameter.The smaller diameter uprights on the size 1 allow more”spring”, permitting less restriction of movement. This isoften desirable for the developing infant.SWASH ® Low Profile IISWASH ® LP II uses a metal pelvic band with padded iliacextensions that are to be shaped and positioned betweenthe crest of the ilium and the ASIS. The double strap frontclosure allows for symmetrical application. In the back,the padded metal posterior frame extends from approximatelyL2/L3 to S1/S2. The metal offers positive non-slipcontact for the abduction control joints, and includes clearmarkings to monitor abduction settings. The joints aretapered downward to accommodate most walker styles.The thigh cuff closure is a simple double Velcro fold-backclosure for easy donning and doffing. The pelvic bandcover and thigh cuff padding are removable for laundering.The uprights for all sizes are 8mm diameter. This increasein diameter offers added strength to manage very hightone, plus it allows cuffs to be completely interchangeablebetween all sizes.Guidelines for Product SelectionThe following are offered as general guidelines only. When possible, it is recommendedto try each style on the patient to best assess which offers optimum function.SWASH ® Classic• When maximum trunk control is required, i.e.,for the candidate who lacks muscle strengthor upper body control to sit upright.• When patient is primarily non-ambulatory(GMFCS IV-V).• When a smaller diameter (6mm) uprights onthe size 1 are desired to permit less restrictionof movement.• When the greater pelvic coverage area triggersmore desirable neuro-sensory motor response.SWASH ® Low Profile II• When the primary goal is to control scissoring gaitand the posterior joints on the SWASH ® Classic interferewith posterior walker, and a new walker is not an option.• When wearer has limited space betweenthe iliac crest and the rib cage.• When maximum upright strength is required to manageadductor tone.• When candidate and/or caregiver acceptance of”bracing” is an issue, the Low profile II is morecosmetically acceptable to some.11
PRE AND POST-FITTING FUNCTIONAL EVALUATIONSPre-Fitting Functional EvaluationsA pre-fitting assessment should be done and documentedwith a team consisting of at least a physical therapist and theorthotist. It is also desirable to have the primary caregiverpresent during this assessment. Each person brings to theevaluation their own areas of expertise and observationalskills. Don’t be surprised if the primary caregiver seesmore than the rest of the medical team! Their observationsand comments can be surprisingly insightful.The assessments should be oriented toward assessing thehip stability/displacement and overall function as opposedto individual components of function. Carefully observefunction or limitations of the adductors, hamstring, andhip flexors. Be aware of and document symmetries foundduring the evaluation. Some facilities are using videotape asone of the ways to document the before and after effectsof the SWASH ® . Clinically proven assessment methodssuch as Gross Motor Function Measure (GMFM), or thePeabody Developmental Motor Scales (PDMS), amongother tests will add validity and proven repeatability to theassessment process.Below is a guide of areas to assess posture and functionPRIOR to SWASH ® fitting:SITTING (90/90 position)• Overall sitting height from sitting surface• Time no touch sitting• Reaching distance capacity• Ball catch capacity• Sit to stand functional performance• General stability and posture• Hip adduction• Pelvic tilt posture due to hamstring tightnessSTANDING• Overall stance height• Foot position and alignment• Reaching capacity with extrinsic support• Reaching capacity without extrinsic support• Stand to squat functional performance• General posture• Femoral alignmentWALKING(with normal ambulatory aid and with normalAFOs if used)• Incidence of scissoring and scissoring posture• Transverse plane alignment both sides(one limb rotated more than the other?)• Stride length• Stride base width• Heel to toe utilization during gait• Speed• Distance capacityPrimary & Secondary GoalsBased on above assessment, establish primary and secondarygoals for the orthotic intervention. For example:Hip alignement? Stretch adductors? Increase walking capacity?Improve sitting posture? Appropriate product selection(Classic or Low Profile, 115° or 123° uprights) and properfit are highly dependent on knowing these goals.Post-Fitting Functional EvaluationsDuring this process, simply repeat the evaluations accomplishedin the pre-fitting evaluation. Note any changes infunctional capacity that are measured or observed.Please consider the following:AgeThe younger wearer typically adapts to the orthosis andshows more immediate improvements than the olderwearer.Acclimatization TimeWhile some differences are usually apparent immediatelyafter fitting, many more changes will become apparentafter days, weeks, or months in the SWASH ® . It may takesome time for the wearer to acclimatize to and to trust theorthosis. Many children will demonstrate a more erect andstable standing posture. It may take some time to becomeacclimatized to this new posture and elevation. Cervicalhyperextension and spinal rotation should diminish aspelvic stability increases. Improvements in standing balanceand stability may be demonstrated after a few hours ordays.Walker, Standing Frame, Crutch AdjustementBe certain that the height of any standing or walkingassistance device is evaluated with the child wearing theSWASH ® . It will often need to be raised to accommodateto the new stance height of the child.Abduction AdjustmentIn initially setting up the orthosis, it is difficult to judge theamount of abduction required to provide optimum hipstability and achieve established goals. If ambulatory andscissoring is still hindering gait, abduction angles willl needto be re-adjusted by the fitter.13
PROTOCOLS AND PROPER FIT GUIDELINESProtocolsWearing timeThe number of hours the orthosis is to be worn should bedetermined by the physician. This time will vary dependingon the degree of involvement of the pathology, the goalsof the rehabilitation program, and the tolerance of thewearer. While up to 24 hour use may be indicated, therecommended wearing time is at least six hours per day,usually during periods of highest activity (sitting, standing,and stepping). The SWASH ® may also be prescribed to beworn at night to control night time scissoring.Fitting over / under clothingThe orthosis should ideally be fitted under clothing tooptimize the control it has over hip alignment. This alsofacilitates the child who is managing their own toilet.Liner care instructionsThe liner in the SWASH ® Classic and the cover of theSWASH ® Low Profile are removable. Both may be removed,hand washed in cool water with mild detergent, anddried flat. Replacement liners and covers are availablethrough your orthotist.Skin careRed marks that appear as a result of wearing the orthosisshould disappear within 30 minutes of removing the orthosis.The most persistent red marks are usually on the inside partof the thigh under the thigh cuff. Consult your orthotistif the red marks do not disappear within 30 minutes afterremoving the orthosis.Orthotist Follow-UpA one-to-two week post-fitting check-up is recommendedto assure the integrity of the othosis and caregiverfitting technique. The primary purpose of this follow-up isto check for the need to adjust hip abduction to assureproper hip alignment.Proper Fit GuidelinesPelvic BandLocation:SWASH ® Classic - Immediatelyover the ASIS.SWASH ® L.P. The metal pelvic bandwith padded iliac extensions shouldbe positioned between the crest ofthe ilium and the ASIS.SymmetryFor both orthoses, make certain the orthosis is applied assymmetrically as possible. The orthosis should NOT berotated on the wearer as this can result in loss of controlof hip alignment.TightnessYou should be able to insert the fingers of one hand betweenthe padding and the abdomen.Amount of abductionThe abduction setting varies considerably from patient topatient, depending on primary and secondary goals for theorthosis. For both non-ambulatory and ambulatory wearers,the ”ideal” is to adjust abduction to provide appropriatehip containment and knee clearance.14
PROTOCOLS AND PROPER FIT GUIDELINESCuffsUprightsLocation - Usually as distal as possible without interferringwithpopliteus, but may be located up to distal 2/3 of femurif flexion influence is present.Left and Right - There is a left and right for the uprights.When standing the 1st curve from the distal end shouldangle to the posterior. If it doesn’t, it is on the wrong side.Closure Gap - There should be no more than 2 inches /5 cm gap gap between the medial and lateral sides of theplastic. Tightness - Comfortably snug - never so tight as tocause red marks or compromise circulation.Length - The distal end of the upright should be in line withthe distal end of the cuff padding.The cuffs are conical shape. They should be fitted so thegreater circumference is proximal.Hip Clearance - The uprights should be as close as possibleto the greater trochanters without impinging on themwhen the hips are flexed.15
BENEFITS AND OUTCOMESBenefits• Limits or controls adduction when sitting, standing andwalking to prevent scissoring• Provides additional abduction for muscle lengthening andsitting stability• Provides support throughout the day• Limits adduction during the night• May reduce hip displacement caused by strong adductors• Improves hip alignment• Can prolong effects of other treatment modalities• Maintains muscle length• May delay the progression to surgeryOutcomes• Improved ambulation when wearing the orthosis. ”Gaitscores showed improved pelvic symmetry, better kneeclearance, and progression in functional walking scales inmost cases”• Longer walking distances using less energy is reported bysome parents• Vertical positions and dynamic walking are associatedwith improved respiratory, bladder and kidney functions• Improved trunk control facilitates upper body functionfor enhanced stretching and other exercises to improvemuscle control and coordination skills• Improved sitting balance means the possibility of usingboth hands to perform tasks such as eating, playing,manipulating objects, and interacting with others insteadof holding the sitting surface for touch balance• Neutralizing the dislocating forces secondary to highadductor tone may arrest or reduce hip displacement• Clinically observable impact on the function of theproprioceptive response. This can generally be seenin thea) Reduced tone of the adductorsb) Improved posture of the trunk andc) Enhanced coordination of the upper extremitiesresulting in better reach targeting• Often helps the wearer overcome pathologicalmovement patterns• Early mobilization may also reduce subluxation anddislocation of the hips• Improved respiratory function as a result of the moreupright posture16
Frequently AskedQuestions about SWASH ®Is the SWASH ® usually worn over or underclothing?The SWASH ® is generally fitted under clothing to optimizethe control the device has in enhancing hip alignment.What about toileting?Generally SWASH ® must be removed for toileting becausethe orthosis interferes with easy donning and doffing ofunderwear and diapers.Will using SWASH ® strengthen adductors?The opposite is true because the SWASH ® serves tostretch the adductors and cause them to <strong>clinical</strong>lypresent with lower tone.When will patients progress to not needingthe SWASH ® ?The SWASH ® helps manage the consequences of highadductor tone. While there may be some carryover inlessened adductor tone after use of the SWASH, it isnot known if it will return if SWASH ® use is totallydiscontinued.Will AFOs still be necessary?The SWASH ® does not alter the need for AFOs. It may,however, change the design criteria for some patients.Because the SWASH ® has a significant influence over transverseplane rotation of the lower extremities, AFOs willgenerally need to be set up in relatively neutral positionrelative to rotation.How long should the patient wear the SWASH ®each day?The SWASH ® is generally worn at least six hours each day.It can also be very appropriate for use as a night splint.Are there any side effects to using the SWASH ® ?Pressure marks may be evident on inside thigh wherethe SWASH ® overcomes the forces of abnormal adductortone. These marks should disappear within 30 minutesof removing the SWASH ® .The patient still seems to sit in too much spinalflexion. Can anything be done about that?115° uprights tend to minimize this problem. Adding asitting wedge (thicker part under seat, narrow part underlegs) can also help to minimize the negative postural effectsof tight hamstrings. If the problem persists, return to theorthotist for further adjustments.How long before a child will ”outgrow”his or her SWASH ® ?SWASH ® will usually fit a child for 2-3 years. Componentsare sold separately, so it is possible for the orthotist toadjust up to a larger cuff or longer uprights should that benecessary.17
INITIAL FITTING ASSESSMENTPatient ID#Physical TherapistDateOrtotistPhysicianWITHOUT SWASHWEARING SWASHSITTING (90/90 position)Hip adductionPelvic tilt posture due to tight hamstringsSitting height from sitting surfaceTime no touch sittingReaching distance capacityBall catch capacitySit to stand functional performanceGeneral stability and postureSTANDINGFemoral alignmentOverall stance heightFoot position and alignmentReaching capacity w/extrinsic supportReaching capacity w/o extrinsic supportStand to squat functional performanceGeneral PostureWALKINGIncidence of scissoringTransverse plane alignment both sides(one limb rotated more than the other?)Stride LengthStride Base WidthHeel to toe utilization during gaitSpeedNeuromuscular control (jerky? fluid? balance issues?)Distance capacity19
SWASH ® Referencelist1 R. N. Boyd et al., The effect of botulinum toxin type A and a variable hip abduction orthosis on grossmotor function: a randomized controlled trial. European Journal of Neurology 2001, 8 (Suppl.5): 109-119.2 Dianne Russel et al., Canada Child Centre for Childhood Disability Research, Hamilton, Ontario,Canada, AACPDM Conference, Washington, DC, 19993 Danielle Truscelli, Philippe Toullet, Philippe Lancert, SWASH Preliminary report published on theFrench medical publication ”la letter de medicine physique & de réadptation” December 19994 Report from ”The 15th Scientific Meeting of the Japanese Society of Prosthetics and Orthotics”,November 27 - 28, 1999, Hiroshima.5 Dormans, J.P., Pellegrino, L., Caring for Children with Cerebral Palsy, A Team Approach. Baltimore:Paul H. Brookes Publishing Co., 1998.6 Batshaw, Mark L., Children with Disabilities. Baltimore: Paul H. Brookes Publishing Co., 19977 R.N. Boyd, S.G. Manion, Effect of the Variable Hip Orthosis, Newcomen Centre, Guy´s Hospital,London, England, Interbor Conferece, Oslo, 19968 R.N. Boyd, New Horizons in Cerebral Palsy, ISPO Melvourne Australia 30-31 March 19959 Atyer-Acevedo, Jane, Physical Therapy for the Child with Cerebral Palsy. Pediatric...10 Physical Therapy, Second Edition, Philadelphia: J.B. Lippincott Company, 199411 Scherzer, Alfred, Tscharnuter, Ingrid, Early Diagnosis and Therapy in Cerebral Palsy, New York:Marcel Dekker, Inc. 199012 Houkam et al., Treatment of Acquired Hip Subluxation in Children with Cerebral Palsy,Journal of Pediatric Orthopedics, Vol. 6, No. 3, New York: Raven Press, 198613 Folio R., Fewell R., Peabody Developmental Motor Scales and Activtiy Cards, Chicago:The Riverside Publishing Co., 198314 Paul A.R. Meyer, MRCP, A Variable Abduction Brace to Treat Hip Subluxation in Cerebral Palsy,Addenbrooke´s Hospital, Cambridge, England15 Jan F.A. Smits, A New Approach for Dynamic Hip Orthotic Management of the Child withCerebral PalsyApril 2009www.allardint.comTel +46 42 25 27 00Fax +46 42 25 27 25ALLARD INTERNATIONALc/o Camp Scandinavia ABKarbingatan 38SE-254 67 Helsingborg SWEDENinfo@allardint.com