Pediatric Symptom Checklist
Pediatric Symptom Checklist Pediatric Symptom Checklist
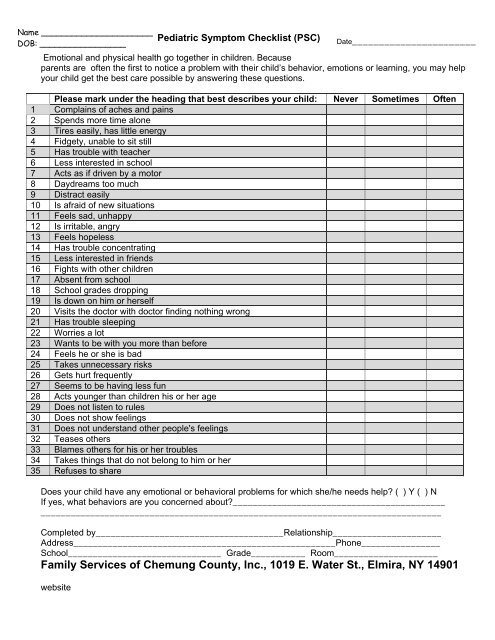
Name ______________________Pediatric Symptom Checklist (PSC)DOB: _________________Date_______________________Emotional and physical health go together in children. Becauseparents are often the first to notice a problem with their child’s behavior, emotions or learning, you may helpyour child get the best care possible by answering these questions.Please mark under the heading that best describes your child: Never Sometimes Often1 Complains of aches and pains2 Spends more time alone3 Tires easily, has little energy4 Fidgety, unable to sit still5 Has trouble with teacher6 Less interested in school7 Acts as if driven by a motor8 Daydreams too much9 Distract easily10 Is afraid of new situations11 Feels sad, unhappy12 Is irritable, angry13 Feels hopeless14 Has trouble concentrating15 Less interested in friends16 Fights with other children17 Absent from school18 School grades dropping19 Is down on him or herself20 Visits the doctor with doctor finding nothing wrong21 Has trouble sleeping22 Worries a lot23 Wants to be with you more than before24 Feels he or she is bad25 Takes unnecessary risks26 Gets hurt frequently27 Seems to be having less fun28 Acts younger than children his or her age29 Does not listen to rules30 Does not show feelings31 Does not understand other people's feelings32 Teases others33 Blames others for his or her troubles34 Takes things that do not belong to him or her35 Refuses to shareDoes your child have any emotional or behavioral problems for which she/he needs help? ( ) Y ( ) NIf yes, what behaviors are you concerned about?____________________________________________________________________________________________________________________________Completed by______________________________________Relationship______________________Address_____________________________________________________Phone________________School_______________________________ Grade___________ Room_____________________Family Services of Chemung County, Inc., 1019 E. Water St., Elmira, NY 14901website
Name ______________________<strong>Pediatric</strong> <strong>Symptom</strong> <strong>Checklist</strong> (PSC)DOB: _________________Date_______________________Emotional and physical health go together in children. Becauseparents are often the first to notice a problem with their child’s behavior, emotions or learning, you may helpyour child get the best care possible by answering these questions.Please mark under the heading that best describes your child: Never Sometimes Often1 Complains of aches and pains2 Spends more time alone3 Tires easily, has little energy4 Fidgety, unable to sit still5 Has trouble with teacher6 Less interested in school7 Acts as if driven by a motor8 Daydreams too much9 Distract easily10 Is afraid of new situations11 Feels sad, unhappy12 Is irritable, angry13 Feels hopeless14 Has trouble concentrating15 Less interested in friends16 Fights with other children17 Absent from school18 School grades dropping19 Is down on him or herself20 Visits the doctor with doctor finding nothing wrong21 Has trouble sleeping22 Worries a lot23 Wants to be with you more than before24 Feels he or she is bad25 Takes unnecessary risks26 Gets hurt frequently27 Seems to be having less fun28 Acts younger than children his or her age29 Does not listen to rules30 Does not show feelings31 Does not understand other people's feelings32 Teases others33 Blames others for his or her troubles34 Takes things that do not belong to him or her35 Refuses to shareDoes your child have any emotional or behavioral problems for which she/he needs help? ( ) Y ( ) NIf yes, what behaviors are you concerned about?____________________________________________________________________________________________________________________________Completed by______________________________________Relationship______________________Address_____________________________________________________Phone________________School_______________________________ Grade___________ Room_____________________Family Services of Chemung County, Inc., 1019 E. Water St., Elmira, NY 14901website
YOUTH EMOTIONAL HEALTH SCREENING PROGRAMScreening Consent FormIF CHILD IS ALREADY RECEIVING EMOTIONAL HEALTH SERVICES,DO NOT COMPLETE THIS FORMI DO WANT MY CHILD TO PARTICIPATE IN THIS SCREENINGI, ______________________________, give permission for my child to participate in thePlease Print Your NameFamily Services Youth Emotional Health Screening Program.Parent/Guardian Signature:_____________________________ Date:________________Please Complete All Of The Following InformationPLEASE PRINT CLEARLY______________________________Child’s Name_____________________________Student Date of Birth____________ ________________ _____________________________Age Male/Female Home Address______________________________School____________________________________Grade_____________________________City, State, Zip___________________________________County_____________________________Home PhoneChild Lives: With Parent_____; In Foster Care _____; With Guardian_____FAMILY SERVICES OF CHEMUNG COUNTY, INC.,1019 EAST WATER ST. ELMIRA, NY 14901607-733-5696website


