Ogilvie's Syndrome.pdf - Henry Ford Health System
Ogilvie's Syndrome.pdf - Henry Ford Health System
Ogilvie's Syndrome.pdf - Henry Ford Health System
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
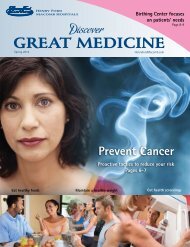
Abdominal XrayMarked dilation ofcolonMaximal diameter of12 cmNo obvious free air
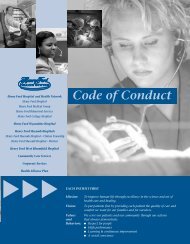
CTAxial ViewMassivecolon dilationAlso noted:Small bowelloops ofnormalcaliber
CTDilatedlarge bowelloopsLargeamount ofstool inrectumStool 9 cmat greatestdiameter
CTRectalstool ball
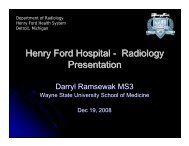
Barium EnemaGastrografin contrastreached midascending colonCecum not distinctlyidentifiedRenal contrast seenin collecting systemand bladder fromrecent CT scan
Differential Diagnosis• Colonic obstruction• Colonic volvulus – cecal or sigmoid• Colorectal carcinoma• Ogilvie syndrome• Ileus – postoperative or paralytic
Diagnosis - Ogilvie syndrome• Patient has a history of multiple sclerosisconsistent with Ogilvie syndrome• Colonic dilation unchanged past 2 yrs• Ogilvie syndrome is also known as acute colonicpseudo-obstruction obstruction (ACPO)• Radiological appearance of acute large bowelobstruction without a mechanical cause• Hallmark - massive cecal dilation• Cecal ischemia and perforation can occur
Discussion - Ogilvie syndrome• Described by British surgeon Sir Ogilvie in 1948• Usually hospitalized patients• Often a recent medical illness or surgical procedure• Also seen in trauma and neurological conditions• Pathophysiology: : Imbalance in the autonomicinnervation of the colon• Decrease in parasymathetic activity leading toadynamic colon similar to Hirschsprung Disease(normal ganglion cells at autopsy)• Increase in sympathetic activity
Discussion cont.• Radiology:• Abdominal x-ray x- dilated cecum ( > 10 cm) and diffuse colonicdilation (ascending & transverse)• Important to rule out mechanical obstruction• Gas shadows in rectum on plain film• Normal colonic filling on radiographic enema• Important to rule out volvulus• Ogilvie syndrome treatments:• Enemas, NG suction, stop mobility impairing medication• Neostigmine – inhibits acetyl cholinesterase → increasedacetylcholine → increased GI motility• Colonoscopic decompression (cecal(recurrence 22-41%), tubececostomy (open or CT guided), subtotal colectomy (ifperforated)
References• Remy, MD, et al. “Olilvie<strong>Syndrome</strong>.” eMedicine Specialties:Gastroenterology: Colon. (2008)• N. Agarwal, , A. Mishra & Z. Kayali : Acute Colonic Pseudo-obstruction (The Ogilvie syndrome): A Case Report and Review ofLiterature . The Internet Journal of Emergency and Intensive CareMedicine. 2003 Volume 7 Number 1