DRUG NAME: PENTOSTATIN - BC Cancer Agency
DRUG NAME: PENTOSTATIN - BC Cancer Agency
DRUG NAME: PENTOSTATIN - BC Cancer Agency
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
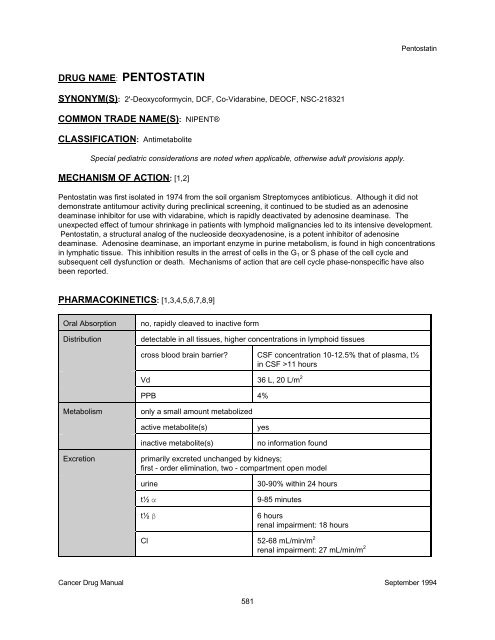
Pentostatin<strong>DRUG</strong> <strong>NAME</strong>: <strong>PENTOSTATIN</strong>SYNONYM(S): 2'-Deoxycoformycin, DCF, Co-Vidarabine, DEOCF, NSC-218321COMMON TRADE <strong>NAME</strong>(S): NIPENT®CLASSIFICATION: AntimetaboliteSpecial pediatric considerations are noted when applicable, otherwise adult provisions apply.MECHANISM OF ACTION: [1,2]Pentostatin was first isolated in 1974 from the soil organism Streptomyces antibioticus. Although it did notdemonstrate antitumour activity during preclinical screening, it continued to be studied as an adenosinedeaminase inhibitor for use with vidarabine, which is rapidly deactivated by adenosine deaminase. Theunexpected effect of tumour shrinkage in patients with lymphoid malignancies led to its intensive development.Pentostatin, a structural analog of the nucleoside deoxyadenosine, is a potent inhibitor of adenosinedeaminase. Adenosine deaminase, an important enzyme in purine metabolism, is found in high concentrationsin lymphatic tissue. This inhibition results in the arrest of cells in the G 1 or S phase of the cell cycle andsubsequent cell dysfunction or death. Mechanisms of action that are cell cycle phase-nonspecific have alsobeen reported.PHARMACOKINETICS: [1,3,4,5,6,7,8,9]Oral AbsorptionDistributionno, rapidly cleaved to inactive formdetectable in all tissues, higher concentrations in lymphoid tissuescross blood brain barrier?CSF concentration 10-12.5% that of plasma, t½in CSF >11 hoursVd 36 L, 20 L/m 2PPB 4%Metabolismonly a small amount metabolizedactive metabolite(s)inactive metabolite(s)yesno information foundExcretionprimarily excreted unchanged by kidneys;first - order elimination, two - compartment open modelurinet½ αt½ β30-90% within 24 hours9-85 minutes6 hoursrenal impairment: 18 hoursCl 52-68 mL/min/m 2renal impairment: 27 mL/min/m 2<strong>Cancer</strong> Drug Manual September 1994581
PentostatinUSES: [1,2,10,11]* Hairy cell leukemiaLess frequent uses include:Chronic lymphocytic leukemiaMycosis fungoidesNon-Hodgkin's lymphomaT-cell lymphomaNo pediatric indications.* Health Protection Branch approved indication.SPECIAL PRECAUTIONS: [6]Pentostatin produces significant immunosuppression, often manifested by herpes simplex and herpeszoster, skin infections and other opportunistic infections. Patients with severe preexisting infectionsshould not receive this agent.Contraindicated in patients with severe renal impairment.Pentostatin has potential mutagenic and carcinogenic properties. Its safe use in pregnancy and its effectson fertility have not been established. Breast feeding is not recommended due to the potential secretion intobreast milk.SIDE EFFECTS: [1,6,7,11,12,13,14,15,16,17,18,19,20,21,22]ORGAN SITE SIDE EFFECT ONSETcentral nervous system lethargy (62%) Efatigue (29%)seizures, coma (rare)EEdermatologic rash (26-49%, occasionally severe) Eextravasation hazardnonegastrointestinal nausea and vomiting (mild-moderate, 40-76%)onset 12-14 hours, may last 48 hoursdiarrhea (12-15%)IIanorexia (16-67%)Ehematologic myelosuppression, recovery 11-18 days EimmunosuppressionEhepatic elevated liver function tests (common, transient) Emusculoskeletal myalgias (9-11%) Eocular painful keratoconjunctivitis (5-16%) E<strong>Cancer</strong> Drug Manual September 1994582
PentostatinORGAN SITE SIDE EFFECT ONSETrenal/metabolicelevated serum creatinine (transient, rare at currentdoses)acute renal failure (mild, reversible)Dose-limiting side effects are underlined.I = immediate (onset in hours to days); E = early (days to weeks);D = delayed (weeks to months); L = late (months to years)EEDose limiting severe renal, hepatic, pulmonary and CNS toxicity, leading in some cases to death, occurredin Phase I studies that used higher doses (20-50 mg/m 2 per course) than currently recommended. Lowerdoses (eg, 4 mg/m 2 ) are relatively well tolerated.Hematologic parameters in patients with hairy cell leukemia are frequently abnormally low at the initiation oftreatment. Therefore, such patients are not readily evaluable for hematologic toxicity.The recovery of dose-related immunosuppression (eg, reduction of CD4 cells) occurs slowly over severalmonths once therapy is finished. No increase in life-threatening opportunistic infections has been reported.Vomiting may increase in frequency and severity with subsequent treatment courses.Lethargy, seizures and coma have been reported. Patients exhibiting such toxicities should not be treateduntil these have resolved. Subsequent treatment with pentostatin should be with lower doses. Effects may begreater in patients receiving high doses, those with poor performance status or with impaired renal function.Neurotoxicity is rarely dose-limiting at
PentostatinAGENT EFFECT MECHANISM MANAGEMENThigh dosecyclophosphamide priorto bone marrowtransplantationfatal cardiac toxicity hasbeen reporteduncertainavoid this combinationfludarabinesevere and/or fatalpulmonary toxicityunknownavoid this combinationvidarabineincreased antiviral andtoxic effectspentostatin inhibitsdegradation ofvidarabinecautionSOLUTION PREPARATION AND COMPATIBILITY: [1,7,24,25]Injection: 10 mg vial; store in the refrigerator (2-8°C). Contains 50 mg mannitol per vial. May also containsodium hydroxide and hydrochloric acid to adjust pH. Preservative-free.Reconstitute powder with 5 mL SWI to a final concentration of 2 mg/mL.Reconstituted solution for injection: Clear, colourless solution. May be stored at room temperature inambient light. The manufacturer recommends use within 8 hours as the solution is preservative-free. Trisselstates only 2-4% drug loss in 72 hours at room temperature.Diluted solution for infusion: Compatible with D5W or NS. Dilutions of 0.18-0.33 mg/mL may be stored atroom temperature under ambient light. Concentrations of 0.18-0.33 mg/mL do not interact with PVC containersor administration sets. Chemical stability in NS for 48 hours at room temperature in glass or PVC containershas been reported (Kane, et al). Dilutions over 20 mcg/mL in dextrose are reported to be stable for up to 51hours in glass containers, while solutions below 2 mcg/mL in dextrose in glass containers lose over 35% ofinitial pentostatin to hydrolysis after 11 hours at room temperature (Kane, et al). The manufacturerrecommends use within 8 hours as the solution is preservative-free.Compatible with ondansetron. It is recommended that pentostatin not be mixed with other drugs.PARENTERAL ADMINISTRATION: [5,26,27,28]SubcutaneousIntramuscularDirect intravenousIntermittent infusionContinuous infusionIntraperitonealIntrapleuralno information available on this routeno information available on this routeslow IV bolus over 5 minutes, with vigorous hydration before and followingadministration (eg, D5-1/2NS 1000 mL before and 500 mL after)in 25-50 mL over 20-30 minutes.not recommended, has been given as a 3 day infusionno information available on this routeno information available on this route<strong>Cancer</strong> Drug Manual September 1994584
PentostatinIntrathecalIntra-arterialIntravesicalno information available on this routeno information available on this routeno information available on this routeDOSAGE GUIDELINES: [5,7,26,27,28]Refer to protocol by which patient is being treated. Numerous dosing schedules exist and depend on disease,response and concomitant therapy. Guidelines for dosing also include consideration of white blood cell count.Dosage may be reduced and/or delayed in patients with bone marrow depression due to cytotoxic/radiationtherapy.Adults:Intravenous: q2w: 4 mg/m 2q1w: 4 mg/m 2 x 3 weeks then 5 weeks restDosage in myelosuppression: No adjustment recommended for patients with anemia, neutropenia orthrombocytopenia at the start of therapy; nor during treatment in patients withanemia or thrombocytopenia. Hold for ANC 0.5 x 10 9 /L. Resume when count returns to predose level.Dosage in renal failure: CrCl (mL/sec) Dose>1 4 mg/m 20.8-1 2 mg/m 2
Pentostatin<strong>PENTOSTATIN</strong> FACT SHEETFOR THE HEALTH CARE PROFESSIONALOTHER <strong>NAME</strong>SUSES2'-deoxycoformycin, DCF, co-vidarabine, DEOCF, NSC-218321,NIPENT®many (refer to monograph)DOSAGE FORMS injection: 10 mg vial (refrigerate, reconstitute with 5 mL SWI)USUAL DOSE RANGE Adults: 4 mg/m 2 IV q2w4 mg/m 2 IV q1w x 3 weeks then rest 5 weeksDOSE REDUCTIONSkidney (renal) failurecentral nervous system side effects (lethargy, seizures, coma)low W<strong>BC</strong> (neutropenia)IV COMPATIBILITY normal saline, dextrose 5%ROUTES direct IV (over 5 minutes with vigorous hydration)intermittent IV (in 25-50 mL over 20-30 minutes)continuous IV (not recommended)EXTRAVASATION HAZARDnoneIMMEDIATE(hours to days)ONSETEARLY(days to weeks)SIDE EFFECT* may be life-threateningside effects in bold, italic type are commonnausea and vomiting (mild-moderate, 40-76%)(onset 12-24 hours, may last 48 hours)* low W<strong>BC</strong>, R<strong>BC</strong>, platelets (myelosuppression, recovery 11-18 days)skin rash* CNS depression (lethargy, fatigue) (seizures, coma, rare)* liver problems (elevated liver function tests, transient)loss of appetite (anorexia, 16-67%)diarrhea (12-15%)muscle aches (myalgias, 9-11%)* kidney problems (elevated creatinine, acute renal failure)eye problems (painful keratoconjuntivitis)<strong>Cancer</strong> Drug Manual September 1994586
PentostatinCONTRAINDICATIONSSIGNIFICANTINTERACTIONS*increases toxicityknown hypersensitivity to pentostatinpregnancy and breast feedinglow W<strong>BC</strong>, R<strong>BC</strong>, platelets (myelosuppression) if evaluableliver failurekidney failure*high dose cyclophosphamide, *fludarabine, *vidarabineLABORATORY MONITORING each treatment: C<strong>BC</strong>, electrolytes, kidney function, liver functionTEACHING AIDS· For the Patient: Pentostatin· For the Patient: Nausea· Chemotherapy and You: a Guide to Self-help During TreatmentNOTES:· Kidney toxicity may be minimized with vigorous hydration (eg, D5-1/2NS 1000 mL over 2-3 hoursbefore administration and 500 mL over 1-2 hours after).· Vomiting may increase in frequency and severity with successive treatment courses.· Skin rash may occur early in therapy without recurrence during continued treatment.<strong>Cancer</strong> Drug Manual September 1994587
PentostatinFOR THE PATIENT: PentostatinOther names: deoxycoformycin, DCF, NIPENT®• Pentostatin (pent-oh-STAT-in) is a drug that is used to treat leukemia and other kinds of cancer.It is a clear liquid that is injected into a vein.• A blood sample will be taken before each treatment. The dose and timing of yourchemotherapy may be changed based on your blood counts and/or other side effects.• Some drugs such as vidarabine (VIRA-A®) may interact with pentostatin. Tell your doctor if youare taking any other drugs as your dose may need to be changed. Check with your doctor orpharmacist before you start taking any new drugs.• The drinking of alcohol (in small amounts) will not affect the safety or usefulness of pentostatin.• Pentostatin may damage sperm and may harm the baby if used during pregnancy. It is best touse birth control while being treated with pentostatin. Tell your doctor right away if you or yourpartner becomes pregnant. Do not breast feed during treatment.• Tell doctors or dentists that you are being treated with pentostatin before you receive anytreatment from them.SIDE EFFECTSNausea and vomiting which is usually mildmay occur starting 12-24 hours after yourtreatment. Some people have little or nonausea.Your white blood cells will decrease duringyour treatments. They will return to normal 11-18 days after your last treatment. White bloodcells protect your body by fighting bacteria(germs) that cause infection. When they arelow, you are at greater risk of having aninfection.Your platelets may decrease during yourtreatments. They will return to normal 11-18days after your last treatment. Platelets help tomake your blood clot when you hurt yourself.You may bruise or bleed more easily thanusual.MANAGEMENTYou may be given an antinausea drug with yourtreatment and a prescription to take at home. Itis easier to prevent nausea than treat it once ithas occurred.·Follow antinausea drug directions closely.·Drink plenty of liquids.·Eat often in small amounts.·Try the ideas in the For the Patient: Nausea.To help prevent infection:·Wash your hands often and always after usingthe bathroom.·Take care of your skin and mouth.·Avoid crowds and people who are sick.·Call your doctor immediately at the first signof an infection such as fever (over 100°F or38°C), chills, cough, sore throat or burningwhen you pass urine.To help prevent bleeding problems:·Try not to bruise, cut or burn yourself.·Clean your nose by blowing gently, do not pickyour nose.·Avoid constipation.·For minor pain, take acetaminophen (eg,TYLENOL®). Do not take ASA (eg,<strong>Cancer</strong> Drug Manual September 1994
PentostatinSIDE EFFECTSTiredness and lack of energy may occur.Hair loss is rare with pentostatin. Your hair willgrow back once you stop treatment withpentostatin. Colour and texture may change.Pain or tenderness may occur where theneedle was placed.MANAGEMENTASPIRIN®) or ibuprofen (eg, ADVIL®).This should return to normal when yourtreatments are finished.·Use a gentle baby shampoo and soft brush.·Avoid hair spray, bleaches, dyes and perms.·Apply warm compresses or soak in warmwater for 15-20 minutes several times a day.SEE YOUR DOCTOR OR GET EMERGENCY HELP IMMEDIATELY IF YOU HAVE:· Signs of an infection such as fever (over 100°F or 38°C); chills; cough; sore throat; pain orburning when you pass urine; redness, pain or swelling of any area of your body; soresforming anywhere on your body.· Signs of bleeding problems such as black, tarry stools; blood in urine; pinpoint red spots onskin.· Seizures or loss of consciousness.SEE YOUR DOCTOR AS SOON AS POSSIBLE (DURING OFFICE HOURS) IF YOU HAVE:· Signs of anemia such as unusual tiredness or weakness.· Signs of liver problems such as yellow eyes or skin, white or clay-coloured stools.· Signs of kidney problems such as lower back or side pain, swelling of feet or lower legs,numbness or tingling in feet or hands.· Changes in eye sight.· Skin rash or itching.CHECK WITH YOUR DOCTOR IF ANY OF THE FOLLOWING CONTINUE OR BOTHER YOU:· Uncontrolled nausea, vomiting or diarrhea.· Easy bruising or bleeding.· Redness, swelling, pain or sores where the needle was placed.REPORT ADDITIONAL PROBLEMS TO YOUR DOCTOR.See Chemotherapy and You: a Guide to Self-help During Treatment available free from theCanadian <strong>Cancer</strong> Society for more information on managing side effects.<strong>Cancer</strong> Drug Manual September 1994
PentostatinBIBLIOGRAPHY:1. Kane BJ, Kuhn JG, Roush MK. Pentostatin: an aenosine deaminase inhibitor for the treatment of hairy cell leukemia. AnnPharmacother 1992;26:939-47.2. Haskell CM, ed. <strong>Cancer</strong> treatment, 3rd ed. Philadelphia: WB Saunders Co, 1990.3. O'Dwyer PJ, Wagner B, Leyland-Jones B, et al. 2'-deoxycoformycin (Pentostatin) for lymphoid malignancies: Rationaldevelopment of an active new drug. Ann Intern Med 1988;108:733-43.4. Smyth JF, Paine RM, Jackman AL, et al. The clinical pharmacology of the adenosine deaminase inhibitor 2'-deoxycoformycin. <strong>Cancer</strong> Chemother Pharmacol 1980;5:93-101.5. McEvoy GK, ed. American hospital formulary service: Drug information 1993. Bethesda: American Society of HospitalPharmacists, 1993:632-7.6. Dorr RT, Von Hoff DD, eds. <strong>Cancer</strong> chemotherapy handbook, 2nd ed. Norwalk: Appleton & Lange, 1994:774-9.7. Parke-Davis Division of Warner-Lambert Canada Inc. Nipent product monograph. Scarborough, Ontario; 1992:November.8. Major PP, Agarwal RP, Kufe DW. Clinical pharmacology of deoxycoformycin. Blood 1981;58:91-6.9. Grever MR, Staubus AE, Balcerzak SP, et al. Clinical pharmacokinetics of 2'-deoxycoformycin in renal impairment. ProcAnnu Meet Am Soc Clin Oncol 1993;12:A361.10. Chabner BA, Myers CE. Clinical pharmacology of cancer chemotherapy. In: DeVita VT, Hellman S, Rosenberg SA, eds.<strong>Cancer</strong>: principles and practice of oncology, 3rd ed. Philadelphia: JB Lippincott Co, 1989.11. Pentostatin and 2-chlorodeoxyadenosine for hairy-cell leukemia. Med Lett Drugs Ther 1992;34(879):89-90.12. Poplack DG, Salian SE, Rivers G, et al. Phase I study of 2'-deoxycoformycin in acute lymphoblastic leukemia. <strong>Cancer</strong> Res1981;41:3343-6.13. Smith JF, Prentice HG, Proctor S, et al. Deoxycoformycin in the treatment of leukemia and lymphoma. Ann NY Acad Sci1985;451:123-8.14. Winick N, Buchanan GR, Murphy SB, et al. Deoxycoformycin treatment for childhood T-cell acute lymphoblastic leukemiaearly in second remission: A pediatric Oncology Group Study. Med Pediatr Oncol 1988;16:327-8.15. Phase II study of 2'-deoxycoformycin in acute lymphoblastic leukemia. NCI, 1979.16. Loffers W, et al. Phase II trial of DCF in adult T-cell lylmphoma. Proceedings of ASCO, 1987;6(739).17. Winick W, et al. DCF in treatment of T-cell acute lymphoblastic leukemia early in second remission. Proceedings of ASCO,1987;6(599).18. Benitz WE, Tatro DS, eds. The Pediatric Drug Handbook. Chicago: Yearbook Medical Publishers, 1988:281.19. Grever MB, Siaw MFE, Jacob WF, et al. The biochemical and clinical consequences of 2'-deoxycoformycin in refractorylymphoproliferative malignancy. Blood 1981;57:406-17.20. Grever MR, Leiby JM, Kraut EH, et al. Low dose deoxycoformycin in lymphoid malignancy. J Clin Oncol 1985;3:1196-1201.21. Drugs of choice for cancer chemotherapy. Med Lett Drugs Ther 1993;35:43-50.22. Brogden RN, Sorkin EM. Pentostatin: a review of its pharmacodynamic and pharmacokinetic properties, and therapeuticpotential in lymphoproliferative disorders. Drugs 1993;46(4):652-77.23. Gryn J, Gordon R, Bapat A, et al. Pentostatin increases the acute toxicity of high dose cyclophosphamide. Bone MarrowTransplant 1993;12:217-20.24. Trissel LA. Handbook on injectable drugs, 7th ed. Bethesda: American Society of Hospital Pharmacists, 1992.25. Trissel LA, Tramonte SM, Grilley BJ. Visual compatability of ondansetron hydrochloride with selected drugs during simulatedY-site injection. Am J Hosp Pharm 1991;48:988-92.26. Wittes RE, ed. Manual of oncologic therapeutics 1991-1992. Philadelphia: JB Lippincott Co, 1991:266.27. Kraut EM, Bouroncie BA, Grever MR. Pentostatin in the treatment of advanced hairy cell leukemia. J Clin Oncol 1989;7:168-72.28. Cassileth PA, Chauvrt B, Spiers AS, et al. Pentostatin induces durable remissions in hairy cell leukemia. J Clin Oncol1991;9:243-6.<strong>Cancer</strong> Drug Manual September 1994590