New Patient Information Form
New Patient Information Form
New Patient Information Form
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
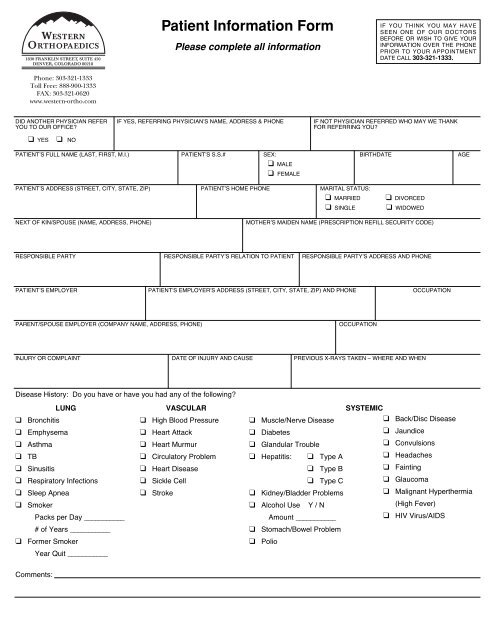
1830 FRANKLIN STREET, SUITE 450DENVER, COLORADO 80218Phone: 303-321-1333Toll Free: 888-900-1333FAX: 303-321-0620www.western-ortho.com<strong>Patient</strong> <strong>Information</strong> <strong>Form</strong>Please complete all informationIF YOU THINK YOU MAY HAVESEEN ONE OF OUR DOCTORSBEFORE OR WISH TO GIVE YOURINFORMATION OVER THE PHONEPRIOR TO YOUR APPOINTMENTDATE CALL 303-321-1333.DID ANOTHER PHYSICIAN REFER IF YES, REFERRING PHYSICIAN’S NAME, ADDRESS & PHONE IF NOT PHYSICIAN REFERRED WHO MAY WE THANKYOU TO OUR OFFICE?FOR REFERRING YOU?❑ YES❑ NOPATIENT’S FULL NAME (LAST, FIRST, M.I.) PATIENT’S S.S.# SEX: BIRTHDATE AGE❑ MALE❑ FEMALEPATIENT’S ADDRESS (STREET, CITY, STATE, ZIP) PATIENT’S HOME PHONE MARITAL STATUS:❑ MARRIED❑ SINGLE❑ DIVORCED❑ WIDOWEDNEXT OF KIN/SPOUSE (NAME, ADDRESS, PHONE)MOTHER’S MAIDEN NAME (PRESCRIPTION REFILL SECURITY CODE)RESPONSIBLE PARTY RESPONSIBLE PARTY’S RELATION TO PATIENT RESPONSIBLE PARTY’S ADDRESS AND PHONEPATIENT’S EMPLOYER PATIENT’S EMPLOYER’S ADDRESS (STREET, CITY, STATE, ZIP) AND PHONE OCCUPATIONPARENT/SPOUSE EMPLOYER (COMPANY NAME, ADDRESS, PHONE)OCCUPATIONINJURY OR COMPLAINT DATE OF INJURY AND CAUSE PREVIOUS X-RAYS TAKEN – WHERE AND WHENDisease History: Do you have or have you had any of the following?LUNG❑ Bronchitis❑ Emphysema❑ Asthma❑ TB❑ Sinusitis❑ Respiratory Infections❑ Sleep Apnea❑ SmokerPacks per Day ___________# of Years ___________❑ <strong>Form</strong>er SmokerYear Quit ___________VASCULAR❑ High Blood Pressure❑ Heart Attack❑ Heart Murmur❑ Circulatory Problem❑ Heart Disease❑ Sickle Cell❑ StrokeSYSTEMIC❑ Muscle/Nerve Disease❑ Diabetes❑ Glandular Trouble❑ Back/Disc Disease❑ Jaundice❑ Convulsions❑ Hepatitis: ❑ Type A ❑ Headaches❑ Type B ❑ Fainting❑ Type C ❑ Glaucoma❑ Kidney/Bladder Problems ❑ Malignant Hyperthermia❑ Alcohol Use Y / N(High Fever)Amount ___________❑ HIV Virus/AIDS❑ Stomach/Bowel Problem❑ PolioComments:
Drug History: In the last six months have you taken any of the following drugs?❑ Steroids❑ Aspirin❑ Birth Control Pills❑ Arthritis Medication❑ Antibiotics❑ Tranquilizers❑ Asthma Medication❑ Narcotics❑ Anti-Coagulants (blood thinners)❑ Other❑ Insulin or diabetic❑ Thyroid❑ Blood Pressure❑ Heart MedicationPlease list your current medications:Allergy and Reaction:❑ Narcotics:❑ Antibiotics:❑ Anesthetics:❑ Other Drugs:❑ Latex:❑ Non-Medical:Have you had any operations within the last six months? ❑ Yes ❑ No Please list:Please list the operations you have had during your life:Please list the major illnesses you have had during your life:INSURANCE INFORMATIONDO YOU HAVE MEDICARE? MEDICARE ID NUMBER: DO YOU HAVE MEDICAID? STATE ID NUMBER❑ YES ❑ NO ❑ YES ❑ NOINSURANCE COMPANY: INSURANCE COMPANY’S ADDRESS: POLICY NUMBER POLICY OWNER AND OWNER’SRELATIONSHIP TO PATIENT:PPO AFFILIATED? ❑ YES ❑ NOIS THE GROUP INSURANCE THROUGH AN EMPLOYER? IF YES, GIVE EMPLOYER’S NAMEIF NOT LISTED ABOVE:❑ YES ❑ NO EMPLOYER:IS PATIENT COVERED BY ANOTHER INSURANCE COMPANY? IF YES, GIVE NAME OF COMPANY:IF EMPLOYER NOT PREVIOUSLY LISTED, PLEASE GIVEEMPLOYER’S NAME, ADDRESS AND PHONEPOLICY NUMBER:❑ YES ❑ NO INSURANCE COMPANY:IS THIS VISIT DUE TO AN INJURY RESULTINGFROM ACCIDENT?❑ YES ❑ NOACCIDENT INFORMATIONIF YES, HOW DID ACCIDENT OCCUR? (EXPLAIN BRIEFLY)WHERE DID ACCIDENT OCCUR? DATE OF ACCIDENT: WAS ACCIDENT WORK-RELATED? IF YES, GIVE NAME OF EMPLOYER AT TIMEOF ACCIDENT:❑ YES ❑ NO EMPLOYER:COMPENSATION CLAIM NUMBER: (IF APPLICABLE)NAME AND ADDRESS OF COMPENSATION CARRIER:IF AUTOACCIDENT RELATED:NAME AND ADDRESS OF AUTO INSURANCE CO.: POLICY NUMBER NAME OF INSURANCE AGENT AND PHONEPPO AFFILIATED? ❑ YES ❑ NOEverything stated above is true and complete to the best of my knowledge and I agree to notify you of any changes.<strong>Patient</strong>’s Signature:Date: