National Road Map Strategic Plan to Accelerate Reduction of - basics
National Road Map Strategic Plan to Accelerate Reduction of - basics
National Road Map Strategic Plan to Accelerate Reduction of - basics
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
United Republic <strong>of</strong> TanzaniaMinistry <strong>of</strong> Health andSocial WelfareThe <strong>National</strong> <strong>Road</strong> <strong>Map</strong> <strong>Strategic</strong> <strong>Plan</strong>To <strong>Accelerate</strong> <strong>Reduction</strong> <strong>of</strong> Maternal, Newborn andChild Deaths in Tanzania 2008 - 2015One <strong>Plan</strong>Reproductive and Child Health SectionApril, 2008
United Republic <strong>of</strong> TanzaniaMinistry <strong>of</strong> Health and Social WelfareThe <strong>National</strong> <strong>Road</strong> <strong>Map</strong> <strong>Strategic</strong> <strong>Plan</strong>To <strong>Accelerate</strong> <strong>Reduction</strong> <strong>of</strong> Maternal,Newborn and Child Deaths in Tanzania2008 - 2015One <strong>Plan</strong>Reproductive and ChildHealth SectionApril 2008
iiWhen a womanundertakes her biologicalrole <strong>of</strong> becomingpregnant and undergoingchildbirth, the society hasan obligation <strong>to</strong> fulfil herbasic human rights,which include the right <strong>to</strong>life, liberty socialsecurity, maternityprotection and nondiscrimination.
TABLE OF CONTENTSAbbreviations ............................................................................................................................................ ivForeword.................................................................................................................................................... viiAcknowledgements ................................................................................................................................... viiiChapter 1:Overview ................................................................................................................................................... 11.1 Introduction ..................................................................................................................................... 11.2 Initiatives <strong>to</strong> Improve Maternal, Newborn and Child Health in Tanzania ...................................... 11.3 Rationale for the <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> <strong>Accelerate</strong> <strong>Reduction</strong> <strong>of</strong> Maternal,Newborn and Child Deaths in Tanzania.......................................................................................... 2Chapter 2:Situation Analysis <strong>of</strong> Maternal, Newborn and Child Health in Tanzania.................................................. 32.1 Maternal Health............................................................................................................................... 32.2 Newborn Health .............................................................................................................................. 62.3 Child Health ................................................................................................................................... 82.4 Cross Cutting Issues ....................................................................................................................... 11Chapter 3:<strong>Strategic</strong> Framework ................................................................................................................................ 15Chapter 4:Implementation Framework ...................................................................................................................... 18Chapter 5:<strong>Strategic</strong> <strong>Plan</strong> and Activities 2008-2015 .................................................................................................. 24Chapter 6:Moni<strong>to</strong>ring Framework ............................................................................................................................ 47ANNEXESSWOT Analysis ......................................................................................................................................... 57Inputs for Improving MNCH at All Levels ............................................................................................... 71Relevant Policy Documents ...................................................................................................................... 42Most Cost Effective Interventions Based on Evidence <strong>to</strong> Date for <strong>Reduction</strong> <strong>of</strong>Perinatal and Neonatal Mortality............................................................................................................... 83Evidence-Based Interventions that Influence Child Health ...................................................................... 84Evidence-Based Interventions for MNCH ................................................................................................ 85Where Does Tanzania Stand in Terms <strong>of</strong> MNCH Service Delivery?........................................................ 88Essential MNCH Medicines, Equipment and Supplies............................................................................. 90Glossary..................................................................................................................................................... 92REFERENCES .......................................................................................................................................... 93iii
RHMTRTISMSMISNLSRHSTISWOTTAMWATASAFTBATHISTDHSTFNCTFRTGNPTPMNCHTRCHSTSPATTUNFPAUNICEFVVFWBWHOWRATZZRCHRegional Health Management TeamReproductive Tract InfectionSafe MotherhoodSafe Motherhood InitiativeSaving Newborn LivesSexual and Reproductive HealthSexually Transmitted InfectionStrengths, Weaknesses, Opportunities and ThreatsTanzania Media Women AssociationTanzanian Social Action FundTraditional Birth AttendantTanzania HIV/AIDS Indica<strong>to</strong>r SurveyTanzania Demographic and Health SurveyTanzania Food and Nutrition CentreTotal Fertility RateTanzania Gender Networking GroupTanzanian Partnership for Maternal, Newborn and Child HealthTanzania Reproductive and Child Health SurveyTanzania Service Provision AssessmentTetanus ToxoidUnited Nations Population FundUnited Nations Children FundVesico Vaginal FistulaWorld BankWorld Health OrganizationWhite Ribbon Alliance TanzaniaZonal Reproductive and Child Healthvi
FOREWORD<strong>Reduction</strong> <strong>of</strong> maternal, newborn and child deaths is a high priority for all, given the persistently high maternal,newborn and child morbidity and mortality rates over the past two decades in African countries, Tanzaniaincluded. It is one <strong>of</strong> the major concerns addressed by various global and national commitments, as reflectedin the targets <strong>of</strong> the Millennium Development Goals (MDGs), Tanzania Vision 2025, the <strong>National</strong> Strategy forGrowth and <strong>Reduction</strong> <strong>of</strong> Poverty (NSGRP-MKUKUTA), and the Primary Health Services DevelopmentProgram (PHSDP-MMAM), among others.Maternal deaths are caused by fac<strong>to</strong>rs attributable <strong>to</strong> pregnancy, childbirth and poor quality <strong>of</strong> health services.Newborn deaths are related <strong>to</strong> the same issues and occur mostly during the first week <strong>of</strong> life. Child healthdepends heavily on availability <strong>of</strong> and access <strong>to</strong> immunizations, quality management <strong>of</strong> childhood illnessesand proper nutrition. Improving access <strong>to</strong> quality health services for the mother, newborn and child requiresevidence-based and goal-oriented health and social policies and interventions that are informed by best practices.Development <strong>of</strong> this plan for reducing maternal, newborn and child mortality is in line with the tenets <strong>of</strong> theNew Delhi Declaration 2005. Tanzania and other countries committed <strong>to</strong> develop One <strong>National</strong> <strong>Plan</strong> Maternal,Newborn and Child Health MNCH for accelerating the reduction <strong>of</strong> maternal, newborn and child deaths, in order<strong>to</strong> improve coordination, align resources and standardize moni<strong>to</strong>ring. Further support for incorporating childhealth interventions in<strong>to</strong> this plan was voiced by various stakeholders and development partners following theApril 2007 launch <strong>of</strong> the Tanzania Partnership for Maternal, Newborn and Child Health (TPMNCH). The<strong>National</strong> <strong>Road</strong> <strong>Map</strong> <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> <strong>Accelerate</strong> <strong>Reduction</strong> <strong>of</strong> Maternal, Newborn and Child Deaths in Tanzania(2008 – 2015) was subsequently developed as Tanzania’s national response <strong>to</strong> the renewed commitment <strong>to</strong>improve maternal, newborn and child care. The Reproductive and Child Health Section (RCHS) <strong>of</strong> the Ministry<strong>of</strong> Health and Social Welfare (MoHSW), in collaboration with a number <strong>of</strong> different stakeholders, has developedthis strategic plan <strong>to</strong> guide implementation <strong>of</strong> all maternal, newborn and child health interventions in Tanzania.The <strong>National</strong> <strong>Road</strong> <strong>Map</strong> <strong>Strategic</strong> <strong>Plan</strong> stipulates various strategies <strong>to</strong> guide stakeholders for Maternal, Newbornand Child Health (MNCH), these include the Government, development partners, non-governmentalorganizations, civil society organizations, private health sec<strong>to</strong>r, faith-based organizations and communities, inworking <strong>to</strong>gether <strong>to</strong>wards attainment <strong>of</strong> the Millennium Development Goals (MDGs) as well as other regionaland national commitments and targets related <strong>to</strong> maternal, newborn and child healthIt is the expectation <strong>of</strong> the Government, particularly the MoHSW, that all stakeholders will make optimal use<strong>of</strong> this strategic framework <strong>to</strong> support the implementation <strong>of</strong> maternal, newborn and child health interventions,as this is in line with the <strong>National</strong> Health Policy and existing MNCH standards, guidelines and pro<strong>to</strong>cols.The Government highly values your partnership in working <strong>to</strong>wards realization <strong>of</strong> the objectives <strong>of</strong> the <strong>National</strong><strong>Road</strong> <strong>Map</strong> <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> <strong>Accelerate</strong> <strong>Reduction</strong> <strong>of</strong> Maternal, Newborn and Child Deaths. Together, we canimprove the health <strong>of</strong> Tanzanian mothers, babies and children, and build a stronger and more prosperous nation.Pr<strong>of</strong>essor David Homeli Mwakyusa (MP),Minister for Health and Social Welfarevii
ACKNOWLEDGEMENTSThe MoHSW wishes <strong>to</strong> express its gratitude <strong>to</strong> the many individuals and development partners who worked withthe Ministry in the development <strong>of</strong> “The <strong>National</strong> <strong>Road</strong> <strong>Map</strong> <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> <strong>Accelerate</strong> <strong>Reduction</strong> <strong>of</strong> Maternal,Newborn and Child Deaths in Tanzania, 2008 – 2015”. The completion <strong>of</strong> the document is a result <strong>of</strong> extensiveconsultations and collaboration with various stakeholders including the RCHS <strong>of</strong> the MoHSW, developmentpartners, interested organizations as well as committed individuals.The MoHSW would like <strong>to</strong> acknowledge all those stakeholders who contributed in one way or another <strong>to</strong> thesuccessful development <strong>of</strong> the document. The Ministry particularly wishes <strong>to</strong> acknowledge the invaluablecontribution <strong>of</strong> the PMNCH Country Support Working Group: Dr. Nancy Terreri (UNICEF HQ); Dr. CiroFranco (BASICS, USA); and Dr. Koki Agarwal (ACCESS/Jhpiego, USA). The MoHSW also acknowledgesthe contribution <strong>of</strong> the technical group members: Dr. Theresa Nduku Nzomo (WHO/AFRO Harare); Dr. SamMuziki (WHO/AFRO Harare); Dr. Thierry Lambrechts (WHO/HQ); and local Consultants led by Dr. Ali Mzigeand Dr. Rosemary Kigadye. Other national technical experts who contributed in the development include: Dr.Catherine Sanga (RCHS, MoHSW), Dr. Neema Rusibamayila (IMCI, MoHSW), Dr. Georgina Msemo(IMCI/SNL, MoHSW), Dr. Mary Kitambi (EPI, MoHSW); Ms. Lena Mfalila (RCHS/SMI, MoHSW); Dr.Elizabeth <strong>Map</strong>ella (ARH, MoHSW); Ms. Hilda Missano (TFNC); Dr. Rutasha Dadi and Dr. Chilanga Asmani(UNFPA); Dr. Theopista John, Dr. Josephine Obel and Dr. Iriya Nemes (WHO Tanzania); Dr. Asia Hussein(UNICEF, Tanzania); and Maryjane Lacoste (ACCESS/Jhpiego, Tanzania).The Ministry would also like <strong>to</strong> acknowledge Ms. Hassara Maulid (MoHSW) for her secretarial work with theinitial drafts <strong>of</strong> this document.Lastly, the Ministry would like <strong>to</strong> acknowledge technical and financial support provided by EC, WHO, UNFPA,UNICEF and One UN Fund for the development and printing <strong>of</strong> the MNCH strategic plan.Wilson C. MukamaPermanent Secretary, MoHSWviii
CHAPTER 1:OVERVIEWPurpose <strong>of</strong> the documentThis document has been conceived for various purposes. The health <strong>of</strong> the mother is closely linked <strong>to</strong> the healthand survival <strong>of</strong> the child. In addition, the socio-economic level <strong>of</strong> the mother and the maternal health status(HIV/AIDS, malaria, nutrition) has an impact on the survival <strong>of</strong> the child. Thus the primary purpose <strong>of</strong> “OneIntegrated Maternal Newborn and Child Health <strong>Strategic</strong> <strong>Plan</strong>” is <strong>to</strong> ensure improved coordination <strong>of</strong>interventions and delivery <strong>of</strong> services across the continuum <strong>of</strong> care. Another purpose <strong>of</strong> the document is <strong>to</strong>guide implementation across operational levels <strong>of</strong> the system so that policy drawn at national level will becarried out at the district and community levels, with support from the regional level. It is anticipated that a jointstrategy will contribute <strong>to</strong> more integrated implementation, improved services, and ultimately a significantreduction in morbidity and mortality <strong>of</strong> Tanzanian women and children.1.1 IntroductionThe <strong>to</strong>tal population <strong>of</strong> Mainland Tanzania is estimated <strong>to</strong> be 39,384,223 (as <strong>of</strong> July 2007) 1 . Most <strong>of</strong> thepopulation (75%) resides in the rural area. The annual growth rate is 2.9% with life expectancy at birth being54 years for males and 56 years for females 2 .The <strong>to</strong>tal fertility rate in Tanzania has been consistently high over the past ten years and currently stands at 5.7children per woman. There are regional variations with urban-rural disparities, where rural women have higherfertility rates than their urban counterparts 3 .The Maternal Mortality Ratio (MMR) has remained high for the last 10 years 4 without showing any decline andis currently estimated <strong>to</strong> be 578 per 100,000 live births 5 . While significant progress has been made <strong>to</strong> reducechild mortality in Tanzania, the neonatal mortality rate remains high at 32 per 1,000 live births, and accountsfor 47% <strong>of</strong> the infant mortality rate which is estimated at 68 per 1,000 live births.The critical challenges in reducing maternal, newborn and child morbidity and mortality comprise twocategories:(a) Health system fac<strong>to</strong>rs - inadequate implementation <strong>of</strong> pro-poor policies, weak health infrastructure, limitedaccess <strong>to</strong> quality health services, inadequate human resource, shortage <strong>of</strong> skilled health providers, weak referralsystems, low utilization <strong>of</strong> modern family planning services, lack <strong>of</strong> equipment and supplies, weak healthmanagement at all levels and inadequate coordination between public and private facilities.(b) Non health system fac<strong>to</strong>rs- inadequate community involvement and participation in planning,implementation, moni<strong>to</strong>ring and evaluation <strong>of</strong> health services, some social cultural beliefs and practices, genderinequality, weak educational sec<strong>to</strong>r and poor health seeking behaviour.1.2 Initiatives <strong>to</strong> improve maternal, newborn and child health in TanzaniaMaternal and child health services were established in Tanzania in 1974. In 1975 the Expanded Programme <strong>of</strong>Immunization (EPI) was initiated <strong>to</strong> strengthen immunization services for vaccine preventable childhooddiseases. Tanzania adopted the Safe Motherhood Initiative (SMI) in 1989, following the <strong>of</strong>ficial launch <strong>of</strong> theGlobal Safe Motherhood Initiative in 1987 in Nairobi, Kenya. Subsequently, the 1994 International Conferencefor Population and Development (ICPD) emphasized access <strong>to</strong> comprehensive reproductive health services andrights. In response <strong>to</strong> the ICPD <strong>Plan</strong> <strong>of</strong> Action, Tanzania established the Reproductive and Child Health Section(RCHS) within the Ministry <strong>of</strong> Health and developed a <strong>National</strong> Reproductive and Child Health Strategy.1CIA World Fact Book, March 20082Census, 20023TDHS 2004/054Maternal Mortality ratio was 529/100,000 live births in TDHS 19965TDHS 2004/051
In 1996 Tanzania adopted the Integrated Management <strong>of</strong> Childhood Illness (IMCI) approach for reduction<strong>of</strong> childhood morbidity and mortality. Various nutrition interventions have also been adopted including theBaby Friendly Hospital Initiative (BFHI) in 1992, the Code <strong>of</strong> Marketing Breast Milk Substitutes in 1994and Vitamin A Supplementation in 1997. Tanzania developed its <strong>National</strong> Strategy on Infant and Young ChildFeeding and Nutrition in 2005.In Tanzania, specific attempts have been made <strong>to</strong> address maternal, newborn and child health (MNCH)challenges through the <strong>National</strong> Health Policy (revised in 2003), the Health Sec<strong>to</strong>r Reforms and the HealthSec<strong>to</strong>r <strong>Strategic</strong> <strong>Plan</strong> (2003-2007). Furthermore, the Reproductive and Child Health Strategy (2005-2010) andthe <strong>National</strong> <strong>Road</strong> <strong>Map</strong> <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> <strong>Accelerate</strong> the <strong>Reduction</strong> <strong>of</strong> Maternal and Newborn Mortality (2006-2010) were also formulated <strong>to</strong> respond <strong>to</strong> these challenges.Improving MNCH is also a major priority area in the <strong>National</strong> Strategy for Growth and Poverty <strong>Reduction</strong>(NSGPR/MKUKUTA) 2005-2010 which has three major interlinked clusters 6 . One <strong>of</strong> the goals clearly outlinedin the second cluster <strong>of</strong> the strategy is <strong>to</strong> improve the survival, health and well being <strong>of</strong> all children and womenand <strong>of</strong> especially vulnerable groups. Under this goal, there are four operational targets related <strong>to</strong> maternal andchild health for moni<strong>to</strong>ring progress <strong>to</strong>wards achieving MDGs 4 and 5.The Health Sec<strong>to</strong>r Support Programme III (2008 – 2012) will incorporate and address MNCH issues in terms<strong>of</strong> alignment with Government policies, resource mobilization and donor harmonization. The newly initiatedPrimary Health Service Development Programme, (PHSDP/MMAM) 2007 – 2017, will address the delivery<strong>of</strong> health services <strong>to</strong> ensure fair, equitable and quality services <strong>to</strong> the community and is envisioned <strong>to</strong> be thespringboard for achieving good health for Tanzanians.The Tanzania MNCH Partnership was <strong>of</strong>ficially launched in April 2007 <strong>to</strong> re-focus the strategies for reducingthe persistently high maternal, newborn and child mortality rates, through adopting the One <strong>Plan</strong> and settingclear targets for improved MNCH.1.3 Rationale for the <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> accelerate reduction <strong>of</strong> maternal, newborn andchild deaths in TanzaniaAnnually, it is estimated that 536,000 women 7 worldwide die from pregnancy- and childbirth-related conditions,as do 11,000,000 under-fives, <strong>of</strong> which 4.4 million are newborns. Most <strong>of</strong> these deaths occur in Sub SaharanAfrica. Tanzania is one <strong>of</strong> the ten countries contributing <strong>to</strong> 61% and 66% <strong>of</strong> the global <strong>to</strong>tal <strong>of</strong> maternal andnewborn deaths, respectively. In Tanzania, the estimated annual number <strong>of</strong> maternal deaths is 13,000, theestimate for under-fives is 157,000, and newborn deaths are estimated at 45,000 8 . In committing <strong>to</strong> MDGs 4and 5, the Government <strong>of</strong> Tanzania agreed <strong>to</strong> reduce the under-five mortality rate by two-thirds and reduce thematernal mortality ration by three-quarters, by 2015.Maternal, newborn and child outcomes are interdependent; maternal morbidity and mortality impacts neonataland under-five survival, growth and development. Thus service demand and provision for mothers, newbornsand children are closely interlinked. Integration <strong>of</strong> MNCH services demands reorganization and reorientation<strong>of</strong> components <strong>of</strong> the health systems <strong>to</strong> ensure delivery <strong>of</strong> a set <strong>of</strong> essential interventions for women, newbornsand children. A focus on the continuum <strong>of</strong> care replaces competing calls for mother or child, with a focus onhigh coverage <strong>of</strong> effective interventions and integrated MNCH service packages as well as other keyprogrammes such as Safe Motherhood (SM), Family <strong>Plan</strong>ning (FP), Prevention <strong>of</strong> Mother <strong>to</strong> Child Transmission(PMTCT) <strong>of</strong> HIV, Malaria, EPI, IMCI, Adolescent Health and Nutrition. Sustained investment and systematicphased scale up <strong>of</strong> essential MNCH interventions integrated in the continuum <strong>of</strong> care are required.6Cluster 1: Growth and <strong>Reduction</strong> <strong>of</strong> Income Poverty; Cluster 2: Improvedquality <strong>of</strong> life and social well being; Cluster 3: Good governance andaccountability.7Maternal Mortality Estimates 2005, WHO, UNICEF, UNFPA, World Bank8Opportunities for Africa’s Newborns 2006, the Partnership for MNCH2
CHAPTER 2:SITUATIONAL ANALYSIS OF MATERNAL, NEWBORNAND CHILD HEALTH IN TANZANIAIntroductionMaternal, newborn and child health care is one <strong>of</strong> the key components <strong>of</strong> the <strong>National</strong> Package <strong>of</strong> EssentialReproductive and Child Health Interventions (NPERCHI) focusing on improving the quality <strong>of</strong> life forwomen, adolescents and children. The major components <strong>of</strong> the package include:• antenatal care;• care during childbirth;• care <strong>of</strong> obstetric emergencies;• newborn care;• postpartum care;• post abortion care;• family planning;• diagnosis and management <strong>of</strong> HIV/AIDS including PMTCT,other sexually transmitted infections and reproductive tractinfections (STI/RTI);• prevention and management <strong>of</strong> infertility;• prevention and management <strong>of</strong> cancer;• prevention and management <strong>of</strong> childhood illness;• prevention and management <strong>of</strong> immunisable diseases;• nutrition care.In spite <strong>of</strong> the good coverage <strong>of</strong> health facilities, not all components <strong>of</strong> the services are <strong>of</strong> good quality andprovided <strong>to</strong> scale; hence, maternal, newborn and child mortalities remain a major public health challenge inTanzania.2.1 Maternal Health• Antenatal careWhen a womanundertakes her biologicalrole <strong>of</strong> becomingpregnant and undergoingchildbirth, the societyhas obligation <strong>to</strong> fulfilher basic human rightsand that <strong>of</strong> her child.According <strong>to</strong> TDHS (2004/05), 94% <strong>of</strong> pregnant women make at least one antenatal care (ANC) visitand 62% <strong>of</strong> women have four or more ANC visits. The number <strong>of</strong> pregnant mothers in Tanzania makingfour or more ANC visits appears <strong>to</strong> have declined slightly from 70% in 1999 9 . However, the quality <strong>of</strong>antenatal care provided is inadequate. About 65% <strong>of</strong> the women have their blood pressure measured and54% have blood samples taken for haemoglobin estimation and syphilis screening. About 41% haveurine analysis done and only 47% are informed <strong>of</strong> the danger signs in pregnancy.Approximately 80% <strong>of</strong> pregnant women received at least 1 dose <strong>of</strong> tetanus <strong>to</strong>xoid (TT), and 56% <strong>of</strong> womenreceived two or more TT doses 10 . Younger mothers, women in their first pregnancy, women <strong>of</strong> the highereducation and wealth strata and urban women are more likely <strong>to</strong> receive two or more doses <strong>of</strong> TT.Despite high ANC attendance, only 14% <strong>of</strong> pregnant women start ANC during the first trimester as per thenational guidelines. The median number <strong>of</strong> months that women are pregnant at their first visit is 5.4. Onethird<strong>of</strong> women do not seek ANC until their sixth month or later 11 . However, early booking has an advantagefor proper pregnancy information sharing and pregnancy moni<strong>to</strong>ring.9TRCHS 199910TDHS 2004/0511TDHS 2004/053
• Malaria in pregnancyPregnancy alters a woman’s immune response <strong>to</strong> malaria, particularly in the first malaria-exposedpregnancy, resulting in more episodes <strong>of</strong> severe infection and anaemia, all <strong>of</strong> which contribute <strong>to</strong> ahigher risk <strong>of</strong> death. Malaria is estimated <strong>to</strong> cause up <strong>to</strong> 15 % <strong>of</strong> maternal anaemia, which is morefrequent and severe in first pregnancies. Malaria is a significant cause <strong>of</strong> low birth weight which is themost important risk fac<strong>to</strong>r for newborn death and is also a risk fac<strong>to</strong>r for stillbirth.Efforts <strong>to</strong> combat malaria among pregnant mothers are being scaled up. Pregnant women are supposed <strong>to</strong>receive two doses <strong>of</strong> SP for intermittent preventive treatment (IPT) <strong>of</strong> malaria during routine antenatal carevisits. However, according <strong>to</strong> TDHS (2004/05), only 22% <strong>of</strong> pregnant women attending the ANC clinicreceive the complete course <strong>of</strong> IPT, and only 16% use Insecticide Treated Nets (ITNs). Recent data fromthe <strong>National</strong> Malaria Control Programme (NMCP) indicate that the proportion <strong>of</strong> pregnant women sleepingunder ITNs has increased <strong>to</strong> 28% 12 .• Intrapartum careOnly 47% <strong>of</strong> all births in Tanzania occur at health facilities and 46% <strong>of</strong> all births are assisted by a skilledhealth worker. Out <strong>of</strong> the 53% <strong>of</strong> births which take place at home, 31% are assisted by relatives, 19% bytraditional birth attendants (TBAs) and 3% are conducted without assistance. As expected, births <strong>to</strong> womenin the highest wealth quintile are more likely <strong>to</strong> be assisted by a skilled birth attendant (87%) than womenin the lowest quintile (31%) 13 .Emergency obstetric care services are crucial for handling complicated deliveries. Findings from TDHS(2004/05) revealed that only 3% <strong>of</strong> all babies were delivered by caesarean section – this figure is belowthe WHO-recommended standard <strong>of</strong> 5-15%, and is partially due delay in timely referral, lack <strong>of</strong> skilledattendance and functioning blood banks at most hospitals and health centres. About 64.5% <strong>of</strong> publichospitals provide Comprehensive Emergency Obstetric Care (CEmOC), whereas only 5.5% <strong>of</strong> public healthcentres are providing Basic Emergency Obstetric Care (BEmOC) 14 . Furthermore, the referral system hasserious challenges including limited number <strong>of</strong> ambulances; unreliable logistics and communicationsystems; and inadequate community-based facilitated referral systems.• Postnatal carePostnatal care is an important component <strong>of</strong> good maternal and baby health care is not very well utilizedin Tanzania. Eighty-three percent <strong>of</strong> women who delivered a live baby outside the health facility did notreceive a postnatal check-up, and only 13% were examined within two days <strong>of</strong> giving birth asrecommended. Women in the highest income quintiles were more likely <strong>to</strong> receive a timely postnatal checkupcompared <strong>to</strong> those in the lowest quintiles 15 .• Prevention <strong>of</strong> Mother-<strong>to</strong>- Child Transmission <strong>of</strong> HIVThe key <strong>to</strong> ensuring an HIV-free start in life is prevention <strong>of</strong> HIV transmission <strong>to</strong> children by preventingHIV in mothers. PMTCT interventions include testing and counselling for HIV, antiretroviral prophylaxisfor HIV-infected pregnant women and their exposed children, treatment <strong>of</strong> eligible women, counselling andsupport for infant feeding, safer obstetric practices and family planning <strong>to</strong> prevent unintended pregnanciesin HIV-infected women. By September 2007, there were about 1,311 PMTCT sites established withinreproductive and child health (RCH) clinics throughout the country 16 . Additional sites need <strong>to</strong> be established<strong>to</strong> provide services as close <strong>to</strong> the community as possible. The goal, objectives and strategies <strong>to</strong> scale upquality PMTCT services are stipulated in the Health Sec<strong>to</strong>r Strategy for HIV/AIDS (2008-2012).12NMCP-MoHSW 200713TDHS 2004/0514MoHSW, 2006. Situation Analysis <strong>of</strong> Emergency Obstetric Care for SafeMotherhood in Public Health Facilities in Tanzania15TDHS 2004/0516NACP 20074
Integration <strong>of</strong> PMTCT interventions in ANC, nutrition programmes, IMCI and other HIV/AIDSservices enhances opportunities for reducing paediatric HIV and its associated deaths.• NutritionMaternal nutrition during the pre- and postnatal periods is extremely important for the outcome <strong>of</strong>pregnancy as well as infant feeding. A good and adequate balanced diet, as well as vitamin and mineralsupplementation, improves birth outcome and maternal well-being.Underweight status contributes <strong>to</strong> poor maternal health and birth outcomes. Overall, 10% <strong>of</strong> Tanzanianwomen <strong>of</strong> reproductive age (15–49 years) are considered <strong>to</strong> be undernourished, having a Body Mass Index(BMI) <strong>of</strong> less than 18.5. Women living in rural areas are more affected compared <strong>to</strong> those living in urbanareas 17 .Maternal under-nutrition, is <strong>of</strong>ten reflected in the proportion <strong>of</strong> children born with low birth weight (below2.5 kg). Representative data on the prevalence <strong>of</strong> low birth weight babies is not readily available butestimates from UNICEF suggest that 10 % <strong>of</strong> Tanzanian newborns are low birth weight 18 .Pregnant women are particularly vulnerable <strong>to</strong> anaemia due <strong>to</strong> increased requirements for iron and folicacid. According <strong>to</strong> TDHS (2004/05), 48% <strong>of</strong> women aged 15-49 years were found <strong>to</strong> be anaemic, whereas58% <strong>of</strong> pregnant women and 48% <strong>of</strong> breast-feeding mothers were anaemic. Ten percent <strong>of</strong> pregnant women<strong>to</strong>ok iron tablets for at least 90 days, while about half (52%) <strong>to</strong>ok iron tablets for less than 60 days, and 38%did not take iron tablets at all. Haemorrhage is the most frequent cause <strong>of</strong> maternal deaths, and pregnantwomen who are anaemic are more vulnerable <strong>to</strong> postpartum haemorrhage.• Family planningSpacing the intervals between pregnancies can prevent 20 <strong>to</strong> 35% <strong>of</strong> all maternal deaths 19 . However, familyplanning services continue <strong>to</strong> face challenges in meeting clients’ expectations and needs. Despite havinghigh knowledge <strong>of</strong> contraceptives (90%), only 26 % <strong>of</strong> married women use any method <strong>of</strong> contraception,with only 20% using a modern method. The most commonly used methods are injectables (8%), pills (6%)and traditional methods (6%) 20 . Current usage <strong>of</strong> any modern method is higher among sexually activeunmarried women than among married women (41% and 26%, respectively). To be noted is the fact thatthe percentage <strong>of</strong> married women using any method <strong>of</strong> contraception has changed little from the 1999TRCHS. The <strong>to</strong>tal demand for FP among married women is 50%, while 22% have an unmet need for FP 21 .Fac<strong>to</strong>rs contributing <strong>to</strong> low contraceptive prevalence include low acceptance <strong>of</strong> modern FP methods, erraticsupplies <strong>of</strong> contraceptives with limited range <strong>of</strong> choices, limited knowledge/skills <strong>of</strong> providers andprovider’s bias affecting informed choice. The situation is worsened by limited spousal communication,inadequate male involvement and lack <strong>of</strong> adolescent-friendly health services and misconceptions aboutmodern family planning methods. In an attempt <strong>to</strong> improve access <strong>to</strong> family planning services, communitybasedprogrammes are being implemented in 46 mainland districts; however, this represents less than half<strong>of</strong> all districts in the country.• Challenges in accessing quality careData from TDHS (2004/05) revealed that the major barriers perceived by women in accessing deliveryhealth services include lack <strong>of</strong> money (40%), long distance <strong>to</strong> health facility (38%), lack <strong>of</strong> transport (37%),and unfriendly services (14%). The high rate <strong>of</strong> home deliveries is also attributable <strong>to</strong> a malfunctioningreferral system, inadequate capacity <strong>of</strong> health facilities in terms <strong>of</strong> available space, skilled attendants andcommodities, and other socio-cultural aspects affecting the pregnant women. Additional fac<strong>to</strong>rs includegender inequalities in decision-making and access <strong>to</strong> resources at household-level.17TDHS 2004/0518State <strong>of</strong> the World’s Children Report, 200819Singh S. et al. 2004. Adding it Up: The Benefits <strong>of</strong> Investing in Sexual andReproductive Health Care. Washing<strong>to</strong>n D.C. and New York: The Alan GuttmacherInstitute and UNFPA.20TDHS 2004/0521TDHS 2004/055
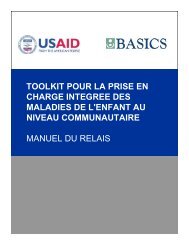
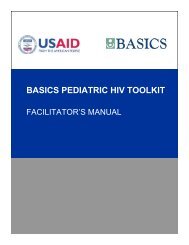
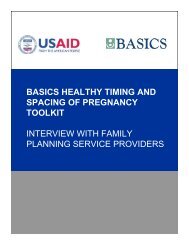
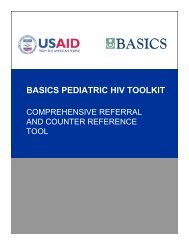
• Maternal morbidity and mortalityAccording <strong>to</strong> TDHS (2004/05), the maternal mortality ratio is estimated at 578/100,000 live births. Majordirect causes <strong>of</strong> maternal mortality include obstetric haemorrhage, obstructed labour, pregnancy inducedhypertension, sepsis and abortion complications.Figure 1: Direct Causes <strong>of</strong> Maternal DeathsSource: The World Health Report, 2005It is estimated that abortion complications contribute <strong>to</strong> about 20% <strong>of</strong> maternal deaths worldwide 22 . InTanzania, induced abortion is illegal hence the actual magnitude <strong>of</strong> the problem is not known. However,several attempts have been made <strong>to</strong> document the severity <strong>of</strong> the issue – in Hai District, for example, it wasreported that nearly a third <strong>of</strong> maternal deaths are related <strong>to</strong> unsafe abortion (Mswia et al, 2003 23 ). Postabortion care (PAC) services can significantly reduce maternal mortality due <strong>to</strong> unsafe abortions; however,only 5% <strong>of</strong> health facilities in Tanzania currently provide this service 24 .Indirect causes leading <strong>to</strong> poor maternal health outcomes are malaria, anaemia, and HIV/AIDS. Withspecific regard <strong>to</strong> HIV, prevalence in Tanzania is estimated <strong>to</strong> be 7% in adults aged 15-49 years, withprevalence among women being higher (8%), compared <strong>to</strong> 6% among men 25 .2.2 Newborn Health• Newborn morbidity and mortalityTanzania is among those countries that have had success in reducing child mortality, but there has been nomeasurable progress in reducing neonatal deaths. The neonatal mortality rate was 40.4 per 1,000 live birthsin 1999 and 32 per 1,000 live births in 2004/05. Up <strong>to</strong> 50% <strong>of</strong> neonatal deaths occur in the first 24 hours<strong>of</strong> life, with over 75% <strong>of</strong> them arising in the first week <strong>of</strong> life. Newborn mortality is a sensitive indica<strong>to</strong>r<strong>of</strong> the quality <strong>of</strong> care provided during the antenatal period, delivery and immediate postnatal period.According <strong>to</strong> modelled estimates for Tanzania, 79% <strong>of</strong> newborn deaths are due <strong>to</strong> three main causes:infections including sepsis/pneumonia (29%), birth asphyxia (27%); and complications <strong>of</strong> preterm birth(23%) (Figure 2). Sepsis was the most common cause <strong>of</strong> death noted in a study conducted in Mbulu and22The World Health Report, 200523Mswia et al, 2003. Community Based Moni<strong>to</strong>ring <strong>of</strong> Safe Motherhood in UnitedRepublic <strong>of</strong> Tanzania24TDHS 2004/0525THIS, 2003/046
Hanang districts <strong>of</strong> rural northern Tanzania 26 . Many <strong>of</strong> these conditions are preventable and closelylinked <strong>to</strong> the absence <strong>of</strong> skilled birth attendance at delivery. Eighty-six percent (86%) <strong>of</strong> neonataldeaths in Tanzania are also low birth weight, many <strong>of</strong> whom are preterm. On average in Tanzania, newborn deaths are 67% higher in the poorest families as compared <strong>to</strong> the wealthier families, and themajority <strong>of</strong> deaths occur in rural areas 27 .Figure 2: Estimated Causes <strong>of</strong> Neonatal DeathsSource: 2004/5 TDHSLow birth weight (birth weight less than2500 grams) and preterm birth (less than36 completed weeks <strong>of</strong> gestation) <strong>to</strong>gethercontribute <strong>to</strong> 28% <strong>of</strong> neonatal deathsglobally 28 . The recent Tanzania DHS(2004/05) asked mothers <strong>to</strong> estimatewhether their infant was “very small,small, average, or large”. They were alsoasked <strong>to</strong> report the actual birth weight, if itwas known. The TDHS data cite aneonatal mortality <strong>of</strong> 86% in the five-yearperiod prior <strong>to</strong> the survey among“small/very small” newborns. However,other all-cause mortality estimates indicatea mortality rate <strong>of</strong> 23% for preterm infants(who are most likely also <strong>of</strong> low birthweight.).• Continuum <strong>of</strong> careIt is important <strong>to</strong> address the coverage <strong>of</strong> interventions along the continuum <strong>of</strong> care from pregnancy,neonatal period, infancy and childhood. It is critical <strong>to</strong> note that the coverage <strong>of</strong> essential interventions islowest at the time when needed most: that is, during child birth and the early neonatal period whenmore than 50% <strong>of</strong> maternal and newborn deaths occur (Figure 3).Figure 3: Coverage <strong>of</strong> Interventions along the Continuum <strong>of</strong> Care in TanzaniaSource: Opportunities for Africa’s Newborns, Lawn JE, et al 200626Hinderraker et al, 200327TDHS, 2004/0528Lancet Neonatal Survival Series, 20057
• Other challengesFurthermore, quality newborn and child care faces other challenges including poor health infrastructureand referral for neonatal care, child care and poor skills <strong>of</strong> service providers related <strong>to</strong> inadequateincorporation <strong>of</strong> neonatal content in pre- and in-service training curricula. A recent study conducted in Dares Salaam in 2005 showed that none <strong>of</strong> the primary and secondary level health facilities was providingbasic/essential newborn care.2.3 Child Health• ImmunizationThe Expanded Programme <strong>of</strong> Immunization (EPI) has performed well over thepast decade with immunization coverage <strong>of</strong> 71% for all vaccines for children 12-23 months (TDHS, 2004/05). Currently the policy is <strong>to</strong> provide each child withone dose <strong>of</strong> BCG, four doses <strong>of</strong> OPV, three doses <strong>of</strong> DTP-HB and one dose <strong>of</strong>measles vaccine. As expected, children born <strong>to</strong> mothers in the lowest wealthquintile are less likely <strong>to</strong> be fully immunized than those born <strong>to</strong> mothers in thehighest wealth quintile.Only 20% <strong>of</strong> womenreceive Vitamin Asupplementationwithin 2monthsafter childbirth.Pneumonia is one <strong>of</strong> the major contribu<strong>to</strong>rs <strong>to</strong>wards under five mortality and it accounted for 21.1% <strong>of</strong>under five deaths in 2006. The Lancet series on child survival identifies Hib vaccine as an intervention thatcould reduce under five mortality due <strong>to</strong> pneumonia by 20%. <strong>Plan</strong>s are under way <strong>to</strong> consider introduction<strong>of</strong> Hib and pneumococcal vaccines in the national policy.Measles outbreaks are still happening despite high measles routine immunization coverage (above 80% inalmost all districts). Tanzania has been implementing the Reaching Every District (RED) strategy <strong>to</strong>improve immunization coverage for all antigens including measles but also conducting periodic measlessupplementation immunization campaigns after every three years.The achievement <strong>of</strong> TT and polio vaccines is evident by the significant reduction in neonatal tetanus deathsand polio cases. The last polio case in the country was identified in 1996; however, there is a high risk <strong>of</strong>wild polio virus importation from polio-endemic countries. In this regard polio eradication initiatives need<strong>to</strong> be sustained until polio is eradicated. Tanzania is close <strong>to</strong> achieving Maternal Neonatal Tetanus (MNT)elimination; however, there are still some pockets in high risk districts. Implementation <strong>of</strong> MNT eliminationstrategies will focus more in high risk districts.• Integrated Management <strong>of</strong> Childhood IllnessCase management <strong>of</strong> common childhood illness is a key step <strong>to</strong> reducing child mortality. Appropriatemanagement <strong>of</strong> malaria, pneumonia, diarrhoea and dysentery can reduce under five mortality by 5, 6, 15and 3% respectively. The IMCI strategy has been implemented at scale in Tanzania from 1996 with alldistricts implementing at different levels <strong>of</strong> coverage. Tanzania was part <strong>of</strong> an IMCI inter-country evaluationand the results were encouraging, but issues around quality <strong>of</strong> care and supervision were noted 29 .IMCI has been found <strong>to</strong> be an effective delivery strategy for various child survival interventions and hascontributed <strong>to</strong> a 13% mortality reduction over a two-year period in those districts in Tanzania where it hasbeen implemented 30 . Management <strong>of</strong> diarrhoeal disease has been improved <strong>to</strong> include low osmolarity oralrehydration solution (ORS) and zinc supplementation. The IMCI clinical guidelines have been updatedaccordingly and have also included the newborn, HIV/AIDS and strengthened nutrition.• Prevention and management <strong>of</strong> malaria29MCE Report, 200530MCE Report, 20058
Malaria contributes <strong>to</strong> 23% percent <strong>of</strong> under five mortality in Tanzania 31 . Use <strong>of</strong> ITNs contributes <strong>to</strong>7 percent reduction <strong>of</strong> overall deaths among under-fives 32 . Only 47% <strong>of</strong> under fives in Tanzania sleepunder ITNs 33 . ITNs are distributed through the health system by vouchers, as well as by free distribution<strong>of</strong> long lasting insecticide treated nets (LLINs) through catch up campaigns and replacement campaigns <strong>to</strong>replace worn out ITNs in the period 2008 – 2012 when appropriate.Malaria management has been improved using the combination therapy <strong>of</strong> Artemether and Lumefantrine(ALu). The MoHSW is training district focal persons for both IMCI and malaria and regional focalpersons for coordination <strong>of</strong> malaria and IMCI interventions. Since a good proportion <strong>of</strong> caretakers seektreatment outside <strong>of</strong> the health facility, the MoHSW is also training the private sellers <strong>to</strong> dispense basicessential drugs <strong>to</strong> the community through Accredited Drug Dispensing Outlets (ADDOs).• Care seekingCare seeking for sick children needs <strong>to</strong> be improved. The TDHS 2004/05 showed that among children withsymp<strong>to</strong>ms prior <strong>to</strong> the survey, half <strong>of</strong> the children (57%) with symp<strong>to</strong>ms <strong>of</strong> Acute Respira<strong>to</strong>ry Infection(ARI) or fever and 47% <strong>of</strong> children with diarrhoea were taken <strong>to</strong> a health facility. Those in urban areas weremore likely than rural children <strong>to</strong> be taken <strong>to</strong> the health facility. However, a vast majority <strong>of</strong> the childrenwith diarrhoea (70%) were also given some form <strong>of</strong> ORT and 54% were given a solution prepared fromORS.In Tanzania, although access <strong>to</strong> health services is good, many people seek care when it is <strong>to</strong>o late or notat all. Attention should be paid <strong>to</strong> the fact that only 57% <strong>of</strong> under-fives receive anti- malarial treatmentwithin 24 hours <strong>of</strong> developing symp<strong>to</strong>ms. In this perspective the MoHSW has always prioritizedcommunity IMCI (c-IMCI) as a way <strong>of</strong> identifying danger signs among under-fives and when <strong>to</strong> seekcare.• NutritionNutrition indica<strong>to</strong>rs for under-fives have shown some improvement over the years but undernutrition is stillwidely prevalent in Tanzania. Stunting, underweight status and wasting among children aged 0-59 monthshave reduced from 44%, 29% and 5% in 1999 <strong>to</strong> 38%, 22% and 3% respectively 34 . Anaemia is also highlyprevalent among under-fives with 72% <strong>of</strong> all 6-59 months children being anaemic. The main causes <strong>of</strong>anaemia are nutritional deficiency, intestinal worms and malaria.Optimal breastfeeding can reduce under-five mortality by up <strong>to</strong> 13% 35 . The majority <strong>of</strong> Tanzanian babiesare breastfed, for a median duration <strong>of</strong> 21 months. Fifty-four percent (54%) are breastfed up <strong>to</strong> two years.However, initiation <strong>of</strong> breastfeeding within one hour <strong>of</strong> birth is only 59% and the exclusive breastfeedingrate (0-5 months <strong>of</strong> age) is estimated <strong>to</strong> be 41% 36 . Early complementary feeding is common with 39% <strong>of</strong>infants below 3 months already introduced <strong>to</strong> complementary foods 37 . About 12% <strong>of</strong> infants are notcomplemented at the age <strong>of</strong> 6-7 months. Furthermore feeding frequency during complementation is <strong>to</strong>o low(about 2-3 feeds a day), nutrient density is low and the preparation and feeding practices are <strong>of</strong>ten unsafe 38 .Children 2 – 5 years old are fed family foods; however, feeding frequency and nutrient density are alsoinadequate in this group.Coverage <strong>of</strong> health workers trained on infant and young child feeding is low and only 68 have beenaccredited as baby friendly 39 . Training on Essential Nutrition Actions (Vitamin A supplementation, exclusivebreastfeeding, complementary feeding, iodine) is in the early stages <strong>of</strong> implementation. Coverage <strong>of</strong>appropriate facility management <strong>of</strong> severe malnutrition is still low and community management <strong>of</strong> severe31Country Health System Fact Sheet 2006, WHO32Lancet Child Survival Series, 200333TNVS Survey, 200734TDHS, 2004/0535Lancet Child Survival Series, 200336TDHS, 2004/0537TDHS, 2004/0538TDHS, 2004/0539Communication with TFNC, April 20089
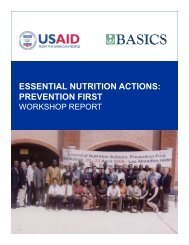
malnutrition has not been implemented.Vitamin A deficiency is the leading cause <strong>of</strong> preventable blindness in children and raises the risk <strong>of</strong> diseaseand death from severe infections. Vitamin A supplementation twice a year has been estimated by the WorldBank (1993) <strong>to</strong> be one <strong>of</strong> the most cost-effective health interventions, yet in Tanzania the coverage is only20% 40 . Currently the biannual Vitamin A supplementation campaign is the main strategy <strong>to</strong> combat vitaminA deficiency and it is estimated that the coverage is 85% 41 .Iodine deficiency during pregnancy has a great impact on physical and mental development <strong>of</strong> the foetusand is related <strong>to</strong> poor educational outcomes and productivity. In Tanzania the prevalence <strong>of</strong> goitre amongschool children is estimated at 7% 42 . Salt iodation is the most effective strategy for the control <strong>of</strong> iodinedeficiency. However, currently only 75% <strong>of</strong> households consume iodated salt 43 .• Child morbidity and mortalityAlthough the most recent Demographic Health Survey (TDHS, 2004/5) has shown decline in under-fiveand infant mortality by 24% and 31% respectively <strong>to</strong> 112 and 68 per 1,000 live births, the infant and underfivemortality rates in Tanzania are still unacceptably high. Every year about 154,000 children die beforereaching their fifth birthday. In addition, as expected, the mortality rates are highest in the lowest, secondand middle wealth quintiles (137, 156 and 147, respectively) as compared <strong>to</strong> the highest wealth quintile(93).Although under-fives constitute about 16% <strong>of</strong> the population, they account for 50% <strong>of</strong> the <strong>to</strong>tal mortalityburden for all ages. Most <strong>of</strong> these deaths are due <strong>to</strong> preventable diseases. Malaria, pneumonia, diarrhoea,HIV/AIDS and neonatal conditions account for over 80% <strong>of</strong> deaths. Malnutrition is a contribu<strong>to</strong>ry fac<strong>to</strong>r<strong>to</strong> about fifty percent <strong>of</strong> all deaths.The under-five mortality rate for children whose mothers were less than 20 years <strong>of</strong> age when they gavebirth is 157/1,000, versus 120/1,000 for children whose mothers were in their twenties. Children whose birthorder is seven or higher have a mortality rate <strong>of</strong> 151/1000, compared with 121/1,000 for those born secondor third.40TDHS, 2004/0541Helen Keller International, 2004/0542TFNC, 2004/0543NBS and TDHS 2004/0510
Figure 4: Causes <strong>of</strong> Deaths for Children Aged less than Five Years,in the Year 2006*Source: WHO, 2006• AdolescentsAdolescents constitute a significant proportion <strong>of</strong> the population, at about 31% 44 . A high percentage <strong>of</strong>adolescents are sexually active and practice unsafe sex. Consequently, the majority <strong>of</strong> them are highlyvulnerable <strong>to</strong> SRH problems that include adolescent pregnancy and early child bearing, the complicationsarising from unsafe abortion, and STIs including HIV/AIDS 45 . In Tanzania, more than half <strong>of</strong> young womenunder the age <strong>of</strong> 19 are pregnant or already mothers, and the perinatal mortality rate is significantly higherfor young women under the age <strong>of</strong> 20 (at 56 per 1,000 pregnancies) than it is for women aged 20-29 (at 39per 1,000 pregnancies), and older women aged 30-39 (32 per 1,000 pregnancies). Obtaining permission <strong>to</strong>access services is a greater obstacle for young women age 15-19 than for their older counterparts. Youngwomen age 15-19 also cited not knowing where <strong>to</strong> go as a barrier <strong>to</strong> accessing services 46 . Hence the need<strong>to</strong> invest in adolescent sexual reproductive health (SRH) services, including HIV/AIDS is paramount giventhe fact that SRH needs are not only basic human rights but that adolescents forma significant section <strong>of</strong> the population and bear a disproportionate burden <strong>of</strong>disease with regards <strong>to</strong> reproductive ill-health and HIV prevalence2.4 Cross-Cutting Issues• <strong>National</strong> Policies and GuidelinesTanzania has mainstreamed maternal, newborn and child survival in<strong>to</strong> its nationalhealth policy. The services for maternal, newborn and child health are exemptedfrom cost sharing. However, the exemption policy faces difficulties in itsimplementation at lower level due <strong>to</strong> lack <strong>of</strong> clarity on how <strong>to</strong> effect theexemption mechanisms.Good governance isparticipa<strong>to</strong>ry,consensus-oriented,accountable,transparent,equitable, andfollows the rule <strong>of</strong>law.Several national policy documents have been developed targeting improvement <strong>of</strong> reproductive and childhealth services, which include maternal and newborn health. However, certain pr<strong>of</strong>essional regulationsand legislations contribute <strong>to</strong> compromised implementation <strong>of</strong> the policies.The MoHSW and partners have developed several clinical national pro<strong>to</strong>cols; however, there is need <strong>to</strong> havean integrated pro<strong>to</strong>col. Although training on RCH interventions has been ongoing nationally through theMoHSW, district councils and NGOs, the quality <strong>of</strong> the trainings, transfer skill <strong>to</strong> practice and follow up44Census, 200245<strong>National</strong> Adolescent Health and Development Strategy, 2004-200846TDHS, 2004/0511
supervision are still challenges that need <strong>to</strong> be addressed. <strong>National</strong> capacity development is alsocompromised by poor working environment; low geographical coverage; weak integration <strong>of</strong> gender andhuman rights issues.• Community Mobilization and ParticipationCommunity-based maternal, newborn and child health interventions are crucial in complementing servicesat the health facility level. Since the Alma Ata Declaration on Primary Health Care (PHC) in 1978 and thesubsequent health sec<strong>to</strong>r reforms initiated in 2000, there has been increased focus on communityparticipation in the delivery <strong>of</strong> health services. Community participation has been strengthened further bylocal Government reforms, which interface the health sec<strong>to</strong>r within the overall Government policy <strong>of</strong>decentralization by devolution. In Tanzania communities play an increasingly important role in thedevelopment <strong>of</strong> the Comprehensive Council Health <strong>Plan</strong>s (CCHPs) through the decentralised districtplanning framework. Further community participation has been strengthened through communityrepresentation on the Council Health Service Boards and Health Facility Governing Committees.Though a few districts have been successful in involving communities in the process <strong>of</strong> planning,moni<strong>to</strong>ring and evaluation <strong>of</strong> health services, their participation is still compromised by the low capacity<strong>of</strong> health boards and health facility governing committees and inadequate outreach activities.Other challenges include weak partnership between clients and service providers, which is compoundedby low awareness <strong>of</strong> clients’ and service providers’ rights and obligations; low public awareness <strong>of</strong>reproductive health matters such as management <strong>of</strong> pregnancy, newborn care and child care and relatedcomplications, socio-cultural barriers; gender inequalities, low women empowerment; and myths andmisconceptions <strong>of</strong> various health-related issues.• Water, Sanitation and HygieneThe proper sanitation, hygiene and use <strong>of</strong> safe water are vital in containing the spread <strong>of</strong> water borne andwater related diseases. The TDHS (2004/0) also showed that during the two weeks that preceded the survey13% <strong>of</strong> children under-five had diarrhoea. The rate was highest among children 6-11 months old (25%).Less than half <strong>of</strong> all households are within 15 minutes <strong>of</strong> their drinking water supply. Nineteen percent <strong>of</strong>urban households have water piped in<strong>to</strong> their compound and 33% from neighbours’ taps while ruralhouseholds primarily rely on public wells both open and protected (43%) and rivers and streams (18%) fortheir drinking water. About a half <strong>of</strong> households (47%) have improved <strong>to</strong>ilets.Improved household water, sanitation and promotion <strong>of</strong> key hygiene behaviour changes will be critical <strong>to</strong>complement and strengthen the essential health package. Various community-based interventions are beingimplemented <strong>to</strong> improve hygiene and sanitation such as Participa<strong>to</strong>ry Hygiene and SanitationTransformation (PHAST) and c-IMCI.• Human ResourcesHuman resources for health is a crisis in the country with only one-third <strong>of</strong> posts filled. The situation isworse especially for the lower-level health facilities, where dispensaries and health centres haveshortages <strong>of</strong> 65.6% and 71.6% respectively 47 . This has a major impact on maternal, newborn andchildcare, most significantly recognizable in the lack <strong>of</strong> skilled attendants during childbirth. Efforts arebeing made by MoHSW <strong>to</strong> recruit additional skilled health providers but challenges remain such as poorskills mix; non-attractive incentive and salary packages; poor motivation; inadequate performanceassessment; rewarding systems; retention <strong>of</strong> staff especially in remote and hard <strong>to</strong> reach areas;.47MoHSW, 200612
• Moni<strong>to</strong>ring and EvaluationMoni<strong>to</strong>ring and evaluation play a critical management function by assessing whether implementation<strong>of</strong> programmes proceeds according <strong>to</strong> plan and leads <strong>to</strong> the desired outcomes. Moni<strong>to</strong>ring <strong>of</strong> maternal,newborn and childhood health in Tanzania has been implemented through HMIS, annual RCH reports,TDHS, Tanzania Service Provision Assessment (TSPA), maternal and perinatal death review reports,Infectious Disease Week Ending Report (IDWE) and other health facility and household surveys. Some <strong>of</strong>the limitations in reporting maternal, newborn and child deaths are the problem <strong>of</strong> incorrect and incompleterecording, proper case definition, data management, source <strong>of</strong> information (i.e. facility versus communitybaseddata) and methods <strong>of</strong> estimation. Further, the use <strong>of</strong> process indica<strong>to</strong>rs is critical for evaluation <strong>of</strong>implementation. However, process indica<strong>to</strong>rs are not widely used at all levels. In order <strong>to</strong> achieve coherentand useful data for moni<strong>to</strong>ring and evaluation <strong>of</strong> maternal, newborn and child health in Tanzania it is crucial<strong>to</strong> strengthen the current health information system <strong>to</strong> address the information gaps for maternal, newbornand child care.• Advocacy and Resource MobilizationAlthough there has been advocacy and commitment at different levels in addressing maternal, newborn andchild health issues, the meagre budget allocation <strong>to</strong> the health sec<strong>to</strong>r has been a hindrance <strong>to</strong> effectiveimplementation <strong>of</strong> the Essential RCH Package. During FY 2005/06, the health budget allocation was Tsh.453.2 billion, which is 10.1% <strong>of</strong> the <strong>to</strong>tal Government budget, below the recommended Abuja target <strong>of</strong>15%. Due <strong>to</strong> other competing health priorities such as malaria, HIV/AIDS and tuberculosis, the budgetallocation for reproductive and child health is still limited.Opportunities and synergies for addressing maternal, newborn and child health include introduction andscaling up <strong>of</strong> the TASAF II initiative, which will enable communities <strong>to</strong> address their infrastructuredevelopment needs, logistics and human capacity gaps, in order <strong>to</strong> provide appropriate maternal, newbornand child care interventions and services. The existence <strong>of</strong> the Joint Rehabilitation Fund, District DemandDriven Initiative, GAVI and Global Fund for AIDS, TB and Malaria, also provide opportunities for thedistricts <strong>to</strong> strengthen maternal, newborn and child health interventions.• Partnerships and CoordinationMaternal, newborn and child health interventions need <strong>to</strong> be addressed in the context <strong>of</strong> a multi-sec<strong>to</strong>ralapproach. Partnerships, resources and more effective and coordinated programmes at all levels areincreasingly needed <strong>to</strong> reach the MDGs.Due <strong>to</strong> other competing health priorities such asMalaria, HIV/AIDS and Tuberculosis, Reproductiveand Child Health budget is still limited. This hasaffected implementation <strong>of</strong> comprehensiveinterventions on maternal, family planning andnewborn care.13
14<strong>Strategic</strong> <strong>Plan</strong>
CHAPTER 3:STRATEGIC FRAMEWORKMaternal, Newborn and Child Health <strong>Strategic</strong> <strong>Plan</strong>The development <strong>of</strong> the MNCH <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> <strong>Accelerate</strong> <strong>Reduction</strong> <strong>of</strong> Maternal, Newborn and Child Deathsis a response <strong>to</strong> the New Delhi Declaration (April 2005) which urged all countries <strong>to</strong> develop strategies <strong>to</strong>reducing the persistently high rates <strong>of</strong> maternal, newborn and child deaths in order <strong>to</strong> reach MDG 4 and 5. Thisplan is expected <strong>to</strong> contribute <strong>to</strong> the achievement <strong>of</strong> MKUKUTA and MMAM goals and targets, as well asobjectives and targets <strong>of</strong> other existing national programmes, interventions and strategies, which focus onimproving MNCH.This strategic plan aims <strong>to</strong> address maternal, newborn and child health and accelerate mortality reduction in anintegrated manner addressing the continuum <strong>of</strong> care. The rationale for taking the integrated approach relies ona number <strong>of</strong> fac<strong>to</strong>rs:1. Specific interventions delivered in a specific time frame have multiple benefits.2. Linking interventions in packages can reduce costs, facilitate greater efficiency in training, moni<strong>to</strong>ring andsupervision, and strengthen supply systems.3. Integration <strong>of</strong> services increases uptake and promotes continuation <strong>of</strong> positive behaviours4. Integration maximizes programme achievements3.1. VisionA healthy and well-informed Tanzanian population with access <strong>to</strong> quality MNCH services, which areaffordable, sustainable and accessible through an effectively functioning health system.3.2. MissionTo promote, facilitate and support in an integrated manner, the provision <strong>of</strong> comprehensive, high impactand cost-effective MNCH services, in order <strong>to</strong> accelerate reduction <strong>of</strong> maternal, newborn and childmorbidity and mortality.3.3. GoalTo accelerate the reduction <strong>of</strong> maternal, newborn and childhood morbidity and mortality, in line withMDGs 4 and 5, by 2015.3.4. ObjectivesThe following are the objectives for the MNCH <strong>Strategic</strong> <strong>Plan</strong>, which should be met by the end <strong>of</strong> the year2015.3.4.1. To reduce maternal mortality from 578 <strong>to</strong> 193 per 100,000 live births.3.4.2. To reduce neonatal mortality from 32 <strong>to</strong> 19 per 1000 live births3.4.3. To reduce under-five mortality from 112 <strong>to</strong> 54 per 1000 live births3.5 Operational targets <strong>to</strong> be achieved by 20151. Increased coverage <strong>of</strong> births attended by skilled attendants from 46% <strong>to</strong> 80%.2. Increased immunization coverage <strong>of</strong> DTP-HB 3 and Measles vaccine <strong>to</strong> above 90% in 90% <strong>of</strong> thedistricts.15
3. New EPI vaccines introduced (Hib, Pneumoccocal, Human Papilloma Virus (HPV) and Rota Virusvaccines).4. Reduced stunting and underweight status among under-fives from38% and 22% <strong>to</strong> 22% and 14%,respectively.5. Increased exclusive breast feeding coverage from 41% <strong>to</strong> 80 %6. PMTCT services provided <strong>to</strong> at least 80% <strong>of</strong> pregnant women, their babies and families.7. 90% <strong>of</strong> sick children seeking care at health facilities appropriately managed.8. Increased coverage <strong>of</strong> under-fives sleeping under ITNs from 47% <strong>to</strong> 80%.9. 75% <strong>of</strong> villages have community health workers <strong>of</strong>fering MNCH services at community level.10. Increased modern contraceptive prevalence rate from 20% <strong>to</strong> 60%11. Increased coverage <strong>of</strong> CEmOC from 64% <strong>of</strong> hospitals <strong>to</strong> 100% and <strong>of</strong> BEmOC from 5% <strong>of</strong> healthcentres and dispensaries <strong>to</strong> 70%12. Increased proportion <strong>of</strong> health facilities <strong>of</strong>fering Essential Newborn Care <strong>to</strong> 75%.13. Increased antenatal care attendance for at least 4 visits from 64% <strong>to</strong> 90%14. Increased number <strong>of</strong> health facilities providing Adolescent friendly reproductive health services <strong>to</strong>80%3.6.Strategies3.6.1. Advocacy and resource mobilization for MNCH goals and agenda in order <strong>to</strong> promote, implement,and scale up evidence-based and cost-effective interventions, and allocate sufficient resources <strong>to</strong> achievenational and international goals and targets;3.6.2. Health System strengthening and capacity development at all levels <strong>of</strong> the health sec<strong>to</strong>r and ensuringquality service delivery <strong>to</strong> achieve high population coverage <strong>of</strong> MNCH interventions in an integratedmanner;3.6.3. Community mobilization and participation <strong>to</strong> improve key maternal, newborn and child care practices,generate demand for services and increase access <strong>to</strong> services within the community;3.6.4. Fostering partnership <strong>to</strong> implement promising interventions among Government (as lead), donors,NGOs, the private sec<strong>to</strong>r and other stakeholders engaged in joint programming and co-funding <strong>of</strong> activitiesand technical reviews;3.6.5.Information, education and communication /behavioural change communication (IEC/BCC).Promotion <strong>of</strong> appropriate reproductive health behaviours is critical in accelerating reduction <strong>of</strong> maternal,newborn and child deaths. With implementation <strong>of</strong> the MNCH <strong>Strategic</strong> <strong>Plan</strong>, the use <strong>of</strong> IEC/BCCapproaches for positive behaviour adoption and create demand for quality maternal, newborn and child care.3.7.Guiding PrinciplesThe following principles will guide the planning and implementation <strong>of</strong> the MNCH <strong>Strategic</strong> <strong>Plan</strong> in order<strong>to</strong> ensure effectiveness, ownership and sustainability <strong>of</strong> the initiative in Tanzania:• Continuum <strong>of</strong> Care: Ensuring provision <strong>of</strong> the continuum <strong>of</strong> care from pregnancy, childbirth andneonatal period through childhood and across all services levels from family/household, community,and primary facility <strong>to</strong> referral care.16
• Integration: All efforts will be made <strong>to</strong> implement the proposed priority interventions at variouslevels <strong>of</strong> the health system in a coherent and effective manner that is responsive <strong>to</strong> the needs <strong>of</strong>the mother, the newborn and the child.• Evidence-based approach: ensuring that the interventions promoted through the plan are based onpriority needs, up-<strong>to</strong>-date evidence, and are cost-effective.• Complementarities: Building on existing programmes by taking in<strong>to</strong> account the comparativeadvantages <strong>of</strong> different stakeholders in the planning, implementation and evaluation <strong>of</strong> MNCHprogrammes.• Partnership: Promoting partnership, coordination and joint programming among stakeholdersincluding the regional secretariat, district councils, private sec<strong>to</strong>r, faith-based sec<strong>to</strong>r, academia,pr<strong>of</strong>essional organizations, civil society organizations, as well as communities, in order <strong>to</strong> improvecollaboration and maximize on the available limited resources by avoiding duplication <strong>of</strong> effort• Addressing underlying causes <strong>of</strong> high mortality: Taking a multi-sec<strong>to</strong>ral and partnership approach<strong>to</strong> address the underlying causes <strong>of</strong> maternal, newborn and child death such as, transport, nutrition, foodsecurity, water and sanitation, education, gender equality and women empowerment <strong>to</strong> ensuresustainability.• Shared responsibility: The family/household is the primary institution for supporting holistic growth,development and protection <strong>of</strong> children. The community has the obligation and the duty <strong>to</strong> ensure thesurvival and health <strong>of</strong> mothers and children and ensuring that every child grows <strong>to</strong> its full potential.The state, on the other hand, has the responsibility for developing a conducive legislation and publicservice provision for survival, growth and development.• Division <strong>of</strong> labour for increased synergy: Defining roles and responsibilities <strong>of</strong> all players andpartners in the implementation, moni<strong>to</strong>ring and evaluation <strong>of</strong> the activities for increased synergy.• Appropriateness and relevance: Interventions must rely on a clear understanding <strong>of</strong> the status andlocal perceptions <strong>of</strong> MNCH in the country.• Transparency and accountability: Promoting a sense <strong>of</strong> stewardship, accountability and transparencyon the part <strong>of</strong> the Government as well as stakeholders for enhanced sustainability.• Equity and accessibility: Supporting scaling-up <strong>of</strong> cost-effectiveinterventions that promote equitable access <strong>to</strong> quality healthservices with greater attention <strong>to</strong> the youth, poor and mostvulnerable children and groups, especially in rural and underservedareas.• Phased planning, and implementation: Promotingimplementation in clear phases with timelines and benchmarks thatenable re-planning for better results. Building and strengtheningexisting health infrastructures will be a priority.For majority <strong>of</strong> women,especially the poor anddisadvantaged groups,the pathway <strong>to</strong> safemotherhood is blockedby the underlyingfac<strong>to</strong>rs that lead <strong>to</strong>• Human rights and gender in health: The right <strong>to</strong> life is a basichuman right. Mainstreaming gender throughout the programmeand adopting a human rights approach as the basis <strong>of</strong> planning andimplementation is important. It is also critical <strong>to</strong> understand thatchildren’s rights are important human rights and therefore need <strong>to</strong> bedelays in accessingappropriate care.respected at all times in order <strong>to</strong> uphold the dignity that enables child development and participation.17
CHAPTER 4:IMPLEMENTATION FRAMEWORK4.1 IntroductionThe MNCH <strong>Strategic</strong> <strong>Plan</strong> has been designed <strong>to</strong> accelerate the reduction <strong>of</strong> maternal newborn and child deathswith the aim <strong>of</strong> attaining MDGs 4 and 5 by 2015. It should be implemented jointly by all stakeholders as a multisec<strong>to</strong>ralstrategy for comprehensive reproductive and child health care.Good governance is a critical element for successful implementation <strong>of</strong> the strategic plan, right from central level<strong>to</strong> the grass root level. Good governance is participa<strong>to</strong>ry, consensus-oriented, accountable, transparent, equitable,and follows the rule <strong>of</strong> law. It assures that corruption is minimised, and voices <strong>of</strong> the most vulnerable in societyare heard in decision making.The MNCH <strong>Strategic</strong> <strong>Plan</strong> will be implemented in collaboration with relevant stakeholders, which includerelated Ministries and agencies, development partners, the civil society, community based organisations,pr<strong>of</strong>essional associations, faith-based organisations, voluntary agencies, and the private sec<strong>to</strong>r, among others.4.2. Specific Roles and Responsibilities <strong>of</strong> Different Levels4.2.1 Ministry <strong>of</strong> Health and Social Welfare (<strong>National</strong> Level)The MoHSW will mobilise resources and advocate for reduction <strong>of</strong> maternal, newborn and child deaths. It willalso be responsible for the overall technical leadership, guidance and advice on the implementation andmoni<strong>to</strong>ring <strong>of</strong> the strategic plan. The following will be the specific roles and responsibilities <strong>of</strong> the variousDirec<strong>to</strong>rates <strong>of</strong> the MoHSW.i) Direc<strong>to</strong>rate <strong>of</strong> Policy and <strong>Plan</strong>ning will ensure adequate budget allocation for MNCH and mainstreaming<strong>of</strong> MNCH indica<strong>to</strong>rs in<strong>to</strong> policy frameworks. The HMIS Unit will facilitate the moni<strong>to</strong>ring <strong>of</strong> all indica<strong>to</strong>rsfrom routine data collection systems including community-based data through Community BasedManagement Information System (CBMIS).ii) Direc<strong>to</strong>rate <strong>of</strong> Hospital Services will ensure availability <strong>of</strong> essential drugs, supplies, equipment anddiagnostics by facilitating efficient procurement and distribution <strong>to</strong> all levels <strong>of</strong> service delivery.iii) Direc<strong>to</strong>rate <strong>of</strong> Human Resource and Development. The training department will be responsible <strong>to</strong> reviewand update pre- and in-service curricula <strong>to</strong> ensure relevant issues for MNCH are adequately addressed.The department will also promote accelerated training <strong>of</strong> mid-level cadres in order <strong>to</strong> increase the availablenumber <strong>of</strong> skilled health workers, and will facilitate effective development, recruitment and deploymen<strong>to</strong>f skilled health workers at health units <strong>to</strong> address the human resource crisis 48 . This will be done incollaboration with the Prime Minister’s Office - Regional Administration and Local Government(PMORALG) , the President’s Office - Public Service Management (POPSM) and Ministry <strong>of</strong> Financeand Economic Affairs..iv) Direc<strong>to</strong>rate <strong>of</strong> Preventive Services will supervise and coordinate all activities with respect <strong>to</strong> allsections under its charge for the realisation <strong>of</strong> the strategic plan objectives. It will particularly undertakethe following activities:• Advocate for the implementation <strong>of</strong> the MNCH <strong>Strategic</strong> <strong>Plan</strong> by• Coordinate the implementation, moni<strong>to</strong>ring <strong>of</strong> MNCH activities• Involve and collaborate with various stakeholders at all levels for planning and implementation <strong>of</strong> theMNCH <strong>Strategic</strong> <strong>Plan</strong>48MMAM18
• Facilitate capacity development at national, zonal, regional and district levels by developingpro<strong>to</strong>cols and training packages for MNCH• Design and develop IEC/BCC materials with stakeholders and disseminate them <strong>to</strong> the intendedusers• In collaboration with the procurement unit, facilitate procurement <strong>of</strong> communication equipment andits installation at hospital, health centres and selected dispensaries• Identify and propose disaggregated indica<strong>to</strong>rs and update moni<strong>to</strong>ring data collection <strong>to</strong>ols <strong>to</strong> includeprocess indica<strong>to</strong>rs for EmOC, newborn care, nutrition, postnatal care, child care and Adolescent healthincluding functioning moni<strong>to</strong>ring and evaluation systems and userfirendly data base• Review and harmonize existing CBMIS, in collaboration with the district councils• Facilitate integration <strong>of</strong> nutrition actions in maternal, newborn and child care programmes.• Promote research on MNCH including FP and nutrition• Capacity developemnt for the implementation <strong>of</strong> maternal, newborn, child and Adolescent health4.2.2 Zonal Level• Disseminate the MNCH <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> their respective districts• Support capacity development in MNCH in the districts• Zonal Training Centres and ZRCH coordina<strong>to</strong>r maintain effective partnership with key stakeholders(MoHSW- RCHS, RHMTs, CHMTs, NGOs, CBOs etc)• Conduct and build research capacity in the regions and districts4.2.3 Regional Level• Provide technical support for effective planning and implementation <strong>of</strong> the integrated MNCH activities inthe CCHPs.• Coordinate, moni<strong>to</strong>r and supervise MNCH activities in the region• Technical support for training and ensuring quality in service provision• Support districts in analysis and utilization <strong>of</strong> MNCH data and disseminate/report <strong>to</strong> the national level4.2.4 District Level• Disseminate MNCH <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> all stakeholders in the District Council including NGOs, FBOs andother private sec<strong>to</strong>r partners.• Incorporate MNCH activities in<strong>to</strong> the CCHPs• Coordinate and supervise all MNCH activities planned and implemented by all stakeholders in the district• Provide technical support for quality MNCH services• Capacity development for facility and community MNCH interventions• Follow up maternal, perinatal, neonatal and child death reviews at health facility (dispensaries, healthcentres, district hospitals, regional hospitals, as well as voluntary agencies and private hospitals) andcommunity levels• Council Management Teams and District Health Boards <strong>to</strong> ensure adequate resource allocation forimplementation and moni<strong>to</strong>ring <strong>of</strong> the MNCH interventions4.2.5 Health Facility (Dispensary, Health Centre and Hospital)• Incorporate MNCH activities in<strong>to</strong> facility health plans• Provide quality MNCH services• Implement quality improvement approaches such as Quality Improvement and Recognition Initiative(QIRI), Pay for Performance, Integrated Management Cascade and Collaborative Approach• Ensure timely availablity <strong>of</strong> essential equipment, supplies and drugs for service MNCH provision• Conduct maternal, perinatal, neonatal and child death reviews, involving the community• Health facility committees <strong>to</strong> moni<strong>to</strong>r and ensure quality MNCH service provision• Provide technical and supportive supervision <strong>to</strong> community interventions19
4.2.6 CommunityThe Village Government and Ward Development Committee through the Primary Health Care (PHC)committee and health facility governing committee will be responsible for supervision and implementation<strong>of</strong> MNCH activities in their areas. Other responsibilities include:• Facilitate development and moni<strong>to</strong>ring <strong>of</strong> community MNCH action plans• Mobilize the community <strong>to</strong> participate in community interventions• Establish and/or strengthen CBMIS• Leverage community resources for the implementation <strong>of</strong> MNCH interventions4.2.7 Roles and Responsibilities <strong>of</strong> other MinistriesKey Ministries should be involved <strong>to</strong> ensure that the reduction <strong>of</strong> maternal, newborn and child mortality ishigh on their agenda. These include Ministry <strong>of</strong> Finance and Economic Affairs (MoFEA), PMORALG,Ministry <strong>of</strong> Community Development Gender and Children (MoCDGC), Ministry <strong>of</strong> Education andVocational Training (MoEVT), Ministry <strong>of</strong> Agriculture, Food Security and Cooperatives (MoAFSC),Ministry <strong>of</strong> Labour, Employment and Youth Development (MoLEYD), Ministry <strong>of</strong> InfrastructureDevelopment (MoID), Ministry <strong>of</strong> Communication, Science and Technology (MoCST), and Ministry <strong>of</strong>Information, Culture and Sports (MoICS).i) Ministry <strong>of</strong> Finance and Economic Affairs• Give priority <strong>to</strong> health, especially MNCH, in budget guidelines for allocation <strong>of</strong> resources• Increase financial resources for health and especially implementation <strong>of</strong> MNCH activities as guided by theMNCH <strong>Strategic</strong> <strong>Plan</strong>ii) Prime Minister’s Office Regional Administration and Local Government• Provide technical support <strong>to</strong> regions and councils for planning and implementation <strong>of</strong> CCHPs• Mobilize funds <strong>to</strong> support implementation <strong>of</strong> CCHPs including CBMIS• Support infrastructural development, rehabilitation and maintenance <strong>to</strong> improve access for MNCH services• Include maternal, perinatal, newborn and child health indica<strong>to</strong>rs in the national health sec<strong>to</strong>r moni<strong>to</strong>ringand evaluation framework.iii) Ministry <strong>of</strong> Education and Vocational Training• Promote universal access <strong>to</strong> education, especially education for girls and women• Review and update components <strong>of</strong> MNCH and SRH in various school and pre-service curricula incollaboration with MoHSW particluarly on provision <strong>of</strong> adolescent friendly servicesiv) Ministry <strong>of</strong> Agriculture, Food Security and Cooperation• Promote food security at household, community, district and national levelsv) Ministry <strong>of</strong> Community Development, Gender and Children• Support community development extension workers <strong>to</strong> supervise and identify problems and derive solutionsfor MNCH in the local context• Facilitate the establishment <strong>of</strong> community mechanisms <strong>to</strong> support emergency transportation for MNCHservices• Advocate for gender issues <strong>to</strong> improve MNCH decision-making at all levels• Support and promote rights-based approach <strong>to</strong> programming for MNCH• Advocate for revision <strong>of</strong> laws, legislations and policies <strong>to</strong> improve MNCH• Promote parental support for adolescents <strong>to</strong> access information and health servicesvi) Ministry <strong>of</strong> Infrastructure Development• Improve road networks <strong>to</strong> facilitate access <strong>to</strong> services at primary and referral levels, especially in ruralareas where the majority <strong>of</strong> Tanzanians live20
vii) Ministry <strong>of</strong> Labour, Employment and Youth Development• In collaboration with the MoHSW and the MoCDGC, develop a Youth Communication Strategy• Develop capacity for life skills and livelihood young people• Advocate for adoption <strong>of</strong> maternity protection conventions (ILO, convention 183)viii) Ministry <strong>of</strong> Communication, Science and Technology• Promote the development, availability <strong>of</strong> and access <strong>to</strong> appropriate technology <strong>to</strong> support MNCH serviceprovisionix) Ministry <strong>of</strong> Information, Culture and Sports• Promote positive RH behaviours including early health care seeking for MNCH services.• Disseminate information aimed at promoting early care seeking behaviour for MNCH and use <strong>of</strong>preventive care services4.2.8 Roles and Responsibilities <strong>of</strong> Development Partners• Provide technical and financial support for the coordination, planning, implementation, capacitydevelopemnt and moni<strong>to</strong>ring and evaluation <strong>of</strong> MNCH services• Advocate for increased global and national commitment <strong>to</strong> the reduction <strong>of</strong> maternal, newborn and childmorbidity and mortality• Mobilise and allocate resources for the implementation <strong>of</strong> MNCH interventions4.2.9 Roles and Responsibilities <strong>of</strong> Civil Society Organisations (NGOs, FBOs, CBOs, Pr<strong>of</strong>essionalAssociations)• Advocate for the rights <strong>of</strong> women and children.• Forge partnership with different stakeholders including political leaders <strong>to</strong> promote MNCH• Implement community based strategies <strong>to</strong> promote healthy behaviours during pregnancy, child birth, postpartum period, childhood and adolescence• Complement governement efforts in the provision <strong>of</strong> quality MNCH services• Disseminate the MNCH <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> accelerate the reduction <strong>of</strong> maternal, newborn and child morbidityand mortality• Mobilize and allocate resources for implementation <strong>of</strong> the MNCH <strong>Strategic</strong> <strong>Plan</strong>4.2.9 Roles and Responsibilities <strong>of</strong> Private Sec<strong>to</strong>r• Complement Government efforts in the provision <strong>of</strong> quality MNCH services• Invest in commodites and supplies for MNCH interventions4.2.10 Role <strong>of</strong> Training and Research Institutions• Undertake relevant MNCH research <strong>to</strong> provide evidence for policy directions and implementation guidance• Review and update curricula <strong>to</strong> ensure relevant MNCH issues are adequately addressed• Provide technical advice and updates on current developments on MNCH and SRH <strong>to</strong> policy makers4.3.Key Strategies <strong>to</strong> be Implemented4.3.1. Advocacy and Resource MobilizationIn advocating for improved MNCH, the following issues will be emphasized:• Increased budget allocation for MNCH interventions including FP and nutrition. The target is <strong>to</strong> mobilizeresources from internal and external sources in order <strong>to</strong> complement the Government’s efforts <strong>to</strong>wardsreducing maternal, newborn and childhood deaths• Revision <strong>of</strong> laws, legislations and policies that hinder effective provision <strong>of</strong> maternal, newborn andchildcare services• Improved production, employment, deployment and retention <strong>of</strong> a skilled health work force at all levels21
4.3.2. Health Systems Strengthening and Capacity DevelopmentHealth system strengthening for MNCH involves improving; service delivery; health workforce;information; medical products, vaccines and technologies; financing; and leadership/ governance as well asmanaging interactions among them, so that more equitable and sustained improvements across services andhealth outcomes will be achieved.4.3.2.1 Capacity development• The strategy aims <strong>to</strong> increase the number <strong>of</strong> skilled health work force required, as well as the knowledgeand skills <strong>of</strong> existing service providers and supervisors so that quality care is provided.• User friendly pro<strong>to</strong>cols will be developed/reviewed and the mechanisms for making essential commoditiesfor MNCH, including FP, available will be strengthened• Basic and comprehensive EmOC as well as essential newborn services will be strengthened at dispensaries,health centres and hopsitals• Skills for planning and management <strong>of</strong> MNCH services, including FP and Nutrition, will be imparted <strong>to</strong>the CHMTs.• Necessary infrastructure, logistics and equipment support will be provided for the effective delivery <strong>of</strong> thecomprehensive MNCH packages.4. 3. 2.2 Referral systems• Referral systems will be improved <strong>to</strong> ensure equitable access <strong>to</strong> quality MNCH services through makingappropriate means <strong>of</strong> transportation available and improve linkages between community and referralfacilities• Communications equipment (e.g., radio calls and mobile phones) will be installed in hospitals, healthcentres and selected dispensaries.• Community emergency committees will be established and oriented <strong>to</strong> emergency preparedness andresponse.• Maternity waiting homes will be established where appropriate.4.3.2.3 Research, Moni<strong>to</strong>ring and Evaluation• Capacity building for conducting operational research will be strengthened at all levels. Districts will beencouraged <strong>to</strong> identify research priority areas according <strong>to</strong> their needs.Essential moni<strong>to</strong>ring <strong>to</strong>ols and indica<strong>to</strong>rs will be developed and mainstreamed in<strong>to</strong> the HMIS. Data will begenerated periodically <strong>to</strong> moni<strong>to</strong>r the miles<strong>to</strong>nes and improvement <strong>of</strong> services provided at health facilities.• Periodic reviews and reporting will be carried out every two years <strong>to</strong> assess progress. A mid-term reviewwill be conducted between 2010 – 2011, and an end <strong>of</strong> term review will be conducted in 2015 <strong>to</strong> report onthe attainment <strong>of</strong> the MDGs.4.3.3. Community Mobilization• Communities will be mobilised <strong>to</strong> participate fully in initiatives aimed at improving maternal, newborn andchild care by:• Educating and sensitising them on community-based MNCH interventions• Mobilizing resources at the village level for MNCH including emergency referral as well as building andstrengthening health facilities.22
• Orienting the facility governing committees <strong>to</strong> the MNCH <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> ensure effectiveimplementation <strong>of</strong> the plan at the health facility and community levels• Re-institutionalizing quarterly village health days4.3.4: Information Education and Communication (IEC)/Behaviour Change Communication (BCC)• Use <strong>of</strong> IEC/BCC approaches will be intensified <strong>to</strong>wards adoption <strong>of</strong> positive behaviours for quality MNCHincluding nutrition and adolescent sexual reproductive health.• The IEC/BCC activities will target community-based initiatives particularly in addressing birthpreparedness, with an emphasis on birth planning for individual couples, transport in case <strong>of</strong> emergency,and promotion <strong>of</strong> key MNCH practises at the household and community levels.4.3.5: Fostering Partnership and AccountabilityEffective implementation <strong>of</strong> the MNCH <strong>Strategic</strong> <strong>Plan</strong> will entail fostering and establishing strategicpartnerships <strong>to</strong> improve coordination and collaboration between communities, partners and among programmesas well as galvanizing resources for long term sustainable actions for MNCH.• Coordinate regular planning, implementation, moni<strong>to</strong>ring and evaluation <strong>of</strong> MNCH activities <strong>to</strong> assessprogress <strong>to</strong>wards attainment <strong>of</strong> the MDGsThe goal <strong>of</strong> this <strong>National</strong><strong>Strategic</strong> <strong>Plan</strong> is <strong>to</strong> acceleratethe reduction <strong>of</strong> maternal,newborn and child mortality andmorbidity, and the attainment <strong>of</strong>the MDGs 4 and 5 in Tanzania.23
CHAPTER 5: STRATEGIC PLAN AND ACTIVITIES: 2008 -2015<strong>Strategic</strong>Objective/OutputActivitiesTimeframe08 09 10 11 12 13 14 15Process Indica<strong>to</strong>rs Responsible Person ResourcesNeeded inUS dollars5.1 Advocacy and Resource Mobilisation5.1.1.1Cost the package for5.1.1Budget allocationfor health,particularly formaternal,newborn & childhealth includingFP and nutritionincreased at alllevels.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Budget formaternal, newbornand child healthincluding FP andnutrition increasedby 50% by 2015.maternal, newborn and childhealth including FP and nutritionby establishing:• Unit cost per intervention perarea;• Operational costs;• Recurrent costs.5.1.1.2. Conduct Advocacy formaternal newborn and child carethrough Deliver Now forWomen and Children campaign5.1.1.3 Develop an advocacypackage targeting the following:MoHSW, PMO-RALG, MoFEAand other relevant line ministries,partners, parliamentarians (usingREDUCE/ALIVE and othermaterials) <strong>to</strong> mobilise human andfinancial resources fromGovernment, political andcommunity leaders.5.1.1.4 Identify focal personsamong members <strong>of</strong> parliamentand other influential leaders <strong>to</strong>advocate for maternal, newbornand child health.X X X The package formaternal, newborn andchild health includingFP and nutrition costedand in place.XXXXXX X XXXX X XXNumber <strong>of</strong> advocacyevents conductedannuallyAdvocacy packagedeveloped anddisseminated.Numbers <strong>of</strong> influentialleaders advocating formaternal, newborn andchild health identified.MoHSW(RCHS, Policy and<strong>Plan</strong>ning)Development PartnersResearch InstitutionsMoHSW(RCHS, HEU)Development PartnersCSOsPr<strong>of</strong>essionalAssociations Academicand ResearchInstitutionsMediaMoHSW (RCHS)Development PartnersCSOs150,000400,000-5.1.1.5 Provide support <strong>to</strong> MNCHchampion and other focal persons.X XX X X X X X80,00024
<strong>Strategic</strong>Objective/Output25Activities5.1.1.6 Conduct advocacy meetings <strong>to</strong>policy/decision - makers on theMNCH <strong>Strategic</strong> <strong>Plan</strong>, <strong>to</strong> supportimplementation <strong>of</strong> the strategy at thecentral, regional and district levels.5.1.1.7 Lobby with the government forsubsidy on ITNs in order <strong>to</strong> ensureequitable access <strong>to</strong> the materials by allvulnerable groups.5.1.1.8 Establish and conduct Mother-Baby Day/ Week, annually at alllevels through:• Public awareness campaigns(media/rallies/debates).• Programme communicationdevelopment.5.1.1.9 Advocate for bi-annual Childand village health days at all levelsthrough :• Public awareness campaigns• Programme Communicationdevelopment5.1.1.10 Sensitize RHMTs and CHMTs<strong>of</strong> the importance <strong>of</strong> including childand village health days in the CCHPs5.1.1.11 Train, establish and supportMedia Groups <strong>to</strong> report on MNCHTimeframe08 09 10 11 12 13 14 15Process Indica<strong>to</strong>rs Responsible Person ResourcesNeeded inUS dollarsXXXXXXXXNumber <strong>of</strong> advocacymeetings conducted.MoHSW (RCHS)CSOsPr<strong>of</strong>essional AssociationsDevelopment Partners880,000XXXXXXXXSubsidy policy on ITN for allvulnerable group in place.X X X X X X X X Mother-Baby Day/Weekcommemorated.XXXXXXXXXXXXXXXXProportion <strong>of</strong> villagesconducting semi annualchild health day.Proportion <strong>of</strong> CCHPs withbudget allocation for VillageHealth Days.MoHSW, MinisterialDepartment Agencies(MDAs)MediaDevelopment PartnersCHMTsPr<strong>of</strong>essional AssociationsCSOsMoHSW, MDAsMediaRHMTsCHMTsNGOs,Pr<strong>of</strong>essional AssociationsVillage GovernmentsDevelopment Partners500,000700,000XXXXXXXXNumber <strong>of</strong> establishedmedia groups.300,000
<strong>Strategic</strong> Objective/Output5.1.2Regulations, lawsand policies <strong>to</strong>support effectiveimplementation <strong>of</strong>maternal, newbornand Child healthreviewed.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Number <strong>of</strong> regulationsapproved by regula<strong>to</strong>rybodies.Number <strong>of</strong> lawsapproved by regula<strong>to</strong>rybodies.26STRATEGIC PLAN AND ACTIVITIES: 2008 -2015ActivitiesTimeframe08 09 10 11 12 13 14 15Process Indica<strong>to</strong>rs Responsible Person Resources Needed inUS dollars5.1.2.1 Review regulations andlegislations related <strong>to</strong> theprovision <strong>of</strong> maternal, newbornand child care.X X X Number <strong>of</strong>regulations, laws andpolicies <strong>to</strong> supporteffective provision <strong>of</strong>quality maternal,newborn and childcare reviewed.MoHSW (RCHS)Pr<strong>of</strong>essionalAssociationsDevelopment PartnersMedical CouncilNurses & MidwivesCouncil CSOs110,0005.1.2.2 Advocate for review andadoption <strong>of</strong> laws such as theMarriage Act <strong>of</strong> 1970, and theSexual Offence Special ProvisionAct (SOSPA) <strong>of</strong> 1998 thatinfluence maternal, newborn andchild health.X X Laws affectingmaternal andnewborn healthreviewed andadopted.MoHSW,Ministry <strong>of</strong> Justice andConstitutional AffairsMCDGC, MDAs,Development Partners,Pr<strong>of</strong>essionalAssociationsCSOs120,000
<strong>Strategic</strong> Objective/Output5.1.3Implementation <strong>of</strong>the exemptionpolicy for maternaland child healthstrengthened.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Exemption policyeffectivelyimplemented.27Activities5.1.3.1 Advocate for exemptionpolicy on MNCH <strong>to</strong> be effectedin voluntary and public healthfacilities ( Service Agreement)TimeframeProcess Indica<strong>to</strong>rs08 09 10 11 12 13 14 15X X Proportion <strong>of</strong> publicand voluntary healthfacilities implementingthe Exemption Policy.Responsible PersonMoHSW (RCHS & Policyand <strong>Plan</strong>ning)Health pr<strong>of</strong>essionalassociationsPrivate sec<strong>to</strong>rCSOsResourcesNeeded inUS dollars50,000
<strong>Strategic</strong> Objective/Output5.1.4Employment,deployment andretention <strong>of</strong> skilledhealth workers at alllevels <strong>of</strong> careimproved.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Number <strong>of</strong> skilledhealth workersincreased <strong>to</strong> 100% <strong>of</strong>established need by201528STRATEGIC PLAN AND ACTIVITIES: 2008 -2015ActivitiesTimeframe08 09 10 11 12 13 14 15Process Indica<strong>to</strong>rs Responsible Person ResourcesNeeded inUS dollars5.1.4.1 Advocate for review <strong>of</strong> the1999 Human ResourcesEstablishment (and 2006 proposedrevision) in line with skilledattendance requirements formaternal, newborn and child care.5.1.4.2 Advocate for recruitment anddeployment <strong>of</strong> skilled healthworkers at all levels <strong>of</strong> care.X X Human ResourceEstablishment <strong>of</strong>MoHSW (1999)reviewed.X X X X X X X X Proportion <strong>of</strong>districts withappropriatenumber <strong>of</strong> skilledhealth workers.MoHSW (DHR, DAP)PMO-RALGPO- Public ServiceManagementMoFEAHealth pr<strong>of</strong>essionalassociations, CSOsDevelopment PartnersMoHSWPMO-RALGHealth pr<strong>of</strong>essionalassociationsDevelopment PartnersCSOs84,00054,0005.1.4.3 Advocate <strong>to</strong> the Government<strong>to</strong> motivate skilled health workersby providing a package <strong>of</strong> incentivesin order <strong>to</strong> ensure optimumperformance.X X X X X X X X Types <strong>of</strong> Incentivepackage providedby theGovernment at alllevels.Proportion <strong>of</strong>districts providingincentive packages.MoHSW (DHR, DAP,Policy & <strong>Plan</strong>ning)PMO-RALGPO-Public ServiceManagementMoFEAHealth pr<strong>of</strong>essionalassociationsCSOs76,000
<strong>Strategic</strong>Objective/OutputActivitiesTimeframe08 09 10 11 12 13 14 15Process Indica<strong>to</strong>rs Responsible Person Resources Needed inUS dollars5.2. Health Systems Strengthening and Capacity Development5.2.1Knowledge andskills <strong>of</strong>supervisors andservice providerson maternal,newborn andchild careincluding FP andnutritionincreased.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Maternal, newbornand child healthservice providedaccording <strong>to</strong>standards.5.2.1.1 Review/develop user-friendlypro<strong>to</strong>cols for antenatal care, postnatalcare, newborn and child care, EmOC,FP and nutrition. Specific activitiesinclude:• Develop/adapt/review anddisseminate CommunityMaternal, Newborn and ChildCare packages• Develop/adapt/reviewstandards job aides and <strong>to</strong>ols forMNCH service provision• Develop/adapt/review anddisseminate Nutrition Packagesincluding ENA, SAM, IYCF/BFHI• Review EPI guidelines forinclusion <strong>of</strong> new vaccines• Adaptation <strong>of</strong> Essential NewbornCare (ENC) and Kangaroo Mothercare guidelines (KMC)• Adaptation and adoption <strong>of</strong> thenew child growth standards andchartsX X X X Pro<strong>to</strong>cols onantenatal care,EmOC, newborncare, severemalnutrition,growth moni<strong>to</strong>ring,child care andpostnatal caredeveloped andadopted by theMoHSW.MoHSW (RCHS,DHS HEU)DevelopmentPartnersHealth pr<strong>of</strong>essionalassociationsCSOs647,00029
<strong>Strategic</strong>Objective/Output30STRATEGIC PLAN AND ACTIVITIES: 2008 -2015ActivitiesTimeframe08 09 10 11 12 13 14 15Process Indica<strong>to</strong>rs ResponsiblePerson5.2.1.2 Support pre-service traininginstitutions <strong>to</strong> provide updated andcompetency-based teaching onmaternal, newborn and child careincluding FP and nutrition (LSS-EmOC, ENC, KMC FANC, PAC, FP,newborn care, nutrition, BFHI, IYCF,SAM, PMTCT , IMCI, ETAT, ReferralCare Package, Immunization) by:• Updating pre-service curricula <strong>to</strong>address current changes inmaternal, newborn and childcare including FP and nutrition• Developing and providing anorientation package and othereducational materials <strong>to</strong> tu<strong>to</strong>rs andclinical precep<strong>to</strong>rs.• Update and standardizeknowledge, clinical and teachingskills <strong>of</strong> tu<strong>to</strong>rs and clinicalprecep<strong>to</strong>rs at medical, nursing andparamedical schools.• Provide schools and clinicalpractice sites with necessaryteaching and clinical practicematerials and equipment5.2.1.3 Update knowledge and skills<strong>of</strong> supervisors on maternal, newbornand child care including FP, nutritionand supervisory skills (LSS-EmOC,ENC, KMC, FANC, PAC, FP,newborn care, nutrition, BFHI, IYCF,PMTCT , IMCI, ETAT, Referral CarePackage, immunization)X X X X X X X X 1000 tu<strong>to</strong>rs/clinicalprecep<strong>to</strong>rs fromvarious institutionsupdated onmaternal andnewborn careincluding FP andnutrition.All preserviceMNCH curricularcomponentsupdated.All preserviceinstitutionsprovided withnecessary teachingmaterials,equipment andsupplies.X X X X X X X X 910 CHMTmembers (130Councils), and 147Zonal and RHMTmembers, allupdated insupervisory skills.MoHSW (RCHS,PMTCT, TFNC)Human ResourceDevelopmentand TrainingHealth TrainingInstitutionsRegula<strong>to</strong>rybodiesPrivateinstitutionsCSOsDevelopmentPartnersMoHSW (RCHS,DRH)DevelopmentPartnersCSOsResources Needed inUS dollars980,0002,750,000
<strong>Strategic</strong>Objective/Output31Activities5.2.1.4 Update knowledge and skills<strong>of</strong> service providers on maternal,newborn and child care includingFP and nutrition (LSS-EmOC, ENC,KMC, FANC, PAC, PNC, FP, ENA,IMCI, ETAT, BFHI, IYCF, PMTCT,SAM, immunization) and link theinterventions <strong>to</strong> malaria, HIV/AIDs,and STIs control programmes.5.2.1.5 Review maternal, perinataland child deaths at all levels (facility& community).• Train service provider onmaternal, perinatal and childdeath reviews• Develop a system <strong>to</strong> review childdeaths• Employ/train the communityhealth workers <strong>to</strong> conduct verbalau<strong>to</strong>psiesProduce weekly, monthly, quarterlyand annual summary reports <strong>of</strong>maternal, perinatal and child deathreviewsTimeframe08 09 10 11 12 13 14 15Process Indica<strong>to</strong>rs ResponsiblePersonX X X X X X X X Number <strong>of</strong> serviceproviders trained inMNCH servicedelivery.MoHSW (RCHS),District Councils,and DevelopmentPartners.CSOsPrivate institutionsHealthpPr<strong>of</strong>essionalassociationsX X X X X X X X Proportion <strong>of</strong> healthfacilities withmaternal, perinataland child deathsreview reports.Proportion <strong>of</strong>facilities with healthworkers trained inmaternal, perinataland child deathreview.MoHSW (RCHS)PMORALGMoCDGCRHMTsCHMTsCMTsResources Needed inUS dollars7,900,0001,000,000
STRATEGIC PLAN AND ACTIVITIES: 2008 -2015<strong>Strategic</strong> Objective/OutputActivitiesTimeframe08 09 10 11 12 13 14 15ProcessIndica<strong>to</strong>rs5.2.2<strong>Plan</strong>ning andmanagementcapacity formaternal andnewborn careincluding FP andnutritionstrengthened.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Relevant sec<strong>to</strong>r(Ministry <strong>of</strong> Finance,MoHSW) allocating15% <strong>of</strong> the Healthbudget for maternaland newborn care.5.2.2.1 Train CHMT/RHMTs onevidence-based planning 1 in order <strong>to</strong>ensure that strategic interventions onmaternal newborn and child careincluding FP and nutrition areincorporated in the CCHP andimplemented.X X X X X X X X Proportion <strong>of</strong>CHMTs andRHMT’s trainedon planning forMNCH.Proportion <strong>of</strong>districts withincreased budgetallocation formaternalnewborn andchild healthinterventions inCCHPs.1 Examples <strong>of</strong> <strong>to</strong>ols <strong>to</strong> be used include <strong>Plan</strong> Rep, costing <strong>to</strong>ols and other relevant sources <strong>of</strong> information32ResponsiblePersonMoHSW(RCHS,Policy and<strong>Plan</strong>ningUnit) DistrictCouncilsDevelopmentPartners.ResourcesNeeded inUS dollars480,000
<strong>Strategic</strong> Objective/OutputActivitiesTimeframe08 09 10 11 12 13 14 15ProcessIndica<strong>to</strong>rs5. 2.3Basic (BEmOC) andComprehensiveEmOC(CEmOC)andnewborn services atall levelsstrengthened.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:% <strong>of</strong> health facilitiesproviding BEmOCand CEmOC andEssential Newborncare5.2.3.1 Strengthen the capacity <strong>of</strong> all dispensariesand all health centres <strong>to</strong> provide BEmOC,essential newborn care and KMC through:• Deployment <strong>of</strong> skilled health workers(Nurse midwives, Clinical Officers,labora<strong>to</strong>ry assistants)• Provision <strong>of</strong> essential equipment andsupplies.• Infrastructural improvement for servicedelivery (Delivery room, postnatal room,labora<strong>to</strong>ry)5.2.3.2 Strengthen the capacity <strong>of</strong> allhospitals and upgrade 50% <strong>of</strong> healthcentres <strong>to</strong> provide CEmOC andessential newborn care through:• Deployment <strong>of</strong> skilled health workers(Nurse midwives, MO, AMOs,Anaesthetists, Labora<strong>to</strong>ry technicians)• Provision <strong>of</strong> essential equipment andsupplies.• Infrastructural improvement forservice delivery (Operating theatres,Labour ward, Blood s<strong>to</strong>rage facilities,incinera<strong>to</strong>rs)• Establish neonatal and KMC unitsX X X X X X X X Proportion <strong>of</strong>health facilitiesproviding BasicEmOC in theessential newborncare.X X X X X X X X Proportion <strong>of</strong>health facilitiesprovidingComprehensiveEmOC andessential newborncare.5.2.3.3 Develop and conduct tailor madetraining for AMOs and Nurses <strong>to</strong>provide CEmOC, Essential Newbornand child health servicesX X X X X X X XNumber <strong>of</strong> AMOstrained usingtailor madecurricular4 Every population <strong>of</strong> 500,000, at least 4 Basic EmOC are needed (See Glossary for components <strong>of</strong> Basic and Comprehensive EmOC)5 Every population <strong>of</strong> 500,000, at least 1 comprehensive EmOC is needed (See Glossary for components <strong>of</strong> Basic and Comprehensive EmOC)33ResponsiblePersonMoHSW(Direc<strong>to</strong>rates<strong>of</strong> Preventiveand HospitalServices)PMO-RALG,CSOsPrivate sec<strong>to</strong>rMoHSW(Direc<strong>to</strong>rates<strong>of</strong> Preventive &HospitalServices),PMO-RALG.APHTAHealthPr<strong>of</strong>essionalAssociationsDevelopmentPartner andUN AgenciesMoHSWPMO-RALG.APHTAHealthPr<strong>of</strong>essionalAssociationsDevelopmentPartner andUN AgenciesResourcesNeeded inUS dollars98,000,00068,000,0001,200,000
STRATEGIC PLAN AND ACTIVITIES: 2008 -2015<strong>Strategic</strong> Objective/OutputActivitiesTimeframe08 09 10 11 12 13 14 15ProcessIndica<strong>to</strong>rs5.2.4Mechanisms foravailability <strong>of</strong>essentialcommodities,supplies andmedicines formaternal, newbornand child healthincluding familyplanningstrengthened.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Essentialcommodities, suppliesand medicines formaternal, newbornand child careavailable all the timeat every health facility5.2.4.1 Forecast demand, procure andsupply essential commodities andsupplies for maternal, newborn andchild care 6 including contraceptives.Emphasis <strong>to</strong> be put on:• Essential obstetric supplies andmedicines for ANC, delivery andpostpartum.• Newborn resuscitation kits, suppliesand drugs.• Contraceptives (pills, IUCD,implants, injectables and condoms).• Vaccines• Labora<strong>to</strong>ry reagents.• Paediatric emergency equipment(oxygen concentra<strong>to</strong>r, glucometers,ambu bags, suction, infusion pumps)and IMCI drugs and supplies• Supplies for therapeutic feeding formanagement <strong>of</strong> severe acutemalnutrition5.2.4.2 Revive and/or establishmaintenance units for various equipmentat the hospital level.X X X X X X X X Percentage <strong>of</strong>health facilitieswith s<strong>to</strong>ck-outs <strong>of</strong>essentialcommodities,supplies andmedicines formaternal,newborn andchild careincludingcontraceptives.X X X X X X X X Proportion <strong>of</strong>hospitals withfunctioningequipmentmaintenanceunits.Essential Newborn equipment and supplies (See Annex 8)ResponsiblePersonMoHSW(Direc<strong>to</strong>rate <strong>of</strong>Hospital Services,RCHS and MSD)District Councils,DevelopmentPartnersCSOsPrivate sec<strong>to</strong>rMoHSW (RCHS,Direc<strong>to</strong>rate <strong>of</strong> HS)RHMTsDistrict CouncilsResourcesNeeded inUS dollars800,000,0005,000,000634
<strong>Strategic</strong> Objective/Output5.2.5Referral system atall levelsstrengthened.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Functional referralsystems in place at alllevels35Activities5.2.5.1 Procure and install communicationequipment (Two way radiocommunication, phones) in districthospitals, selected health centres anddispensaries.5.2.5.2 Procure and utilise ambulances forreferral purposes, at least one per districthospital and one per health centre andselected dispensaries.5.2.5.3 Procure mo<strong>to</strong>rbike Ambulance forHealth Centre /dispensaries whereapplicable5.2.5.4 Provide sufficient fuel forvehicles/mo<strong>to</strong>rbikes5.2.5.5 Conduct maintenance services forcommunication equipments andvehicles/mo<strong>to</strong>rbikes5.2.5.6 Orient regional and district healthcommittees on obstetric, newborn andchild emergency preparednessTimeframe08 09 10 11 12 13 14 15ProcessIndica<strong>to</strong>rsX X X X X X X X Proportion <strong>of</strong>health units with2way Radiocommunicationequipment.X X X X X X X X Proportion <strong>of</strong>health facilitieswith functioningambulances andmo<strong>to</strong>rbikes forreferral.X X X X X X X X Proportion <strong>of</strong>regional/districthealthcommitteesoriented onemergencypreparedness.ResponsiblePersonMoHSW/RCHSDistrictCouncilsDevelopmentPartnersCSOsPrivate sec<strong>to</strong>rMoHSWRCHSPMORALGMoIDDistrictCouncilsDevelopmentPartnersCSOsPrivate sec<strong>to</strong>rMoHSW/RCHSZTCsRHMTsCHMTsDevelopmentPartnersCSOsResourcesNeeded inUS dollars4,600,0008,000,0001,000,000
<strong>Strategic</strong> Objective/Output36STRATEGIC PLAN AND ACTIVITIES: 2008 -2015ActivitiesTimeframe ProcessIndica<strong>to</strong>rs5.2.5.7 Orient other support staff(community health workers,ambulance drivers and attendants) onemergency and responsepreparedness.08 09 10 11 12 13 14 15X X X X X X X X Number <strong>of</strong> healthfacilities withsupport stafforiented onemergency andresponsepreparedness.5.2.5.8 Establish/revive communityemergency committee in everyvillage <strong>to</strong> mobilise communityresource for emergency transport andfor blood donors.X X X X X X X X Proportion <strong>of</strong>villages withfunctioningemergencycommittees forMNCH.5.2.5.9 Establish maternity waitinghomes where applicable.X X X X X X X X Proportion <strong>of</strong>health facilities(whereapplicable)linked <strong>to</strong>functioningmaternitywaiting homes.ResponsiblePersonMoHSW/RCHSZTCs,RHMTsCHMTs,Development PartnersCSOsPMORALGMoCDGCMoHSW/RCHS,DistrictCouncilsCHMTVillageGovernmentDevelopment PartnersCSOsMoHSW/RCHSDistrictCouncilsCHMTsVillageGovernmentDevelopment PartnersCSOsPrivate sec<strong>to</strong>rResourcesNeeded inUS dollars2,000,000700,000600,000
<strong>Strategic</strong> Objective/OutputActivitiesResearch, Moni<strong>to</strong>ring and Evaluation5.2.6.1 Develop and updatemoni<strong>to</strong>ring and evaluationframework for MNCH5.2.6HMIS capacity <strong>to</strong>capture informationon maternal, neonataland child indica<strong>to</strong>rsincluding FP andnutrition improved.<strong>Strategic</strong> OutputIndica<strong>to</strong>r :Key Maternal, newbornand child healthindica<strong>to</strong>rs reportedannually through HMIS5.2.6.2 Update moni<strong>to</strong>ring datacollection <strong>to</strong>ols <strong>to</strong> include EmOCprocess indica<strong>to</strong>rs and other missinginformation on nutrition, post abortalcare, postnatal care, newborn andchild care and referral forms, registerfor referral, log-books.5.2.6.3 Produce, disseminate,distribute updated data collection<strong>to</strong>ols at all levels.37Timeframe08 09 10 11 12 13 14 15ProcessIndica<strong>to</strong>rsXXXXX X Moni<strong>to</strong>ring andevaluationframework forMNCH in place.Moni<strong>to</strong>ring datacollection <strong>to</strong>olsupdated.X X X Proportion <strong>of</strong>facilities usingupdated datacollection <strong>to</strong>ols.ResponsiblePersonMoHSW (HMISUnit)NBS (PovertyMoni<strong>to</strong>ringUnit)CHMT andDevelopmentPartnersMOHSW(RCHS, HIS)MSDCHMTsCSOsPrivate sec<strong>to</strong>rResourcesNeeded inUS dollars210,000740,000
<strong>Strategic</strong> Objective/Output5.2.7Moni<strong>to</strong>ring andevaluation frameworkfor MNCHstrengthened andimplemented.<strong>Strategic</strong> OutputIndica<strong>to</strong>r :Progress on Maternal,newborn and child healthstatus/trends reported.38STRATEGIC PLAN AND ACTIVITIES: 2008 -2015ActivitiesTimeframe08 09 10 11 12 13 14 15ProcessIndica<strong>to</strong>rs5.2.7.1 Orient health serviceproviders/supervisors on MNCHmoni<strong>to</strong>ring and evaluationframework and effective datamanagement (data collection, analysisand utilization.)5.2.7.2. Conduct supportivesupervision for MNCH in both publicand private health facilities.5.2.7.3 Conduct follow up <strong>of</strong> healthworkers after training on MNCHpackages.X X X X X X X X Number <strong>of</strong> healthserviceproviders/supervisorsoriented on datamanagement.XXXXXXXXXXXXXXXXProportion <strong>of</strong>health facilitiesreceivingquarterlysupportivesupervision.Proportion <strong>of</strong>health workersthat receivedfollow up aftertraining onMNCH packagesyearly.5.2.7.4 Conduct periodic surveys onquality <strong>of</strong> care, client satisfaction andcare seeking behaviour in selecteddistricts and fac<strong>to</strong>rs facilitating orhindering access for maternal,newborn and child care.5.2.7.5 Conduct Biennial Reviewmeetings <strong>to</strong> assess progress on theimplementation.X XXXXXXNumber <strong>of</strong>surveysconducted onquality assurance<strong>of</strong> servicedelivered.Number <strong>of</strong>review meetingsconducted.ResponsiblePersonMoHSW (HMISUnit)RHMTsCHMTsMoHSW(Inspec<strong>to</strong>rateUnit, RCHS)RHMTsCHMTsCSOs.MoHSWPMORALGDevelopmentPartnersResearchinstitutionsNBSAcademicinstitutions,Healthpr<strong>of</strong>essionalassociationsCSOsResourcesNeeded inUS dollars1,000,000950,000830,000
<strong>Strategic</strong> Objective/Output39Activities5.2.7.6 Document and share bestpractices on maternal, newborn andchild health.5.2.7.7 Institutionalize maternal,newborn and child mortality reviewapproaches at all levels• Vital registration system(birth and death)• Confidential enquiry• Near miss surveys• Mortality surveys• Verbal au<strong>to</strong>psy• Other appropriate reviewmechanismsTimeframe08 09 10 11 12 13 14 15ProcessIndica<strong>to</strong>rsX X X X X X X X Number <strong>of</strong> bestpracticesdocumented andscaled up.X X X X X X X X Number and type<strong>of</strong> MNCHmortality reviewreports.ResponsiblePersonMoHSW/RCHSCSOsDevelopmentPartnersPrivate sec<strong>to</strong>rMoHSW/RCHSRHMTs,CHMTsFacilitiesVillageGovernmentsRITANBSResearch andacademicinstitutionsDevelopmentPartnersCSOsResourcesNeeded inUS dollars400,000500,000
<strong>Strategic</strong> Objective/Output5.2.8Community basedmanagementinformation systemstrengthened.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Community baseddata effectivelycollected and used inplanning40STRATEGIC PLAN AND ACTIVITIES: 2008 -2015Activities5.2.8.1 Review and harmonize existingcommunity based managementinformation <strong>to</strong>ols.Timeframe08 09 10 11 12 13 14 15ProcessIndica<strong>to</strong>rsX X X Harmonizedcommunity basedmanagementinformation <strong>to</strong>olsin place.5.2..8.2 Orient village Governments onthe community based managementinformation <strong>to</strong>ols.X X X X X X X X Proportion <strong>of</strong>villageGovernmentmembersoriented oncommunity baseddatamanagement.5.2.8.3 Train community health workersand other service providers oncommunity based informationmanagement.X X X X Proportion <strong>of</strong>communityhealth workersand serviceproviders trainedon datamanagement.ResponsiblePersonRCHSHMISPMO-RALG,RHMTsCHMTsDevelopmentPartnersCSOs,VillageGovernmentsRCHSHMISPMO-RALGRHMTsCHMTsDevelopmentPartnersCSOsVillageGovernmentsRCHSHMISPMO-RALGRHMTsCHMTsVillageGovernmentsDevelopmentPartnersCSOsResourcesNeeded inUS dollars78,000600,0001,200,000
<strong>Strategic</strong> Objective/Output5.2.9 Capacity forconducting MNCHoperationalresearchstrengthened<strong>Strategic</strong> outputindica<strong>to</strong>r:Evidence on MNCHavailable for planningand programmedevelopment41Activities5.2.9.1 Identify MNCH operationalresearch priorities5.2.9.2 Conduct MNCH operationalresearch and document and disseminateresultsTimeframe08 09 10 11 12 13 14 15X XXX X X X X X XProcessIndica<strong>to</strong>rsNumber <strong>of</strong>MNCHoperationalresearchesconducted.ResponsiblePersonMoHSW-RHCS,Research andacademicinstitutionsResourcesNeeded inUS dollars1,000,000
<strong>Strategic</strong> Objective/Output5.2.10Quality assuranceand management(supervision, clientsatisfaction,performanceassessment)strengthened.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Proportion <strong>of</strong> healthfacilities deliveringMNCH servicesaccording <strong>to</strong>nationally definedservice standards42STRATEGIC PLAN AND ACTIVITIES: 2008 -2015Activities5.2.10.1 Adapt quality assuranceapproaches for MNCH (QIRI, PIA, COPE,Collaborative)5.2.10.2 Orient supervisors and serviceproviders on quality assurance methodsfor MNCH services.5.2..10.3 Orient service providers on theClient Health Charter as <strong>to</strong>ol <strong>to</strong> improverelationship with client.5.2.10.4 Update code <strong>of</strong> conduct and jobdescription.5.2.10.5 Orient health facility committeesand district health boards on ClientService Charter <strong>to</strong> ensure satisfac<strong>to</strong>ryclient-service relationship.Timeframe08 09 10 11 12 13 14 15Process Indica<strong>to</strong>rs ResponsiblePersonX X Number <strong>of</strong> qualityassuranceapproaches adaptedXXXXXXXXXXXXXXXXXXXXXXXXXXNumber <strong>of</strong>supervisors andservice providersoriented on qualityassuranceapproaches.Proportion <strong>of</strong> healthservice providersoriented on ClientService Charter atall levels.Code <strong>of</strong> conduct andjob descriptionupdated.MoHSW(RCHS,Inspec<strong>to</strong>rateunit) RHMTsDistrictCouncilsCHMTsDevelopmentPartnersCSOsMoHSW(RCHS,Inspec<strong>to</strong>rateunit) RHMTsDistrictCouncilsCHMTs,DevelopmentPartnersCSOsProportion <strong>of</strong> healthfacility committeesand district healthboards oriented onclient-servicerelationship at alllevels.ResourcesNeeded inUS dollars150,000820,000
<strong>Strategic</strong> Objective/OutputActivities5.3 Community Mobilisation5.3.1Community basedmaternal, newbornand child healthcare including FPand nutritionstrengthened5.3.1.1 Train community based healthworkers on MNC care includingcommunity IMCI.5.3.1.2 Train Employed CHW onComprehensive Maternal, Neonatal andchild Package.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Maternal, newbornand child health careservices provided atcommunity level5.3.1.3 Re-instutionalize quarterly villagehealth days5.3.1.4 Conduct monthly outreach andmobile clinic services for MNCH.5.3.1.5 Provide community healthworkers with necessaryequipment, commodities,supplies and transport.5.3.1.6 Develop and implementincentive mechanism forcommunity health workers7 Required ratio 1/30 households43Timeframe08 09 10 11 12 13 14 15Process Indica<strong>to</strong>rs ResponsiblePersonX X X X X X X X Proportion <strong>of</strong>villages withX X X X X X X XX X X X X X X XX X X X X X X XX X X X X X X Xcommunity healthworkers 7 , trainedon maternal,neonatal and childhealth issuesincluding nutritionand FP.Proportion <strong>of</strong>villages conductingvillage health days.MoHSW/RCHS, MoCDGCPMORALGRHMTs,DistrictCouncilsCHMTs,VillageGovernments,DevelopmentPartnersCSOsX X X X X X X XProportion <strong>of</strong>dispensaries andhealth centresconductingmonthly outreachand mobile clinicservices.Proportion <strong>of</strong>villages withincentivemechanism forcommunity healthworkers.ResourcesNeeded inUS dollars3,200,000
STRATEGIC PLAN AND ACTIVITIES: 2008 -2015<strong>Strategic</strong> Objective/ Activities Timeframe Process Responsible ResourcesOutput 08 09 10 11 12 13 14 15 Indica<strong>to</strong>rs Person Needed inUS dollars5.3. 2Communityparticipation inmaternal newbornand child healthcare increased.<strong>Strategic</strong> OutputIndica<strong>to</strong>rsCommunity leadersand membersparticipating activelyin MNCH issues5.3.2.1 Sensitize community leadersand communities onparticipa<strong>to</strong>ry planning ,implementation and moni<strong>to</strong>ring<strong>of</strong> community based MNCHinterventions.5.3.2.2 Orient health facility committeesand district health boards onClient Service Charter <strong>to</strong> ensuresatisfac<strong>to</strong>ry client-servicerelationshipX X X X X X Proportion <strong>of</strong>villages withcommunityleaders andmemberssensitised onmaternal,newborn andchild healthissues.Proportion <strong>of</strong>villages planswith MNCHactivities.X X X X X X X X Proportion <strong>of</strong>health facilitycommittees anddistrict healthboards orientedon clientservicerelationship atall levels.MoHSW/RCHS,MoCDGCPMORALGDistrictCouncilsCHMTs,CommunitiesCSOsDevelopmentPartnersMoHSW,DistrictCouncils2, 500,000625,00044
<strong>Strategic</strong> Objective/Output5.4 Behaviour Change5.4.1Key communityand householdpractises formaternal, newbornand child careimproved .<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Improved practisesfor maternal,newborn and childhealth care at alllevels.45Activities5.4.1.1 Design, develop IEC/BCCmessages and materials for communitymembers (men, women and adolescents)for specific maternal newborn and childissues, with emphasis on:• Postnatal and Newborn care;• Advantages <strong>of</strong> early attendance <strong>to</strong>health facilities (ANC);• Birth preparedness;• Essential nutritional practices andactions for maternal newborn andchild;• Causes <strong>of</strong> maternal, newborn andchild deaths and identification <strong>of</strong>Danger signs;• Early Care seeking and compliance• Home management <strong>of</strong> commonchildhood illness• Disease prevention (ITN’s,immunization, hygiene andsanitation)• Interventions <strong>to</strong> prevent HIV andMother <strong>to</strong> Child transmission <strong>of</strong> HIV• Repositioning family planning• Prevention on early and unwantedpregnancies• Role <strong>of</strong> men in Maternal newbornand child health careTimeframe08 09 10 11 12 13 14 15Process Indica<strong>to</strong>rs ResponsiblePersonX X X X X IEC/BCC messagesand materialsaddressing specificmaternal andnewborn issuesdeveloped forcommunitymembers.MoHSW,PMORALG,MoCDGC,MoEVT, MoISCDistrictCouncils,CHMT’s,VillageGovernment,DevelopmentPartners ,Media , CSOs,ResourcesNeeded inUS dollars500,000
STRATEGIC PLAN AND ACTIVITIES: 2008 -2015<strong>Strategic</strong> Objective/OutputActivities5.4.1.2 Disseminate and distributeIEC/BCC messages and materials forcommunity members through differentmedia.5.4.1.3 Develop the capacity <strong>of</strong>community theatre groups <strong>to</strong>disseminate MNCH messages5.5 Fostering Partnership5.5.1.1 Orient partners on One MNCH<strong>Strategic</strong> <strong>Plan</strong>5.5.1Partnership andcoordination forMNCH activities atall levels improved.<strong>Strategic</strong> OutputIndica<strong>to</strong>r:Coordinated responseand leveraging <strong>of</strong>resources for MNCHactivities.5.5.1.2 Conduct joint planning andcoordination meetings withstakeholders/partners for maternal,newborn and child care at all levels5.5.1.3 Conduct quarterly PMNCHcommittee meetings5.5.1.4 Conduct bi-annual PMNCHforumTimeframe08 09 10 11 12 13 14 15X X X X X X X XX X X X X X X XXXXXXXXXXXXXXXXXXXXXXXXXXXProcess Indica<strong>to</strong>rs ResponsiblePersonProportion <strong>of</strong> IEC/BCCmaterials disseminatedthrough different media(<strong>Road</strong> shows, TV, Radioetc).Number <strong>of</strong> communitytheatre groupsestablished <strong>to</strong> disseminateMNCH messages.Number <strong>of</strong> orientationsessions on One MNCH<strong>Strategic</strong> <strong>Plan</strong> conducted.Number <strong>of</strong> joint planningand coordinationmeetings conducted.Number <strong>of</strong> PMNCHcommittee meetings heldannually.Number <strong>of</strong> PMNCH foraheld.MoHSW ,PMORALGMoCDGCMoEVT, MoISCDistrict CouncilsCHMTs, VillageGovernments,DevelopmentPartners , MediaCSOs.MoHSW/RCHSMOCDGC,PMORALGRegionalSecretariatDistrict CouncilsDevelopmentPartners Healthpr<strong>of</strong>essionalassociationsCSO ‘s5.5.1.4 Provide support <strong>to</strong> the PMNCHsecretariat for Partnership co-ordinationX X X X X X X X Functional secretariat forpartnership in place.GRAND TOTAL US$ 230,222,000MoHSWDevelopmentPartners Healthpr<strong>of</strong>essionalassociationsCSO ‘s46ResourcesNeeded inUS dollars6,000,000750,000685,000320,000
CHAPTER 6MONITORING FRAMEWORKMaternal, newborn and child care programmes will be evaluated based on an agreed set <strong>of</strong> indica<strong>to</strong>rs, bothqualitative and quantitative. Routine health information systems currently track outputs such as number <strong>of</strong>admissions, management <strong>of</strong> childhood illnesses, immunization, antenatal care, births, and caesarean sections.There is little information on quality <strong>of</strong> maternal and newborn care, such as intrapartum care, stillbirth rate,babies receiving resuscitation and outcome, and percentage <strong>of</strong> newborns receiving essential newborn care.List <strong>of</strong> indica<strong>to</strong>rs <strong>to</strong> assess MNCH Progressa) Indica<strong>to</strong>rs at <strong>National</strong> level:Sources <strong>of</strong> data will be a combination <strong>of</strong> HMIS, District Health Surveys, Household surveys, Health Facilitysurveys, Demographic Health Surveys (DHS), Tanzania Service Provision Assessment surveys (TSPA),Roll back Malaria M&E surveys and financial records. Collected data will be grouped according <strong>to</strong> gender,age groups, income/wealth quintiles, geographical location (rural and urban) as well as ethnic groups..b) Community Indica<strong>to</strong>rs:• Proportion <strong>of</strong> communities that have set up functional emergency preparedness committees and plansfor MNCH including FP and nutrition• Proportion <strong>of</strong> pregnant women that have birth preparedness plans• Proportion <strong>of</strong> women and children who needed referral who went for referral• Proportion <strong>of</strong> women with knowledge <strong>of</strong> danger signs <strong>of</strong> obstetric, neonatal and child healthcomplications• Proportion <strong>of</strong> district management task forces and committees with representation from communities• Proportion <strong>of</strong> facilities with a designated staff responsible for community health services• Proportion <strong>of</strong> villages conducting quarterly village health days• Proportion <strong>of</strong> villages with community health workers implementing MNCH interventions• Coverage <strong>of</strong> access <strong>to</strong> potable water (improved drinking water source)• Coverage <strong>of</strong> improved latrines• Use <strong>of</strong> solid fuels for cooking• Households’ care-seeking rate for diarrhoea, malaria and pneumonia• ITN use in under-fives and pregnant womenc) Neonatal Indica<strong>to</strong>rs• Neonatal mortality rate• Prevalence <strong>of</strong> low birth weight• Early initiation <strong>of</strong> breast feeding (within the first hour)• Proportion <strong>of</strong> district hospitals that have functional newborn resuscitation facilities in the deliveryroom• Number <strong>of</strong> perinatal deaths (still births, deaths within the first seven days <strong>of</strong> life)• Postnatal care attendance rate• Proportion <strong>of</strong> district hospitals implementing Kangaroo Mother Care for management <strong>of</strong> Low BirthWeight• Proportion <strong>of</strong> district hospitals that are accredited baby friendly• Postnatal vitamin A coverage47
d) Family <strong>Plan</strong>ning Indica<strong>to</strong>rs• Contraceptive prevalence rate by method, by age group, by socio economic quintiles• Met need for FP by age group.• Total fertility rate.• Age specific fertility rates• Number <strong>of</strong> individuals accepting contraceptives new accep<strong>to</strong>rs• Number <strong>of</strong> FP service delivery points per 500,000 population <strong>of</strong>fering full range <strong>of</strong> contraceptiveinformation counselling and supplies.e) Maternal Health Indica<strong>to</strong>rs:• Maternal mortality ratio• Proportion <strong>of</strong> deliveries taking place in a health facility• Proportion <strong>of</strong> births assisted by a skilled attendant• Proportion <strong>of</strong> facilities <strong>of</strong>fering BEmOC services and CEmOC services• Coverage <strong>of</strong> met need for obstetric complications (coverage <strong>of</strong> women with obstetric complications thathave received EmOC out <strong>of</strong> all women with obstetric complications)• Caesarean sections as a percentage <strong>of</strong> all live births• Case Fatality Rate for obstetric complications• Proportion <strong>of</strong> first level facilities (PHC) with two or more skilled attendants• Percentage <strong>of</strong> pregnant women attended at least once by skilled personnel; percentage attended byskilled personnel at least four times• Proportion <strong>of</strong> HIV positive women provided with ARV’s during pregnancy• Proportion <strong>of</strong> pregnant women with access <strong>to</strong> PMTCT services• Prevalence <strong>of</strong> positive syphilis serology in pregnant women• Percentage <strong>of</strong> pregnant women tested and treated for syphyllis• Percentage <strong>of</strong> pregnant women receiving two doses <strong>of</strong> SP• Percentage <strong>of</strong> service delivery points providing youth friendly servicesf) Child Health Indica<strong>to</strong>rs• Under-five mortality rate• Exclusive breastfeeding rate
• Measles immunization coverage• DTP- HB3 immunization coverage (Hib coverage after introduction)• Proportion <strong>of</strong> HIV positive children accessing ARV• Proportion <strong>of</strong> HIV exposed infants accessing ARV prophylaxisg) Increased Political Will and Commitment Indica<strong>to</strong>rs:• Proportion <strong>of</strong> Government budget allocated <strong>to</strong> health• Proportion <strong>of</strong> MoHSW/ district budget allocated <strong>to</strong> MNCH and FP• Availability <strong>of</strong> policies addressing increased coverage for skilled care• Development plans integrating MNCH (Development Vision 2025, MKUKUTA, MMAM,HSSP)h) Indica<strong>to</strong>rs for Measuring Progress <strong>of</strong> the MNCH <strong>Strategic</strong> <strong>Plan</strong>• Existence <strong>of</strong> Partnership for Maternal Newborn and Child Health (Partnership)• Total resources mobilized for MNCH <strong>Strategic</strong> <strong>Plan</strong>• Biennial implementation report tracking progress on indica<strong>to</strong>rs listed above49
Table 2: Results-based MatrixMKUKUTA broad outcomes:• Improved quality <strong>of</strong> life and social well-being, with particular focus on the poorest and most vulnerable groups.• Reduced inequalities in outcomes (e.g. education, survival, health) across geographic, income, age, gender and other groups.MKUKUTA (Goal 2.2): To improve survival and well-being <strong>of</strong> all children and women and <strong>of</strong> especially vulnerable groups.MKUKUTA (Goal 2.5): To ensure effective systems <strong>to</strong> permit universal access <strong>to</strong> quality and affordable public services.<strong>Road</strong>map Operation targets:1. Increased coverage <strong>of</strong> births attended by skilled attendants from 46% in 2004/5 <strong>to</strong> 80%.2. Increased immunization coverage <strong>of</strong> DTP-HB 3 and Measles vaccine <strong>to</strong> above 90% in 90% <strong>of</strong> the districts.3. Introduced new vaccines <strong>to</strong> EPI (Hib, Pneumoccocal, Human papiloma (HPV) and rota virus vaccine) .4. Reduced stunting and underweight among under-fives from _38% and 22% <strong>to</strong> 22% and 14% respectively.5. Increased exclusive breast feeding coverage from 41% <strong>to</strong> 80 %6. PMTCT services provided <strong>to</strong> at least 80% <strong>of</strong> pregnant women, their babies and families.7. 90% <strong>of</strong> sick children seeking care at health facilities appropriately managed.8. Increased coverage under-fives sleeping under ITN’s from 16% <strong>to</strong> 80% .9. 75% <strong>of</strong> villages have community health workers <strong>of</strong>fering MNCH services at community level.10. Increased modern contraceptive prevalence rate from 20% <strong>to</strong> 60%11. Increased coverage <strong>of</strong> comprehensive EMOC from 64% <strong>of</strong> hospitals <strong>to</strong> 100% and basic EMOC from 5% <strong>of</strong> Health centres and Dispensaries <strong>to</strong> 70%12. Increase the number <strong>of</strong> health facilities <strong>of</strong>fering Essential Newborn Care <strong>to</strong> 75%.13. Increased antenatal care attendance for at least four visits from 64% <strong>to</strong> 90%Focus Area Indica<strong>to</strong>rs <strong>of</strong> Results Means <strong>of</strong> Verification Assumptions6.1 Advocacy and Resource MobilisationIncreased budget allocation for health especially for maternal and newborn • 15% <strong>of</strong> Government budgetallocated <strong>to</strong> health.services at all levels.• % Health budget available <strong>to</strong>cater for maternal, newborn andchild health services at all levels.•Budget for maternal, newborn andchild health including FP andnutrition increased by 50% by 2015.• Medium Term ExpenditureFramework (MTEF) cash flow atcentral level.• Comprehensive Council Health<strong>Plan</strong> cash flow at district level.• Cash and receipt at all levels.• Public Expenditure Reviewreports• HIPC funds allocated <strong>to</strong> health.• Stable economic growth.• Basket fund available• Commitment by donors/ partners50
Focus Area Indica<strong>to</strong>rs <strong>of</strong> Results Means <strong>of</strong> Verification AssumptionsRegulations/ laws/policies that hinder effective implementation <strong>of</strong>maternal and newborn care byrelevant regula<strong>to</strong>ry bodies reviewed.• Number <strong>of</strong> regulations and laws approved by regula<strong>to</strong>ry bodies • Policy documents available for implementation.• Willingness <strong>of</strong> regula<strong>to</strong>ry bodies <strong>to</strong>review and endorse policy documents.Implementation <strong>of</strong> the exemptionpolicy for maternal and child healthstrengthened. .• • Exemption policy guidelines inExemption policy effectivelyimplementedplace at all facility levels.• Survey findings.• Exemption mechanisms implementedaccording <strong>to</strong> policy.Employment, deployment andretention<strong>of</strong> skilled health workers atall levels <strong>of</strong>care improved.•Number<strong>of</strong> skilled health workersincreased <strong>to</strong> 100% by 2015• Human resource survey• Health Statistics Abstract•6.2 Health Systems Strengthening and Capacity Development• Proportion <strong>of</strong> health facilitiesKnowledge and skills <strong>of</strong> supervisorsand service providers on maternal,newborn and child care including FPand nutrition increased.providing quality maternal andnewborn care.• Maternal, newborn and childhealth service providedaccording <strong>to</strong> standards.• Proportion <strong>of</strong> under-fivesreceivingcorrect anti-malarialtreatment.• Proportion <strong>of</strong> under-fivesreceiving appropriate anti-biotictreatmentfor pneumonia anddysentery.• Proportion <strong>of</strong> under-fivesreceiving ORS and zinc treatmentin management <strong>of</strong> diarrhoea• Percentage <strong>of</strong> pregnant womenreceiving <strong>to</strong> doses <strong>of</strong> SP• Percentage <strong>of</strong> pregnant womentested and treated for syphilis• Training and follow up reports• Health facility survey• Services statistics• Tanzania Service ProvisionAssessment (TSPA),• Service Availability <strong>Map</strong>ping(SAM)• Roll back malaria (RBM) survey• Resources for updating knowledge andskills available.• Availability <strong>of</strong> personnel <strong>to</strong> be trained.51
Results based MatrixFocus Area Indica<strong>to</strong>rs <strong>of</strong> Results Means <strong>of</strong> Verification Assumptions<strong>Plan</strong>ning and management capacity formaternal and newborn care includingFP and nutrition strengthened.• Relevant sec<strong>to</strong>rs (Ministry <strong>of</strong>Finance, MoHSW) allocating atleast 15% <strong>of</strong> Government budgetfor health.•MoHSW allocating 15% <strong>of</strong> theHealth budget for maternal andnewborn care.• Training reports MTEF cashflow at all levels.• CCHP cash flow at district level.• Cash and receipt at all levels.• Public Expenditure Reviewreports• <strong>Plan</strong>ning and management <strong>to</strong>olsavailable.• Stable economic growth.• Basket fund available• Commitment by donors/ partners• Evidence-based maternal andnewborn care planning at RCHSand CHMT• <strong>Plan</strong>ning documents.• CCHPs• MTEF• Personnel available.• Proportion <strong>of</strong> districts with • CCHP cash flow • Stable economic growth.increased budget allocation for• Basket fund availablematernal newborn and child healthinterventions in CCHPBasic and Comprehensive EmOCand newborn services at all levelsstrengthened.• % <strong>of</strong> health facilities providing Basic • Health facility surveyand comprehensive EmOC and • service statistics (TSPA, SAM)Essential Newborn care• Proportion <strong>of</strong> births assisted by • Demographic Health Survey,a skilled attendantHousehold surveys• CHMT and HF managers trained on how<strong>to</strong> measure/ use the indica<strong>to</strong>rs.• Availability <strong>of</strong> funds• Availability <strong>of</strong> skilled attendants• Availability <strong>of</strong> skilled attendants• Proportion <strong>of</strong> caesarean sectionsas a percentage <strong>of</strong> live births.• Service statistics • Availability <strong>of</strong> skilled attendants• Case fatality rate due <strong>to</strong> obstetric • Service statistics • Availability <strong>of</strong> skilled attendantscomplications.• • Inven<strong>to</strong>ry reportsEssential commodities, supplies andmedicines for maternal, newborn andchild care available all the time atevery health facility• Health facility surveys (TSPA)• Annual ContraceptiveProcurement Tables (CPTs)• Monthly contraceptive s<strong>to</strong>ckstatus reports from MSD• Adequate resource available• Political will and commitment52
Focus Area Indica<strong>to</strong>rs <strong>of</strong> Results Means <strong>of</strong> Verification Assumptions• • Inven<strong>to</strong>ry reportsMechanisms for availability <strong>of</strong> essentialcommodities, supplies and medicines formaternal, newborn and child healthincluding family planning strengthened.Essential commodities, supplies andmedicines for maternal, newborn andchild care available all the time atevery health facility• Health facility surveys (TSPA)• Annual ContraceptiveProcurement Tables (CPTs)• Monthly contraceptive s<strong>to</strong>ckstatus reports from MSD• Adequate resource available• Political will and commitmentReferral SystemReferral system at all levelsstrengthened.• Functional referral systems inplace at all levels• Percentage <strong>of</strong> all women withmajor obstetric complicationstreated in EmOC facilities (me<strong>to</strong>bstetric need)• Percentage <strong>of</strong> referred underfiveswho actually go for referral• Special Survey• Service statistics reports• Availability <strong>of</strong> funds <strong>to</strong> improve referralsystem• Willingness <strong>of</strong> community members <strong>to</strong>participate in emergency preparednessResearch, Moni<strong>to</strong>ring and EvaluationHMI S capacity <strong>to</strong> capture information on maternal, neonatal and child indica<strong>to</strong>rs including FP and nutrition improved.• Key Maternal, newborn and childhealth indica<strong>to</strong>rs reported annuallythrough HMIS• Health statistics reports• Health Statistics Abstract• HMIS reviewed <strong>to</strong> incorporate maternaland newborn health indica<strong>to</strong>rs53
Results based MatrixFocus Area Indica<strong>to</strong>rs <strong>of</strong> Results Means <strong>of</strong> Verification AssumptionsMoni<strong>to</strong>ring and evaluation framework forMNCH strengthened and implemented.• Progress on Maternal, newborn andchild health status/trends reported.• Maternal mortality rate• Under-five mortality rate• Infant mortality rate• Neonatal mortality rate• Contraceptive prevalencerate by method, by agegroup, by socio economicquintiles• Under weight, stuntingrate• Exclusive Breast Feedingrate• Measles immunizationcoverage• DTP-HB3 immunizationcoverage• Special reports/surveys• Service statistics reports• Supervision reports• Mortality review andnotification reports• Demographic health survey,• Census• Vital statistics• Adequate resources <strong>to</strong> conductOperational Research• Capacity <strong>to</strong> conduct researchCommunity based managementinformation system strengthened.Quality assurance and management(supervision, client satisfaction,performance assessment) strengthened.• Proportion <strong>of</strong> health facilitiesreceiving quarterly supportivesupervision.• Proportion <strong>of</strong> health workers thatreceived follow up after training onMNCH packages yearly• Number <strong>of</strong> surveys conducted onquality assurance <strong>of</strong> service delivered.• Number and type <strong>of</strong> MNCHmortality review reports.Birth registration rate• Community based data effectivelycollected and used in planning.• Proportion <strong>of</strong> health facilitiesdelivering MNCH services according<strong>to</strong> nationally defined servicestandards• Proportion <strong>of</strong> clients satisfiedwith maternal and newbornservices• Community development plans.• CBMIS data available• Health facility and householdSurveys• Service statistics• Supervision reports• Adequate resources <strong>to</strong> facilitate planningat community level.• Capacity and capability <strong>of</strong> the communitymembers <strong>to</strong> use evidence basedinformation for planning.• Standards for quality improvement willbe implemented.54
Focus Area Indica<strong>to</strong>rs <strong>of</strong> Results Means <strong>of</strong> Verification Assumptions<strong>to</strong> health facility for care sick/postnatal••Percentage <strong>of</strong> pregnant womenattended at least once by skilledpersonnel; percentage attended byskilled personnel at least four timesHouseholds care seeking rate fordiarrhoea, malaria, pneumonia andneonatal conditions55
56When a woman undertakes her biological role<strong>of</strong> becoming pregnant and undergoingchildbirth, the society has obligation <strong>to</strong> fulfilher basic human rights and that <strong>of</strong> her child.
ANNEX 1SWOT ANALYSIS57
ANNEX 1: SWOT ANALYSIS(A) Maternal CareSTRENGTHS WEAKNESSES OPPORTUNITIES THREATS(i) Policy Issues• Existence <strong>of</strong> national policieswhich address maternal healthsuch as the <strong>National</strong> HealthPolicy, Reproductive and ChildHealth Policy, MKUKUTA,MMAM etc.• The <strong>National</strong> Health Policy andthe Reproductive and ChildHealth Policy emphasise amultisec<strong>to</strong>ral approach <strong>to</strong>reproductive health issues, whichinclude male involvement.• The <strong>National</strong> Health Policypromotes the right <strong>of</strong> all women<strong>to</strong> access quality reproductivehealth services.• Existence <strong>of</strong> various <strong>to</strong>ols such asthe RCH Strategy, RCH EssentialPackage and policy guidelineswhich address maternal health.• Maternal health is reflected inthe District <strong>Plan</strong>ning Guidelineas one <strong>of</strong> the key reproductiveand child health interventions.• Existence <strong>of</strong> establishment/manning level (1999) <strong>of</strong> healthstaff for health delivery tiers• Some existing health cadres havebeen reviewed (MCHA,RMA/CA upgrading)• Minimal budget allocation <strong>to</strong> health sec<strong>to</strong>respecially maternal health (at all levels)• Weak multisec<strong>to</strong>ral linkages at all levels inaddressing maternal health• The RCH strategy have not been able <strong>to</strong>prioritise key interventions <strong>to</strong> reducingmaternal death• Inadequate dissemination and interpretation<strong>to</strong> user-friendly formats <strong>of</strong> RCH policies,strategy and guidelines.• Some managers and supervisors at all levelsare not familiar with policies and guidelinesrelated <strong>to</strong> RCH• CCHP do not comprehensively addressingRH/maternal and child health interventions• RCH Coordina<strong>to</strong>r not full member <strong>of</strong> CHMTbut more <strong>of</strong> co-opted member (in somedistricts) as such not able <strong>to</strong> influence districthealth plans• Manning level not implemented accordinglydue <strong>to</strong> insufficient linkages and mixed roles <strong>of</strong>HS and LG.• Establishment/manning level <strong>of</strong> staff has notbeen reviewed according <strong>to</strong> recentdevelopments in RCH care (PMTCT, VCT,ARH/YFS)• Current deployment system doesn’t follow themanning level guidelines.• Development partners andGovernment aligning <strong>to</strong>joint support according <strong>to</strong>Joint Assistance Strategy.• Existence <strong>of</strong> Health basketfunds <strong>to</strong> support districthealth services• Establishment <strong>of</strong> MNCpartnership at central level• Existence <strong>of</strong> Governmentled SWAPs, MOH Technicalcommittee andsubcommittee that can beused <strong>to</strong> push Maternal andNewborn health issues• Existing Annual HealthSec<strong>to</strong>r Reviews have takenin<strong>to</strong> considerationRH/Maternal health issues• Political will andcommitment is showingpositive signs <strong>to</strong>wardsaddressing maternal health(DHA <strong>to</strong>ol)• Existence <strong>of</strong> Health SWAPS• Zonal RCH reviews Careand Treatment <strong>Plan</strong> givesopportunity <strong>to</strong> mainstreammaternal health care• More focus on HIV/AIDS thanRH/Maternal health• Short time <strong>to</strong>wardsattainment <strong>of</strong> MDGs• Bigger proportion <strong>of</strong> healthsec<strong>to</strong>r budget is donordependant.• Donor driven initiatives• Reproductive health conceptmay be overridden bymaternal health (threat <strong>of</strong>returning <strong>to</strong> old MCH concept)• Competing priorityprogrammes• HIV/AIDS• Human resources• Logistic Managementcapacity• TBA policy review and part <strong>of</strong>the Annual Health Sec<strong>to</strong>rReview miles<strong>to</strong>ne58
STRENGTHS WEAKNESSES OPPORTUNITIES THREATS• Exemption policy for deliveriesand all RCH services• Decentralisation <strong>of</strong> healthservices <strong>to</strong> district level (advancehealth sec<strong>to</strong>r reforms)• Existence <strong>of</strong> various financialresources <strong>to</strong> health sec<strong>to</strong>r at thedistrict level (Basket, Block,District own source, cost sharing,NHIF, CHF etc)• Existence <strong>of</strong> Paramedical,Medical and NursingInstitutions for pre-servicetraining• Existence <strong>of</strong> training guidelineson PAC, LSS, FP, PMTCT+, STI,FANC• Availability <strong>of</strong> committedDevelopment Partnerssupporting RH/maternal health• MTEF allocated funds forprocurement <strong>of</strong> contraceptives• Maternal nutrition linked withchild nutrition in the RCHpackage• Community based RCHguidelines, strategic plan (draft)available• Infrastructure at all levelsoverseeing health services -national, regional, district andcommunity• Inadequate number <strong>of</strong> skilled serviceproviders that can be trained and capture theknowledge required on specific skills.• Some skilled providers are not allowed <strong>to</strong> dolife saving skills procedures due <strong>to</strong> statu<strong>to</strong>ryregulations e.g. IV drip giving, manualremoval <strong>of</strong> retained placenta, MVA usage.• There's no mechanism <strong>to</strong> assess prequalification<strong>of</strong> service providers in terms <strong>of</strong>attitude and psychological behaviour beforejoining nursing and medical schools.• Weak incentive package <strong>to</strong> service providers• Poor motivation and inadequate performanceassessment and rewarding <strong>of</strong> serviceproviders• Inconsistency <strong>of</strong> Skilled attendance definitionand how do we attain Skilled attendance inour settings• Inadequate <strong>Plan</strong>s for human resourcedevelopment including continuing educationon maternal health issues• Lack <strong>of</strong> continuing education among tu<strong>to</strong>rs atpre-service and regional institutions.• Poor interpretation and implementation <strong>of</strong>exemption policy for maternal health• Informal payments hinders implementation <strong>of</strong>exemption policy• Due <strong>to</strong> minimal allocation <strong>to</strong> RCH services,women are asked <strong>to</strong> purchase or come withessential supplies/drugs for delivery sincethey are frequently out <strong>of</strong> s<strong>to</strong>ck• Existence <strong>of</strong> Annual RMOs,DMOs and RCH Meetingsas fora <strong>to</strong> discussRH/maternal and newbornissues• Increasing Governmentand DPs attention onaddressing Humanresource crisis• Presence <strong>of</strong> guidelines fromFCI on caring behavioursamong service providers• Ongoing review onincentive package for healthcare providers• Introduction <strong>of</strong> OPRA at alllevels.• MKUKUTA• Existing plans <strong>of</strong>strengthening andexpanding ZTC for inservicetrainings.• Overstretching <strong>of</strong> healthsystem as per currentdevelopment which is alreadycompromised.59
STRENGTHS WEAKNESSES OPPORTUNITIES THREATS• Lack <strong>of</strong> costed RCH package includingmaternal health that can justify how muchis being exempted• At all levels there has been slow follow upand scaling up <strong>of</strong> interventions related <strong>to</strong>maternal health• Inadequate documentation <strong>of</strong> evidencebased intervention focusing on maternalhealth• Untimely/Irregular review <strong>of</strong> Pre-Servicetraining curriculum <strong>to</strong> include currentmaternal health developments.• Lack <strong>of</strong> postnatal guides• Policy not allowing MVA kit <strong>to</strong> be madeavailable except when there's presence <strong>of</strong>skilled attendant and after being trained.• Poor coordination and linkages betweendifferent ac<strong>to</strong>rs from central <strong>to</strong> local level.• Existence <strong>of</strong> vertical programme/projectssupport <strong>to</strong> RH (including FP/maternalhealth)• Weak linkages between Direc<strong>to</strong>rates <strong>of</strong>Preventive, Hospital and Training at MOH• PMNCH promotes needfor MNCH <strong>Strategic</strong> <strong>Plan</strong>where all partners buy in• Existence <strong>of</strong> ReproductiveHealth CommoditySecurity committee underGovt leadership• Existence <strong>of</strong> IYCFstrategy• Maternal nutritionaspects integrated in<strong>to</strong>Infant and young childfeeding strategy• Existence <strong>of</strong> Healthinsurance (NHIF) andsome coming up• Birth and deathregistration (vitalstatistics) in place in fewvillages which can beadopted in the rest <strong>of</strong> thecountry.• Existing health MCHstructure fromcommunity <strong>to</strong> hospitallevel• Use <strong>of</strong> alternative serviceproviders <strong>to</strong> supporthealth system such asretired health skilledstaff, performancecontract and Retentionschemes in MKUKUTA60
STRENGTHS WEAKNESSES OPPORTUNITIES THREATS• Inadequate linkages and collaborationbetween RCH Section with TFNC andPMTCT Unit• Role <strong>of</strong> TBA in prevention <strong>of</strong> maternalmortality is unclear. (Role remains unclearin the strategies. Weaknesses in SWOTshould guide strategies• CHF exist in most areas but with limiteduse <strong>of</strong> the funds for maternal health care• Few districts have implemented communitybased RCH program• Village health committee not legallyrecognised.• Shortage <strong>of</strong> Skilled attendance (morepronounced in rural areas)• Unattractive working condition especially inrural areas(ii) Health Systems• Presence <strong>of</strong> ZRCHCO, RRCH Coand DRCHCo• Service delivery points welldistributed <strong>to</strong> consultant,regional and district hospitalsfollowed by health centres anddispensaries.• Indent system for obtainingessential drugs and supplies• Integration <strong>of</strong> FP and HIV/AIDScondom supply/request atdistrict level• Health services including maternal care no<strong>to</strong>perating for 24 hours• Low knowledge on SRH among serviceproviders• Despite training on Focused ANC, there's stillproblem in its implementation due <strong>to</strong> attitudeand low educational background <strong>of</strong>providers who cannot capture the skills;inadequate supplies such as Hb, RPR,contraceptives etc.• Limited training <strong>of</strong> Service providers on PAC,FP, LSS• RH services not youth friendly• Inadequate/inappropriate EmOC (basic andcomprehensive services) at facility level• Existence <strong>of</strong> both privateand public health facilitiesthat provide maternalhealth services.• <strong>Plan</strong> <strong>to</strong> strengthen ZTC• Existence <strong>of</strong> good practiceson youth friendly services(AYA, UMATI, UNICEFsupported interventions)• Existence <strong>of</strong> goodpractices/research onmaternal care improvement(though a few)- FCI, WDP,Care, TEHIP, QIRI• Overwhelming the ZTCcapacity• Cultural barriers61
STRENGTHS WEAKNESSES OPPORTUNITIES THREATS• Local Government authoritiesreforms are supportingimplementation <strong>of</strong> HSR• Presence <strong>of</strong> referral structurewithin the health delivery system• Most <strong>of</strong> essential RCH servicesare in place (ANC, Intrapartum/obstetric, FP, STI, Immunization,PMTCT, Post partum) IMCI at alllevels.• Lack <strong>of</strong> functioning <strong>of</strong> blood banks at hospitaland health centre level• Inadequate coverage <strong>of</strong> PAC services• Essential equipment, supplies and drugs onmaternal care including FP not readilyavailable• Bottlenecks in procurement <strong>of</strong> drugs, suppliesand equipment (both ways district level andMSD)• Fragmented program support in provision <strong>of</strong>essential supplies e.g. syphilis screeningreagents• Facility buildings and providers’ attitude notaccommodating male and youth friendlyservices• Presence <strong>of</strong> vast Geographical area with poortransport/roads, inadequate health facilitiesand therefore poor geographical accessibility<strong>to</strong> EMOC• Inadequate ambulances within the country• Many health units do not have reliablecommunication system (radio call, mobile)• Lack <strong>of</strong> pro<strong>to</strong>cols on specific maternalhealth/obstetric care• Counselling skills on FP, PAC, PMTCT andmaternal nutrition not adequately providedby service providers• Limited postnatal care due <strong>to</strong> lack <strong>of</strong> guidelines• Blood safety programme• Existence <strong>of</strong> RHMT andCHMT which coordinatesdistrict health activitiesincluding maternal healthcare• Currently JointRehabilitation Programmehas been initiated at districtlevel which can be used <strong>to</strong>accommodate structureimprovement for maternaland newborn care• Existence <strong>of</strong> mobilecommunication network inrural areas• Presence <strong>of</strong> job aid forEMOC(iii) Support Systems• Existence <strong>of</strong> Communitydevelopment <strong>of</strong>ficers at districtand ward level.• Premises <strong>of</strong> most health facilities areinadequate and non-user friendly (privacy,space)• Inadequate awareness and advocacy onmaternal complications/care at all levelsincluding health facilities support staff62
STRENGTHS WEAKNESSES OPPORTUNITIES THREATS(iv) <strong>Plan</strong>ning, Moni<strong>to</strong>ring and Evaluation• <strong>Plan</strong>ning decentralised <strong>to</strong>district level• Moni<strong>to</strong>ring <strong>of</strong> Maternal deathdone through week endingreporting, HMIS, DHS andAnnual ZRCH Co reports• Presence <strong>of</strong> HMIS in all healthdelivery systems• Supervision system in place• Presence <strong>of</strong> health facilitycommittee and district boards inmajority <strong>of</strong> districts• Presence <strong>of</strong> CHMT in all districts• Poor mainstreaming <strong>of</strong> maternal healthintervention in<strong>to</strong> CCHP and thereafter in<strong>to</strong>Overall Council <strong>Plan</strong>s as such intervention isnot addressed Multisec<strong>to</strong>ral.• Centralization <strong>of</strong> services/health plans atCHMT level and less on lower level• District Health planning process rarely takein<strong>to</strong> consideration inclusion <strong>of</strong> other relevantmulti sec<strong>to</strong>ral <strong>of</strong>ficers (Education,Agriculture, Engineer, Communitydevelopment) in addressing maternal healthissues.• Inadequate capacity <strong>of</strong> CHMT <strong>to</strong> plan for RCHactivities including maternal health• Poor record keeping and therefore planning isnot evidence based• Most CHMTs still see RCH includingmaternal health interventions asdonor/project supported and notresponsibility <strong>of</strong> district budgets• Family <strong>Plan</strong>ning given less priority inplanning at district level (CCHP).• Conflicting priorities during joint supervision• District health boards andhealth facility committeespresent according <strong>to</strong> setguidelines• Existence <strong>of</strong> TEHIP <strong>to</strong>olthough has limitation onRCH intervention package• Proposal for recordsmanagement improvementhas been made <strong>to</strong> MoHSW• Process and impactindica<strong>to</strong>rs have beenidentified and defined inrecently released RCHstrategy• Existence <strong>National</strong> EMOCsurvey document willprovide benchmark <strong>of</strong>EMOC situationcountrywide.• Insufficient involvement <strong>of</strong> other stakeholdersin the district during planning process,moni<strong>to</strong>ring and evaluation• Village and ward plans not capturingmaternal and newborn interventions/issues• Maternal health indica<strong>to</strong>rs used are mainlyimpact and less/none on process indica<strong>to</strong>rs• Some EMOC process indica<strong>to</strong>rs are difficult<strong>to</strong> calculate since some data is not captured inthe routine HMIS/facility based data records.• Inadequate utilisation <strong>of</strong> data/indica<strong>to</strong>rs forplanning purpose and prioritisation at all• Introduction <strong>of</strong> maternaland perinatal deathreviews• Existence <strong>of</strong> variousnational surveys (Census,DHS, THIS) that can givepicture on RCH situation• Current there's demanddriven capacity buildinginitiative (piloted in lakezone regions) that requiresdistrict <strong>to</strong> demand for63
STRENGTHS WEAKNESSES OPPORTUNITIES THREATSlevels.• Inadequate functioning <strong>of</strong> HMIS• Lack <strong>of</strong> disaggregated data by sex and agespecific• Insufficiently capturing data from privatehealth facilities• Weak/absence <strong>of</strong> Community BasedManagement Information System• Poor documentation <strong>of</strong> clients notes includingtreatment plan, referral notes at facility level• Low coverage <strong>of</strong> supervision• Lack <strong>of</strong> comprehensive and integratedSupervision <strong>to</strong>ol and process• Inadequate accountability among serviceproviders and managers/supervisors• Weak system for moni<strong>to</strong>ring and addressingclients complaints/suggestions• Poor supportive supervision due <strong>to</strong>inadequate skills, commitment and attitude.trainings (under DANIDAsupport)• Quality <strong>of</strong> Care framework<strong>to</strong> consolidate supervisory<strong>to</strong>ols• Presence <strong>of</strong> Client healthservice charter andGuidelines on roles andresponsibilities <strong>of</strong> HFcommittees/districtboards.(v) Community• Presence <strong>of</strong> Primary HealthCommittee/Village healthcommittees that discuss issues onmaternal health.• Presence <strong>of</strong> c-IMCI corps• Presence <strong>of</strong> Community BasedRCH <strong>Strategic</strong> plan, guidelines• Community recognised as keystakeholders in both Local Govtand health sec<strong>to</strong>r reforms.• Local Government reforms havea structure/link down <strong>to</strong> thevillage level.• Weak implementation <strong>of</strong> district guide <strong>of</strong>involving community• Low population coverage• Limited male involvement on issues related <strong>to</strong>maternal health• Obstetric emergencies are not considered bythe Community emergency committee• Community plans not incorporated in<strong>to</strong> theCCHP.• Weak capacity <strong>of</strong> health facility committeesand district boards• The process <strong>of</strong> developing bylaws and thetime it takes <strong>to</strong> be effected.• Inadequate outreach services due <strong>to</strong> poorplanning, inadequate resources.• Inadequately functioning village healthcommittees since they're not facilitated.• Presence <strong>of</strong> O& ODplanning process• Allocation <strong>of</strong> 10% <strong>of</strong> CCHPfunds <strong>to</strong> communityinterventions.• Presence <strong>of</strong> TASAF II thatprovides financial supportfor community based socialservice delivery.• Presence <strong>of</strong> communitymobilization andempowerment initiatives onreproductive health.• Existence <strong>of</strong> the CBDprogramme• Health facilities committeesand district health boards• Presence <strong>of</strong> harmfultraditional practices that canadversely affect maternal andnewborn e.g. taking herbs thathave oxy<strong>to</strong>xic effects can lead<strong>to</strong> ruptured uterus.64
STRENGTHS WEAKNESSES OPPORTUNITIES THREATS• Knowledge on Birth preparedness is pooramong communities• Community not aware <strong>of</strong> their rights andobligations in improving maternal health care• Gender inequalities existing in the communitycontributes <strong>to</strong> poor maternal health outcomes• Low awareness on reproductive systemfunctions and pregnancy related issues suchas danger signs/complicationsrecognised legally• Ability <strong>of</strong> communities <strong>to</strong>devise by-laws <strong>to</strong> addressissues related <strong>to</strong> maternalhealth such as violence,delivery at homes, etc.• Existence <strong>of</strong> Communitybased maternal health caresystem in some areas• Existence <strong>of</strong> client healthservice charter• Existence <strong>of</strong> CSOs/NGOs(vi) Public-Private Partnership• One <strong>of</strong> components <strong>of</strong> HSRstrategy• Presence <strong>of</strong> active Association <strong>of</strong>Private Hospitals in Tanzaniaand PRINMAT• Non-for pr<strong>of</strong>it sec<strong>to</strong>r (FBOs)providing maternal careespecially in rural areas.•• Inadequate coordination in planning andimplementation among partners at centraland district level• Partnership policy guidelines present butmore visible/known at central level and lessat district level.• Some Private health facilities/CSOs notsubmitting data <strong>to</strong> district/central level• Majority <strong>of</strong> Private for Pr<strong>of</strong>it provide serviceson other health issues and less on maternalhealth care• Faith based organizations providing limitedmaternal services (no FP service provided)• Some CSOs that are pro-life provide negativeinformation on contraceptives.• Existence <strong>of</strong> Pr<strong>of</strong>essionalassociations (AGOTA,TAMA)• Existence <strong>of</strong> advocacygroups that are non-healthpr<strong>of</strong>essionals (TAMWA,TGNP, TAWLA, Privatemedia companies, WRA)• Competition for recognitionand resources between publicand private sec<strong>to</strong>r.65
(B) Newborn CareSTRENGTHS WEAKNESSES OPPORTUNITIES THREATS(i) Policy Issues• <strong>National</strong> health policy includeschild health• <strong>National</strong> strategy on Infant andChild Nutrition and plan <strong>of</strong> actionin place• Policy guideline on RCH availableand reflecting neonatal health care• Availability <strong>of</strong> PMTCT and HIVCare and treatment guides thatintegrates neonatal care• Exemption policy for under-fivesincludes neonatal healthservices/care• Institutionalisation <strong>of</strong> IMCI withinthe MoHSW structure/RCHS• IMCI deals with neonate from 8 thday <strong>of</strong> life• C-IMCI promotes communitymaternal care and lactation• Established postnatal follow upfirst week <strong>of</strong> life• Establishment <strong>of</strong> baby friendlyhospital services within somehospitals• Reviewed LSS manualincorporated Newborn careaccording <strong>to</strong> WHO guidelines• Availability <strong>of</strong> committeddevelopment partners supportingnewborn health• Neonatal care obtaining limitedbudget allocation within the healthsec<strong>to</strong>r/RCH services• Nursing training not comprehensivelyaddressing neonatal care• Age specific interventions for 0-1months are not well spelt out in policyguides on RCH• Policy guideline <strong>to</strong> manage newborncare is lacking• Routine health data lacks neonatalhealth progress includingcommunity-based data.• Lack <strong>of</strong> understanding on themagnitude <strong>of</strong> neonatal healthproblems• IMCI does not address first week <strong>of</strong>life• Facility IMCI does not include homecare and care seeking for newborns• Lack <strong>of</strong> concentration on maternalcare and immunization and absence<strong>of</strong> a guide• Inadequate availability <strong>of</strong>paediatricians and neonatal nurses• Lack <strong>of</strong> costing <strong>of</strong> Neonatal carepackage• Lack <strong>of</strong> postnatal guide thus notincorporating newborn care• Decentralisation <strong>of</strong> health services <strong>to</strong> districtlevel (advance health sec<strong>to</strong>r reforms) canaccommodate newborn care• Financial resource allocation <strong>to</strong> the districtlevel (from various sources)• Establishment <strong>of</strong> MNC partnership at centrallevel• On going reviews <strong>of</strong> MoHSW in addressinghuman resource crisis• Existence <strong>of</strong> ZTC, Nursing and Medicalschools• HIV Care and Treatment <strong>Plan</strong> giveopportunity <strong>to</strong> mainstream newborn care.• Coverage <strong>of</strong> IMCI case management Highadding first week could rapidly increasecoverage• Donors, partners interested <strong>to</strong> supportincorporation <strong>of</strong> newborn care• Policy guide on Infant and early feeding fornewborn introduced• Existence <strong>of</strong> Health basket funds <strong>to</strong> supportdistrict health services• Existence <strong>of</strong> Govt led SWAPs, MoHSWTechnical committee and subcommittee thatcan be used <strong>to</strong> push Maternal and NB healthissues• Existence <strong>of</strong> Annual RMOs, DMOs and RCHMeetings a forum <strong>to</strong> discuss RH/maternaland newborn issues• Short time <strong>to</strong>wardsattainment <strong>of</strong> MDGs• For mother not aware<strong>of</strong> their HIV serostatus• Multiplicity <strong>of</strong>guidelinesoverwhelms serviceproviders• HIV pregnant mothersface stigma/dilemmain infant feedingoptions• Bigger proportion <strong>of</strong>health sec<strong>to</strong>r budget isdonor dependant• Donor driveninitiatives??• Harmful practisesand beliefs• Women notempowered• Traditional practiseshindering postnatalattendance66
STRENGTHS WEAKNESSES OPPORTUNITIES THREATS(ii) Health Systems• Infrastructure at all levelsoverseeing health services -national, regional, district andcommunity• Presence <strong>of</strong> ZRCHCO, RRCH Coand DRCHCo• Service delivery points welldistributed <strong>to</strong> consultant, regionaland district hospitals followed byhealth centres and dispensaries.• Lack <strong>of</strong> appropriate resuscitationequipment and supplies e.g. infusionpumps, injectables phenobarbi<strong>to</strong>ne etc• Unattractive working conditionespecially in rural areas• Health services including neonatalcare not operating for 24 hours• HMT are unaware in addressingneonatal health issues• Limited training <strong>of</strong> Service providerson LSS which has a component <strong>of</strong>neonatal care• Inadequate/inappropriate EMOC(basic and comprehensive services) atfacility level• Some neonatal supplies/ equipmentsare not made available at MSD• Poor supply plan at service deliverypoint/districts• Neonatal services are not adequatelyprovided by majority for public andprivate health facilities• Facility buildings not suitableproviding neonatal services• Kangaroo method for low birthweight babies in resource poorcountries has not been adopted.• Under-fives care does not focus agespecific with special needs, as a resultneonatal are not taken in<strong>to</strong>consideration, especially the 1 st week• Existence <strong>of</strong> Paediatric Association <strong>of</strong>Tanzania (PAT) and other healthpr<strong>of</strong>essional associations.• The ongoing Joint Rehabilitation Fundswithin districts can facilitate improvingbuildings <strong>to</strong> provide neonatal care• Presence <strong>of</strong> District Nursing Officer andHospital matron that can focus on neonatalcare• Presence <strong>of</strong> Indent system for obtainingessential drugs and supplies• <strong>Plan</strong> <strong>to</strong> strengthen ZTC• Existence <strong>of</strong> RHMT and CHMT whichcoordinates district health activitiesincluding maternal & newborn care• Rehabilitation <strong>of</strong> health facilities• Partners ready <strong>to</strong> support• Overwhelming the ZTCcapacity(ii) Systems Support• Local Government authoritiesreforms are supportingimplementation <strong>of</strong> HSR• There's vast Geographical area withpoor transport/roads, inadequatehealth facilities and therefore poorgeographical accessibility <strong>to</strong> EMOC• Currently Joint Rehabilitation Programmehas been initiated at district level which canbe used <strong>to</strong> accommodate structureimprovement for maternal and newborn care67
STRENGTHS WEAKNESSES OPPORTUNITIES THREATS• Presence <strong>of</strong> referral structurewithin the health delivery system• Inadequate ambulances within thecountry• Many health units do not havereliable communication system(radio call, mobile)• Inadequate awareness and advocacyon Neonatal care at all levelsincluding health facilities supportstaff• Existence <strong>of</strong> mobile communication networkuntil rural areas(iv) <strong>Plan</strong>ning, Moni<strong>to</strong>ring and Evaluation• <strong>Plan</strong>ning decentralised <strong>to</strong> district level• Poor mainstreaming <strong>of</strong> neonatalhealth intervention in<strong>to</strong> CCHP• Centralization <strong>of</strong> services/healthplans at CHMT level and less onlower level• Inadequate capacity <strong>of</strong> CHMT <strong>to</strong> planfor RCH activities including neonatalhealth• Poor record keeping and thereforeplanning is not evidence based• District health boards and health facilitycommittees present according <strong>to</strong> setguidelines• Proposal for records managementimprovement has been made <strong>to</strong> MoHSW• Introduction <strong>of</strong> maternal and perinatal deathreviews(v) Community• Presence <strong>of</strong> HMIS in all healthdelivery systems• Supervision system in place• Presence <strong>of</strong> health facilitycommittee and district boards inmajority <strong>of</strong> districts• Presence <strong>of</strong> CHMT in all districts••• Inadequate functioning <strong>of</strong> HMIS• Lack <strong>of</strong> disaggregated data by sexand age specific• Weak/absence <strong>of</strong> Community BasedManagement Information System• Supervision undertaken is notcomprehensive and does not captureneonatal care• Weak implementation <strong>of</strong> districtguide <strong>of</strong> involving community• Quality <strong>of</strong> Care framework <strong>to</strong> consolidatesupervisory <strong>to</strong>ols• Presence <strong>of</strong> Client health service charter andGuidelines on roles and responsibilities <strong>of</strong> HFcommittees/district boards.• Presence <strong>of</strong> O& OD planning process whichinvolves the community• According <strong>to</strong> district health planning guidesthere's 10% funds allocated for communityintervention• Conflicting prioritiesduring jointsupervision• Presence <strong>of</strong> harmfultraditional practicesthat can adverselyaffect maternal andnewborn68
70For majority <strong>of</strong> women, especially thepoor and disadvantaged groups, thepathway <strong>to</strong> safe motherhood is blockedby the underlying fac<strong>to</strong>rs that lead <strong>to</strong>delays in accessing appropriate care.
ANNEX 2INPUTS FOR IMPROVINGMATERNAL, NEWBORN ANDCHILD HEALTH AT ALLLEVELS71
ANTENATAL CARETRAINED HEALTH CAREPROVIDER COMMUNITYProvide IEC, health education andcounselling <strong>to</strong> women, men,families and communities about:• The needs <strong>of</strong> pregnant women• Danger signs and appropriateaction• Birth preparedness, includinglocal transportation foremergencies• Work, rest and nutrition• HIV/STD prevention• The importance <strong>of</strong> socialsupportInvolve the husband/partner in IECand counselling sessions<strong>Plan</strong>ning for birth and emergenciesAdolescent girls encouraged <strong>to</strong>continue <strong>to</strong> go <strong>to</strong> schoolPromote beneficial traditionalpractices and advise againstharmful onesPromote ITNsIdentify pregnant women and referearly <strong>to</strong> antenatal clinicProvide follow up care and supportbetween scheduled antenatal clinicvisitsIdentify problems andcomplication and referRecord community-based healthinformation (e.g. number <strong>of</strong>women referral for antenatal care)72DISPENSARY HEALTH CENTRE HOSPITAL SUGGESTED INPUTSAs at community level, plus:Obtain targeted his<strong>to</strong>ry andperform physical examination,moni<strong>to</strong>r progress <strong>of</strong> pregnancy andassess maternal and fetal wellbeingDevelop an individualised birthplan (e.g. place <strong>of</strong> delivery, birthattendant, emergencypreparedness)Perform standard testing:• Syphilis (including treatment asneeded)• Urinalysis• Haemoglobin• Pregnancy confirmationScreen for other STDs whereapplicable and provide appropriatetreatment and counsellingAssess Female genital mutilationManage minor complications such asmild anaemia, uncomplicated urinarytract infection and mild vaginalinfections, uncomplicated malariaProvide tetanus <strong>to</strong>xoid immunizationProvide intermittent presumptivetreatment <strong>of</strong> malariaSell/dispense ITNsAs at dispensary level, plus:Manage certain problems andcomplications (e.g. mild pre-eclampsia,incomplete abortion); refer more seriouscomplicationsOffer voluntary counselling and testingfor HIV as possibleProvide FP and post abortion carePre-referral treatment <strong>of</strong> severecomplications- pre-eclampsia- eclampsia- bleeding- infection- complicated abortionSupport <strong>of</strong> women with special needse.g. adolescents and women living withviolenceManage or refer for PMTCTTreatment <strong>of</strong> mild <strong>to</strong> moderateopportunistic infections in pregnantwomen with HIVAs at health centre level, plus:Manage major problems andcomplications- ec<strong>to</strong>pic pregnancy- Anaemia- severe pre-eclampsia- eclampsia- bleeding- infection- other medical complicationsTreatment <strong>of</strong> abortion complicationsTreatment <strong>of</strong> severe HIV infectionTreatment <strong>of</strong> severe malariaCommunity levelIEC messages/materials about:• The needs <strong>of</strong> pregnant women• Danger signs and appropriate action• Birth preparedness, including local transportationfor emergencies• HIV/STD prevention• Insecticide-treated bed nets (ITNs)• The importance <strong>of</strong> male involvementRefresher in-service training for community-level healthworkers about using IEC messages/materialsIn-service training for supervisors <strong>of</strong> community-levelhealth workers <strong>to</strong> enable them <strong>to</strong> conduct refresher on jobtraining <strong>of</strong> community-level workersIn-service training for community-level health workersinvolved in antenatal care, including problem/complicationidentification and referral; follow up support, recordingDispensary levelIn-service training for healthcare providers responsible forantenatal care about:• Content <strong>of</strong> antenatal care• Revised schedule <strong>of</strong> visits• Assessment skills (his<strong>to</strong>ry taking and physicalexamination; routine testing)• Care provision, including the development <strong>of</strong>individualized birth plan, health education andcounsellingSupplies for syphilis testing, urinalysis, haemoglobin, andother STD tests as necessaryTreat intestinal parasites as neededProvide iron, folic acid and othermicronutrient supplementationManage certain problems andcomplications (e.g. anaemia, PIH,Consistent supply <strong>of</strong> TT vaccine, syringes/needles,antihelminthic drugs, basic drugs such as antimalarial drugs(SP), antibiotics and fungicides ( (SP) and ITNs, iron, folicacid and other micronutrient supplements
TRAINED HEALTH CAREPROVIDER COMMUNITY73DISPENSARY HEALTH CENTRE HOSPITAL SUGGESTED INPUTSslight bleeding); refer otherproblemsProvide additional healtheducation and counselling about:• Preparation for breastfeeding• Prevention and recognition <strong>of</strong>STDs/HIV/AIDS• Prevention <strong>of</strong> malaria andhelminth infestationMother-<strong>to</strong>-child transmission <strong>of</strong>HIV/AIDSHealth Centre levelAll <strong>of</strong> the above and:• Supplies for HIV testing, IV fluids, parental drugs(antibiotics, MgSO4, antimalarials)Supplies and training for Manual Vacuum AspirationsIn-service training for healthcare providers responsible forantenatal care about:• Content <strong>of</strong> antenatal care and treatment mildcomplications as well as pre-referral treatment• Revised schedule <strong>of</strong> visits• Assessment skills (his<strong>to</strong>ry taking and physicalexamination; routine testing)• Care provision, including the development <strong>of</strong>individualised birth plan, health education andcounsellingHospital levelAll <strong>of</strong> the above and:Competency-based training for doc<strong>to</strong>rs in the managemen<strong>to</strong>f eclampsia, severe anaemia, ec<strong>to</strong>pic pregnancySupplies, equipment and drugs for the management <strong>of</strong>complications (blood transfusion, labora<strong>to</strong>ry tests, obstetriccare and surgery)
CARE DURING CHILDBIRTH including obstetric emergency situationsTRAINED HEALTH CAREPROVIDER COMMUNITYProvide a warm and caring approach<strong>to</strong> the womanMoni<strong>to</strong>r progress <strong>of</strong> labour usingsimple aideIf delivery occurs at community level:Follow clean and safe deliverypracticesDiscuss and reach consensus on thelabour and birthing position <strong>of</strong>mother’s choiceRecognise problems or complicationsearly and referInspect placenta; examine perineumfor injuries and refer as neededAfter deliver, notify maternal andfoetal outcomes and report <strong>to</strong> nextlevelCare for the newborn baby includingKMC, recognise danger signs andrefer as appropriatePerform obstetric first aid includingstabilisationArrange for transport and accompanymother <strong>to</strong> the next levelRecord community-based healthinformation (e.g. number <strong>of</strong> womenwith complications referredDISPENSARY HEALTH CENTRE HOSPITAL SUGGESTED INPUTSAs at community level, plus:Obtain targeted his<strong>to</strong>ry andperform physical examinationDiagnose labour and moni<strong>to</strong>rprogress using adapted WHOpar<strong>to</strong>graphProvide supportive care andpain reliefPerform interventions such asamnio<strong>to</strong>my and episio<strong>to</strong>my,only if necessaryInspect placenta and vagina forinjuriesRepair minor lacerations andepisio<strong>to</strong>miesActively manage the thirdstage <strong>of</strong> labour (oxy<strong>to</strong>cin,controlled cord traction, fundalmassage)Care for the baby after birthincl. KMC, moni<strong>to</strong>r the babyand treat or refer as appropriateNewborn resuscitationRecognize complications early(e.g. malpresentations,prolonged or obstructed labour,hypertension, bleeding andinfection) and manage or referas appropriatePerform emergency obstetricprocedures including:• Repair <strong>of</strong> vaginal and cervicallacerations• Vacuum extraction• Manual vacuum aspiration(MVA)Manual removal <strong>of</strong> the placentaAs at dispensary level, plus:Treatment <strong>of</strong> abnormalities andcomplications (prolonged labour,vacuum extraction, breachpresentation, episio<strong>to</strong>my, repair <strong>of</strong>genital tears, manual removal <strong>of</strong>placenta and treatment <strong>of</strong> moderatepost-haemorrhagic anaemiaPre-referral management <strong>of</strong> seriouscomplications (obstructed labour,fetal distress, preterm labour, severeperi- and postpartum haemorrhage)Emergency management <strong>of</strong>complications if birth is imminentSupport for the family in case <strong>of</strong>maternal deathAs at health centre, plus:Treatment <strong>of</strong> severe complications inchildbirth and the immediatepostpartum period, including caesareansection, blood transfusion andhysterec<strong>to</strong>my)- obstructed labour- malpresentations- eclampsia- severe infections- bleedingInduction and augmentation <strong>of</strong> labourManagement <strong>of</strong> complications related <strong>to</strong>FGMPrevention <strong>of</strong> Mother <strong>to</strong> Childtransmission <strong>of</strong> HIV by mode <strong>of</strong>delivery, provision <strong>of</strong> ARV’s, guidanceand support for chosen infant feedingoption.Community levelIn-service training for community-level health workersabout appropriate interpersonal support for the womanduring childbirth; simple labour moni<strong>to</strong>ring; clean andsafe delivery practices; early recognition <strong>of</strong> and response<strong>to</strong> obstetric complicationsBasic delivery kitsWHO adapted par<strong>to</strong>graph formsDispensary levelAs for the community level, plus:In-service training about:• Assessment <strong>of</strong> woman in labour• Clean and safe delivery practices• Use <strong>of</strong> WHO adapted par<strong>to</strong>graph• Amnio<strong>to</strong>my/episio<strong>to</strong>my• Active management <strong>of</strong> third stage• Recognition <strong>of</strong> and response <strong>to</strong> problems/complications• Essential newborn care• KMCConsistent supply <strong>of</strong>Gloves, aprons, soap and water, antiseptic solution, basicinstruments for amnio<strong>to</strong>my and episio<strong>to</strong>my, oxy<strong>to</strong>cin,Vitamin A basic oral drugs, par<strong>to</strong>graph forms, suturematerials/needle holder, Vaginal speculum,, suturematerials/needle holder, vacuum extrac<strong>to</strong>r, MVAequipment, IV fluids and infusion setsIn-service training about:Competency-based skills training for clinical <strong>of</strong>ficers andnurse-midwives in:• Repair <strong>of</strong> vaginal and cervical lacerations• Vacuum extraction• MVA• Manual removal <strong>of</strong> the placenta• Emergency management <strong>of</strong> complications if birth isimminent• Pre-referral management <strong>of</strong> serious complications• Treatment <strong>of</strong> minor complication• Essential newborn careAvailability <strong>of</strong> Newborn resuscitation equipment74
TRAINED HEALTH CAREPROVIDER COMMUNITY75DISPENSARY HEALTH CENTRE HOSPITAL SUGGESTED INPUTSInitiate management and referpatients with:• Haemorrhage• Eclampsia• Obstructed labourPuerperal infectionsDelivery and immediate care <strong>of</strong>the newborn including KMCand immediate initiation <strong>of</strong>breastfeedingImmediate postpartum care <strong>of</strong>the mother:- Assessment <strong>of</strong> maternal wellbeing and detection <strong>of</strong>complications (e.g. bleeding,infections, hypertension andanaemia)- Advice on danger signs,emergency preparedness andfollow-upVitamin A administrationRecording and reporting ondeliveryHealth Centre levelAll <strong>of</strong> the above plus:Continuous Supply <strong>of</strong>: Vacuum extraction equipment, IVfluids and IV sets, MGSO4, parental utero<strong>to</strong>nics andantibiotics, drugs and equipment for essential newborncare.Hospital levelAll <strong>of</strong> the above plus:Health workers trained in:• Management <strong>of</strong> obstetric complications andemergencies including Surgery (caesarean sectionand other abdominal obstetric surgery ec<strong>to</strong>pic pregnancy,hysterec<strong>to</strong>my)• Providing safe anaesthesia for pregnant women• Safe blood transfusion• PMTCTStable supply <strong>of</strong>:Equipment and drugs for anaesthesia, instruments andconsumable supplies for obstetric surgery, bloodtransfusion equipment , Oxygen, labora<strong>to</strong>ry equipment forboth biochemical and microbiological assessments andARV’s.
NEWBORN CARETRAINED HEALTH CAREPROVIDER COMMUNITYProvide immediate care <strong>of</strong> thenewborn, including the following:• KMC stimulate and warmbaby• Clear airway ifnecessary <strong>to</strong> establishrespiration• Tie, cut and care <strong>of</strong> cordusing clean, safe procedures• Establish breastfeedingimmediately after birthAvoid contacts with sickfamily membersExtra care for low-bithweightbabies including KMCRecognition <strong>of</strong> danger signsand referralCounselling on homecare,danger signs, safe disposal <strong>of</strong>baby s<strong>to</strong>ols, nutrition, ITNand hygiene for newborn,need for growth moni<strong>to</strong>ringand immunizations76DISPENSARY HEALTH CENTRE HOSPITAL SUGGESTED INPUTSAs at community level, plus:Ensure warmth <strong>of</strong> sick orpreterm/low birth weight babies asnecessaryPerform basic newbornResuscitationProvide newborn immunizations andadminister eye careProvide counselling and support for:• Care <strong>of</strong> the newborn• Care <strong>of</strong> preterm/low birth weightbabies, including skin-<strong>to</strong>-skinmethod• Breastfeeding• Counselling and support onfeeding fro HIV positive mothersMoni<strong>to</strong>ring and assessment <strong>of</strong>wellbeing, detection <strong>of</strong>complications (breathing, infections,prematurely, low birth weight,injury, malformation)Infection prevention, control androoming-inImmunization according <strong>to</strong> nationalguidelineInitiate management <strong>of</strong> newbornillness and refer <strong>to</strong> appropriate level<strong>of</strong> careAs at dispensary level, plus:Care if moderately preterm, low birthweight or twin; support forbreastfeeding, warmth, frequentassessment <strong>of</strong> wellbeing and detection<strong>of</strong> complications e.g. feedingdifficulties, jaundice or other perinatalproblems.Treatment <strong>of</strong> mild <strong>to</strong> moderate:- local infections (cord, skin, eye,thrush)- birth injuriesPre referral management <strong>of</strong> infantswith severe problems:- very preterm babies And/or low birthweight- severe complications- malformationsPresumptive treatment <strong>of</strong> congenitalsyphilisManagement <strong>of</strong> minor <strong>to</strong> moderateproblems such as feeding difficultiespre-referral management <strong>of</strong> severeproblems such as convulsions andinability <strong>to</strong> feedRecognize danger signs giveappropriate pre-referral treatment andrefer as appropriateAs at health centre level, plus:Management <strong>of</strong> severe newbornproblems such as:- neonatal sepsis- neonatal Jaundice- neonatal Tetanus- breathing difficulties- severe birth trauma and asphyxia- correctable malformations- Neonatal syphilis- failure <strong>to</strong> thriveRefer for further care, if necessaryCommunity levelIn-service training for community-level health workersin essential newborn careIEC messages/materials about:• The danger signs <strong>of</strong> newborn illness and theneed <strong>to</strong> seek immediate care• The importance <strong>of</strong> immunizations, growthmoni<strong>to</strong>ring and follow up• Infant and young child feedingIn-service training for community-level health workersin essential newborn careDispensary levelAll <strong>of</strong> the above plus:Training <strong>of</strong> health workers in essential newborn careContinuous supply <strong>of</strong>: Essential drugs and vaccinesand equipment for newborn resuscitation (mucousextrac<strong>to</strong>r, newborn tube and mask device for newbornresuscitation)Health centre levelAll <strong>of</strong> the above plus:Continuous supply <strong>of</strong>: oxygen, I.V. fluids, parentalantibioticsHospital:All <strong>of</strong> the above plus:Training <strong>of</strong> health workers and lab-technicians in:- management <strong>of</strong> the severely sicknewborn babyAdditional follow-up visits for highrisk babies (preterm, after severecomplications, low-birthweightbabies HIV-exposed babies, babieswith feeding problems and babieson replacement feedingContinuous supply <strong>of</strong> labora<strong>to</strong>ry test equipment,equipment and supplies for anaesthesia and surgerySupporting mother if perinatal death
POSTPARTUM CARETRAINEDHEALTHCARE PROVIDERAT COMMUNITYProvide IEC <strong>to</strong> women, men,families and communities about:• the needs <strong>of</strong>postpartum women• breastfeeding• danger signs for mother andbaby• the importance <strong>of</strong> socialsupport- ITNPromote beneficialtraditional practices anddiscourage harmful onesRefer for first postpartum carevisitwithin 48 hours <strong>of</strong> deliveryProvide follow-up care andsupport between postpartum clinicvisitsand refer for problems andcomplicationsRecord community-based healthinformation (e.g., number <strong>of</strong>womenreferred for postpartum care)77DISPENSARY HEALTH CENTRE HOSPITAL SUGGESTED INPUTSAs at community level plus: As at dispensary level,As at health centre level,Community Level:Obtain pregnancy/birthhis<strong>to</strong>ry and performphysical examination <strong>of</strong>mother and babyRecognise problems orcomplications early(infections, bleeding andanaemia) and manageappropriately or refer forfurther careIron and folic acidsupplementationProvide vitamin A andMicronutrientsupplementation whereAppropriateProvide counselling about:- Breastfeeding and baby care- Maternal nutrition-home care- ITN- Danger signs andappropriate care seekingContraception andresumption <strong>of</strong> sexual activity• Other RH concerns(e.g., STDs/HTV)Manage moderate postpartumproblems/complicationsincluding:• mild <strong>to</strong> moderate anaemia- Mild puerperal depressionPre-referral treatment <strong>of</strong> severeproblems such as severe post partumbleeding, puerperal sepsis and severepuerperal depression.Manage severe postpartumcomplications problems- severe haemorrhage- severe post partum infections- severe post partum depression- female sterilizationIEC messages about:• the needs <strong>of</strong> postpartum women• breastfeeding• immunization• danger signs for mother and baby• beneficial traditional practices and the importance <strong>of</strong>avoiding harmful onesIn-service training for community-levelhealth workers about the importance <strong>of</strong> early postpartumreferral and follow up care, recordingDispensary levelIn-service training for healthcare providers responsible forpostpartum care about:• Content <strong>of</strong> postpartum care• Schedule <strong>of</strong> visits• Assessment skills (his<strong>to</strong>ry taking and physicalexamination <strong>of</strong> mother and baby• Care provision, including micronutrientsupplementation and counselling about breastfeeding,baby care, maternal nutrition, contraception, and otherRH concerns I(e.g. STDs/HIV)• Pre-referral treatment and referral <strong>of</strong> women withcomplicationsConsistent supply <strong>of</strong> vitamin A and othermicronutrients and basic oral drugsHealth centre levelAll <strong>of</strong> the above plus:Consistent supply <strong>of</strong> IV. Fluids, Parental drugs(antibiotics, antimalarials, MgSO4), gloves, soap andother equipments for manual removal <strong>of</strong> placentaHospital LevelAll <strong>of</strong> the above plus:Training <strong>of</strong> health workers in managing severecomplications including surgical, labora<strong>to</strong>ry andanaesthesiological proceduresContinuous supply <strong>of</strong> equipment and utilities for surgery, labora<strong>to</strong>ry tests both microbiology and biochemistry,oxygen, equipment and utilities for blood transfusion.
POSTABORTION CARETRAINED HEALTH CAREPROVIDER COMMUNITYProvide IEC <strong>to</strong> women, men,adolescents and communities about:• The dangers <strong>of</strong> unsafe abortion• The need <strong>to</strong> seek immediate care ata health facility for complicationsRecognise signs <strong>of</strong> abortion earlyRapidly assess condition <strong>of</strong> patientStabilise and refer immediatelyInitiate management <strong>of</strong> shockInitiate treatment <strong>of</strong> sepsisRefer patient for further care, ifnecessaryProvide post-abortion family planning(FP) counselling and methods andother RH services as necessary (e.g.STDs/HIV)78DISPENSARY HEALTH CENTRE HOSPITAL SUGGESTED INPUTSAs at community level, plus: As at dispensary level, plus:As at health centre level, plus: Community levelRapidly assess condition <strong>of</strong>patientInitiate management <strong>of</strong> shockInitiate treatment <strong>of</strong> sepsisRefer patient for further care, ifnecessaryProvide post abortioncounselling and familyplanning methodsProvide other RH services asnecessary (e.g. treatment <strong>of</strong>STDs)Perform manual vacuum aspiration(MVA)Refer cases not appropriate for MVAInitiate pre-referral treatment <strong>of</strong> andrefer for further care as neededManage complications, including:• Intra-abdominal injury• Uterine perforation• Transfusion for blood loss• Sharp curettage• InfectionIEC messages/materials about:• The dangers <strong>of</strong> unsafe abortion• The need <strong>to</strong> seek immediate care at a health facility forcomplications• Options for family planning and access <strong>to</strong> FP servicesIn service training for Community health workers aboutthe early recognition <strong>of</strong> and response <strong>to</strong> signs <strong>of</strong> abortionDispensary levelIn-service training for healthcare providers about the earlyrecognition <strong>of</strong> and response <strong>to</strong> signs <strong>of</strong> abortionIn-service service training for health care providers aboutpost abortion FP counselling and methodsConsistent supply <strong>of</strong> IV fluids and infusion sets,intramuscular(IV/AM) antibiotics, syringesHealth centreAll <strong>of</strong> the above plus:Service providers trained in assessment <strong>of</strong> complicationsrelated <strong>to</strong> post abortion, performance <strong>of</strong> MVA , earlyrecognition <strong>of</strong> danger signs, pre-referral, referralmanagement and post abortion counselling <strong>of</strong> women onFPConsistent supply <strong>of</strong> IV fluids and infusion sets,intravenous/intramuscular (IV/IM) antibiotics,syringes/needles, contraceptives (oral pills, injectables,condoms), MVA equipment, gloves, soap and water,antiseptic solutionHospital levelAll <strong>of</strong> the above plus:Competency-based skills training for doc<strong>to</strong>rs in surgicalprocedures for intra-abdominal injury and uterineperforationEquipment and drugs for anaesthesia, instruments andconsumable supplies for obstetric surgery, bloodtransfusion equipment
FAMILY PLANNINGTRAINED HEALTH CAREPROVIDER COMMUNITYProvide IEC <strong>to</strong> women, men,adolescents and communities aboutthe health benefits <strong>of</strong>:• Delaying first pregnancy• Spacing births and limiting familysizeCounsel clients for FP, including allmethodsProvide contraceptive pillsProvide barrier methods (condoms,foams, jellies)Refer clients for other FP services asnecessaryRecord community-based healthinformation (e.g. number <strong>of</strong> clientsrecruited for FP)79DISPENSARY HEALTH CENTRE HOSPITAL SUGGESTED INPUTSAs at community level, plus:Obtain targeted his<strong>to</strong>ry;perform physical examinationAs at dispensary level, plus:Provide Norplant insertion andremovalAs at health centre level, plus:Perform surgical sterilization(permanent methods)Community levelIEC messages/materials about the health benefits <strong>of</strong>:• Delaying first pregnancy• Spacing births and limiting family sizeScreen for STDs; treat asnecessaryProvide counselling about allmethod and provide method <strong>of</strong>choice, including IUD andinjectables (where skills andsupplies are available)Refer as neededRefer clients who desire surgicalsterilizationIn-service training for community level health workersabout FP counselling for:• Condoms and other barrier methods• Spermicides• Oral and injectable contraceptives• IUD• Permanent methodsIn-service training for community level health workersabout• Distribution <strong>of</strong> pills and barrier methods• Referral• RecordingDispensary levelAll <strong>of</strong> the above plus:In-service training for healthcare providers responsible forFP services about assessment and screening, includinghis<strong>to</strong>ry and physical examination; counselling; STDscreening and treatment, method provision; referralConsistent supply <strong>of</strong> Vaginal speculum, gloves, soap andwater, IUD insertion kits, antiseptic solutionHealth Central levelAll <strong>of</strong> the above plus:Continuous supply <strong>of</strong> oral and injectable contraceptives,IUDs, condoms, foams, jellies, Norplant and equipment forremoval.Hospital levelAll <strong>of</strong> the above plus:Competency-based skills training for doc<strong>to</strong>rs in male andfemale sterilization procedures and anaesthesiologyContinuous supply <strong>of</strong> Surgical instruments and supplies aswell as supplies and drugs for local and generalanaesthesia
PREVENTION AND MANAGEMENT OF CHILDHOOD ILLNESSTRAINED HEALTH CAREPROVIDER COMMUNITYProvide IEC <strong>to</strong> mothers, fathers,families and communities about:• Recognition <strong>of</strong> diseases• The danger signs <strong>of</strong> illnesses• Promotion <strong>of</strong> key healthcarepractices• Availability and use <strong>of</strong> oralrehydration solution (ORS)• Nutrition• Breastfeeding• Immunization• Insecticide treated bednets• Water and sanitation• Household preparedness forprevention and treatment <strong>of</strong>illnessDISPENSARY HEALTH CENTRE HOSPITAL SUGGESTED INPUTSAs at community level, plus:Assess and manage according<strong>to</strong> the IMCI guidelineuncomplicated cases <strong>of</strong>::• Diarrhoea• Acute respira<strong>to</strong>ry infection(ARI)• Malaria• Malnutrition• Other childhood illnesses• Paediatric HIVUse <strong>of</strong> oral and IM antibiotics,medicationsRecognition <strong>of</strong> danger sign andpre-referral treatment andreferral according <strong>to</strong> IMCIguideline.Counsel caregiver onappropriate homecare andnutritionProvide growth moni<strong>to</strong>ring,vitamin A supplementationand vaccination servicesEnsure all children areassessed and managedcomprehensively during allpoints <strong>of</strong> contact with thehealth facility including(assessment and treatment <strong>of</strong>illnesses, growth moni<strong>to</strong>ringand nutritional counselling,immunization status)As at dispensary level, plus:Use <strong>of</strong> IV fluids medicationsAs at health centre level, plus:Labora<strong>to</strong>ry diagnosis <strong>of</strong> respira<strong>to</strong>ryinfections, diarrhoea, malaria, anaemiaTreatment <strong>of</strong> child with complicatedillnessesProvision <strong>of</strong> HIV testing and treatmentfor Children with HIVCommunity levelIEC messages/materials about:• Recognition <strong>of</strong> diseases• The danger signs <strong>of</strong> illnesses• Promotion <strong>of</strong> key healthcare practices• Availability and use <strong>of</strong> ORS• Nutrition• Breastfeeding• Immunization• Insecticide treated bednets• Water and sanitation• Household preparedness for prevention and treatment <strong>of</strong>illnessCommunity-level health workers with improved skills aboutthe prevention, recognition, home care and referral <strong>of</strong>common childhood diseasesDispensary levelIn-service training for healthcare providers in Theprevention and management <strong>of</strong> childhood illness, growthmoni<strong>to</strong>ring, immunization services, counselling for parents<strong>of</strong> sick children, recognition <strong>of</strong> danger signs, pre-referraltreatment and timely referralConsistent supply <strong>of</strong>: Injectable medications, Antimalarials,Antibiotics, Syringes/needles, ORS, ZincHealth centre levelAs above plus:Training <strong>of</strong> lab assistant in biochemical andmicrobiological testsContinuous supply <strong>of</strong> IV sets, syringes, needles and parentaldrugs (anticonvulsants, antibiotics, antimalarials, IV fluids),equipment and utilities for biochemical and microbiologicallabora<strong>to</strong>ry testsHospital levelAll <strong>of</strong> the above plus:Training <strong>of</strong> health workers in management <strong>of</strong> severely illchild including triage, evaluation <strong>of</strong> x-rays80
TRAINED HEALTH CAREPROVIDER COMMUNITY81DISPENSARY HEALTH CENTRE HOSPITAL SUGGESTED INPUTSContinuous supply <strong>of</strong> essential drugs for management <strong>of</strong> theseverely sick child, nasogastric tubes, oxygen equipment,self inflating resuscitation bags with masks, folly catheters,Gloves, disinfectants, nebuliser, equipment for lumbarpuncture, formulas for management <strong>of</strong> sever acutemalnutrition, equipment for blood transfusion, X-ray facility
ANNEX 3RELEVANT POLICY DOCUMENTSMoHSW (2004). Reproductive and Child Health Strategy, 2005-2010.MoHSW- Expanded Programme on Immunization (2005). Comprehensive Multiyear <strong>Plan</strong>, 2006-2010.MoHSW (1999). Staffing Levels for Health Facilities and Institutions.MoHSW (2000). <strong>National</strong> Package <strong>of</strong> Essential Reproductive and Child Health Interventions.MoHSW (2002) EPI Multi Country Evaluation ReportMoHSW (2003). <strong>National</strong> Policy Guidelines for Reproductive and Child Health Services.MoHSW (2004). <strong>National</strong> Adolescent Health and Development Strategy, 2004 -2008.MoHSW (2005). Standards for Adolescent Friendly Reproductive Health Services.MoHSW (2005). Guidelines for Reforming Hospitals at Regional and District Levels.MoHSW (2005). Communication Strategy for Child Health, 2005-2010.MoHSW (2005). <strong>National</strong> Tracer Standards and Indica<strong>to</strong>rs for Quality Improvement in Health Care.MoHSW (2005). Proposed Staffing levels for Health Facilities and Training Institutions.MoHSW (2006). The <strong>National</strong> <strong>Road</strong> <strong>Map</strong> <strong>Strategic</strong> <strong>Plan</strong> <strong>to</strong> <strong>Accelerate</strong> <strong>Reduction</strong> <strong>of</strong> Maternal and NewbornDeaths in Tanzania, 2006-2010.MoHSW (2006). Situation Analysis <strong>of</strong> Emergency Obstetric Care for Safe Motherhood in Public HealthFacilities in TanzaniaMoHSW (2007). Primary Health Services Development Programme (PHSDP/MMAM), 2007-2017.MoHSW (2007). Tanzania <strong>National</strong> Health Policy (draft).MoHSW (2007) Tanzania <strong>National</strong> Voucher Scheme Survey.MoHSW (2008). Human Resource for Health <strong>Strategic</strong> <strong>Plan</strong>, 2008-2013.MoHSW (2008). <strong>National</strong> Supervision Guidelines for Quality Health Care Services (Draft).MoHSW (2007) Postnatal Care Guidelines (draft)MoHSW (2007) Maternal and Perinatal Death Audit Guidelines (draft)MoHSW (2007) Kangaroo Mother Care Guidelines (draft)MoHSW, Prime Ministers Office Regional Administration and Local Government (2007). ComprehensiveCouncil Health <strong>Plan</strong>ning Guidelines.MoPE (2006). Tanzania Population, Reproductive Health and Development. Population and <strong>Plan</strong>ning SectionTanzania Partnership for Maternal Newborn and Child Health Work <strong>Plan</strong>, 2007-2008.Vice President’s Office ( 2005). <strong>National</strong> Strategy for Growth and <strong>Reduction</strong> <strong>of</strong> Poverty (NSGRP).82
ANNEX 4MOST COST EFFECTIVE INTERVENTIONS BASED ON EVIDENCE TODATE FOR REDUCTION OF PERINATAL AND NEONATAL MORTALITYPre conceptionAmount <strong>of</strong>Evidence<strong>Reduction</strong> (%) in all cause neonatalmorbidity and mortality/major riskfac<strong>to</strong>r if specified (effect range)Folic acid supplementation 1V Incident in neural tube defect: 72%(42-87%)AntenatalTetanus <strong>to</strong>xoid immunization.V1V33%-58%Incidence <strong>of</strong> neonatal tetanus 88-100%Syphilis screening and treatment 1V Prevalence dependantPre eclampsia and eclampsia. prevention(calcium supplementationIPT for malaria.Detection and treatment <strong>of</strong> symp<strong>to</strong>maticbacteriuriaIntrapartum1V Incidence <strong>of</strong> prematurity 34%(-1-57%)Incidence <strong>of</strong> low birth weight31%(-1-53%)1V1V32%(-1-53%)Incidence <strong>of</strong> prematurity, low birthweight 40 %( 20-55%)Antibiotics for pre term rupture <strong>of</strong>membranes.1V Incidence if infections 32 %( 13-47%)Corticosteroids for preterm labour 1V 40 %( 25-52%)Detection and treatment <strong>of</strong> breech (csection)1V 40%(25-52%Labour surveillance (including1V Early neonatal death40%par<strong>to</strong>graph)Clean delivery practices 1V Incidence <strong>of</strong> neonatal tetanus.55-90%PostnatalResuscitation <strong>of</strong> new born V 6-42%Breast feedingV 55-87%Prevention and management <strong>of</strong>1V 18-42%hypothermiaKangaroo mother care 1V Incidence <strong>of</strong> infections52 %( 7-75%)Community based pneumonia casemanagement.V 27% (18-35%).Source: Neonatal Survival 2 Darmstadt, G. Bhutta, ZA, Cousens, S, Taghreed, A, Walker, N, de Bernis, L, Evidence-Based, Low-costinterventions: How many newborn babies can we save?www.the lancet.com published on line 3 March 2005 http:// image. The lancet.com/extras/05 art 17 web. The authors use scale rangingfrom 1 <strong>to</strong> 5, with 5 having the most evidence <strong>of</strong> effectiveness 183
ANNEX 5Evidence-Based Interventions that Influence Child HealthVarious evidence-based child health interventions have been identified. These interventions can contribute <strong>to</strong>reduction in neonatal and under-five mortality when implemented in high coverage 90%. The packaging <strong>of</strong>these interventions results in<strong>to</strong> great/significant impact.Interventions Preventive % <strong>of</strong> reduction Neonates Child PregnantmotherLactatingmotherB reastfeeding13%X XXComplementary feeding 6% XVitamin A supplementation 2% X X XVaccination-measles 1% XFamily and Community care package 10-20% X X X XI TN7%X X XWater, sanitation and hygiene 3% X X X XKMC for low birth weight 2% XResuscitation <strong>of</strong> newborn 4% XZ inc5%XC lean delivery4%XXNevirapine and replacement feeding 2% XTreatment interventionsAntibiotics for dysentery 3% xAntibiotic for sepsis 6% X XO ral rehydration15%X XAntibiotic for pneumonia 6% X XA ntimalaria5%X XZ inc4%XEmergence neonatal care: managementOf serious illness (infectionsAsphyxia, prematurity,jaundice)XCommunity mobilization and engagement and antenatal and postnatal domiciliary. Behaviour changecommunication <strong>to</strong> promote evidence-based neonatal care practices (breastfeeding, thermal care, clean and cordcare), care seeking, demand for quality clinical care) Promotion <strong>of</strong> clean delivery and referral <strong>of</strong> complications(home birth) Kangaroo mother care.84
ANNEX 6EVIDENCE-BASED INTERVENTIONS FOR MATERNAL,NEWBORN AND CHILD HEALTHIntervention packageThe following evidence based interventions are expected <strong>to</strong> be provided at all levels.1. For Adolescent girls and women in childbearing age (Pre-pregnancy)• Adolescent friendly health services• Family planning• Folic acid.• Iron tablets• Tetanus <strong>to</strong>xoid• Prevention, care and treatment for HIV/AIDS2. Post abortion care• Manual vacuum aspiration and if not available sharp curettage• Utero<strong>to</strong>nic drug (ergometrin or misopros<strong>to</strong>l)• I.V. antibiotics if infection suspected3. During Antenatal period: at least 4 antenatal care visits for normal pregnancies, including one visitwithin the first 3 months <strong>of</strong> pregnancy.Key ante-natal services include• Confirmation <strong>of</strong> pregnancy• Moni<strong>to</strong>ring <strong>of</strong> progress <strong>of</strong> pregnancy and assessment <strong>of</strong> maternal fetal well-being• Prevention, care and treatment for HIV/AIDS (PMTCT).• Tetanus <strong>to</strong>xoid immunization.• Counselling on nutrition, breastfeeding, healthy life style.• Insecticide treated bed nets• Development <strong>of</strong> birth preparedness plan, emergencies, referral care in case <strong>of</strong> complication,breastfeeding and advice on danger signs.• Screen for protein and anaemia including blood group• Iron and folic acid supplementation.• Deworming• Identification and treatment <strong>of</strong> bacteriuria• Identification and treatment <strong>of</strong> problems complicating pregnancy: hypertension, bleeding,malpresentation, multiple pregnancy, etc.• Screening and treatment <strong>of</strong> syphilis and malaria. (IPT and promotion <strong>of</strong> ITN).• Assessment for female genital mutilation4. Services delivered during Labour, delivery, and first 1 <strong>to</strong> 2 hours• killed attendance at birth• Moni<strong>to</strong>ring progress <strong>of</strong> labour, maternal and fetal well being with par<strong>to</strong>graph• Providing supportive care and pain relief• Clean and safe delivery• Temperature maintenance <strong>of</strong> mother and child including Kangaroo Mother Care.• Immediate and exclusive breast-feeding.• Cord and eye care.• Emergency obstetric care for complications including*:85
• Treatment <strong>of</strong> abnormalities and complications (prolonged labour, vacuum extraction, breechpresentation, episio<strong>to</strong>my, repair <strong>of</strong> genital tears, manual removal <strong>of</strong> placenta)• Pre-referral management <strong>of</strong> serious complications (e.g. obstructed labour, fetal distress, preterm labour,severe peri- and postpartum haemorrhage)• Emergency management <strong>of</strong> complications if birth is imminent• Treatment <strong>of</strong> severe complications in childbirth and immediate postpartum period, including caesareansection, blood transfusion and hysterec<strong>to</strong>my:• Induction and augmentation <strong>of</strong> labour• Antibiotics for premature rupture <strong>of</strong> membranes*• Neonatal resuscitation. *• Management <strong>of</strong> newborn complications. *• Prevention, care and treatment <strong>of</strong> HIV/AIDS(PMTCT)• Active management <strong>of</strong> third stage <strong>of</strong> labour• Vitamin A supplementation5. Maternal care: 1 <strong>to</strong> 2 hours care and after delivery <strong>to</strong> six weeks.• Prevention and detection <strong>of</strong> complications (e.g. infections, bleeding and anaemia)• Anaemia prevention and control (iron and folate supplementation)• Information and counselling on nutrition, safe sex and family planning• Advice on danger signs and emergency preparedness• Provision <strong>of</strong> contraceptive methods• Promote use <strong>of</strong> ITN• Pre-referral treatment <strong>of</strong> complications (e.g. severe postpartum bleeding and puerperal sepsis)*• Treatment <strong>of</strong> complications (anaemia, postpartum bleeding, infections and postpartum depression)*6. Newborn care: 1 <strong>to</strong> 2 hours care and after delivery <strong>to</strong> 2 months.• Promotion, protection and support for exclusive breast-feeding.• Moni<strong>to</strong>ring and assessment <strong>of</strong> wellbeing and detection <strong>of</strong> complications• Rooming-in• Eye care• Temperature management (kangaroo mother care)• Cord care and hygiene.• Information and counselling on home care, breastfeeding, hygiene and advice on danger signs and careseeking.• Promotion <strong>of</strong> ITN• Recognition <strong>of</strong> danger signs and prompts care seeking.• Detection and management <strong>of</strong> local infections, diarrhoea, and feeding problems• Special care for the small baby (low birth weight). *• Treatment <strong>of</strong> infections*• Pre-referral management <strong>of</strong> infants with severe problems (Very preterm babies and/or very low birthweight; severe complications; malformations)*• Presumptive treatment <strong>of</strong> congenital syphilis*• Prevention, care and treatment <strong>of</strong> HIV/AIDS (PMTCT). *• Management <strong>of</strong> complication, serious infections, severe jaundice, very low birth weight babies, pretermbirth, breathing difficulties, severe birth trauma and asphyxia*.• Management <strong>of</strong> correctable malformations*• Treatment <strong>of</strong> neonatal tetanus*• Follow up <strong>of</strong> new born in need <strong>of</strong> special care*86
7. Older infants and children (2 month <strong>to</strong> 5 years)Preventive• Assessment <strong>of</strong> infants wellbeing, detection <strong>of</strong> complications and responding <strong>to</strong> maternal concerns• Information and counselling on home care• Additional follow-up visits for high risk babies (pre-term or after complicated delivery or neonatalperiod)• Exclusive breast-feeding up <strong>to</strong> 6 months• Continued breastfeeding (at least up <strong>to</strong> 2 years)• Nevirapine and replacement feeding (PMTCT)• Safe and appropriate complementary feeding (from 6 months)• Insecticide treated nets• Immunization• Vitamin A supplementation twice a year• De worming twice a year• Water, sanitation, hygiene.• Growth moni<strong>to</strong>ring and follow-up interventions• Salt iodationCurative• Integrated management <strong>of</strong> childhood illnesses• Oral rehydration therapy and Zinc for diarrhoea*• Antibiotics for dysentery*• Antibiotics for pneumonia*• Treatment <strong>of</strong> malaria with recommended combination therapy*• Vitamin A for measles*• Detection and management <strong>of</strong> severe and moderate malnutrition*• Care and treatment <strong>of</strong> HIV/AIDS*• Pre-referral management <strong>of</strong> severe conditions*• Quality management <strong>of</strong> seriously sick children*Note: All interventions should be available for all pregnant women, newborns and children except thosemarked* which need <strong>to</strong> be provided only for illness or complications.*Indicates care if condition arises adapted from: Newborn Health; Policy and <strong>Plan</strong>ning Framework, Part 1, 2004/5 WHO andSave the Children.87
ANNEX 7WHERE DOES TANZANIA STAND IN TERMS OF MNCHSERVICE DELIVERY?PROCEDURE SCORE % DEFICIT EXPECTED 2015Antenatal care four visit 68% 32% 90%Blood Pressure taken 65% 35% All must have BP checkedBlood taken forHaemoglobin and Syphilisscreening50% 50% More than 70% must bescreenedUrine Analysis 41% 59% All must have urine checkedif equipment availableInformation <strong>of</strong> dangersigns in pregnancychildbirth47% 53% At risk mothers should beidentifiedDelivery at health facilities 47% 53% Health facility deliveries80%Skilled birth attendant46% 54% Skilled birth attendant 80%deliveriesDelivery by CaesareanSection3% 12% 15% should be delivered byC/SEmergency Obstetric Carein hospitals64.5% 35.5% All first referral centres mustprovide EmOCEmergency Obstetric CareHealth Centres5.5% 94.5% To achieve MDG 5 allHealth Centres must provideEmOCBreastfeeding at any giventime95%5% All women should breastfeedExclusive breastfeeding 41% 58% EBF rate 0-6 mo 80%rate 0 – 6msVitamin Asupplementation within 2months after delivery20% 80% All post delivery mothersshould receive Vitamin AIron tablets for at least 90days <strong>to</strong> pregnant mothersTetanus ToxoidCurrent usage <strong>of</strong>contraceptivesCommunity BasedProgrammes RCH10% 90% All women for ANC must begiven Iron/Folic acid80% 20% 90%26%married,41%unmarried46 districtsout <strong>of</strong> 12434%19%78 districtshave no CBDProgrammeCPR 60%(Modern FP methods)All districts should target <strong>to</strong>have CBD88
PROCEDURE SCORE % DEFICIT EXPECTED 2015Basic Essential NewbornCare with Resuscitationequipment like AMBUBAGS and OxygenPMTCTNone in DSMfor secondaryand primaryhealthfacilities1347 Healthfacilities haveestablishedby Dec. 2007Paediatric HIV care and RefferaltreatmentHospitalsIntegrated case60% <strong>of</strong> sickmanagement <strong>of</strong> Childhood children seenIllnessesby IMCItrained HWCommunity IMCI 41 out <strong>of</strong> 114LGA’simplementingMunicipalitieshospitals inDAR and healthcentres mustestablish BasicEssentialNewborn Care<strong>to</strong> decongestMNH neonateward3524 HealthFacilitiesRegional and DistrictHospitals100% <strong>of</strong> sickchildren seen byIMCI trainedAll labour wards in thecountry must have a smallunit for care <strong>of</strong> neonatesAll hospitals andhealth centres country wideshould have PMTCTestablished and coordinatedthrough RCH servicesAll Hospitals country wide80% <strong>of</strong> health facilities have60 % <strong>of</strong> health workerstrained in IMCIHW73 LGA’s All districts should have c-IMCI CORP’s in at least75% <strong>of</strong> villagesORS use rate 54% 46% 90% ORS use ratesZinc supplements fordiarrhoeaAnti- Malarial treatmentwithin 24hrs <strong>of</strong> fever onsetITN coverage for underfivesImmunization coverage forall antigensFacility management <strong>of</strong>severe malnutritionCommunity Managemen<strong>to</strong>f Severe MalnutritionBaby friendly healthfacilities0% 100% 80%57% 43% 80% prompt treatment21% 79% 80%71% 29% Over 85%6 hospitals Most <strong>of</strong> the hospital All hospitalsdo not manage severemalnutrition0 LGA’s 114 LGA’s Established in all LGA’s28% 72% All hospitals baby friendly89
ANNEX 8ESSENTIAL MATERNAL NEWBORN AND CHILD HEALTHMEDICINES, EQUIPMENT AND SUPPLIESA. Neonate and Child medicines1. Chloramphenicol inj 1g2. Benzathine Penicillin inj 5 MU3. Gentamicin inj 40mg4. Procaine Penicillin Fortified inj; 4 MU/vial5. Cotrimoxzole syrup 200/40 mg /5 ml susp6. Cotrimoxzole tab 400/80mg7. Cotrimoxzole paediatric tab 100/20mg8 Amoxycillin 250mg tab9 Amoxycillin syrup 250mg/5ml or 125mg/5ml10 Salbutamol metred dose inhaler 100μg/puff(0.1mg/enhale)11. Salbutamol tab 1mg12. IV infusion Ringers Lactate 250mls13. IV infusion Normal Saline14. Low Osmolarity Oral Rehydration Solution sachets15. Zinc dispersable tablets 20mg16. Quinine injection 300mg/ml; 2ml17. Quinine tab 300mg18. Quinine syrup 150/300mg19. 25% Dextrose IV infusion20. Artemether Lumefantrine (Alu) (paediatric21. Paracetamol tab 500mg22. Paracetamol syrup 120mg23. Vitamin A 200,000 IU oil capsule with nipple24. Vitamin A 100,000 IU oil capsule with nipple25. Vitamin A 50,000 IU oil capsule with nipple26. Oxytetracycline eye ointment 0.1% 5g tube27. Cipr<strong>of</strong>loxacin ear drops28. Ferrous Sulphate 100mg/ml29. Ferrous fumarate 20mg/ml30. Fe/folic acid tab 200mg/0.25 mg31. Nystatin oral susp 100,000IU/ml32. Gentian Violet paint 0.5%33. Mebendazole tab 500mg34. Formula 100 (F100)35. Formula 75 (F-75)36. Combined Mineral Vitamin Mix37. Metronidazole 250mg38. Daizepam inj 5mg/ml; 2ml vial39. Phenobarbi<strong>to</strong>ne inj 200mg/ml;40. Vitamin K1 inj41. Savlon solution42. Povidone Iodine solution10%43. Water for inj44. Metered infusion giving sets45. Cannula size 25G46. Cannula size 24G47. Scalp vien 23 G48. Blood infusion giving setsB. Child Essential equipment and supplies1. Oxygen concentra<strong>to</strong>r2. Haemoglobimometers3. Glucometers4. Glucostics5. Suction Machines6. Suction catheters 6FG, 8FG7. Paediatric resuscitation kit8. Nebulisers9. Paediatric infusion pump10. Warming devices11. Thermometers- normal reading12. Thermometers-low reading13. NGT, 5-814. Feeding cups15. Nasal prongs16. Weighing scale17. Syringes, disposable- 2mls/5mls18. Feeding syringes 20mls19. Feeding syringes 50mls20. Cot<strong>to</strong>n wool absorbent non sterile 500gm21. Plaster adhesive, plastic perforated 25mm x 10m22. RCH 1 card23. Methylated spirit24. Inpatient record book25. Inpatient moni<strong>to</strong>ring formC. Neonatal Essential Equipments and supplies:1. Towels2. Cord ties or clamp, sterile blade3. Container <strong>of</strong> eye ointment/drops4. Clock with second hand5. Clinical thermometers (preferably low reading6. Secca weighing scales7. Newborn size Masks, size 0 and 18. Self inflating bag9. Suction machine10. Suction tubes11. Surgical blades12. Surgical gloves and clean gloves13. Canulas14. Bucket <strong>of</strong> water15. Small graduated feeding cups16. Container for expressed breast milk17. Kettle or jug18. Gallipot19. Heater radiant/movable20. Resuscitation tables21. Pho<strong>to</strong>therapy machines22. Pulse Oxemetry23. Stands24. Exchange blood transfusion set90
25. Linen Baby Package, blankets, sheets and pillowsfor mothers26. Scissors27. Waste disposal containersD. Maternal medicines1. Ergometrine 0.5mg inj2. Oxy<strong>to</strong>cin 5 IU/ml , 10 IU/ml;3. Frusemide 10mg / ml4. Magnesium Sulphate inj 50% (500mg / ml)5. Fe/ Folic acid 200mg /0.250mg tab6. Folic acid 5mg tab7. Ferrous Sulphate 100mg/ml8. Ferrous fumarate 20mg/ml9. Lidocaine inj 1% 10ml vial10. Mebendazole 100mg tab11. Aminophyline 100mg tab12. Aminophyline 25mg/ml 10ml inj13. Amoxycillin 250mg tab14. Methlydopa (Aldoment) 250mg15. Chloramphenicol inj 1g16. Co-trimoxazole 400/80mg tabs17. Cloxacillin 250mg tab18. Clotrimazole vaginal pessary19. Ceftriaxone 500mg tab20. Erythromycin 500mg tab21. Cipr<strong>of</strong>loxacin 500mg tab22. Tetracycline or doxycycline500mg tab23. Diazepam 5mg/ml 2ml inj24. Doxycycline 100mg tabs25. Epinephrine (Adrenaline) 1mg/ml inj; 1ml26. Metronidazole 250mg tab27. Procaine penicillin Fort. 4MU/vial28. Sulfadoxine 500mg/Pyrimethamine 25 mg (SP) tabs29. Nevirapine (adult, infant)30. Zidovudine (AZT) (adult, infant)31. Lamivudine (3TC)32. FP contraceptive - pills (COC,POC), injectables,IUCD, condoms ( FP & HIV prevention)33. Vaccine - Tetanus <strong>to</strong>xoid , BCG, OPV, DTP, Measles34. Dextrose 5% (IV infusion)35. Normal Saline 0.9% (IV infusion)36. Ringers lactate IV infusion37. Glucose 50% solution38. Water for injectionE. Maternal essential equipment and supply1. Infusion giving sets (I.V giving set)2. Blood infusion giving sets3. Cannula size 14 – 18 G4. Catgut chromic 2.0, 3.05. Cot<strong>to</strong>n wool absorbent non sterile 500g6. Gauze absorbent BPC 90 cm x 100m hosp quality7. Surgical latex rubber sterile gloves 7.58. Syringe disposable 5ml + needle9. Syringe disposable 2ml + needle10. Catheters 30cc two ways11. Umbilical cord tie, cot<strong>to</strong>n, (Ligature) 3mm; 100m12. Sheeting rubber Mackin<strong>to</strong>sh 1 meter13. Cot<strong>to</strong>n sheet / green 1 meter14. Savlon solution15. Povidone Iodine solution 10%16. Bleach (chlorine base compound)17. Soap bar 113g18. Impregnated bed net19. Register Books for – ANC, FP, Delivery, Neonatal,Child, Postnatal20. Client cards - Ante-natal cards -RCH 4, FP card -RCH 5F. Maternal equipment1. Blood pressure machine and stethoscope2. Foetal stethoscope3. Delivery kit4. Lapara<strong>to</strong>my set5. IUCD insertion kit6. Manual Aspiration kit7. Vacuum extrac<strong>to</strong>r, Bird, manual/SET,8. D&C curettage /SET:9. Dressing Tray, sets, 300 x 200 x 30 mmG. Maternal tests reagents1. RPR testing kit;2. Test strips for urinalysis, glucose ,protein ,;3. HIV testing kit (2 types),4. Hemoglobin testing kit5. Container for catching urine,91
ANNEX 9GLOSSARYBasic emergency obstetric care:Caesarean section rateComprehensive emergency obstetriccareContraceptive Prevalence rateExclusive breast feedingInfant mortality rateMaternal deathMaternal mortality ratioNeonatal deathNeonatal mortality ratePerinatal deathsReproductive healthSkilled careSkilled attendantsUnder-five mortality rateFunctions that can be provided by an experienced nurse/midwife orphysician, saving the lives <strong>of</strong> many women, and stabilizing women whoneed <strong>to</strong> go further for more sophisticated treatmentNumber <strong>of</strong> caesarean section performed per <strong>to</strong>tal number <strong>of</strong> birthsIncludes basic EMOC functions as well as blood transfusion andcaesarean sectionsComprehensive Post Abortion CareThe percentage <strong>of</strong> women using method <strong>of</strong> family planningAn infant receives only breast milk and no other liquids or solids, NOTeven water, with the exception <strong>of</strong> drops or syrups consisting vitamins,mineral supplements <strong>of</strong> medicines.The probability <strong>of</strong> dying before the first birthday expressed per 1000 livebirthsThe death <strong>of</strong> a woman while pregnant or within 42 days <strong>of</strong> termination <strong>of</strong>pregnancyThe number <strong>of</strong> pregnancy rated deaths per 100,000 live birthsProbability <strong>of</strong> dying within the first 28 days birth.Probability <strong>of</strong> dying within the first month <strong>of</strong> life expressed per 1000 livebirthDeath <strong>of</strong> a foetus from 28 weeks <strong>of</strong> gestation <strong>to</strong> seven completed days <strong>of</strong>life including still birthsReproductive health is a state <strong>of</strong> complete physical, mental and socialwell being and not merely the absence <strong>of</strong> disease or infirmity, in allmatters relating <strong>to</strong> reproductive system and its functions and process. Thisimplies the rights <strong>to</strong> have satisfying and safe sex life, the capability <strong>to</strong>reproduce and the freedom <strong>to</strong> decide if, when and how <strong>of</strong>ten <strong>to</strong> do so.Refers <strong>to</strong> the care provided <strong>to</strong> the woman and her newborn duringpregnancy, childbirth and immediately after, by an accredited andcompetent provider who has at her/his disposal necessary equipment andthe support <strong>of</strong> a functioning health system including transport and referralfacilities for emergency obstetric and newborn care.Is an accredited health pr<strong>of</strong>essional such as the midwife, doc<strong>to</strong>r or a nursewho has been educated and trained <strong>to</strong> pr<strong>of</strong>iciency in the skills needed <strong>to</strong>manage normal (uncomplicated) pregnancies, childbirth and theimmediate postnatal period, and in the identification, management andreferral <strong>of</strong> complication in women and newborns.The probability <strong>of</strong> dying between birth and fifth birthday92
REFERENCESAjibola S. (2004). African Health Moni<strong>to</strong>r: Reducing Maternal and Newborn Mortality in Africa; WHORegional Office for Africa, Brazzaville; AFRICAN HEALTH MONITOR.Bale J.R. Stall B.J. Lucas A.O. (eds.) (2003). Improving Birth Outcomes: Meeting the Challenges in DevelopingWorld, A Committee on Improving Birth Outcome Board on Global Health; Washing<strong>to</strong>n D.C. THE NATIONALACADEMIC PRESS.Hinderraker et al., BJOG, 2003Liljestrand, J. and Gryboski, K. Maternal mortality as a Human Rights Issue. In Murphy, E. And Ringheim,K, eds. Reproductive Health and Rights: reaching the Hardly Reached. Washing<strong>to</strong>n, DC: PATH (2001).Mswia R., Lewanga M et al, (2003). Community Based Moni<strong>to</strong>ring <strong>of</strong> Safe Motherhood in United Republic <strong>of</strong>Tanzania, WHO Bulletin 81:87-94.<strong>National</strong> Bureau <strong>of</strong> Statistics, Dar-es-Salaam, ORC Macro, Calver<strong>to</strong>n, Maryland, USA: Tanzania Demographicand Health Survey, 1996.<strong>National</strong> Bureau <strong>of</strong> Statistics, Dar-es-Salaam, ORC Macro, Calver<strong>to</strong>n, Maryland, USA: Tanzania ServiceProvision Assessment Survey 2006 (TSPA).<strong>National</strong> Bureau <strong>of</strong> Statistics, Dar-es-Salaam, ORC Macro, Calver<strong>to</strong>n, Maryland, USA: Tanzania Demographicand Health Survey, 2004-2005.Regional Reproductive Health Newsletter (2004). <strong>Road</strong> <strong>Map</strong>: African Union resolves <strong>to</strong> tackle MaternalMortality: DIVISION OF FAMILY AND REPRODUTIVE HEALTH (DRH) – WHO/AFRO.UNICEF. State <strong>of</strong> the World Children Report 2008.The Lancet Child Survival Series, Vol 362, 2003The Lancet Neonatal Series, Vol 365, 2005.The Lancet Maternal Series, Vol 368, 2006The Partnership for Maternal Newborn and Child Health (2006). Opportunities for Africa’s Newborns.Urassa E, Carlstedt A, Nystrom L, Massawe S, Lindmark G. 2002 Quality assessment <strong>of</strong> the antenatalprogram for anaemia in rural Tanzania. International Journal for quality in Health Care 14: 441-448.World Bank (1993). Human Development Report.WHO, UNICEF, UNFPA, WB (2005). Maternal Mortality Estimates.93
Reproductive and Child Health SectionApril 2008