Chronic Care in Europe Towards High Performing Health Systems
Chronic Care in Europe Towards High Performing Health Systems
Chronic Care in Europe Towards High Performing Health Systems
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Chronic</strong> <strong>Care</strong> <strong>in</strong> <strong>Europe</strong><strong>Towards</strong> <strong>High</strong> Perform<strong>in</strong>g <strong>Health</strong> <strong>Systems</strong>Becom<strong>in</strong>g the Best: Build<strong>in</strong>g Susta<strong>in</strong>ability<strong>High</strong> Perform<strong>in</strong>g <strong>Health</strong> <strong>Systems</strong>Institute of <strong>Health</strong> Economics, Alberta, 15 April 2011Ellen NolteCécile Knai, Annalijn Conkl<strong>in</strong> and the DISMEVAL Consortium
There is a grow<strong>in</strong>g number of peoplewith chronic illness‣ ~20% to over 40% of population <strong>in</strong> EU aged 15 years and overreport a long stand<strong>in</strong>g health problem‣ ~ 2/3 of those who have reached pensionable age have at least2 chronic conditions‣ People with chronic diseases are more likely to utilise healthservices‣ Individual chronic diseases (e.g. diabetes) account for 2-15% ofnational health expenditure <strong>in</strong> some <strong>Europe</strong>an countriesSources: van den Akker et al., 1998; DZA 2005; Suhrcke et al. 2005; Eurobarometer 2007
Requirements for chronic illness careGoals• enhance functional status, m<strong>in</strong>imise distress<strong>in</strong>g symptoms,prolong life through secondary prevention and enhance quality oflifeRequirements• complex response over extended period of time• co-ord<strong>in</strong>ated <strong>in</strong>puts from a wide range of professionals• access to essential medic<strong>in</strong>es and monitor<strong>in</strong>g systems• promotion of active patient engagement
<strong>Health</strong>care not well equipped to meetrequirements of chronic illness care‣ Fragmentation of services act<strong>in</strong>g as barrier tocoord<strong>in</strong>ation of services along the cont<strong>in</strong>uum of care• structural and f<strong>in</strong>ancial barriers divid<strong>in</strong>g providers at theprimary/secondary care (& at the health and social care<strong>in</strong>terface)• dist<strong>in</strong>ct organisational and professional cultures anddifferences <strong>in</strong> terms of governance and accountability‣ Fail<strong>in</strong>gs <strong>in</strong> care coord<strong>in</strong>ation not only <strong>in</strong> countriestraditionally characterised by fragmentation‣ '[v]ery few health systems, even those that rate high onprimary care, achieve high coord<strong>in</strong>ation of care‘ (Starfield etal. 2005)
Patients with chronic disease reportdeficiencies <strong>in</strong> care coord<strong>in</strong>ation1008060%40200<strong>in</strong>efficient care/time wastedspecialist did not have <strong>in</strong>formation on medical historydischarge gapsSource: Schoen et al. 2009
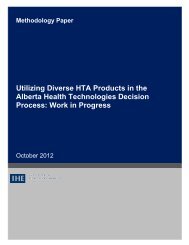
Source: Powell Davies et al. 2008Evidence that care coord<strong>in</strong>ationimproves outcomesMa<strong>in</strong> focus of <strong>in</strong>tervention(number of studies)Changed relationships between serviceproviderse.g. case management, multi-discipl<strong>in</strong>ary teams (33)Coord<strong>in</strong>ation of cl<strong>in</strong>ical activitiese.g. jo<strong>in</strong>t consultations, shared assessments (37)Improv<strong>in</strong>g communication between serviceproviderse.g. case conferences (56)Support for cl<strong>in</strong>icianse.g. supervision for cl<strong>in</strong>icians, rem<strong>in</strong>der systems (33)Information systems to support co-ord<strong>in</strong>atione.g. care plans; decision support; register (47)Support for health/social care service userse.g. education, rem<strong>in</strong>ders; assistance (19)Proportion (%) of studies with positiveoutcome for<strong>Health</strong>65.5%(19/29)61.3%(19/31)55.3%(26/47)57.1%(16/28)60.5%(23/38)35.3%(6/17)All studies 55.4%(36/65)Service usersatisfaction66.7%(8/12)33.3%(4/12)54.5%(12/22)57.1%(8/14)36.8%(7/19)50.0%(3/6)45.2%(14/31)Cost sav<strong>in</strong>g16.7%(2/12)20%(3/15)14.3%(2/21)8.3%(1/12)15.4%(2/13)14.3%(1/7)17.9%(5/28)
Support for patient engagement andself-management rema<strong>in</strong>s sub-optimal1008060%40200discuss goalsgiven written planalways given clear <strong>in</strong>structions about symptoms to watch out forSource: Schoen et al. 2009
What does this mean for health systems?‣ An effective response to the ris<strong>in</strong>g burden of chronicdisease requires a health system environment that allowsfor the development and implementation of structuredapproaches to chronic disease management‣ Countries are develop<strong>in</strong>g new models of healthcaredelivery to achieve better coord<strong>in</strong>ation of services acrossthe entire cont<strong>in</strong>uum of care‣ Review of approaches and models <strong>in</strong> place <strong>in</strong> 13countries across <strong>Europe</strong>
HE Pr<strong>in</strong>cipal fund<strong>in</strong>g Governance of the public health system(US$PPP)Austria 3,836 Statutory health<strong>in</strong>suranceResponsibility shared by central government, n<strong>in</strong>e state governments andcorporatist actors; states responsible for hospital sectorDenmark 3,630 General taxation Responsibility shared by central government, regions and municipalitiesEngland(UK)(3,230) General taxation Responsibility is at central level by government and agencies at arm’s lengthfrom government; local organisations organise healthcare deliveryEstonia 1,226 Statutory health<strong>in</strong>suranceFrance 3,778 Statutory health<strong>in</strong>suranceGermany 3,692 Statutory health<strong>in</strong>suranceHungary 1,419 Statutory health<strong>in</strong>suranceItaly 2,825 National andregional taxationResponsibility concentrated at the central level with some <strong>in</strong>volvement of localauthorities especially <strong>in</strong> the hospital sectorResponsibility traditionally concentrated at national level with gradualdecentralisation of (selected) governance functions to regional agenciesResponsibility for the health system shared by central government, 16 stategovernments and corporatist actors; states responsible for hospital sectorResponsibility for the health system is at central level by government andagencies at an arm’s length from governmentResponsibility for the health system is shared by the central government andthe 20 regions with regions hav<strong>in</strong>g extensive autonomyLatvia 1,112 General taxation Responsibility for the health system is concentrated at the central level bygovernment and agencies at an arm’s length from governmentLithuania 1,178 Statutory health<strong>in</strong>suranceNetherlands 3,749 Statutory health<strong>in</strong>suranceSpa<strong>in</strong> 2,791 National andregional taxationSwitzerland 4,620 Mandatory health<strong>in</strong>suranceResponsibility for the health system is concentrated at the central levelResponsibility for the health system shared by federal and local authorities andcorporatist actorsResponsibility for organis<strong>in</strong>g publicly funded healthcare rests largely with the 17regions; national government sets regulatory framework and allocates fund<strong>in</strong>gShared by the federal and 26 cantonal governments with the cantons hav<strong>in</strong>gextensive autonomy
Conceptual framework for assessment:<strong>Chronic</strong> care modelSource: Wagner 1998
The majority of approaches tend to focuson populations with def<strong>in</strong>ed conditions‣ Most frequently targeted conditions: diabetes type 2,asthma/COPD, cardiovascular disease (chronic heart failure,IHD, stroke), cancer, mental health problems‣ Approaches with generalist focus tend to be organised aroundolder people• Frequently available <strong>in</strong> selected regions only and/or operated aspilot studies‣ Types of approaches vary across and with<strong>in</strong> countries• <strong>Care</strong> coord<strong>in</strong>ation (GP acts as pr<strong>in</strong>cipal coord<strong>in</strong>ator) and• Multidiscipl<strong>in</strong>ary team work<strong>in</strong>g (frequently led by GP)• Managed discharge• Nurse-led care• Case management
The majority of approaches tend to focuson populations with def<strong>in</strong>ed conditions‣ Most frequently targeted conditions: diabetes type 2,asthma/COPD, cardiovascular disease (chronic heart failure,IHD, stroke), cancer, mental health problems‣ Approaches with generalist focus tend to be organised aroundolder people• Frequently available <strong>in</strong> selected regions only and/or operated aspilot studies‣ Types of approaches vary across and with<strong>in</strong> countries• <strong>Care</strong> coord<strong>in</strong>ation (GP acts as pr<strong>in</strong>cipal coord<strong>in</strong>ator) and• Multidiscipl<strong>in</strong>ary team work<strong>in</strong>g (frequently led by GP)• Managed discharge• Nurse-led care• Case management
Strengthen<strong>in</strong>g coord<strong>in</strong>ation throughstructured disease management‣ ‘Disease management programmes’• Austria: ‘Therapie aktiv’ (diabetes) (national); regional projects• Denmark: DMPs (various) (national through regions)• France: Sophia (diabetes) (national)• Germany: DMPs (various) (national)• Hungary: DMP (asthma) (national); diabetes care management(national)• Netherlands: <strong>Care</strong> groups (various) (national)‣ wide variation <strong>in</strong> extent to which non-medical staff is <strong>in</strong>volved<strong>in</strong> care delivery (e.g. Netherlands, Hungary, Italy)‣ GP/family physician tends to rema<strong>in</strong> pr<strong>in</strong>cipal provider/’carecoord<strong>in</strong>ator’ (e.g. Austria, Germany, France)
Strengthen<strong>in</strong>g the role of nurses <strong>in</strong> caredelivery and coord<strong>in</strong>ation‣ Common <strong>in</strong> systems with tradition <strong>in</strong> multidiscipl<strong>in</strong>ary teamwork<strong>in</strong>g‣ Nurse-led cl<strong>in</strong>ics• England, Hungary, Italy, Netherlands‣ Nurse-led case management• England, Italy, Netherlands, Spa<strong>in</strong>‣ Challeng<strong>in</strong>g <strong>in</strong> systems where primary care traditionallyprovided by doctors <strong>in</strong> solo-practice and few support staff• Enhanced functions <strong>in</strong> care coord<strong>in</strong>ation or case managementunder development/piloted (e.g. Denmark, France; Lithuania)• Enhanced functions <strong>in</strong> patient self-management support and/orselected medical tasks but under supervision of GP/physician(Austria, France, Germany)
Reduc<strong>in</strong>g barriers between sectors‣ Manag<strong>in</strong>g the primary/secondary care and/or secondarycare/rehabilitation <strong>in</strong>terface• Provider networks (France)• Integrated care contract<strong>in</strong>g (Germany)• <strong>Care</strong> Coord<strong>in</strong>ation Pilot (Hungary)• ‘SIKS’ project (Copenhagen, Denmark)• ‘From On-demand to Proactive Primary <strong>Care</strong>’ (Tuscany, Italy)• (some) Reform pool projects (Austria)• Stroke service Delft (Netherlands)‣ Manag<strong>in</strong>g the health and social care <strong>in</strong>terface• (some) Integrated <strong>Care</strong> Pilots (England)• Partnership for Older People Project (England)• Multifunctional community centres (Hungary)• Improv<strong>in</strong>g <strong>in</strong>tersectoral collaboration (pilot) (Lithuania)
The majority of approaches are fundedfrom ‘usual’ sources‣ Start-up fund<strong>in</strong>g‣ Support<strong>in</strong>g payers (municipalities, Denmark; <strong>in</strong>tegrated carepilots, England; <strong>in</strong>tegrated care contracts, Germany)‣ Support<strong>in</strong>g providers (provider networks, France)‣ F<strong>in</strong>ancial <strong>in</strong>centives‣ Incentivise payers (municipalities, Denmark; DMPs, Germany)‣ Incentivise providers (DMPs, Austria; GPs (diabetes care),Denmark; provider networks, France; DMPs, Germany; someregional projects, Italy; care groups, Netherlands; Quality &Outcomes Framework, UK)‣ Incentivise patients (provider networks, France; DMPs,Germany; care groups, Netherlands)
Approaches generally provide some formof patient self-management support‣ Wide variation <strong>in</strong> the level of support provided• Provision of <strong>in</strong>formation material (eg brochures, <strong>in</strong>teractivewebsite) access to coach<strong>in</strong>g and counsell<strong>in</strong>g• Patient <strong>in</strong>volvement <strong>in</strong> development of treatment plan and goalsett<strong>in</strong>g common <strong>in</strong> theory, level of implementation <strong>in</strong> practiceunclear• Support typically provided by health professionals‣ Typically provided by physician or tra<strong>in</strong>ed nurse‣ Lay-led support uncommon (eg Expert Patients Programme(EEP) <strong>in</strong> England; EEP adaptation <strong>in</strong> selected regions <strong>in</strong> Spa<strong>in</strong>)
The use of elements of decision-supportand cl<strong>in</strong>ical <strong>in</strong>formation systems varies‣ Elements of decision-support most commonly <strong>in</strong>clude guidel<strong>in</strong>esand protocols• Dedicated staff tra<strong>in</strong><strong>in</strong>g common for those strategies that <strong>in</strong>volvedelegation of tasks to non-medical staff‣ Use of cl<strong>in</strong>ical <strong>in</strong>formation systems tends to be the leastdeveloped strategy <strong>in</strong> most approaches• Usually limited to participants with<strong>in</strong> a given care approachand/or standardises documentation for quality assurance• England and Estonia provide examples for consistent use ofstandardised electronic medical records, electronic book<strong>in</strong>g andrem<strong>in</strong>der systems throughout the primary care system
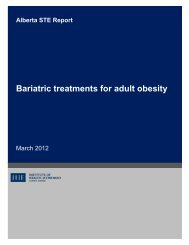
Population segmented across the spectrum of ‘health risk’<strong>Health</strong>yLow<strong>High</strong>DiagnosisDiseaseTreatmentComplicationsManagementRisk m<strong>in</strong>imisationDisease managementAcute careSource: adapted from Petersen & Kane 1997
Integrat<strong>in</strong>g prevention <strong>in</strong>to chronic care‣ “In Austria the area of risk m<strong>in</strong>imisation ... is still considered as lessimportant (perhaps not <strong>in</strong> theory, but certa<strong>in</strong>ly when it comes to f<strong>in</strong>d<strong>in</strong>gf<strong>in</strong>ancial means for those programmes). Approaches concern<strong>in</strong>gdisease management are start<strong>in</strong>g to get some attention at the moment.Provisions for acute care are very good”[Austria]‣ “[T]he Netherlands is good at the diagnosis phase and good atcomplications treatment [and] the last few years is ga<strong>in</strong><strong>in</strong>g more<strong>in</strong>terest <strong>in</strong> disease management ... Risk m<strong>in</strong>imisation or prevention, thediscussion is start<strong>in</strong>g, the discussion of who is <strong>in</strong> charge of riskm<strong>in</strong>imisation, the people themselves or local government or the health<strong>in</strong>surer... This is the discussion that runs now.”[Netherlands]
Fragmentation of responsibilitiesrema<strong>in</strong>s a challenge...‣ “[W]e have a very complicated political and governmental structure […];the national and regional governments […] have the competencies formost th<strong>in</strong>gs you can th<strong>in</strong>k of. But then we have councils […] <strong>in</strong> charge ofthe whole social th<strong>in</strong>g and they don’t manage the same budget and theydon’t have the same bosses or <strong>in</strong>terests. So there you have the bigproblem”[Spa<strong>in</strong>]‣ “[S]o we have ambulatory care, hospital care, we have some services,public or private, <strong>in</strong> try<strong>in</strong>g to do some preventive care but they are verydisconnected and fragmented ... prevention is weak and is a big issue,the reaction to that from the state has been, you know, they just produceplans .... There is not a systemic reaction to how to improve prevention <strong>in</strong>general.”[France]
... as does the creation of newresponsibilities...‣ “[T]he municipalities should have a central place <strong>in</strong> [solv<strong>in</strong>g] problems ofthe healthcare sector. [They have the responsibility] to create new healthcentres [...designed to overcome] barriers to coord<strong>in</strong>ation [but]municipalities do not have the competence and knowledge abouthealthcare. And there is no systematic development <strong>in</strong> this area; [...] it isdependent on learn<strong>in</strong>g from the regional level”[Denmark]
... and a cont<strong>in</strong>ued misalignment of(f<strong>in</strong>ancial) <strong>in</strong>centives‣ “the practitioners are paid by fee for service; [...] their vision of healthcarehas been for a long time about patients com<strong>in</strong>g to your office and yourprimary issue is to diagnose...”[France]‣ “[T]the problem with primary prevention is that sickness funds are <strong>in</strong>competition [but] primary prevention [efforts] have to be not only targetedto our own <strong>in</strong>surees but also on the <strong>in</strong>surees of other sickness funds. Sowe are not very motivated to make big primary prevention programmeswhen we know that other organisations will take benefit from it and wehave to pay for it.“[Germany]
<strong>Towards</strong> high perform<strong>in</strong>g health systemsKey elements‣ Provision of adequate <strong>in</strong>centives‣ Creation of an appropriately prepared workforce‣ Information technology‣ Embedd<strong>in</strong>g prevention <strong>in</strong> all stages‣ Creation of systems to enable patients to self-manage effectivelyNeed for‣ Contextually appropriate approaches‣ Consistency of policies‣ Balanc<strong>in</strong>g top-down and bottom-up‣ Ongo<strong>in</strong>g evaluation (what works best <strong>in</strong> what circumstances)
http://www.euro.who.<strong>in</strong>t/en/home/projects/observatory/publications/studies
www.dismeval.eu