

Treatment Summary User Guide - National Cancer Survivorship ...
Treatment Summary User Guide - National Cancer Survivorship ...
Treatment Summary User Guide - National Cancer Survivorship ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
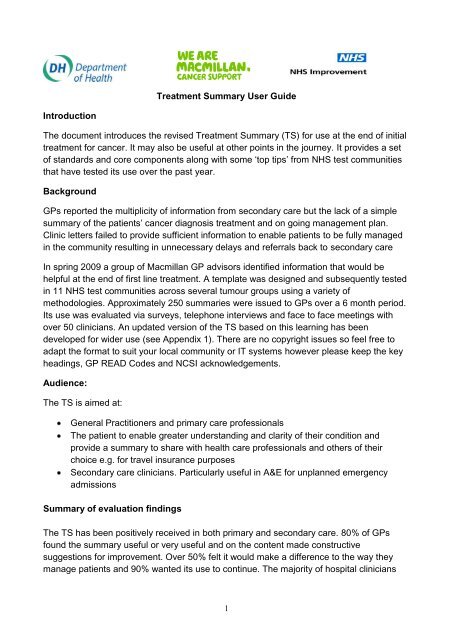
ecognised the value of summarising what could be months of treatment and holistic careinto a concise summary. Some voiced concerns about the complexity of content andlength of time it took to complete whilst others found it had little impact on time once theybecame familiar with it... One clinician felt that ‘it made us document and communicatebetter’ another thought it to be ‘excellent’. .Presentation and completion methodologyThere are three presentation styles organisations may wish to consider, the standardform/template, a letter that follows the template headings or an electronic solution.Most test communities used the template and boxes in the format provided, othersconverted to a letter template to improve ease of use by secretarial staff. Two sites createdelectronic versions using an access database with a series of drop down menus to aid thespeed of completion. One site transmitted the TS electronically to the GP, others printedand posted. One consultant completed the TS in place of the clinic letter and provided acopy for the patient to take with them when leaving the clinic.Recommended PracticeThe following standards support the use of the TSThe completed TS should be sent to both the patient (having agreed to be copied intoall correspondence) and the GP within 2 weeks of the appointment at the end oftreatmentTS updates should be generated at other key points e.g. following recurrence, furthertreatment or a transition to end of life careEffort should be made to complete all sections. Information about prognosis should becompleted sensitively and in accordance with the patient wishes.The TS should not replace detailed care plan based on an assessment of needMembers of the MDT involved in the patients care should contribute to the completionof the TSGPs should be encouraged to use the TS in conjunction with <strong>Cancer</strong> Care Review andto highlight any necessary monitoring or reviews requiredRevised <strong>Treatment</strong> <strong>Summary</strong> templatesThe TS has been amended since testing to remove less useful informationAppendix 1 provides the revised TS template with updated GP READ codes.Appendix 2 provides a user guide with rational for data inclusion and an indication ofthe essential and desirable fields required should local re-design of the form bepreferred.Appendix 3 provides an example template with prompt notes2
Appendix 4 provides the same information in a letter templateHints and Tips for implementation:The following hints and tips have been provided by the NHS Improvement testcommunities:Engage administrative staff early in change process and encourage them to suggestthe best way to implement locallyKeep primary leads informed of planned changes to documentation and be receptive tofurther changes they may suggest.Avoid handwriting the TS - type wherever possibleProvide a laminated prompt list in clinic for clinicians to use as they dictateTo encourage uptake, encourage testing for say 5 patients and then review contentand process. Ensure process review occurs.If redesigning template beware of removing fields as they may be useful to othersCreate template letter with headings to enable easier typingUse the TS in place of a clinic letter on one clinic occasion and retain a copy in thecase notesEnsure that the medical records department are aware of the additional proforma andaware of the appropriate place in the notes for filing (this will avoid them being removedfrom the patient’s records inappropriately).Colour code the form/letter to denote sections for doctor and CNS to completeTo save time some sections can be completed by others prior to the appointment withthe remaining sections completed by the doctor at the timeAttach the template prompt list to the front of case notes prior to the patient being seenin clinic as a reminder to complete on this visitPre-fill the boxes where possible such as for common signs and symptoms ofrecurrence, treatment toxicitiesFor complex tumour group consider separate list of signs and symptoms, what to doand key contacts if help required (examples available on request to NHS Improvement<strong>Survivorship</strong> Team)If template set up as electronic database, add common signs symptoms andmedications as drop down menusShare testing and experience with other colleagues to encourage wider testing andspread of the use of the TS.Provide GP READ codes attached to each letter or issue separatelyFeedbackTo provide feedback and comment please contact: survivorshipteam@macmillan.org.ukor Dr Rosie Loftus – GP Macmillan Lead rloftus@macmillan.org.uk or Noeline Youngnyoung@macmillan.org.uk3
Appendix 1<strong>Treatment</strong> <strong>Summary</strong>Insert GP Contact DetailsLogo and AddressInsert TrustDear Dr XRe: Add in patient name, address, date of birth and record numberYour patient has now completed their initial treatment for cancer and a summary of their diagnosis,treatment and ongoing management plan are outlined below. The patient has a copy of thissummary.Diagnosis: Date of Diagnosis: Organ/StagingLocal/Distant<strong>Summary</strong> of <strong>Treatment</strong> and relevant dates:<strong>Treatment</strong> Aim:Possible treatment toxicities and / or late effects:Alert Symptoms that require referral back to specialist team:Advise entry onto primary care palliativeor supportive care registerYes / NoDS 1500 application completedYes/NoPrescription Charge exemptionarrangedYes/NoContacts for re referrals or queries:In Hours:Out of hours:Other service referrals made: (delete asnec)Secondary Care Ongoing Management Plan: (tests, appointments etc) District NurseAHP.Social WorkerDieticianClinical Nurse SpecialistPsychologistBenefits/Advice ServiceOtherRequired GP actions in addition to GP <strong>Cancer</strong> Care Review (e.g. ongoing medication, osteoporosis or cardiac screening)<strong>Summary</strong> of information given to the patient about their cancer and future progress:Additional information including issues relating to lifestyle and support needs:Completing Doctor: Signature: Date:4
GP READ CODES FOR COMMON CANCERS (For GP Use only). Other codes available if required.(Note: System codes are case sensitive so always ensure codes are transcribed exactly as below).System 1(5 digitcodes)All other systemsVersion 3 fivebyte codes(October 2010release)Diagnosis:DiagnosisLung Malignant Tumour XaOKG Malignant neoplasm of bronchus or B22z.lungCarcinoma of Prostate X78Y6 Malignant neoplasm of prostate B46..Malignant tumour of rectum XE1vW Malignant neoplasm of Rectum B141.Bowel Intestine X78gK Malignant neoplasm of Colon B13..Large Bowel X78gN Malignant neoplasm of female breast B34..Female Malignant Neoplasia B34.. Malignant neoplasm of male breast B35..Male Malignant NeoplasiaB35..Histology/Staging/Grade:Histology/Staging/Grade:Histology Abnormal 4K14. Histology Abnormal 4K14.Tumour grade X7A6m Tumour staging 4M…Dukes/Gleason tumour stage XaOLF Gleason grading of prostate Ca 4M0..Recurrent tumour XaOR3 Recurrence of tumour 4M6..Local Tumour SpreadX7818Mets from 1° XaFr. Metastatic NOS BB13.<strong>Treatment</strong><strong>Treatment</strong>Palliative Radiotherapy 5149. Radiotherapy tumour palliation 5149.Curative Radiotherapy XalpH Radiotherapy 7M371Chemotherapy x71bL Chemotherapy 8BAD.RadiotherapyXa851<strong>Treatment</strong> Aim:<strong>Treatment</strong> Aim:Curative procedure Xallm Curative treatment 8BJ0.Palliative procedure XaiL3 Palliative treatment 8BJ1.<strong>Treatment</strong> toxicities/late effects:Osteoporotic # Xa1TO At risk of osteoporosis 1409.Osteoporosis XaELC Osteoporosis N330.InfectionXa9uaOngoing Management PlanOngoing Management PlanFollow up arranged (1yr)XaL..No FU 8HA1. No follow up arranged 8HA..Referral PRN8HAZ.Referrals made to other services:Referrals made to other services:District Nurse XaBsn Refer to District Nurse 8H72.Social Worker XaBsr Refer to Social Worker 8H75.Nurse SpecialistXaAgqSALTXaBT6Actions required by the GPActions required by the GPTumour marker monitoring Xalqg Tumour marker monitoring 8A9..PSA Xalqh PSA 43Z2.Osteoporosis monitoring XalSd Osteoporosis monitoring 66a..Referral for specialist opinion XalstAdvised to apply for freeprescriptions9D05 Entitled to free prescription 6616.5
<strong>Cancer</strong> Care Review Xalyc <strong>Cancer</strong> Care Review 8BAV.Palliative Care Review XalG1 Palliative Care Plan Review 8CM3.Medication:Medication:New medication started byXEOhn Medication given 8BC2.specialistMedication changed by specialist 8B316 Medication changed 8B316Advice to GP to start medication XaKbFAdvice to GP to stop medication XaJC2Information to patient:Information to patient:DS1500 form claim XaCDx DS1500 completed 9EB5.Benefits counselling 6743. Benefits counselling 6743.<strong>Cancer</strong> information offered XalmL <strong>Cancer</strong> information offered 677H.<strong>Cancer</strong> diagnosis discussed XalpL <strong>Cancer</strong> diagnosis discussed 8CL0.Aware of diagnosisXaQlyUnaware of prognosisXaVzECarer aware of diagnosisXaVzAMiscellaneous:Miscellaneous:On GSF palliative care framework XaJv2 On GSF Palliative Care Framework 8CM1.GP OOH service notified Xaltp GP OOH service notified 9e0..Carers details 9180. Carer details 9180.6
<strong>Treatment</strong> <strong>Summary</strong> <strong>User</strong> <strong>Guide</strong> Appendix 2Field Rationale for inclusion EssentialorDesirableDiagnosisImportant for the GP and patient to know type of cancer and location of Ecancer and the likely source of secondary recurrence.Organ Staging/local or distant spread Information about staging and spread provides insight into prognosis and D(Grade)Date of Diagnosis<strong>Summary</strong> of <strong>Treatment</strong> and relevantdates<strong>Treatment</strong> AimPossible treatment toxicities and or lateeffects of treatmentAdvise entry onto palliative or supportivecare registerrisk of recurrenceTo understand length of time patient has known diagnosis and time periodbetween referral from primary care and diagnosis to learn where delayscan be minimised in future. Important data to monitor treatment outcomesin relation to survivorship. Helps plan date of GP <strong>Cancer</strong> Care Review.To understand the range and order of modality treatment, understand thelikely sequence of treatment effects. Essential to inform future treatmentchoice if further disease occurs. Important information for patients wishingto take out insurance or a mortgage.To understand whether treatment intended is curative, non curative,palliative or for symptom relief as this will help GPs to understand aims oftreatment and refer back to secondary care or other services appropriately.Also help GPs to anticipate future care needs.Patients undergoing cancer treatments may be more prone to toxicity andlate effects of treatment such as osteoporosis or heart disease. Inclusionof risks in this summary triggers the entering of the patient onto routine GPsurveillance (QOF related). Signs and symptoms addressed earlier mayimprove quality of life and treatment outcomes from side effects or lateconsequences of treatment.Inclusion of suggested or preferred treatment associated with toxicities andlate effects can be initiated without referral back to the specialist.Raises awareness of common late effects and reduces delays to furtherinvestigation and treatment. This may also impact on survival rates assymptoms are picked up soonerInclusion of the patient on the palliative care register ensures that theprimary health care teams are made aware that a patient is nearing end of7DEEED
DS 1500 status and prescriptionexemptionAlert symptoms that require referral backto specialist teamContact for re referrals or queries in andout of hoursSecondary Care On-going ManagementplanReferrals to other servicesRequired GP actions including medicationetclife and that increased input maybe required to support patient and carers.The register is shared with all relevant OOH doctors, ambulance service,community district nursing teams, Macmillan support team, social care,hospice as appropriate. Patients can then receive the appropriate support,information and benefits in a timely manner.If no DS 1500 completed the GP will be prompted to arrange. Also ensuresthat exemption charges are waived for any cancer treatment - anentitlement for all patients with a diagnosis of cancerThis should include those symptoms that may be suggestive of arecurrence or specific symptoms relating to the effects of treatment whereurgent referral back to the specialist team is advised.Confirms contact details for the patient or GP for advice on care ortreatment or to arrange urgent review. The out of hours contact could be award, the acute oncology team or relevant on call teamInclude any planned outpatient reviews and surveillance tests dates (orapproximated timescales). This provides a framework for GPs. If indicated,further tests can be scheduled prior to the further outpatient visits. Patientswill be better informed about follow up plans and what to expect. It isreassuring to patients and carers to see the planned care, surveillance andsupport, they then know what to expect and when.Helps avoid duplication of referral if the patient visits the GP betweenappointments and is unsure of who is involved in their care. Particularlyuseful in respect social care referrals and whether the patient is known toother agencies. Can help to reinforce the importance of attendingappointments with other agencies. Useful to also include details related tothird sector support and centres such as Maggie’s if available.To provide clarity on the expectation of GPs in respect of the patients ongoingcare and how they can support them. Also provides prompts e.g. toadd patients to routine screening programmes to help mitigate late effectsof treatment. Patients will be more empowered to approach GPs if theyrequire further advice and support. Can give specific request to GPs toensure continuity of care and avoid ambiguity. Provides GPs with guidanceand advice on which drugs if any need stopping and when and whetherDEEEDE8
<strong>Cancer</strong> Care Review<strong>Summary</strong> of information given to thepatient about their cancer and futureprognosisAdditional Information given includingissues relating to lifestyle and supportneedsREAD Codesany adjusting between follow up appointments or following discharge. Mayavoid inappropriate prescriptions, overdose or misuse. Particularlyimportant if the GP is going to continue to prescribe long term i.e.endocrine manipulation. Patients will also know what to expect from GP.Inclusion of this reminder helps ensure the patient is entered onto theregister and that they are formally reviewed by the GP within 6 months ofdiagnosis. This is a requirement for QOF points within all general practicesSharing information on what has been discussed with the patient and theircarer improves the quality and openness of the discussion that the GP canhave with the patient.To confirm which lifestyle advice has been given or signposted and detailsof local support groups and psychosocial support, complementarytherapies, returning to work advice etcGP READ codes are similar to hospital HRG codes and used to identifydiagnosis, tests and treatments. Both are complex systems and requiremanual input. Inclusion of the READ codes in the TS prompts andencourages GPs to accurately code patients. This helps improve patientsafety in terms of surveillance, disease tracking and audit. It is theresponsibility of the GPs to assign the appropriate codes and enter on theirsystems. Note Codes may differ depending on GP IT system in useDE*DD9
<strong>Treatment</strong> <strong>Summary</strong> Example Appendix 3Dear Dr JonesRe: John Smith, Somewhere Road, Anywhere AB1 CD23 DoB: 10.10.10 NHS No: 123456Your patient has now completed their initial treatment for cancer and a summary of their diagnosis;treatment and ongoing management plan are outlined below. The patient has a copy of this summary.Diagnosis:Colorectal <strong>Cancer</strong>Date of Diagnosis:10 th Feb 2010Organ/Staging – Dukes T2Local/Distant – N0<strong>Summary</strong> of <strong>Treatment</strong> and relevant dates:Surgery – Resection (March 10) and reversal of stoma (Sept 10)Radiotherapy - May – June 2010Possible treatment toxicities and / or late effects:Diarrhoea following pelvic radiotherapy.<strong>Treatment</strong> Aim:CurativeAdvise entry onto primary carepalliative or supportive care registerNoDS1500 application completed- NoPrescription Charge exemptionarranged- YesAlert Symptoms that require referral back to specialist team:Diarrhoea for more than 2 weeks not relieved by loperamide/codeineBlood or mucus per rectumFurther change in bowel functionAbdominal pain that persists for longer than 4 weeks and does notrespond to simple analgesiaContacts for re referrals or queries:In Hours: 01234 567890 (CNS team)Out of hours: 01234 987654 (oncologyward)Referrals made to other services:Secondary Care Ongoing Management Plan: (tests, appointments etc)Community DieticianBenefits/Advice ServiceNext OP Review - Jan 2011CEA next due in Jan 2011 then annually until 2015CT scan (abdo and chest) next due Sept 2011Colonoscopy repeat next due Sept 2015Required GP actions in addition to GP <strong>Cancer</strong> Care Review (e.g. ongoing medication, osteoporosis or cardiacscreening)Please review dose of XXXXX in two months. if symptoms of XXXX resolved reduce to 4mg daily<strong>Summary</strong> of information given to the patient about their cancer and future progress:Patient and wife informed that the cancer in his colon was non invasive and that he has received surgery and radiotherapywith curative intent. He is aware however that it may recur in the future and we have briefly discussed the further treatmentavailable should this be required. He is fully aware of the symptoms of recurrence and what to do should any occur.Additional information relating to lifestyle and support needsPatient advised to quit smoking and referred to smoking cessation clinicPatient keen to join local colorectal support group and plans to attend next session in NovemberCompleting Doctor: Charles Goodenough Signature: Date: 30.10.1010
Template in letter formatAppendix 4Date: XXXXXXXXDear Dr Enter GP name XXXXRe:Your patient has now completed their initial treatment for cancer and a summary of their diagnosis;treatment and ongoing management plan are outlined below. The patient has a copy of this summary.Diagnosis:Date of diagnosis:Organ/Staging:Local/Distant<strong>Summary</strong> of <strong>Treatment</strong> and relevant dates:<strong>Treatment</strong> Aim:Possible treatment toxicities and / or late effects:Alert symptoms that require referral back to specialist team:Secondary Care Ongoing Management Plan: (tests, appointments etc)Other service referrals made: e.g. Dietician, Psychologist, Social WorkerRequired GP actions in addition to <strong>Cancer</strong> Care Review (e.g. Medication, osteoporosis/cardiacscreening)<strong>Summary</strong> of information given to the patient about their cancer and prognosis:Additional information including issues related to lifestyle and support needs:Advise on entry to primary care palliative or supportive care register: (Yes/No)DS1500 application completed: (Yes/No/N/A)Prescription charge exemption arranged: (yes or No)Contact for re-referral or any queries;In hoursOut of hours:Yours sincerelyConsultant xxxxxxxxCC: Insert patient name11





![Download the how to guide [PDF] - Macmillan Cancer Support](https://img.yumpu.com/47067428/1/184x260/download-the-how-to-guide-pdf-macmillan-cancer-support.jpg?quality=85)






![HOPE Protocol [PDF, 420KB] - National Cancer Survivorship Initiative](https://img.yumpu.com/32566432/1/184x260/hope-protocol-pdf-420kb-national-cancer-survivorship-initiative.jpg?quality=85)