SECTION 5: Provider Claims Information - TRICARE Overseas
SECTION 5: Provider Claims Information - TRICARE Overseas
SECTION 5: Provider Claims Information - TRICARE Overseas

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
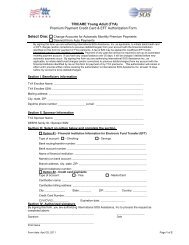
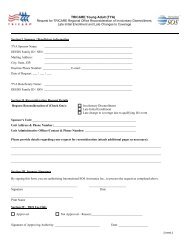
<strong>TRICARE</strong> overseas Program<strong>Provider</strong> ManualPart 1: Patient’s and Sponsor’s DetailsAlways choose the<strong>TRICARE</strong> option.Please enter the patient’sDOB using the formatMM DD YY and tick M or F toindicate the patient’s gender.Enter the sponsor’s ID number (10-digit DODBenefit or 9-digit Social Security Number (SSN))and name using the format Last Name, FirstName, Middle Initial. This information will appearon the patient’s Military ID Card.Enter the patient’s name,using the format Last Name,First Name, Middle Initial andthe patient’s full physicaladdress including post code.Enter the patient’s relationshipto the sponsor.Fields highlighted in greencan be left blankEnter the sponsor’sfull address if different thanthe patient’s.If the patient has OHI enterthe name of the insured partyusing the format Last Name,First Name, Middle Initial, thepolicy number and in field 9denter the name of theinsurance plan.<strong>TRICARE</strong> is always the secondarypayer. If the patient has OHI policy,tick ‘YES’ here and thencomplete 9, 9a and 9d.If the patient does not have OHIpolicy, section 9 can be left blank.Enter the sponsor’s DOB,using the format MM DD YYand indicate the sponsor’sgender marking either M forMale or F for Female.SECTIoN 5<strong>Provider</strong> <strong>Claims</strong> <strong>Information</strong>Fields highlighted in greencan be left blank59