THE PALLIATIVE CARE HANDBOOK Advice on clinical management
THE PALLIATIVE CARE HANDBOOK Advice on clinical management
THE PALLIATIVE CARE HANDBOOK Advice on clinical management

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<str<strong>on</strong>g>THE</str<strong>on</strong>g> <str<strong>on</strong>g>PALLIATIVE</str<strong>on</strong>g> <str<strong>on</strong>g>CARE</str<strong>on</strong>g><str<strong>on</strong>g>HANDBOOK</str<strong>on</strong>g><str<strong>on</strong>g>Advice</str<strong>on</strong>g> <strong>on</strong> <strong>clinical</strong><strong>management</strong>SEVENTH EDITIONOctober 2010In associati<strong>on</strong> withWessex andAv<strong>on</strong>, Somerset & Wiltshire Cancer ServicesSpecialist Palliative Care Units
CONTENTSIntroducti<strong>on</strong> 3General principles of symptom <strong>management</strong> 4Guidance from NICE <strong>on</strong> Specialist Palliative Care 4Pain 5Use of str<strong>on</strong>g opioids 7Opioid preparati<strong>on</strong>s 9Relative potencies of various opioid analgesics 10Opioids and renal or hepatic impairment 12Opioids and driving 13Adjuvant treatments for specific pains 13Pains amenable to nerve blocks 15Acute pain of short durati<strong>on</strong> and Breakthrough pain 15N<strong>on</strong>-pharmacological approaches to pain c<strong>on</strong>trol 16Gastrointestinal symptomsNausea and vomiting 17Antiemetic drug profiles 19Intestinal obstructi<strong>on</strong> 20Mouth problems 22Anorexia and anorexia/cachexia syndrome 24C<strong>on</strong>stipati<strong>on</strong> 25Diarrhoea 26Fistulae 26Ascites 27Respiratory symptomsBreathlessness 28Cough 31Hiccup 32Neurological problemsRaised intracranial pressure 33Fits 34Spinal cord compressi<strong>on</strong> 351* indicates that this is best managed by specialists
Depressi<strong>on</strong> 36Anxiety 37Insomnia 38Drowsiness 39C<strong>on</strong>fusi<strong>on</strong> 40Restlessness 42Skin problemsItch 43Sweating 44Fungating wounds 45Lymphoedema 46Miscellaneous problemsFatigue/weakness 47Anaemia 48Bleeding/haemorrhage 49Venous thromboembolism 50Hypercalcaemia 51Use of steroids 52Diabetes <strong>management</strong> 53End stage c<strong>on</strong>diti<strong>on</strong>s: End stage heart failure, 54End stage kidney failure, End stage COPD 55Syringe drivers 56The last few days of life 58Psychological, spiritual and social care 60Culture 61Breaking bad news 62DNACPR discussi<strong>on</strong>s 64Advance Care Planning 65Dealing with denial and collusi<strong>on</strong> 66Spiritual care 68BereavementBereavement 70Unresolved/abnormal grief 72Index of drugs, dressings etc 73Acknowledgements 78* indicates that this is best managed by specialists 2
INTRODUCTIONPalliative care:• is the active total care of patients and their families, usually when theirdisease is no l<strong>on</strong>ger resp<strong>on</strong>sive to potentially curative treatment, although itmay be applicable earlier in the illness• provides relief from pain and other symptoms• aims to achieve the best possible quality of life for patients and families• resp<strong>on</strong>ds to physical, psychological, social and spiritual needs• extends as necessary to support in bereavement.This handbook c<strong>on</strong>tains guidance to help GPs, community nurses and hospitalstaff as well as specialist palliative care teams. It aims to provide a checklist forthe <strong>management</strong> of comm<strong>on</strong> problems in palliative care, with some informati<strong>on</strong><strong>on</strong> drug treatment. It is not a comprehensive textbook. Further advice can besought from the specialist staff identified <strong>on</strong> the back cover or from any hospiceor specialist palliative care unit. More detailed drug informati<strong>on</strong> may be found inthe British Nati<strong>on</strong>al Formulary (BNF), or from the Palliative Care Formulary(PCF), see below.Nati<strong>on</strong>al Service Frameworks for heart failure, renal failure and other c<strong>on</strong>diti<strong>on</strong>sare increasingly emphasising the importance of providing good palliative care tothese patient groups as well as to those with cancer. The material in thisHandbook is intended to apply across a range of diagnoses.Cauti<strong>on</strong>ary note: some of the drug usage recommended is outside productlicence, whether by way of indicati<strong>on</strong>, dose, or route of administrati<strong>on</strong>. However,the approaches described are recognised as reas<strong>on</strong>able practice within palliativemedicine in the UK. The rINN names for drugs are used throughout.Abbreviati<strong>on</strong>sRoutes: csci = c<strong>on</strong>tinuous subcutaneous infusi<strong>on</strong> (via a syringe driver).sl = sublingual.sc = subcutaneous injecti<strong>on</strong>.po = by mouth.pr = per rectumTimings: om, nocte = each morning, each night.od, bd = <strong>on</strong>ce, twice daily.tds, qds = three, four times daily.q4h, q6h = every four, six hours.Further reading/drug informati<strong>on</strong>• The Oxford Textbook of Palliative Medicine (4 th ed. Hanks GW et. al.),c<strong>on</strong>siders all aspects of palliative care in greater detail.• The Palliative Care Formulary (3 rd ed. Twycross R, Wilcock A), also <strong>on</strong>lineat www.palliativedrugs.com and www.pallcare.info, gives more detailedadvice <strong>on</strong> the drugs used in palliative care.3* indicates that this is best managed by specialists
GENERAL PRINCIPLES OF SYMPTOM MANAGEMENT• Accurate and full assessment is essential for both diagnosis and treatment.• Be aware of the importance of n<strong>on</strong>-physical factors in symptomatology -emoti<strong>on</strong>al, psychological, social and spiritual problems are often mixedtogether with physical symptoms.• When symptoms are difficult to c<strong>on</strong>trol there may be more than <strong>on</strong>e cause, orthere may be hidden emoti<strong>on</strong>al, psychological, social and spiritual factors.• Use appropriate therapies to maintain the best possible quality of life andindependence, and to allow patient and carers to focus <strong>on</strong> other importantissues.• Be careful that drug side effects do not become worse than the originalproblem.• Sensitive explanati<strong>on</strong> and inclusi<strong>on</strong> of patient and carers in decisi<strong>on</strong> makingare essential parts of symptom <strong>management</strong>.• A multiprofessi<strong>on</strong>al approach is essential, and may be facilitated by the use ofa patient held drug card/shared informati<strong>on</strong> card.• C<strong>on</strong>sider referral for a specialist palliative care opini<strong>on</strong>:- if there is a problem which does not resp<strong>on</strong>d as expected- in complex situati<strong>on</strong>s which may benefit from specialist expertise- for support for the hospital or primary health care team.• C<strong>on</strong>tinually reassess.GUIDANCE FROM NICE ON SPECIALIST <str<strong>on</strong>g>PALLIATIVE</str<strong>on</strong>g> <str<strong>on</strong>g>CARE</str<strong>on</strong>g>The Nati<strong>on</strong>al Institute for Clinical Excellence (NICE) has made the followingstatements in its Supportive and Palliative Care Guidance (2004). The fullGuidance can be seen at www.nice.org.uk.A significant proporti<strong>on</strong> of people with advanced disease experience a range ofcomplex problems that cannot always be dealt with effectively by generalistservices. Hospices and specialist palliative care services have been establishedacross the country over the past four decades to help minimise these problems.Areas of expertise within specialist palliative care to which patients and carersmay need access include:• unresolved symptoms and complex psychosocial issues for patients withadvanced disease• complex end of life issues• complex bereavement issues.Specialist palliative care should be available to those with any diagnosis, not<strong>on</strong>ly those with cancer. Services should as a minimum include specialistpalliative care inpatient facilities and hospital and community teams. <str<strong>on</strong>g>Advice</str<strong>on</strong>g>should be available <strong>on</strong> a twenty-four hour, seven days a week basis.* indicates that this is best managed by specialists 4
PAINDiagnosisAccurate diagnosis of the cause(s) of pain is necessary for a rati<strong>on</strong>al approach totherapy. There are many comp<strong>on</strong>ents to pain and all relevant physical, psychosocialand spiritual factors need to be taken into account. It must not be assumedthat pain has been caused by the primary diagnosis: debility, previous treatmentand unrelated causes must also be c<strong>on</strong>sidered.The analgesic ladder approach (see over) is the basis for prescribing in all typesof pain, but careful choice of appropriate adjuvant drugs will increase the chanceof effective palliati<strong>on</strong>.Causes / Risk Factors1 Physical Nociceptive pain caused by somatic, visceral or b<strong>on</strong>e injury.Neuropathic pain caused by nerve injury.2 N<strong>on</strong>-physical Anger, anxieties, fears, sadness, helplessness.Spiritual, social and family distress.AssessmentObtain the patient’s own descripti<strong>on</strong> and assessment of their pain(s):1 What is the pain like? • site and radiati<strong>on</strong> – a body diagram is helpful• character – list the patient’s descriptors• intensity – use a severity or rating scale• exacerbating and relieving factors• effect <strong>on</strong> functi<strong>on</strong> and sleep.2 What is causing the pain? • the disease, by direct invasi<strong>on</strong>, pressure, etc• the treatment, eg c<strong>on</strong>stipati<strong>on</strong>, mucositis• debility, eg pressure sores, muscle stiffness• unrelated pathologies, eg vascular disease.3 Is it a specific type of pain? • b<strong>on</strong>e – worse <strong>on</strong> movement, weight bearing• nerve – burning or shooting, radiates• liver – hepatomegaly, RUQ tenderness• raised ICP – headache worse lying down• colic – intermittent, cramping.4 Other factors • psychological, social and spiritual distress.All pains have a significant psychological comp<strong>on</strong>ent, and fear, anxiety anddepressi<strong>on</strong> will all lower the pain threshold. Remember also the likelyeffects of life changes associated with terminal disease including loss offinancial security, altered body image and compromised sexual functi<strong>on</strong>.Together with more existential and religious uncertainties, these factors canhave a major impact <strong>on</strong> the way a pers<strong>on</strong> perceives and copes with pain.5* indicates that this is best managed by specialists
ManagementThe World Health Organisati<strong>on</strong> (WHO) ‘analgesic ladder’ emphasises that:• analgesics should be given regularly• it is essential to use an analgesic appropriate to the severity of the pain• a patient whose pain does not resp<strong>on</strong>d to weak opioids needs a trial of<strong>management</strong> with str<strong>on</strong>g opioids• all patients taking opioids should also be prescribed laxatives• the oral route is preferred for all steps of the ladder• additi<strong>on</strong>al methods of pain c<strong>on</strong>trol must be c<strong>on</strong>sidered in all patients.Step 1Mild painN<strong>on</strong>-opioidStep 2Moderate painWeak opioid+/- n<strong>on</strong>-opioidStep 3Severe painStr<strong>on</strong>g opioid+/- n<strong>on</strong>-opioidCo-analgesiaAdjuvant drugs - see pp 13 - 14Nerve blocks, TENS, relaxati<strong>on</strong>, acupunctureSpecific therapiesRadiotherapy, chemotherapy, surgeryAddress psychological problemsStep 1 N<strong>on</strong> opioidsParacetamol: Oral, rectal or iv (500mg - 1g qds, maximum 4g per day).NSAIDs: Useful for pain aggravated by movement or inflammati<strong>on</strong>,risk/benefit balance must always be c<strong>on</strong>sidered,gastric protecti<strong>on</strong> is str<strong>on</strong>gly advised eg PPIs, misoprostol,renal impairment is not uncomm<strong>on</strong>,relatively c<strong>on</strong>tra-indicated in heart failure,choice of NSAID is largely dictated by local preference:• ibuprofen (200 - 400mg tds or qds)• diclofenac (tabs SR 75mg bd, supps 100 - 150mg daily)• naproxen (tabs 500mg bd).Step 2 Weak opioidsCodeine 30mg with paracetamol 500mg (co-codamol 30/500), 1 - 2 qds.Tramadol 50 - 100mg qds or tramadol MR 100 - 200mg bd.Other weak opioids, including dihydrocodeine, offer no advantages.Step 3 Str<strong>on</strong>g opioids (see following pages).* indicates that this is best managed by specialists 6
USE OF STRONG OPIOIDSMorphine remains the first-line str<strong>on</strong>g opioid of choice.1 To gain c<strong>on</strong>trol of the pain:A Usually start with immediate release morphine (liquid or tablets), every4 hours, 2.5 - 10mg, with prn doses equal to the 4-hourly dose. (Theeventual effective dose will rarely be more than 30mg 4 hourly).B If using modified release morphine, give 10 - 30mg bd, depending <strong>on</strong>previous weak opioid, with prn doses of immediate release morphine eachup to 1/6th of the total daily dose. Note that pain c<strong>on</strong>trol may take l<strong>on</strong>gerto achieve.Elderly patients and those with renal or hepatic impairment (see p12) arelikely to need lower or less frequent doses2 Reassess pain c<strong>on</strong>trol at least daily, recording severity if helpful:Titrate the dose to achieve pain relief, increasing the dose by 30 - 50% every2 - 3 days, or so<strong>on</strong>er if needed. A typical dose sequence is:5 - 10 - 15 - 20 - 30 - 40 - 60 - 90 - 120 - 150 - 200mg.3 Once pain is c<strong>on</strong>trolled, the 4-hourly regime is usually changed to modifiedrelease morphine: the 12-hourly dose will be three times the 4-hourly dose.4 The prn dose for breakthrough pain will be up to the same as the 4-hourlydose ie 1/6th of the daily dose. Wait for 30 minutes after breakthroughmedicati<strong>on</strong> to assess resp<strong>on</strong>se. If pain c<strong>on</strong>tinues, further breakthroughmedicati<strong>on</strong> may be allowed but the pain will require reassessment.5 Review doses regularly: if using two or more breakthrough doses per day(with benefit), c<strong>on</strong>sider increasing the regular dose as suggested in 2 above.6 C<strong>on</strong>tinuing pain, particularly with persisting side effects eg drowsiness,nausea or c<strong>on</strong>fusi<strong>on</strong>, may indicate that this pain is not fully opioid resp<strong>on</strong>sive– other approaches may be more appropriate, rather than increasing the opioiddose (see pp13 - 16). If side effects occur but pain is well c<strong>on</strong>trolled, reducedose.7 To avoid c<strong>on</strong>fusi<strong>on</strong> between preparati<strong>on</strong>s with names that seem similar topatients, and to ensure c<strong>on</strong>sistent bioavailability, we recommend that bothimmediate release and slow release preparati<strong>on</strong>s, as well as transdermalanalgesics, are prescribed by their brand name.Instructi<strong>on</strong>s to the patient and carer1 Emphasise the need for regular administrati<strong>on</strong>.2 Explain about breakthrough medicati<strong>on</strong>.3 Warn about possible side effects.4 Reassure that when used for pain relief, morphine is not addictive and that itsuse does not prejudice future pain relief.7* indicates that this is best managed by specialists
Unwanted effects of str<strong>on</strong>g opioids1 C<strong>on</strong>stipati<strong>on</strong> is virtually inevitable – use prophylactic laxatives (see p25).2 Nausea is fairly comm<strong>on</strong> when initiating opioids, particularly with higherdoses or rapid dose escalati<strong>on</strong>. Slow titrati<strong>on</strong> usually avoids this. If antiemeticneeded – metoclopramide 10mg tds, cyclizine 50mg tds or haloperidol 1.5mgnocte.3 Drowsiness implies too high a dose; if persistent, reduce dose and/or c<strong>on</strong>siderother opti<strong>on</strong>s.4 Hallucinati<strong>on</strong>s also imply too high a dose, often preceded by vivid dreams.5 Other troublesome symptoms include dry mouth, hiccups, sweating.6 Respiratory depressi<strong>on</strong> is very rarely seen if opioids titrated sensibly.Signs of excess opioid/opioid toxicity (seek advice):• increasing drowsiness• vivid dreams/hallucinati<strong>on</strong>s• pinpoint pupils• muscle twitching/myocl<strong>on</strong>us/jerking*• hyperalgesia <strong>on</strong> light touch.*These problems may occur with any opioid, especially morphine, when there issignificant renal or hepatic impairment (see p12), dehydrati<strong>on</strong> or infecti<strong>on</strong>.Nalox<strong>on</strong>e should <strong>on</strong>ly be c<strong>on</strong>sidered (in small aliquots up to 100mcg) ifsignificant respiratory depressi<strong>on</strong>, because pain c<strong>on</strong>trol will be dramaticallyreversed.Changing from <strong>on</strong>e str<strong>on</strong>g opioid to anotherWhen oral administrati<strong>on</strong> is not possible because of dysphagia, vomiting orweakness, c<strong>on</strong>sider changing to a transdermal patch (see p11) or to csci using asyringe driver (see pp10, 25).Other reas<strong>on</strong>s for changing str<strong>on</strong>g opioids can be: reducti<strong>on</strong> in side effects egc<strong>on</strong>stipati<strong>on</strong> (fentanyl, buprenorphine less c<strong>on</strong>stipating), problems with oralcompliance etc.If there is difficulty achieving good pain c<strong>on</strong>trol without unacceptable sideeffects, changing the str<strong>on</strong>g opioid may be appropriate. However, most problemscan be solved by improving the titrati<strong>on</strong>, or using adjuvant drugs.The dose c<strong>on</strong>versi<strong>on</strong> (total daily or prn dose) from oral morphine to sc morphineis normally 2:1, and from oral morphine to sc diamorphine 3:1 (see p10), butallow flexibility depending <strong>on</strong> the need for increased or decreased analgesia.Seek specialist advice when:• c<strong>on</strong>verting from higher doses of <strong>on</strong>e opioid to another, because c<strong>on</strong>versi<strong>on</strong>ratios may be different at higher doses*• pain persists but there is opioid toxicity*• c<strong>on</strong>verting to or from methad<strong>on</strong>e.** indicates that this is best managed by specialists 8
Morphine preparati<strong>on</strong>sImmediate release oral morphine:• Oramorph liquid 10mg/5ml, oramorph c<strong>on</strong>centrated soluti<strong>on</strong> 100mg/5ml.• Sevredol tablets 10mg, 20mg, 50mg.Modified release oral morphine:• Zomorph capsules† 10mg, 30mg, 60mg, 100mg, 200mg (12 hourly).• MST C<strong>on</strong>tinus tablets 5mg, 10mg, 15mg, 30mg, 60mg, 100mg, 200mg(12 hourly).• MST C<strong>on</strong>tinus suspensi<strong>on</strong> 20mg, 30mg, 60mg, 100mg, 200mg (12 hourly).C<strong>on</strong>tents of sachets to be mixed with water. Expensive.• Morphgesic SR tablets 10mg, 30mg, 60mg, 100mg (12 hourly).• MXL capsules† 30mg, 60mg, 90mg, 120mg, 150mg, 200mg (daily).Morphine sulphate injecti<strong>on</strong> 10mg, 15mg, 20mg, 30mg per 1ml ampoule.Morphine can be used in syringe drivers, as cheaper than diamorphine, butvolume limitati<strong>on</strong>s at higher dose.Morphine suppositories 10mg, 15mg, 20mg, 30mg.Other oral and injectable str<strong>on</strong>g opioidsSee overleaf for the Table of Opioid Equivalents.Diamorphine has been the str<strong>on</strong>g opioid of choice for parenteral use at higherdoses because of its greater solubility than morphine, but is more expensive.Subcutaneous diamorphine is up to 3 times more potent than oral morphine.Maximum recommended c<strong>on</strong>centrati<strong>on</strong> is 250mg/ml.a) Ampoules 5mg, 10mg, 30mg, 100mg, 500mg. Dissolve in water for injecti<strong>on</strong>.Oxycod<strong>on</strong>e is available for oral and injectable use, as an alternative to morphine,with slightly different side effect profile.a) OxyNorm liquid 5mg/5ml, 50mg/5ml (immediate release, 4 hourly).b) OxyNorm capsules 5mg, 10mg, 20mg (immediate release, 4 hourly).c) OxyC<strong>on</strong>tin tablets 5mg, 10mg, 20mg, 40mg, 80mg (12 hourly).d) OxyNorm injecti<strong>on</strong>, 10mg/ml, 50mg/ml.Hydromorph<strong>on</strong>e is also available for oral use, as an alternative to morphine,with slightly different side effect profile. It may be safer in mild to moderaterenal failure.a) Pallad<strong>on</strong>e capsules† 1.3mg, 2.6mg (4hourly).b) Pallad<strong>on</strong>e SR capsules† 2mg, 4mg, 8mg, 16mg, 24mg (12hourly).Methad<strong>on</strong>e* may be useful in patients with pain, particularly neuropathic,poorly resp<strong>on</strong>sive to morphine or with unacceptable side effects. However, it hasa variable metabolism and dangerous accumulati<strong>on</strong> can occur. Steady statepotency of oral methad<strong>on</strong>e to morphine ranges from 3:1 to 10:1. Dose titrati<strong>on</strong>involves a prn regime over 5 - 8 days before switching to a 12hourly regime. Itsuse is best restricted to those with extensive experience.† indicates that capsule can be opened and c<strong>on</strong>tents sprinkled <strong>on</strong> food or drink9* indicates that this is best managed by specialists
Fentanyl is most comm<strong>on</strong>ly used as a transdermal patch (see p11) or in shortacting buccal, sublingual or intranasal formulati<strong>on</strong>s for pains of short durati<strong>on</strong>(see pp15/16) but, like alfentanil, can be used sc and via syringe driverparticularly for pain in patients with severe renal failure (see p55). Csci dose issimilar to patch eg 600mcg/24h = 25mcg/h patch, at higher doses alfentanil ispreferred because of volume. Fentanyl injecti<strong>on</strong> 50mcg/ml.Alfentanil* has a rapid <strong>on</strong>set but short durati<strong>on</strong> of acti<strong>on</strong>. It may be useful fortreatment of procedure pain such as dressing changes either by subcutaneousinjecti<strong>on</strong> or as a buccal spray (see pp15/16). It can be given by syringe driverparticularly in patients with renal failure who exhibit toxicity reacti<strong>on</strong>s with otheropioids. It is approximately ten times more potent than sc diamorphine.Alfentanil injecti<strong>on</strong> 500mcg/ml, 2ml amp.We do not recommend pethidine for regular use in chr<strong>on</strong>ic cancer pain. Forc<strong>on</strong>versi<strong>on</strong> from pethidine to morphine seek specialist advice.*Table of relative potencies of oral and subcutaneous opioid analgesicsThis table provides <strong>on</strong>ly an approximate guide to opioid equivalents, becausecomprehensive data are lacking. Doses always need to be re-titrated after achange of opioid. Breakthrough dose is normally up to 1/6th total daily dose.Drug and route ofadministrati<strong>on</strong>Dose ratioto oralmorphineApproximate dose equivalents(examples) in mgOral codeine 10 - 12 300 - 360 - -Oral tramadol 7 - 10 200 - 300 - -Oral morphine 1 30 90 240Subcutaneous morphine 1 / 2 15 45 120Subcutaneous diamorphine 1 / 3 10 30 80Oral oxycod<strong>on</strong>e† 1 / 2 15 45 120Subcutaneous oxycod<strong>on</strong>e† 1 / 3 10 30 80Oral hydromorph<strong>on</strong>e 1 / 7.5 4 12 32Subcutaneous hydromorph<strong>on</strong>e 1 / 15 2 6 16Subcutaneous alfentanil 1 / 30 1 3 8† oxycod<strong>on</strong>e oral:sc is not the manufacturers 2:1 because oral ratio to morphineis more correctly 2:3. However, sc oxycod<strong>on</strong>e: sc diamorphine is 1:1.* indicates that this is best managed by specialists 10
Str<strong>on</strong>g opioids available for transdermal use (patches)Patches can be useful especially when there is vomiting or other problems withthe oral route, intractable c<strong>on</strong>stipati<strong>on</strong> despite laxatives, or other side effects are aproblem with opioid resp<strong>on</strong>sive pain. They are unsuitable for acute or variablepain, and for the opioid naïve (with the possible excepti<strong>on</strong> of BuTrans).Note that:• patients c<strong>on</strong>verting from 12hrly modified release morphine should apply thefirst patch at the same time as taking the final 12hrly dose• patients c<strong>on</strong>verting from 4hrly immediate release morphine must c<strong>on</strong>tinueregular morphine for the first 12 hours• oral immediate release or sc opioid should always be prescribed forbreakthrough pain (see table below)• laxatives should be reduced by up to 50% and then titrated to need• reassessment of pain c<strong>on</strong>trol should take place at a minimum of 36 andpreferably 72hrs. Any upward titrati<strong>on</strong> in dose should be in steps of no morethan 25-50%.• there is a possibility of withdrawal symptoms when c<strong>on</strong>verting frommorphine, which resp<strong>on</strong>d to small doses of immediate release oral morphine• see p58 for advice <strong>on</strong> the use of patches at the end of life.FentanylThere are now a number of different brands of fentanyl patches – use matrixrather than reservoir.a) Patches 12, 25, 50, 75 and 100mcg/hr (every 72 hours).BuprenorphineCurrent patches are either low dose BuTrans (weekly) or higher dose Transtec(twice weekly). Dose increments are smaller and safer than with fentanylpatches. Any partial ag<strong>on</strong>ist effect is not <strong>clinical</strong>ly apparent.a) Transtec patch 35, 52.5, 70mcg/hr (twice weekly)b) BuTrans patch 5, 10, 20mcg/hr (every 7 days).Buprenorphine is also available as sl tablet and injecti<strong>on</strong> (neither recommended).Table of approximate equivalents of patches and prn opioid dosesOral morphine (total mg/24 hrs) 30 60 120 180 240Transdermal fentanyl (microgram/hr) 12 25 37 50 75Transdermal buprenorphine (microgram/hr) 20 - 35 35 70 105 140Oral morphine for breakthrough (mg) 5 10 20 30 40sc diamorphine for breakthrough (mg) 2.5 2.5 - 5 5 - 7.5 10 15sc morphine for breakthrough (mg) 2.5 5 10 15 2011* indicates that this is best managed by specialists
Opioids and renal or hepatic impairmentMetabolites of morphine and some other opioids accumulate in renal impairment(of which eGFR is a better indicator than serum creatinine in patients with loss ofmuscle bulk), leading to opioid toxicity manifested as:• increasing drowsiness or c<strong>on</strong>fusi<strong>on</strong>• vivid dreams/hallucinati<strong>on</strong>s• muscle twitching/myocl<strong>on</strong>us/jerking*• hyperalgesia <strong>on</strong> light touch or <strong>on</strong> being turned.*This is an important cause of ‘terminal agitati<strong>on</strong>’. It may resp<strong>on</strong>d to a reducti<strong>on</strong>in the dose and/or frequency of administrati<strong>on</strong>, but it is often better to switch toan opioid which does not accumulate in renal impairment such as fentanyl,buprenorphine or alfentanil (see p55).Opioid toxicity may also occur in hepatic impairment, but <strong>clinical</strong> difficulties d<strong>on</strong>ot usually arise unless the impairment is severe: prothrombin time (or INR) is amore sensitive indicator of severe impairment than standard liver functi<strong>on</strong> tests.All opioids can precipitate c<strong>on</strong>fusi<strong>on</strong> and encephalopathy, but oral opioids willbe particularly affected by the loss of first pass metabolism. Careful re-titrati<strong>on</strong> isnecessary using both a reducti<strong>on</strong> in the dose and a lengthening of dose interval,while c<strong>on</strong>sidering an alternative opioid. In the dying patient, maintenance ofgood analgesia remains very important.Opioid Renal impairment Hepatic impairmentModerate Severe* Moderate Severe*morphine Reduce dose Avoid Normal dose Reduce dosediamorphine Reduce dose Avoid Normal dose Reduce dosefentanyl Normal dose Normal dose Normal dose Reduce dosehydromorph<strong>on</strong>e Reduce dose Reduce dose Normal dose Reduce doseoxycod<strong>on</strong>e Reduce dose Avoid Normal dose Reduce dosemethad<strong>on</strong>e Normal dose Normal dose Normal dose Reduce dosealfentanil Normal dose Normal dose Normal dose Reduce dosebuprenorphine Normal dose Normal dose Normal dose Reduce dose*Always seek specialist advice in cases of severe renal or hepatic impairment.* indicates that this is best managed by specialists 12
Opioids and drivingDoctors have a legal resp<strong>on</strong>sibility to advise patients if a disability is likely tomake them a danger when driving. Taking morphine for medicinal reas<strong>on</strong>s doesnot automatically disqualify from driving, but the following advice should begiven:• Do not drive for at least two days, and preferably five, after starting orincreasing morphine• Check fitness to drive by taking a trusted passenger and driving for 10 - 15minutes <strong>on</strong> quiet roads• Inform the insurance company. If this is not d<strong>on</strong>e the patient may find they arenot covered, irrespective of fault. It is illegal to drive uninsured.ADJUVANT TREATMENTS FOR SPECIFIC PAINSA B<strong>on</strong>e pain1 C<strong>on</strong>sider early referral for palliative radiotherapy - usually a single fracti<strong>on</strong> iseffective. Radioactive isotope treatment may be used for multiple scleroticmetastases.2 NSAIDs may be effective but beware side effects: disc<strong>on</strong>tinue if not helping.Gastro-protective agents should usually be prescribed.3 IV infusi<strong>on</strong>s of bisphosph<strong>on</strong>ates may reduce pain in patients with b<strong>on</strong>emetastases, especially from breast and prostate cancer and myeloma: drugsand doses as per hypercalcaemia (see p51).4 C<strong>on</strong>sider referral to an orthopaedic surge<strong>on</strong> for internal fixati<strong>on</strong> for metastasesin l<strong>on</strong>g b<strong>on</strong>es at risk of fracture.5 Vertebroplasty or cement fixati<strong>on</strong> may be appropriate for isolated vertebralcollapse in selected patients.B Abdominal painExclude/diagnose oesophago-gastritis, peptic ulcer, perforati<strong>on</strong>, urinary tractinfecti<strong>on</strong> or ureteric obstructi<strong>on</strong>.1 C<strong>on</strong>stipati<strong>on</strong> is a comm<strong>on</strong> cause; for treatment see p25.2 For colic (bowel or ureteric) use an anticholinergic. Hyoscine butylbromide ismore effective by sc injecti<strong>on</strong> 20mg or csci 40 - 120 (-240*)mg/24hrs. Otheroral agents include mebeverine, alverine and propantheline.3 For liver capsule pain c<strong>on</strong>sider dexamethas<strong>on</strong>e 4 - 8mg/per day (see p52)and/or NSAIDs.4 For pancreatic pain c<strong>on</strong>sider coeliac plexus block (see p15).5 For pain arising from retroperit<strong>on</strong>eal lymph nodes c<strong>on</strong>sider dexamethas<strong>on</strong>e4 - 8mg/per day (see p52), gabapentin or other neuropathic analgesics (seep14) or nerve blocks (see p15)6 For bladder spasm c<strong>on</strong>sider oxybutynin 2.5 - 5mg bd-qds or tolterodine 2mgbd, amitriptyline 10 - 50mg nocte, or NSAIDs. If catheterized and noresp<strong>on</strong>se to the above, intravesical bupivacaine 0.25%, 20mls for 15 mins tds.13* indicates that this is best managed by specialists
C Rectal painExclude c<strong>on</strong>stipati<strong>on</strong> by abdominal and rectal examinati<strong>on</strong>. Tenesmus and deepseated pelvic pains may resp<strong>on</strong>d to:1 Local steroid (Colifoam, Predsol etc) or systemic steroids, NSAIDs,amitriptyline or gabapentin (see below).2 Drugs for relief of muscle spasm:• nifedipine immediate release capsules 10 - 20mg orally or sl after opening• glyceryl trinitrate ointment 0.1 - 0.2% bd• benzodiazepines, eg diazepam 2 - 10mg nocte3 Local radiotherapy for tumour especially if steroid treatment is successful.4 Nerve blocks (see p15).D Muscle pain1 Physiotherapy, aromatherapy, relaxati<strong>on</strong>, heat pad.2 Muscle relaxants: diazepam, baclofen, cl<strong>on</strong>azepam, dantrolene, tizanidine.E Neuropathic painOften aching in nature, sometimes burning or shooting, and may be worse aftermovement or at night. May not resp<strong>on</strong>d in a predictable way to pain-relievingmedicati<strong>on</strong>. May presage cord compressi<strong>on</strong>. Usually due to compressi<strong>on</strong> ordamage of the spinal cord, nerve roots, nerve plexi or peripheral nerves;occasi<strong>on</strong>ally originates in the thalamus or cortex.Specialist palliative care team or chr<strong>on</strong>ic pain team will be happy to advise andreferral is suggested at an early stage.The following treatments may be effective:1 Dexamethas<strong>on</strong>e 4 - 8mg daily (see p52) for short term relief of pressure.2 Try opioid titrati<strong>on</strong>, but be aware that this sort of pain is often not very opioidsensitive and opioid toxicity is a risk whichever opioid is tried.3 Tricyclic antidepressants eg amitriptyline 10 - 75mg or dosulepin 25 - 75mgnocte. Venlafaxine* and mirtazapine have also been used. SSRIs do notappear to be of benefit.4 Gabapentin titrating from 300mg/day (100mg/day in elderly) in divided dosesup to maximum 2700mg/day, or pregabalin initially 75mg bd max 300mg bd.5 Other antiepileptics can be tried: sodium valproate 400 - 800mg/day,carbamazepine 200 - 1200mg/day.6 Cl<strong>on</strong>azepam starting at 500mcg nocte or diazepam 2 - 10mg/day sometimeshelp.7 Other drugs used by specialists include baclofen*, cl<strong>on</strong>idine*, ketamine* andmethad<strong>on</strong>e*.8 Other approaches include TENS, acupuncture and nerve blocks (see nextpage).* indicates that this is best managed by specialists 14
Pains amenable to nerve blocksMany pains are amenable to interventi<strong>on</strong> by a pain <strong>management</strong> specialistanaesthetist. Neural blockade can be temporary with local anaesthetic or semipermanentwith neurolytic agents such as phenol. Injected steroids areparticularly useful when pain is due to compressi<strong>on</strong> of the nerve.1 Back pain due to metastases often resp<strong>on</strong>ds to epidural injecti<strong>on</strong> of high dosesteroid and local anaesthetic. Caudal injecti<strong>on</strong>s are easily performed and areuseful for sacral pain. Thoracic and cervical epidurals are more difficult.2 Pancoast tumour or other brachial plexopathy : brachial plexus block.3 Rib pain may be temporarily abolished by intercostal injecti<strong>on</strong> of localanaesthetic proximal to the lesi<strong>on</strong>. L<strong>on</strong>ger term benefit may result frominfiltrati<strong>on</strong> with depot steroid. If helpful, permanent block may be obtainedwith cryoprobe.4 Chest wall pain can be very difficult to c<strong>on</strong>trol, especially when it occurs as aresult of mesothelioma. Intercostal and paravertebral blocks can be effective,but if ineffective, early referral for percutaneous cervical cordotomy(Portsmouth or Exeter) is recommended. Some specialists perform thoracicepidurals or even intrapleural infusi<strong>on</strong>s.5 Upper abdominal pain, especially due to pancreatic tumour, resp<strong>on</strong>ds tocoeliac plexus block in around 80%. This can be performed under directvisi<strong>on</strong> at laparotomy, or under CT c<strong>on</strong>trol.6 Lower abdominal and pelvic pain : lumbar plexus block can give worthwhilebenefit but with a lower success rate.7 Perineal pain : saddle anaesthesia using intrathecal phenol (as with allneurolytic techniques this is the province of the specialist).8 Hip pain may be helped by a variety of procedures, including direct injecti<strong>on</strong>of local anaesthetic and steroid into the joint, psoas compartment block, andblock of the obturator nerve together with the nerve to quadratus femoris.9 Intrathecal or epidural opioid and local anaesthetic infusi<strong>on</strong>s may help indifficult pains.Acute pain of short durati<strong>on</strong> and Breakthrough painThere are some pains which are often of quite short durati<strong>on</strong>, either predictablefrom specific incidents eg moving a fractured limb or changing a painfuldressing, or unpredictable.Breakthrough pain is usually defined as transient flare up of pain from generallyc<strong>on</strong>trolled background pain.The principles for <strong>management</strong> are the same as for any other pain ie correctdiagnosis, remove causes where possible, and assess whether opioid sensitive,and whether NSAID more appropriate.• Treatment opti<strong>on</strong>s are, usually, shorter acting immediate release preparati<strong>on</strong>s• The dose required is not necessarily predictable from background dosage andrequires individual titrati<strong>on</strong>• When the incident is predictable give 20 - 30mins beforehand15* indicates that this is best managed by specialists
Drug opti<strong>on</strong>s:1 Morphine, immediate release oral or sc; diamorphine or oxycod<strong>on</strong>e sc.(Effect may last a lot l<strong>on</strong>ger than durati<strong>on</strong> of the pain episode).2 Fentanyl preparati<strong>on</strong>s: short acting buccal, sublingual or intranasal.(Quicker acting and usually lasting 1 - 2 hours)3 Alfentanil* by sc injecti<strong>on</strong> or buccal spray (special order) 250 - 500mcg ifopioid naïve.4 Nitrous oxide (as Ent<strong>on</strong>ox), not for regular use as it is addictive.NON-PHARMACOLOGICAL APPROACHES TO PAIN CONTROLA Emoti<strong>on</strong>al and spiritual support (see also pp62, 68)1 Within a careful assessment of the pain:• assess what the pain means for the patient• assess their general emoti<strong>on</strong>al, psychological and spiritual state• assess their current coping style – is it helpful, is this their usual approachor has it changed with the disease/pain?• assess impact <strong>on</strong> family/carers2 Identify and communicate (to patient & family, health professi<strong>on</strong>als):• causes of pain and <strong>management</strong> plan• the correct use/expectati<strong>on</strong>s of medicati<strong>on</strong>s and other treatments• understanding of the patient’s pers<strong>on</strong>al situati<strong>on</strong>• practical and emoti<strong>on</strong>al support availableB Help to develop coping strategiesCoping strategies developed for chr<strong>on</strong>ic pain may be useful within the palliativecare setting. They are based <strong>on</strong> living with pain, adapting living to the newrequirements and the maintenance of normal activity as far as possible. Manychr<strong>on</strong>ic pain clinics have <strong>clinical</strong> psychologists who specialise in this field.C Relaxati<strong>on</strong> and distracti<strong>on</strong> techniques and creative/complementarytherapiesThere are a number of techniques and therapies, provided by a wide range ofprofessi<strong>on</strong>als, which aim to encourage relaxati<strong>on</strong>, finding distracti<strong>on</strong> and otherinterests. Most patients will find at least some of these approaches will help.D Transcutaneous electrical nerve stimulator (TENS) or Acupuncture* indicates that this is best managed by specialists 16
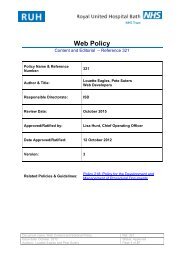
NAUSEA AND VOMITINGMechanismsRaised intra-cranialpressure,Cerebellar diseasePain, unpleasantsights, smell,anxiety, fearCerebral cortexMoti<strong>on</strong>; positi<strong>on</strong>Vestibular nuclei(H 1 & ACh M )Vomiting Centre(5HT 2 , ACh M / H 1 )Endogenous toxinsor drugs eg opioids,cytotoxics.Hypercalcaemia,uraemia, liverfailure, ket<strong>on</strong>es,carcinomatosis,radiotherapy.BloodCSFChemoreceptortrigger z<strong>on</strong>e(D 2 )(5HT 3 )(NK1)Gastric irritati<strong>on</strong>,gastric stasis,gastroenteritis.Intestinal obstructi<strong>on</strong>.C<strong>on</strong>stipati<strong>on</strong>.Pharyngeal /oesophageal stimuli.(D 2 , ACH M , 5HT 3 )Release ofemetogenicagentsVagal &sympatheticafferents(5HT 3 , 5HT 4 )17* indicates that this is best managed by specialists
Causes / Risk factorsThere are many causes of nausea and vomiting and often more than <strong>on</strong>e cause ispresent. Mechanisms are outlined <strong>on</strong> the previous page. See next page forprofiles of antiemetics.Management1. Treat cause if possible eg stopping/changing/reducing drugs.2. N<strong>on</strong>-drug measures include relaxati<strong>on</strong> and psychotherapeutic techniques,acupuncture, ginger and Seabands.3. In established nausea and vomiting may need to use antiemetics via n<strong>on</strong>-oralroutes for initial c<strong>on</strong>trol eg csci via syringe driver.4. Drug therapy (see next page for drug profiles):CauseDrug therapyRaised intracranial pressure, Dexamethas<strong>on</strong>e (see p52)& cerebellar disease Cyclizine or levomepromazineAnxiety Levomepromazine, benzodiazepines (see p37)Moti<strong>on</strong>, positi<strong>on</strong>alCyclizineHyoscine hydrobromideDrugs, endogenous toxins MetoclopramideHaloperidol, prochlorperazineLevomepromazineChemotherapy, andC<strong>on</strong>sult <strong>on</strong>cology colleaguesradiotherapyEarly: 5HT 3 antag<strong>on</strong>ists or prokineticsDelayed: dexamethas<strong>on</strong>e, levomepromazineGastric stasisMetoclopramide, domperid<strong>on</strong>eErythromycin*Gastric irritati<strong>on</strong>Review medicati<strong>on</strong>AntacidsProt<strong>on</strong> pump inhibitorsMisoprostol 400mcg bd if caused by NSAIDsIntestinal stasisMetoclopramide 40 - 80mg dailyIntestinal obstructi<strong>on</strong>See separate secti<strong>on</strong> p20C<strong>on</strong>stipati<strong>on</strong>See separate secti<strong>on</strong> p25IndeterminateMetoclopramideLevomepromazine or CyclizineDexamethas<strong>on</strong>e 4 - 8mg omTrial of others* indicates that this is best managed by specialists 18
Antiemetic drug profiles (see also p57):Cyclizine• H 1 antihistamine with anticholinergic acti<strong>on</strong>• 50mg tds orally or by sc injecti<strong>on</strong>• 100 - 150mg over 24 hours by csci (skin irritati<strong>on</strong>)Dexamethas<strong>on</strong>eDomperid<strong>on</strong>eHaloperidol †19• reduces intracerebral swelling, other modes ofacti<strong>on</strong> uncertain• may help emesis of indeterminate cause• 4 - 8mg od for 5 day trial• dopamine D 2 antag<strong>on</strong>ist and prokinetic• unlikely to cause sedati<strong>on</strong> / extrapyramidal effects• 10 - 20mg tds - qds orally• 30 - 60mg suppositories bd rectally• pure dopamine D 2 antag<strong>on</strong>ist, not prokinetic• often used for opioid induced nausea• may cause extrapyramidal effects• 1.5 - 5mg nocte, oral or sc• 2.5 - 5mg over 24 hours by csciHyoscine hydrobromide • antimuscarinic anticholinergic (AChM)• 0.3 - 0.6mg up to qds sl (Kwells) or sc• 0.8 - 2.4mg over 24 hours by csci (sedating)• 1mg every 72 hours by transdermal patchLevomepromazine † • activity at multiple sites (5HT 2 , D 2 , ACh M /H 1 )• can cause hypotensi<strong>on</strong> in susceptible patients• antiemetic at modest doses 5 - 25mg daily, uselowest effective dose unless sedati<strong>on</strong> required,usually given as single oral dose nocte or by csciMetoclopramide † • dopamine D 2 antag<strong>on</strong>ist and prokinetic• 10 - 20mg tds - qds oral or sc; can be by csci• 5HT 4 ag<strong>on</strong>ist (bowel prokinetic) (40 - 80mg daily)• 5HT 3 antag<strong>on</strong>ist at high doses (>100mg daily)Prochlorperazine † • predominantly D 2 antag<strong>on</strong>ist, weak anti-ACh M /H 1• 5 - 10mg tds orally or 3 - 6mg bd as buccal tablets• 12.5mg tds by deep im injecti<strong>on</strong> - do not give sc5HT3 antag<strong>on</strong>ists• <strong>on</strong>dansetr<strong>on</strong> and others (see Secti<strong>on</strong> 4.6 of BNF)• used to c<strong>on</strong>trol early emesis after chemotherapyand abdominal radiotherapy• avoid prol<strong>on</strong>ged use, cause c<strong>on</strong>stipati<strong>on</strong>Neurokinin1 antag<strong>on</strong>ists* • used as an adjunct with emetogenic chemotherapy† avoid in Parkins<strong>on</strong>ism and dyst<strong>on</strong>ia* indicates that this is best managed by specialists
INTESTINAL OBSTRUCTIONIntestinal obstructi<strong>on</strong> in associati<strong>on</strong> with advanced cancer is often complex anddifficult to c<strong>on</strong>trol. Early discussi<strong>on</strong> with specialist palliative care team isrecommended. Has both mechanical (intestinal narrowing) and functi<strong>on</strong>al (poormotility) elements.Diagnosis1 Range of symptoms depends <strong>on</strong> level of blockage, but these include:• vomiting often with little preceding nausea• c<strong>on</strong>stipati<strong>on</strong>, although some flatus and/or stool may still be passed• abdominal distensi<strong>on</strong> and generalised discomfort• colic may or may not be a feature• bowel sounds may be hyperactive or scanty.2 Examine previous operati<strong>on</strong> notes; abdominal x-ray may be helpful.3 Exclude simple c<strong>on</strong>stipati<strong>on</strong> by rectal and abdominal examinati<strong>on</strong>.Causes / Risk factors1 Most comm<strong>on</strong> with primary tumours of ovary and col<strong>on</strong>, but may occur withalmost any primary site, including breast and lung.2 Tumour mass within lumen.3 Tumour <strong>on</strong> perit<strong>on</strong>eal surface causing oedema or adhesi<strong>on</strong>s.4 Infiltrati<strong>on</strong> within muscle coats preventing normal peristalsis.5 Damage to aut<strong>on</strong>omic nerve plexuses by tumour infiltrati<strong>on</strong> of mesentery.6 Pancreatic carcinoma may cause gastric stasis by unknown mechanism.7 Adhesi<strong>on</strong>s, radiati<strong>on</strong> fibrosis, metabolic disturbance, c<strong>on</strong>stipati<strong>on</strong>, sepsis.ManagementThis will depend <strong>on</strong> the site of obstructi<strong>on</strong>; whether complete or incomplete;bowel motility; and the patient’s wishes and general c<strong>on</strong>diti<strong>on</strong>.1 C<strong>on</strong>sider surgery or stenting if there are <strong>clinical</strong> features to suggest a singlesite of obstructi<strong>on</strong>, especially where colic is a prominent symptom, or wheredistensi<strong>on</strong> is such as to require venting.2 If inoperable, aim to c<strong>on</strong>trol symptoms without the need for c<strong>on</strong>tinuous ‘dripand suck’ but:a) nasogastric intubati<strong>on</strong> or percutaneous venting gastrostomy may bepreferred by patients with gastroduodenal obstructi<strong>on</strong> where drug treatmenthas been unsuccessful;b) hydrati<strong>on</strong> with 1+ litre per day iv or sc may relieve thirst (not dry mouth),but may increase vomit volume.3 Treat dry mouth (see p23).4 Treat symptomatic gastro-oesophageal reflux.* indicates that this is best managed by specialists 20
5 Drug therapy:C<strong>on</strong>stant abdominal pain• Str<strong>on</strong>g opioids, eg morphine, diamorphine by csci.Colic• Avoid/stop stimulant and bulking laxatives.• Avoid prokinetic antiemetics (metoclopramide, domperid<strong>on</strong>e).• Hyoscine butylbromide 40 - 120 (- 240*)mg daily by csci.• Mebeverine, alverine po may help if <strong>on</strong>ly intermittent partial obstructi<strong>on</strong>.Nausea and vomitingAim to abolish nausea and to reduce vomiting to a minimum.• Cyclizine - see p19• Levomepromazine - see p19• Haloperidol - see p19• Metoclopramide (see p19) may help where there is gastric stasis or ileus but isc<strong>on</strong>tra-indicated in the presence of colic; the resp<strong>on</strong>se is unpredictable if therehas been a gastro-jejunostomy• Anti-secretory agentsa) If high (gastroduodenal) obstructi<strong>on</strong>:• hyoscine butylbromide 40 - 120 (- 240*)mg daily by csci reducessecreti<strong>on</strong>s• H 2 blocker (ranitidine) may reduce volume of gastric secreti<strong>on</strong>s.b) If small bowel obstructi<strong>on</strong> c<strong>on</strong>sider:• hyoscine butylbromide (see above)• octreotide* initially 300 - 500mcg per day by csci: reduces volume ofintestinal secreti<strong>on</strong>s and inhibits motility. Effect may take several days toappear. The final effective dose is likely to be 200 - 800mcg per day.Laxatives• Check that lower rectum is empty.• Do not use if there is complete obstructi<strong>on</strong>.• If there is partial intermittent obstructi<strong>on</strong>, can use faecal softeners withcauti<strong>on</strong>:docusate sodium up to 200mg tdsmagnesium hydroxide mixture 20 - 30 ml od or bdmacrogols (eg Movicol) 1 sachet up to tds.Shrinkage of tumour masses• Dexamethas<strong>on</strong>e 4 - 8mg daily may help to relieve peri-tumour oedema and sorelieve obstructi<strong>on</strong>, particularly at the gastric outlet.• Horm<strong>on</strong>e/cytotoxic therapy is occasi<strong>on</strong>ally indicated if the patient’s overallc<strong>on</strong>diti<strong>on</strong> is good, especially in primary tumours of ovary, col<strong>on</strong> or breast.• Radiotherapy is occasi<strong>on</strong>ally appropriate for low large bowel tumours.21* indicates that this is best managed by specialists
MOUTH PROBLEMSGood mouth care is essential to the well being of debilitated patients. Althoughmouth problems are very comm<strong>on</strong> (up to 90% of patients in some surveys), it isoften a neglected area of care.Diagnosis1 Assess oral cavity daily using a pen torch and spatula. Note the state of thelips, teeth/dentures (remove the dentures for examinati<strong>on</strong>), mucousmembranes and t<strong>on</strong>gue, and also the type/volume of saliva.2 Assess nutriti<strong>on</strong>al status - quality of diet and adequacy of fluid intake.3 Assess mental state - will determine the patient’s ability and willingness toparticipate in his or her care.Causes / Risk factors1 Dry mouth (xerostomia) especially from drugs (opioids, tricyclicantidepressants, antimuscarinics), dehydrati<strong>on</strong> (reduced intake or diuretics)and local radiotherapy.2 Poor oral and dental hygiene.3 Poor oral intake leading to decreased masticati<strong>on</strong>.4 Poor nutriti<strong>on</strong>al state, especially if leading to vitamin deficiencies.5 Infecti<strong>on</strong>s: viral, bacterial and fungal.6 Some cytotoxics can cause mucositis and acute ulcerati<strong>on</strong>; radiotherapy cancause mucositis.7 Corticosteroids and diabetes predispose to oral candidosis.8 Oral tumours.Management1 Review medicati<strong>on</strong>s causing dry mouth or other oral problems.2 Treat oral infecti<strong>on</strong>s.3 Maintain frequent attenti<strong>on</strong> to good oral hygiene.4 Alcohol-free chlorhexidine mouthwash may be used in debilitated patients -inhibits plaque formati<strong>on</strong> and is antiseptic.5 Maintain good denture care by cleaning and rinsing thoroughly. Dentures canbe named by writing <strong>on</strong> them with a pencil and applying a coat of nail varnish.* indicates that this is best managed by specialists 22
Specific problemsLack of good quality saliva1 Salivary stimulants • Sugar free chewing gum• Pilocarpine 5 - 10mg tds (or 1 - 2 drops 4%,flavoured to taste), bethanecol 10mg tds2 Saliva substitutes • Spray eg Xerotin (n<strong>on</strong>-acidic, no animal products)• Gels eg Biotène oral balance3 Sips of water or ice cubes may give short term relief.Oral Thrush1 Increase the flow of saliva as described above.2 Nystatin oral suspensi<strong>on</strong> 1 - 5ml qds for at least 7 days.3 Fluc<strong>on</strong>azole 50mg daily by mouth for 7 days. Less effective in xerostomia.Note that there is increasing resistance to triazole antifungals.4 Ensure that dentures are thoroughly cleaned and disinfected.Painful mouth1 Treat infecti<strong>on</strong>s - metr<strong>on</strong>idazole for fungating tumours in the mouth, herpesorogingivitis is extremely painful (may need aciclovir).2 For symptomatic relief use Difflam or soluble aspirin gargle, flurbiprofenlozenges or systemic NSAIDs by other routes.3 Aphthous ulcers may resp<strong>on</strong>d to local steroid, eg hydrocortis<strong>on</strong>e pellets.4 For chemotherapy induced mucositis try Mugard or sucralfate suspensi<strong>on</strong>.5 Other analgesic opti<strong>on</strong>s: oramorph liquid held in the mouth, localanaesthetic (lidocaine) spray, may cause initial stinging.Excessive salivati<strong>on</strong> or drooling with swallowing problems1 May be helped by hyoscine hydrobromide patch 1mg / 72hrs, atropinedrops 1% sub lingual, glycopyrr<strong>on</strong>ium or hyoscine butylbromide via csci(see p57), or amitriptyline (low dose) via gastrostomy. These may makethe saliva unacceptably sticky, in which case propranolol can bec<strong>on</strong>sidered.2 Some units offer botulinum toxin injecti<strong>on</strong> to the salivary glands to reducesalivati<strong>on</strong>.3 In severe cases, radiotherapy to the salivary glands may be c<strong>on</strong>sidered.23* indicates that this is best managed by specialists
ANOREXIADiagnosis1 A reduced interest in food which at its most severe may manifest as nausea.2 Often associated with taste changes.3 May increase (appetite diminishes) as the day goes <strong>on</strong>.4 Distinguish from mouth problems, difficulties with swallowing, and earlysatiety due to gastric stasis.Causes / Risk factors1 Extensive malignancy (but occasi<strong>on</strong>ally occurs as a presenting symptom).2 Unc<strong>on</strong>trolled symptoms.3 Psychological, emoti<strong>on</strong>al and spiritual distress eg anxiety and depressi<strong>on</strong>.4 Drugs, especially cytotoxics, digoxin.Management1 Treat nausea, pain and other symptoms.2 Reduce psychological distress with support and counselling.3 Treat depressi<strong>on</strong>, preferably not using SSRIs as can increase anorexia.4 Review drugs.5 Aim to provide frequent, small, attractive porti<strong>on</strong>s within pleasant and socialsurroundings.6 Drug therapy - if drugs are needed and there are no c<strong>on</strong>tra-indicati<strong>on</strong>s:• alcohol before meals• megestrol acetate 160 - 320mg daily: may take 2 - 3 weeks to resp<strong>on</strong>d(increased risk of thrombosis)• dexamethas<strong>on</strong>e 2 - 4mg or prednisol<strong>on</strong>e 10 - 30mg om (see p52).ANOREXIA/CACHEXIA/FATIGUE SYNDROMEDiagnosis1 A syndrome of loss of appetite, fatigue, and profound weight and muscle loss.2 There is usually an associated rise in acute-phase proteins, eg CRP.Causes / Risk factors1 Usually associated with cancer but may occur with heart failure and chr<strong>on</strong>icinfecti<strong>on</strong> or inflammati<strong>on</strong>.2 Cytokine release leading to proteolysis, lipolysis, increased resting energyexpenditure, and hypothalamic disturbances including anorexia.Management1 Correct associated problems (see above).2 Fatigue <strong>management</strong> programme - gentle but regular exercise programme toreduce muscle loss and promote adaptive behaviour.3 Dexamethas<strong>on</strong>e 2 - 4mg om or NSAIDs to reduce inflammatory process.4 Anecdotal evidence for methylphenidate* or modafinil* to improve fatigue.5 Evidence is unclear <strong>on</strong> the place of fish oils (eg Maxepa), nutriti<strong>on</strong>alsupplements (eg Prosure) and anabolic steroids.* indicates that this is best managed by specialists 24
CONSTIPATIONC<strong>on</strong>stipati<strong>on</strong> is comm<strong>on</strong> in patients with advanced disease. It can causeabdominal pain and urinary retenti<strong>on</strong>. Even if not eating, patients can becomec<strong>on</strong>stipated due to accumulati<strong>on</strong> of faecal matter formed from gut secreti<strong>on</strong>s,cells and bacteria. It is far better to anticipate and prevent c<strong>on</strong>stipati<strong>on</strong> than towait until treatment is urgent.Diagnosis1 Passing harder and/or less frequent stools than normal.2 Faecal impacti<strong>on</strong> may present with overflow (‘spurious diarrhoea’).3 Rectal examinati<strong>on</strong>: empty or impacted, collapsed or cavernous?4 Exclude intestinal obstructi<strong>on</strong>.Causes/Risk factors1 Drugs, especially oral opioids, antidepressants, antispasmodics, <strong>on</strong>dansetr<strong>on</strong>.2 Inactivity, immobility, weakness, lack of privacy.3 Dehydrati<strong>on</strong> due to poor fluid intake, vomiting, polyuria, fever.4 Hypercalcaemia.5 C<strong>on</strong>current disease including painful anal c<strong>on</strong>diti<strong>on</strong>s, neurological disorders.Management1 Reduce or eradicate underlying cause(s) as far as possible.2 If general c<strong>on</strong>diti<strong>on</strong> allows, mobilise and encourage fluids.3 Drug treatments:a) Use softeners if stool is hard, stimulants if soft stool is not expelled.b) Patients taking regular opioids will usually and routinely need both,although macrogols al<strong>on</strong>e are often sufficient.StimulantsSenna 2 - 4 tablets nocte or bd.Bisacodyl tablets 5 - 20mg nocte or bd.Sodium picosulphate soluti<strong>on</strong> 5 - 10ml od/bd.SoftenersDocusate sodium capsules 200mg nocte or bd.OsmoticsMacrogols (eg Movicol) 1 sachet od or bd.Magnesium hydroxide 20 - 30ml od or bd.Lactulose 10 - 15ml bd (not advised, excess wind).Combined preparati<strong>on</strong>s Codanthramer liquid or capsules (two strengths).Codanthrusate liquid or capsules.4 Often, patients need suppositories or enemas for established c<strong>on</strong>stipati<strong>on</strong>. Ifrectal faeces, glycerol or bisacodyl suppositories usually given. If the rectumis empty but col<strong>on</strong> loaded with hard stool, use arachis oil retenti<strong>on</strong> enemaovernight (check no peanut allergy) followed by phosphates enema. If opioidrelated c<strong>on</strong>stipati<strong>on</strong> c<strong>on</strong>sider methylnaltrex<strong>on</strong>e sc (dose according to weight).5 Manual evacuati<strong>on</strong> should be a last resort, and c<strong>on</strong>sent obtained after fullexplanati<strong>on</strong>. Sedati<strong>on</strong> may be required.25* indicates that this is best managed by specialists
DIARRHOEADiagnosisThe patient who speaks of ‘diarrhoea’ may be referring either to the frequency orto the looseness of bowel moti<strong>on</strong>s. An accurate history and examinati<strong>on</strong> arecrucial: assess for watery/liquid stools usually with an increased stool frequency.Causes / Risk Factors1 Excess laxative use.2 Impacted faeces with overflow (spurious diarrhoea).3 Side effects of some drugs, eg chemotherapy, antibiotics, PPIs, NSAIDs.4 Infecti<strong>on</strong>s, including C. difficile, upper GI bacterial overgrowth, giardia.5 Partial intestinal obstructi<strong>on</strong>.6 Previous treatment: pelvic radiotherapy, extensive bowel resecti<strong>on</strong>.7 On initiati<strong>on</strong> of enteral feeding.8 Pancreatic insufficiency, characterized by bulky, offensive stools which float.9 Effects of some tumours, eg carcinoid, mucus secreti<strong>on</strong> in rectal cancer.10 Other - eg inflammatory bowel disease, bile salt malabsorpti<strong>on</strong>, sec<strong>on</strong>darylactose intolerance, aut<strong>on</strong>omic neuropathy (diabetes, paraneoplastic), IBS.Management1 Review all drugs, including laxatives and n<strong>on</strong>-prescripti<strong>on</strong> drugs.2 Screen for infecti<strong>on</strong>s and prescribe antibiotics as appropriate.3 Address dehydrati<strong>on</strong> if appropriate.4 Specific treatmentsSteroids given locally or systemically for radiati<strong>on</strong> induced diarrhoea.Pancreatic enzymes (Cre<strong>on</strong> capsules; 3 strengths) for steatorrhoea.Metr<strong>on</strong>idazole for bacterial overgrowth/blind loop syndrome.Octreotide* (see pp21, 57) for faecal fistulae, carcinoid syndrome.Colestyramine for bile salt malabsorpti<strong>on</strong>.5 Symptomatic treatmentsLoperamide 2 - 4mg every 6 hours; binds to opioid receptors in gut.Codeine phosphate 30 - 60mg tds - qds.Co-phenotrope (Lomotil) 2 tablets up to qds.FISTULAEManagement1 Assess fistula size, site and type, and patient's overall c<strong>on</strong>diti<strong>on</strong>.2 Prevent excoriati<strong>on</strong> with a barrier product.3 Collect effluent in a closed stoma bag. A good seal is needed to minimiseleakage and odour. If necessary seek advice from stoma care nurses.4 Metr<strong>on</strong>idazole may be helpful if there is blind loop or overgrowth ofanaerobes.5 Surgical interventi<strong>on</strong> may be appropriate.6 Octreotide* by csci may be helpful in reducing effluent, see pp21, 57.* indicates that this is best managed by specialists 26
ASCITESDiagnosis1 Clinical assessment: progressive distensi<strong>on</strong>, shifting dullness, fluid thrill.2 Abdominal ultrasound (with marking for paracentesis if appropriate).3 Exclude tumour masses, organomegaly, distended bladder, intestinalobstructi<strong>on</strong>.Causes / Risk factors1 Perit<strong>on</strong>eal metastases - may be associated with extra-abdominal primary sites.2 Tumour obstructing retroperit<strong>on</strong>eal/diaphragmatic lymph system.3 Hypoalbuminaemia, usually associated with extensive liver metastases.4 Sec<strong>on</strong>dary sodium retenti<strong>on</strong>.5 Venous compressi<strong>on</strong> or thrombosis of inferior vena cava or hepatic vein.6 Other c<strong>on</strong>current disease, eg heart failure, cirrhosis.Management1 If symptoms are minor, explanati<strong>on</strong> and reassurance may be sufficient.2 Paracentesis may be appropriate for patients with a tense, uncomfortable,distended abdomen, especially if associated with breathlessness. Can useultrasound to identify suitable locati<strong>on</strong>. Drain up to 5 litres of fluid per day,but sudden release of abdominal tensi<strong>on</strong> may lead to venous decompressi<strong>on</strong>,hypotensi<strong>on</strong> and collapse. Remove drain after 1 - 2 days, there is no advantagein draining to dryness. If leakage c<strong>on</strong>tinues after drain is removed, place stomabag over puncture site.3 Perit<strong>on</strong>eo-venous shunt (eg Denver or LeVeen shunt) may be c<strong>on</strong>sidered forselected patients who require frequent paracentesis as electrolytes and albuminare c<strong>on</strong>served, or indwelling drainage systems eg PleurX.4 Drug therapyAnalgesia (from paracetamol up to str<strong>on</strong>g opioids) for abdominal pain ordiscomfort of distensi<strong>on</strong>.Antiemetics: domperid<strong>on</strong>e or metoclopramide for gastric stasis.Diuretics: furosemide (especially if dependent oedema) 40 - 80mg od;spir<strong>on</strong>olact<strong>on</strong>e (especially if low albumin) 50 - 200mg od. Diuretics are lesslikely to be effective if due to perit<strong>on</strong>eal metastases. M<strong>on</strong>itor electrolytes,renal functi<strong>on</strong> and blood pressure.Corticosteroids: dexamethas<strong>on</strong>e 2 - 4mg om may reduce lymph blockage.Laxatives as appropriate to treat c<strong>on</strong>stipati<strong>on</strong>.Cytotoxic chemotherapy (local or systemic) may be appropriate, especially forprimary carcinomas of ovary, breast or col<strong>on</strong> - seek <strong>on</strong>cological advice.27* indicates that this is best managed by specialists
BREATHLESSNESSBreathlessness is usually multifactorial. There is inevitably a psychologicalcomp<strong>on</strong>ent – being breathless is always frightening and patients often haveunspoken fears about how they will die.Investigati<strong>on</strong>s eg chest x-rays, scans and blood tests may be needed to excludereversible causes but are often of limited value; oxygen saturati<strong>on</strong> will guide theuse of oxygen. A therapeutic trial of treatments, either singly or in combinati<strong>on</strong>,is often necessary to find out what works in an individual patient.Causes / Risk factorsA1Impaired gas exchange.Airflow obstructi<strong>on</strong>a) Large airways: tumourextrinsic compressi<strong>on</strong>laryngeal palsyradiati<strong>on</strong> strictureb) Small airways: lymphangitis carcinomatosaCOPD, asthma2 Decreased effective lung volume effusi<strong>on</strong>spneumothoraxextensive tumourcollapseinfecti<strong>on</strong>gross abdominal distensi<strong>on</strong>3 Increased lung stiffnessfibrosispulm<strong>on</strong>ary oedemalymphangitis carcinomatosa4 Decreased alveolar gas exchange pulm<strong>on</strong>ary embolismpericardial effusi<strong>on</strong>thrombotic tumourfibrosis5 Pain pleurisychest wall infiltrati<strong>on</strong>rib/vertebral fracturesliver capsule pain6 Neuromuscular failure paraplegiachr<strong>on</strong>ic neuromuscular diseasesphrenic nerve palsycachexia, dec<strong>on</strong>diti<strong>on</strong>ingparaneoplastic syndromesB Increased demand1 Anxiety2 Anaemia3 Metabolic acidosis* indicates that this is best managed by specialists 28
ManagementGeneral treatmentsCan be employed whilst investigating for an identifiable and correctable cause.General and specific <strong>management</strong>s should be used in parallel. C<strong>on</strong>siderc<strong>on</strong>sulting the respiratory team.ABN<strong>on</strong> drug treatments• A fan (hand held or fixed) or cool air across the face is often helpful.• Proper positi<strong>on</strong>ing for easier breathing.• Explore the patient’s fears about breathlessness.• General and specific reassurance (eg that the patient will not suffocate).• Explanati<strong>on</strong> of the mechanisms of breathlessness.• Breathing exercises, relaxati<strong>on</strong> training ) ‘pulm<strong>on</strong>ary rehabilitati<strong>on</strong>’ byCounselling and readaptati<strong>on</strong> ) physiotherapist/specialist nurse• Acupuncture, aromatherapy, reflexology.Drug treatments• Nebulised saline often helps where there are tenacious secreti<strong>on</strong>s.• Opioids often help reduce the subjective sensati<strong>on</strong> of breathlessness; thereis no evidence that they shorten life. If opioid naïve, start <strong>on</strong> 2.5mg of oralmorphine 4 hourly prn and titrate upwards. If already <strong>on</strong> morphine for pain,the dose may need to be increased by 25 - 50% for co-existingbreathlessness. Morphine/diamorphine often used via csci when severebreathlessness. Nebulised opioids are no l<strong>on</strong>ger advised.• Benzodiazepines are often used in combinati<strong>on</strong> with opioids for theiranxiolytic effect. Use diazepam 2 - 10mg daily for background c<strong>on</strong>trol withopti<strong>on</strong> of lorazepam 0.5 - 1mg sublingually (quick-acting) for acute crisesand panic. Midazolam 2.5 - 10mg sc stat or 5 - 50mg per 24 hours by csci ifpatient is not able to take oral medicati<strong>on</strong>.• Oxygen has variable effects; it is difficult to predict who will benefit otherthan by individual therapeutic trial, but patients with oxygen saturati<strong>on</strong>s
DEDecisi<strong>on</strong>s about ventilati<strong>on</strong>When a patient may be at risk of respiratory failure, the risks/benefits ofmechanical ventilati<strong>on</strong> (invasive or n<strong>on</strong>-invasive) should be c<strong>on</strong>sidered and,where appropriate, discussed with the patient in order to avoid crisisdecisi<strong>on</strong>s about ventilati<strong>on</strong>. In the majority of cases invasive ventilati<strong>on</strong>will not be appropriate. Careful documentati<strong>on</strong> of the decisi<strong>on</strong> is necessary.Sudden major airway obstructi<strong>on</strong>This is a palliative care emergency requiring urgent sedati<strong>on</strong>, eg midazolam10mg iv or sc. The cause should then be treated if possible.Specific treatments1 Extensive lung metastases: dexamethas<strong>on</strong>e 4 - 8mg daily (see p52).2 Lymphangitis carcinomatosa: dexamethas<strong>on</strong>e 4 - 8mg daily (see p52),chemotherapy.3 Large airway narrowing: radiotherapy, endobr<strong>on</strong>chial stents, dexamethas<strong>on</strong>e4 - 8mg daily (see p52).4 Br<strong>on</strong>choc<strong>on</strong>stricti<strong>on</strong>: inhaled br<strong>on</strong>chodilators, steroids.5 a) Pleural effusi<strong>on</strong>: drainage, pleurodesis, PleurX catheterb) Pericardial effusi<strong>on</strong>: drainage, sometimes formati<strong>on</strong> of a pericardialwindow.c) Ascites: drainage (see p27).6 Infecti<strong>on</strong>: antibiotics as appropriate.7 Respiratory secreti<strong>on</strong>s: physiotherapy, nebulised saline, mucolytics egcarbocisteine (if thick). (Upper airway secreti<strong>on</strong>s – see pp23, 59).8 Pulm<strong>on</strong>ary emboli: anticoagulati<strong>on</strong> as appropriate (see p50).9 Pulm<strong>on</strong>ary oedema: diuretics, low dose opioids.10 Chest wall/pleuritic pain: NSAIDs, steroids, opioids, nerve blocks,radiotherapy, cordotomy (see Pain secti<strong>on</strong>).11 MND, other neuromuscular disorders: nasal or mask BiPAP, mainly nocte(seek Respiratory Team advice early).12 Laryngeal obstructi<strong>on</strong>/stridor: urgent ENT opini<strong>on</strong>, tracheostomy,dexamethas<strong>on</strong>e 4 - 8mg daily (see p52).13 Laryngeal nerve palsy: vocal cord injecti<strong>on</strong>, ENT opini<strong>on</strong>.14 Anaemia: transfusi<strong>on</strong> if appropriate (see p48).* indicates that this is best managed by specialists 30
COUGHDiagnosis1 Ask about sputum (and if possible observe) – quantity, c<strong>on</strong>sistency, colour.2 Is cough affected by positi<strong>on</strong>?3 Examine chest. Chest x-ray may be helpful.4 PEFR to check for reversibility – br<strong>on</strong>chospasm may present with cough.Causes / Risk factors1 Nasopharyngeal – post-nasal drip, candidosis, tumour.2 Laryngeal – tumour, inflammati<strong>on</strong>, infecti<strong>on</strong>.3 Br<strong>on</strong>chial – inflammati<strong>on</strong>, tumour, infecti<strong>on</strong>, ACE inhibitors,tracheo-oesophageal fistula.4 Pulm<strong>on</strong>ary – pneum<strong>on</strong>ia, alveolitis/fibrosis, abscess, br<strong>on</strong>chiectasis,oedema.5 Pleural – pleural effusi<strong>on</strong>.6 Mediastinal – tumour, lymphadenopathy.7 Gastric reflux – with or without frank aspirati<strong>on</strong>.ManagementTreat the cause where possible.1 More upright body positi<strong>on</strong>.2 Steam inhalati<strong>on</strong>s, nebulised saline, mucolytic for thick secreti<strong>on</strong>s.3 Chest physiotherapy where appropriate.4 Treat infecti<strong>on</strong>s unless the chest infecti<strong>on</strong> is a terminal event.5 Radiotherapy may help if cough is caused by tumour.6 Drug therapyGeneral:a Inhalati<strong>on</strong>s: benzoin co tincture, menthol & eucalyptus.b Simple linctus.c Low dose oral opioids: codeine, morphine.Specific:a Nasopharyngeal – post-nasal drip: antibiotics, nasal steroid spray.b Laryngeal – steroids via inhaler.– local anaesthetics* via nebuliser : bupivacaine 0.5%,5ml tds, at least 30 minutes before any food or drink;risk of idiosyncratic br<strong>on</strong>chospasm, may be severe.c Br<strong>on</strong>chial – br<strong>on</strong>chodilators in standard doses.– steroids orally or inhaled.– local anaesthetics* (see above).d Gastric reflux – antacids c<strong>on</strong>taining simetic<strong>on</strong>e or alginate.– prokinetic agents (see p19).31* indicates that this is best managed by specialists
HICCUPCauses / Risk factors1 Peripheral (diaphragmatic or phrenic nerve irritati<strong>on</strong>)• gastric distensi<strong>on</strong> or irritati<strong>on</strong>• liver enlargement/involvement• intrathoracic nodes/tumour• tumour irritati<strong>on</strong>/involvement of diaphragm.2 Central (medullary stimulati<strong>on</strong>)• raised intracranial pressure• brain stem CVA/tumour• uraemia (also causes gastric stasis).Management1 Rebreathing with a paper bag (raises pCO 2 levels).2 Drinking cold water or taking a teaspo<strong>on</strong> of granulated sugar (pharyngealstimulati<strong>on</strong>).3 Phrenic nerve block for intractable hiccup.4 Drug therapyPeripheral causes:metoclopramide 10mg tds - qdsdomperid<strong>on</strong>e 10 - 20mg tds - qdsantacids c<strong>on</strong>taining simetic<strong>on</strong>eprot<strong>on</strong> pump inhibitors or ranitidine 150mg bddexamethas<strong>on</strong>e 4 - 8mg odbaclofen 5mg od - tdsnifedipine 10mg od - tdsCentral causes:haloperidol 0.5mg od - tdsdexamethas<strong>on</strong>e 4 - 8mg oddiazepam 2mg od - bd or midazolam by cscichlorpromazine* 25mg od - tds (very sedating)or levomepromazine by csciN<strong>on</strong>e of these treatments is c<strong>on</strong>sistently reliable.* indicates that this is best managed by specialists 32
RAISED INTRACRANIAL PRESSUREDiagnosis1 Severe headache worse when lying down or straining.2 Vomiting, c<strong>on</strong>vulsi<strong>on</strong>s, mental symptoms, diplopia, restlessness.3 Papilloedema may be present.4 CT/MRI scan may be appropriate.Causes / Risk factors1 Cerebral metastases (comm<strong>on</strong> with some primaries, eg lung, breast,melanoma, and rare with others, eg prostate).2 Primary cerebral tumour.3 Other causes – abscess, cerebro-vascular event, sagittal sinus thrombosis,sec<strong>on</strong>dary hydrocephalus following surgery.Management1 Raise head of the bed.2 C<strong>on</strong>sider cranial irradiati<strong>on</strong> or neurosurgery for malignancy if prognosis/statuswarrants it.3 Drug therapy:Dexamethas<strong>on</strong>e up to 16mg per day. Avoid doses after 2pm as may add toinsomnia. Gradually reduce dose to minimum effective (see p52),m<strong>on</strong>itoring that symptoms remain c<strong>on</strong>trolled. Withdraw dexamethas<strong>on</strong>e ifno improvement after 7 days <strong>on</strong> 16mgs daily. (Phenytoin andcarbamazepine may reduce therapeutic effect by up to 50%, and vice versa,by enzyme inducti<strong>on</strong>).Analgesics for headache – eg paracetamol.Antiepileptics should be c<strong>on</strong>sidered in the presence of cerebral malignancy,but normally reserved for those who have had fits (see p34).Acetazolamide* 250 - 500mg od - bd, anecdotal evidence for benefit.33* indicates that this is best managed by specialists
FITSDiagnosis1 Identify whether grand mal, focal fit, absence or status epilepticus.2 Exclude syncopal attacks, cardiac arrhythmias, TIAs etc.Causes / Risk factors1 Previous epilepsy, brain trauma/surgery, brain tumours or metastases.2 Drugs lowering epileptic threshold: eg phenothiazines, tricyclics, tramadol.3 Drug interacti<strong>on</strong>s: antiepileptics have many variable and unpredictableinteracti<strong>on</strong>s; they also reduce the effect of steroids. Plasma levels ofphenytoin and carbamazepine can be checked; allow <strong>on</strong>e week after any dosechange for plasma levels to reach steady state.4 Drug withdrawal, eg steroids, alcohol.5 Metabolic disturbance, eg hypoxia, hyp<strong>on</strong>atraemia, hypoglycaemia.ManagementPreventi<strong>on</strong> of fits1 Sodium valproate initially 100 - 200 mg bd/tds increasing every 3 days to1 - 2 grams per day.Carbamazepine initially 100 - 200mg od/bd increasing by 100 - 200mgevery 2 weeks to 800 - 1200mg per day.Phenytoin 200 - 400mg nocte adjusted according to plasma level.Lamotrigine initially 25 - 50mg od, increasing by 50mg every 2 weeks to100 - 200mg daily.Avoid combinati<strong>on</strong> therapy if possible.2 If unable to take oral medicati<strong>on</strong>:midazolam 10 - 60mg/24 hours by csciphenobarbital* 400 - 800mg/24 hours by cscicl<strong>on</strong>azepam* 1 - 4mg/24 hours by cscicarbamazepine suppositories bd (note 125mg pr is equivalent to 100mg po).3 Dexamethas<strong>on</strong>e 8 - 16mg per day if brain tumour/metastases.Grand mal c<strong>on</strong>vulsi<strong>on</strong>s1 First aid precauti<strong>on</strong>s, explanati<strong>on</strong> and reassurance.2 Diazepam rectally 10 - 20mg or midazolam intranasally or buccally 5 - 10 mg.Status epilepticus1 Outside hospital: diazepam rectally 10 - 20 mg.midazolam 5 - 10 mg intranasally, buccally or slowlyiv and repeat as necessary after 15-20 minutes.2 In hospital: lorazepam 4 mg iv.c<strong>on</strong>sider iv infusi<strong>on</strong> of phenytoin or phenobarbital.* indicates that this is best managed by specialists 34
SPINAL CORD COMPRESSIONDiagnosisOccurs in 5 - 10% of patients with advanced cancer. It is therefore essential to bealert for early signs, which can be subtle (eg heaviness of the legs). Do not waitfor signs to become unequivocal: early diagnosis and urgent treatment withinhours are vital to improved outcome, mobility and c<strong>on</strong>tinence. Once paralysed,<strong>on</strong>ly 5% walk again, but some survive more than <strong>on</strong>e year.1 Often back pain with or without radiati<strong>on</strong> in the territory of a nerve root,followed by sensory changes, bladder or bowel disturbance, and leg weakness,but can be any combinati<strong>on</strong> of these.2 If at thoracic level, there is likely to be a sensory level with brisk reflexes; ifcauda equina compressi<strong>on</strong>, reflexes may be diminished.Causes / Risk factors1 Epidural invasi<strong>on</strong> from vertebral body metastases or paravertebral nodes.2 B<strong>on</strong>y deformity from vertebral body collapse.3 Blood borne epidural or intradural metastases.4 Primary spinal cord tumour.ManagementDepending <strong>on</strong> patient’s general c<strong>on</strong>diti<strong>on</strong>:1 Immediate: • dexamethas<strong>on</strong>e 16mg per day• emergency MRI scan, or CT scan if MRI unavailable• urgent referral to <strong>clinical</strong> <strong>on</strong>cologist and discuss withneuro/spinal surgical team.2 a) If gradual <strong>on</strong>set, or if rapid <strong>on</strong>set but paraplegia present less than 24 hours,surgical decompressi<strong>on</strong> may be possible; otherwise radiotherapy.b) If rapid <strong>on</strong>set and established paraplegia, radiotherapy may not help exceptfor pain relief.3 Established paraplegia: • pressure area care• urinary catheter• bowel regulati<strong>on</strong> – allow some c<strong>on</strong>stipati<strong>on</strong> anduse regular enemas or suppositories• physio and OT assessment – wheelchair, homemodificati<strong>on</strong>s• c<strong>on</strong>sider prophylaxis against venous thrombosis• psychological readjustment.4 Specialist palliative care assessment for <strong>management</strong> and/or rehabilitati<strong>on</strong> isrecommended.35* indicates that this is best managed by specialists
DEPRESSIONIt is important to distinguish between <strong>clinical</strong> depressi<strong>on</strong>, profound sadness anddementia. Be aware that many of the usual somatic symptoms of depressi<strong>on</strong> suchas anorexia, weight loss and sleep disturbance may already be present in patientswith malignant disease. Depressi<strong>on</strong> may be hidden behind a brave but hollowsmile or even overt joking. A therapeutic trial of antidepressants may beacceptable.DiagnosisBiological symptoms• Diurnal variati<strong>on</strong> in mood; may be agitati<strong>on</strong>.• Sleep disturbance, especially with frequent or early morning waking.• Anorexia that does not improve with steroids.Psychological symptoms• Persistent, pervasive low mood with loss of pleasure and enjoyment.• Morbid guilt, feelings of helplessness and worthlessness/low self esteem.• Suicidal ideas and intenti<strong>on</strong>s.Causes / Risk factors1 Past history of depressi<strong>on</strong>.2 Need to adjust to many life changes over a short period of time.3 Poor symptom c<strong>on</strong>trol.4 Immobility and isolati<strong>on</strong> with poor quality of life and lack of support.5 Inadequate or inaccurate informati<strong>on</strong> about illness or prognosis.6 Early dementia.7 Drugs – corticosteroids (predominantly <strong>on</strong> withdrawal), benzodiazepines,some cytotoxics, antihypertensives and neuroleptics.Management1 Minimise the causes, especially 3 - 5 above.2 Provide psychological support.3 Drug therapy is recommended in moderate to severe depressi<strong>on</strong>. NICEguidance is that first line treatment should be with an SSRI. Alternativeswithin palliative care would include mirtazapine, amitriptyline anddosulepin. If there is a lack of resp<strong>on</strong>se or unacceptable side effects,c<strong>on</strong>sider a switch to another SSRI or to mirtazapine.* indicates that this is best managed by specialists 36
ANXIETYDiagnosis1 Feeling of being <strong>on</strong> edge, restless or agitated, apprehensi<strong>on</strong>.2 Inability to c<strong>on</strong>centrate.3 Physical effects such as sweating, tachycardia, staring eyes with dilatedpupils.4 Anxiety may be a presenting feature of an underlying depressi<strong>on</strong>.Causes / Risk factors1 Past history of anxiety.2 Poor symptom c<strong>on</strong>trol.3 Inadequate/inaccurate informati<strong>on</strong>.4 Unfamiliar surroundings.5 Uncertainty about the future.6 C<strong>on</strong>cern for family/finances etc.7 Early dementia.8 Depressi<strong>on</strong>9 Steroid treatment/salbutamol therapy.10 Withdrawal of drugs eg opioids/benzodiazepines.Management1 Support for patient and family.2 Appropriate informati<strong>on</strong> and discussi<strong>on</strong> with patient and family.3 Relaxati<strong>on</strong> techniques and complementary therapies.4 Treatment of depressi<strong>on</strong> if present (see p36).5 If part of agitati<strong>on</strong> with c<strong>on</strong>fusi<strong>on</strong>, see p41.6 Drug therapy:Diazepam 2mg bd and/or 5mg at night – for short term use.Propranolol 40mg bd to tds for somatic symptoms.Lorazepam 0.5 - 1mg given sublingually may be helpful in panic attacks.If the patient is unable to swallow or has a syringe driver for other reas<strong>on</strong>s,c<strong>on</strong>sider midazolam 10 - 20mg per 24 hours by csci.37* indicates that this is best managed by specialists
INSOMNIADiagnosisInsomnia is a subjective complaint of poor sleep. This can mean insufficient,interrupted or n<strong>on</strong>-restorative sleep or sleep at the wr<strong>on</strong>g time. It is important todistinguish between an inability to get to sleep (eg anxiety, c<strong>on</strong>fusi<strong>on</strong>) and atendency to wake early or repeatedly (eg depressi<strong>on</strong>, urinary problems, pain).Causes / Risk factors1 Anxiety or depressi<strong>on</strong>.2 Poor symptom c<strong>on</strong>trol.3 Nocturia.4 Envir<strong>on</strong>mental changes – inpatient admissi<strong>on</strong>, interrupti<strong>on</strong>s by staff.5 Fear – eg of going to sleep or of nightmares. Beware of well-intenti<strong>on</strong>edreassurance that ‘you will die in your sleep’.6 Drugs – stimulants (caffeine etc), steroids (worse if given later than 2pm),diuretics, opioids (vivid dreams, hallucinati<strong>on</strong>s), fluoxetine, propranolol(nightmares).7 Drug withdrawal – alcohol, benzodiazepines, barbiturates.Management1 Minimise the causes – c<strong>on</strong>trol symptoms as far as possible, keep interrupti<strong>on</strong>sto a minimum, reduce drug therapy or give stimulants early in the day, counselabout fears and anxieties.2 Establish a good sleep pattern – allow a siesta to prevent going to bed tooearly.3 Encourage a c<strong>on</strong>sistent bedtime ritual, a warm milky drink may help.4 Encourage relaxati<strong>on</strong> techniques.5 Drug therapy:Benzodiazepines eg temazepam 10 - 20mgZopicl<strong>on</strong>e 3.75 - 7.5mg, zolpidem 5 - 10 mg or zalepl<strong>on</strong> 5 - 10mg may havefewer residual effects than benzodiazepines.Clomethiazole (1 - 2 capsules) has a short durati<strong>on</strong> of acti<strong>on</strong>.Amitriptyline 10 - 150mg or dosulepin 25 - 75mg if early morning waking.Melat<strong>on</strong>in* 2mg for 1 - 3 weeks – increasing anecdotal evidence for use insome sleep disturbances eg day-night reversal.Note – all as a single dose at night, short term use advised– hypnotics may increase risk of falls and nocturnal c<strong>on</strong>fusi<strong>on</strong>.* indicates that this is best managed by specialists 38
DROWSINESSCauses / Risk factorsOrganic1 Disease progressi<strong>on</strong> and likely impending death.2 Infecti<strong>on</strong>, especially within respiratory and urinary tracts.3 Raised intracranial pressure.Biochemical1 Metabolic abnormalities:• uraemia, especially if <strong>on</strong> opioids• hyper/hypoglycaemia• hypercalcaemia• hyp<strong>on</strong>atraemia• hepatic failure• respiratory failure (blood gas analysis likely to be inappropriate).2 Drugs :Opioids, tricyclic antidepressants, benzodiazepines, antimuscarinics,antihistamines.Other1 Fatigue.2 Insomnia.3 Psychological withdrawal.4 Post-ictal.Management1 Assess accurately; if the patient is near to death due to advanced disease,further interventi<strong>on</strong>s are unlikely to be appropriate.2 Correct physical causes listed above if indicated.3 Review doses of opioids and other sedative drugs.4 Drug therapy:Dexamethas<strong>on</strong>e up to 16mg daily for raised ICP.Antidepressants for retarded depressi<strong>on</strong> (see p36).Dexamethas<strong>on</strong>e 2 - 4mg daily may act as stimulant.Methylphenidate* 2.5mg bd initially may act as stimulant.39* indicates that this is best managed by specialists
CONFUSIONDelirium is typified by acute c<strong>on</strong>fusi<strong>on</strong>, often with visual illusi<strong>on</strong>s orhallucinati<strong>on</strong>s, together with increased or decreased psychomotor activity andfluctuating level of c<strong>on</strong>sciousness or attenti<strong>on</strong>. It must be distinguished fromdementia, which is associated with gradual <strong>on</strong>set poor short-term memory andno impairment of c<strong>on</strong>sciousness, and which will not be c<strong>on</strong>sidered here.Diagnosis1 Disturbance of c<strong>on</strong>sciousness with reduced ability to focus attenti<strong>on</strong>.2 Generalised impairment of cogniti<strong>on</strong> affecting memory, orientati<strong>on</strong>, attenti<strong>on</strong>and planning and organisati<strong>on</strong>al skills.3 Short history (usually hours to days) often with fluctuati<strong>on</strong> during the day.4 Evidence from the history, examinati<strong>on</strong>, or investigati<strong>on</strong>s that there may be aphysical cause.Causes / Risk factors1 Age and pre-existing cognitive deficit.2 Drugs – eg opioids, tricyclic antidepressants, antimuscarinics, any sedativedrug, baclofen; higher dose corticosteroids may cause hypomania.3 Infecti<strong>on</strong>, especially within respiratory and urinary tracts.4 Biochemical abnormalities – see list under Drowsiness, p39.5 Intracerebral causes – space-occupying lesi<strong>on</strong>s, infecti<strong>on</strong>s, strokes.6 Envir<strong>on</strong>ment changes – excessive unfamiliar stimuli, inpatient admissi<strong>on</strong>,social isolati<strong>on</strong>.7 Poor symptom c<strong>on</strong>trol – pain, c<strong>on</strong>stipati<strong>on</strong>, urinary retenti<strong>on</strong>, anxiety,depressi<strong>on</strong>.8 Alcohol or drug withdrawal.Opioid toxicity exacerbated by uraemia*, dehydrati<strong>on</strong> or infecti<strong>on</strong> is animportant cause of c<strong>on</strong>fusi<strong>on</strong> and hallucinati<strong>on</strong>s. Look for c<strong>on</strong>stricted pupils,myocl<strong>on</strong>ic jerks, skin hyperaesthesia. See p12.* indicates that this is best managed by specialists 40
Management1 Treat or minimise the possible causes, especially drugs and infecti<strong>on</strong>s.2 Minimise stimuli: nurse in a room with diffused lighting, little extraneousnoise, and few staff changes.3 Attempt to keep patient in touch with reality and envir<strong>on</strong>ment – eye c<strong>on</strong>tactand touch are often helpful.4 Allay fear and suspici<strong>on</strong> – explain all procedures, d<strong>on</strong>’t change positi<strong>on</strong> ofpatient’s bed, if possible have a friend or relative of patient present.5 Stress that patient is not going mad and that there may well be lucid intervals.6 Drug therapy:Oxygen if cyanosed/hypoxic and oxygen saturati<strong>on</strong>s are
RESTLESSNESSThis may be akin to delirium in some<strong>on</strong>e very close to death, or mayoccasi<strong>on</strong>ally reflect unresolved psychological or spiritual distress, especially ifthis has previously been a problem.Causes / Risk factors1 Physical discomfort – unrelieved pain, distended bladder or rectum, inabilityto move, insomnia, uncomfortable bed, breathlessness.2 Drugs – opioid toxicity (especially in renal, liver impairment), hyoscinehydrobromide (paradoxical agitati<strong>on</strong>), phenothiazines (akathisia).3 Infecti<strong>on</strong>.4 Raised intracranial pressure.5 Biochemical abnormalities – hypercalcaemia, uraemia, hypoxia.6 Psychological/spiritual distress – anger, fear, guilt. Beware especially ifpatient has been unwilling to discuss illness.Management1 Must be a multi-professi<strong>on</strong>al approach involving family or main carers.2 Accurately assess the patient.3 Ameliorate all physical elements if possible, eg analgesia, catheterisati<strong>on</strong>.4 Listen to the patient and discuss anger, fear and guilt if possible.5 May be very distressing for the family who will need much support. Theirpresence may help or may worsen the patient’s agitati<strong>on</strong>.6 If there are hallucinati<strong>on</strong>s or frank delirium, see p41.7 Drug therapy (see also p59):Diazepam – 2mg bd and/or 5mg nocte orally, 5 - 10mg pr.Midazolam – 10 - 60mg per 24 hours by csci or in divided doses scor buccal (may <strong>on</strong>ly last ~2 hours).Levomepromazine – 25 - 150mg per 24 hours orally or by csci.Cl<strong>on</strong>azepam* – 0.5 - 2mg per 24 hours by csci.Phenobarbital* – 200 - 1200mg per 24 hours by csci (with water butno other drugs) or sc in divided doses.* indicates that this is best managed by specialists 42
ITCHCauses/Risk factorsHistamine mediated1 Allergies, acute urticaria, insect bites.Histamine unrelated (unlikely to resp<strong>on</strong>d to antihistamines)1 Hepatic disease: eg biliary obstructi<strong>on</strong>.2 Chr<strong>on</strong>ic renal failure.3 Lymphoma.4 Paraneoplastic phenomen<strong>on</strong>.5 Parasites, eg scabies, fleas.6 Skin diseases, eg eczema, psoriasis.7 Graft versus host disease after allogenic b<strong>on</strong>e marrow transplant.8 Ir<strong>on</strong> deficiency.9 Systemic opioid therapy.Management1 Alleviate causes if possible.2 Avoid provocative influences eg rough clothing, vasodilators, overheating.3 Try to break the itch/scratch cycle – clip nails, cott<strong>on</strong> gloves, paste bandages.4 Add a handful of sodium bicarb<strong>on</strong>ate to a cool bath. Pat rather than rub dry.5 Avoid washing with soap and bubble bath; use a pH balanced soap substituteor emollient bath additives (see BNF secti<strong>on</strong> 13.2.1.1).6 Apply emollients topically (see BNF secti<strong>on</strong> 13.2.1) to combat dryness.7 Apply topical antipruritic loti<strong>on</strong>s (see BNF secti<strong>on</strong> 13.3) or use menthol 2% inaqueous cream.8 Drug therapy:• Antihistamineschlorphenamine 4mg qdsloratadine 10mg od (n<strong>on</strong>-sedating).• In obstructive jaundice stenting for comm<strong>on</strong> bile duct obstructi<strong>on</strong>colestyramine 4 - 8g daily (in intrahepatic stasis)rifampicin* 150 - 300mg od (enzyme inducer)naltrex<strong>on</strong>e* 25mg od (but reverses opioid analgesia)buprenorphine patch* 10 - 35mcg/h.• In uraemia<strong>on</strong>dansetr<strong>on</strong> 8mg odgabapentin (low dose)naltrex<strong>on</strong>e* 25mg od (but reverses opioid analgesia).• In lymphoma chemotherapy/radiotherapy; corticosteroidscimetidine 400mg bd.• In polycythaemia r v aspirin 75 - 150mg od.• Paraneoplastic pruritus paroxetine 5 - 20mg odmirtazapine 7.5 - 15mg nocte.• Other opti<strong>on</strong>s paroxetine 5 - 20mg odgabapentin* 100 - 300mg tds (for neuropathic itch)UVB phototherapy.9 C<strong>on</strong>sider early advice from dermatologist or palliative care physician.43* indicates that this is best managed by specialists
SWEATINGCauses / risk factors1 Fever.2 Envir<strong>on</strong>mental changes.3 Emoti<strong>on</strong>al – fear and anxiety (mainly c<strong>on</strong>fined to axillae, palms, and soles).4 Extensive malignancy, lymphomas and carcinoid.5 Aut<strong>on</strong>omic disturbance.6 Intense pain.7 Drugs – opioids, antidepressants (older and newer), steroids, alcohol.8 Horm<strong>on</strong>al disturbance – eg menopause, tamoxifen, goserelin.Management1 Treat the underlying disease, including infecti<strong>on</strong>s where appropriate.2 Stop causative drugs – try alternatives.3 Alter envir<strong>on</strong>ment – fans, reduce room temperature (unless cold sweats),avoid heavy bedclothes, wear cott<strong>on</strong> clothes or wicking material rather thansynthetic or mixed fibres, use moisture absorbing mattress covers, frequentbaths or sp<strong>on</strong>ging.4 Psychological support for anxiety.5 Drug therapy:Various drugs have been used with varying success:Paracetamol 1g qds (nocte for night pyrexias).NSAIDs: diclofenac SR 75mg nocte - bd, naproxen 250 - 500mg bd.Cimetidine 400 - 800mg nocte (be aware of interacti<strong>on</strong>s).Corticosteroids: dexamethas<strong>on</strong>e 2 - 4mg daily.Beta-blockers: propranolol 10 - 40mg od - qds.Anticholinergics: propantheline 15mg nocte - tds, oxybutynin 2.5 - 5mg bd,glycopyrr<strong>on</strong>ium by csci.Antidepressants: eg amitriptyline 10 - 75mg nocte.Cl<strong>on</strong>idine 25mcg od - bd for horm<strong>on</strong>al disturbance if HRT not appropriate.Thalidomide* 100 - 200mg nocte (in malignancy).* indicates that this is best managed by specialists 44
FUNGATING WOUNDSCauses/Risk factorsTumour infiltrati<strong>on</strong> of epithelium and its surrounding blood and lymphaticvessels.General Management1 Assess wound and patient’s overall c<strong>on</strong>diti<strong>on</strong>. C<strong>on</strong>sider <strong>management</strong> goal.2 Radiotherapy may reduce bleeding and discharge; surgery and skin graftingmay aid healing.3 Oral antibiotics may reduce infecti<strong>on</strong> and odour (see below).4 Clean wound with 0.9% sodium chloride at body temperature.5 Ensure adequate analgesia if painful.Specific <strong>management</strong>Examples of different brands of dressings are provided: further informati<strong>on</strong> isavailable in Appendix 8 of the BNF. We recommend that in the first instance theadvice of the local tissue viability nurse is sought, as there are likely to be specificlocal guidelines for the <strong>management</strong> of wounds.1 Of wound itself:light exudateheavy exudatecavitybleedinginfectedpainhydrogel.alginate dressing (eg Sorbsan) or fibrous hydrocolloid(eg Aquacel) with absorbent pads.alginate rope (eg Sorbsan) with foam dressing(eg Allevyn, Cavi-Care).alginate (eg Kaltostat or Sorbsan);may need to soak dressings with saline before removing;adrenaline 1:1000 either directly to wound or in dressing.metr<strong>on</strong>idazole gel (eg Anabact) and charcoal dressing(eg Clinisorb, Actisorb plus).morphine (or diamorphine) 10mg mixed in a hydrogel gel;short acting opioid preparati<strong>on</strong> for dressing changes (seep15/16)2 Systemic drug therapy:analgesics paracetamol, NSAIDs, opioids (see secti<strong>on</strong> <strong>on</strong> Pain).antibiotics metr<strong>on</strong>idazole orally to reduce pain and odour.antipruritic sedating antihistamine eg chlorphenamine.45* indicates that this is best managed by specialists
LYMPHOEDEMADiagnosisBy history and examinati<strong>on</strong>. Differentiate from heart failure, immobility, venousinsufficiency and obstructi<strong>on</strong>, chr<strong>on</strong>ic renal failure, hypoalbuminaemia, limbdependency.Causes/ Risk factors1 Primary c<strong>on</strong>genital or familial lymphoedema.2 Sec<strong>on</strong>dary obstructi<strong>on</strong> from tumour spread, surgery, or radiotherapy.3 Recurrent streptococcal infecti<strong>on</strong>s.ManagementManagement is based <strong>on</strong> skin care, lymph drainage, compressi<strong>on</strong> and exercise.1 Treatment should be undertaken by a trained practiti<strong>on</strong>er.2 Early referral to the local lymphoedema service will give the best chance ofmaximum improvement and c<strong>on</strong>trol of the c<strong>on</strong>diti<strong>on</strong> as cure is not possible.3 Clear explanati<strong>on</strong> of the lymphatic system, reas<strong>on</strong>s for c<strong>on</strong>diti<strong>on</strong> and meansof treatment will encourage compliance.4 Treat infecti<strong>on</strong>s before beginning treatment, according to local protocols.C<strong>on</strong>stant vigilance for and prompt treatment of further infecti<strong>on</strong>s is essential.5 Instructi<strong>on</strong>s <strong>on</strong> daily skin care of affected limb(s): use aqueous or similarcream; general advice to avoid cuts, sunburn, insect bites and injecti<strong>on</strong>s inaffected limb.6 M<strong>on</strong>itor progress by regular measurement and assessing c<strong>on</strong>diti<strong>on</strong> of tissues.7 Regular simple light superficial and proximal massage may help; should betaught with suitable exercise by trained practiti<strong>on</strong>er.8 Manual lymphatic drainage may help, taught by a trained practiti<strong>on</strong>er.9 Properly measured graduated compressi<strong>on</strong> hosiery worn daily except duringacute inflammatory episode; remove at night.10 Multi-layered compressi<strong>on</strong> bandaging may be appropriate for a limited periodinitially.11 Occasi<strong>on</strong>ally a multi-chambered sequential pneumatic compressi<strong>on</strong> unit mayhelp reduce limb volume unless there is quadrant/midline oedema. Use at lowpressures and in c<strong>on</strong>juncti<strong>on</strong> with other measures. May help reduce fibrosis.12 With advanced disease and severe obstructi<strong>on</strong> pain may be exacerbated bycompressi<strong>on</strong>; balance the interventi<strong>on</strong> with the patient’s overall c<strong>on</strong>diti<strong>on</strong>.Simple lymphatic drainage or supportive bandaging often reduce the pain.13 Drug therapy:Diuretics may help if there is heart failure or hypoalbuminaemia.Steroids may shrink lymphadenopathy but can increase fluid retenti<strong>on</strong>.Antibiotics may be needed l<strong>on</strong>g term if there is recurrent infecti<strong>on</strong>. Choice ofantibiotic will be governed by local protocols.* indicates that this is best managed by specialists 46
FATIGUE / WEAKNESSDiagnosis1 Fatigue is characterised by variable physical and mental lethargy, sleepdisturbance and perceived weakness; often worse at the beginning and end ofthe day. Frequently part of anorexia/cachexia/fatigue syndrome (see p24).Fatigue is of central rather than peripheral origin.2 True weakness suggests neuromuscular disorder or cachexia.Causes / Risk factors1 Advancing cancer.2 Anorexia/cachexia/fatigue syndrome (see p24 for further informati<strong>on</strong>).3 Anaemia.4 Infecti<strong>on</strong>.5 Emoti<strong>on</strong>al distress.6 Metabolic: hyp<strong>on</strong>atraemia, hypokalaemia, uraemia, hypercalcaemia, liverimpairment, adrenal insufficiency, hyperthyroidism, hypothyroidism.7 Chemotherapy and radiotherapy.8 Corticosteroids after prol<strong>on</strong>ged use may cause profound proximal myopathy.9 Other drugs:sedatives, diuretics, antihypertensives.10 Neuromuscular damage: by tumour to brain, spinal cord or peripheral nerves,MND, myopathy, peripheral neuropathy, myasthenia gravis, Lambert-Eat<strong>on</strong>myasthenic syndrome.11 Prol<strong>on</strong>ged bed rest.Management1 Take a good history to assess functi<strong>on</strong>al interference, emoti<strong>on</strong>al state, mentalcapacity and sleep pattern.2 Examine to assess muscle wasting, specific weakness and neurologicalabnormality.3 Review drug regimen paying particular attenti<strong>on</strong> to cardiac medicati<strong>on</strong>.4 Check blood count, electrolytes, liver functi<strong>on</strong> and calcium levels and correctmetabolic disturbances where possible and appropriate.5 Provide support for emoti<strong>on</strong>al distress, hopelessness.6 Treat any depressi<strong>on</strong> as appropriate.7 Provide dietary support as appropriate.8 Help with coping and acceptance using exercise programmes, energyc<strong>on</strong>servati<strong>on</strong> techniques and advice <strong>on</strong> rest, sleep and stress reducti<strong>on</strong> – ie afatigue <strong>management</strong> programme.9 If part of anorexia/cachexia/fatigue syndrome, see also p24.10 Drug therapy: methylphenidate* 2.5 - 5mg bd may act as stimulant.47* indicates that this is best managed by specialists
ANAEMIADiagnosis1 Symptoms – tiredness, weakness, breathless <strong>on</strong> exerti<strong>on</strong>.2 Blood counts – haemoglobin, RBC indices, platelets and WBC.Causes / Risk factors1 Increased rate of RBC loss:• Bleeding– acute (anaemia may not be revealed immediately);– chr<strong>on</strong>ic (microcytic, reticulocytes, thrombocytosis).• Haemolysis – primary, sec<strong>on</strong>dary eg autoimmune process, drugs, infecti<strong>on</strong>(macrocytosis, reticulocytes, raised bilirubin).2 Reduced RBC producti<strong>on</strong>:• Chr<strong>on</strong>ic disease and renal disease (normochromic, normocytic ormicrocytic).• B<strong>on</strong>e marrow infiltrati<strong>on</strong> – leukaemia, lymphoma, carcinoma (especiallycarcinomas of prostate or breast).• Aplastic – especially drugs (including NSAIDs, antibiotics, antic<strong>on</strong>vulsants,antipsychotics, hypoglycaemics, but many drugs have been implicated).• Sideroblastic sec<strong>on</strong>dary to malignancy.• Infecti<strong>on</strong>, debility.• Deficiency of ir<strong>on</strong> (microcytic), B 12 or folate (macrocytic).Management1 Treat cause if appropriate – see Bleeding/Haemorrhage (next page), ir<strong>on</strong>, B 12or folate if deficient, review medicati<strong>on</strong> eg aspirin, NSAIDs.2 C<strong>on</strong>sider transfusi<strong>on</strong> if specific symptomatic benefit is anticipated withHb < 9.5 g/dl and not macrocytic. Transfusi<strong>on</strong> can cause heart failure indebilitated or elderly patients; use 2 - 4 units maximum per day withfurosemide cover.If the anaemia is chr<strong>on</strong>ic, patients may adapt even if Hb 8.0 g/dl. Do nottransfuse unless a specific benefit is anticipated.3 Reassess <strong>on</strong>e week after transfusi<strong>on</strong> for any symptomatic relief. If little reliefthen transfusi<strong>on</strong> need not be repeated if the haemoglobin falls again: c<strong>on</strong>siderother causes and treatments for symptoms.* indicates that this is best managed by specialists 48
BLEEDING / HAEMORRHAGECauses / Risk Factors1 Tumour invasi<strong>on</strong>.2 Platelet or coagulati<strong>on</strong> disorders, including disseminated intravascularcoagulati<strong>on</strong>, heparin-induced thrombocytopenia.3 Infecti<strong>on</strong> – eg haemoptysis, haematuria, vaginal bleed, fungating wounds.4 Drugs – heparin, warfarin, aspirin, NSAID, SSRI antidepressants.5 Peptic ulcerati<strong>on</strong>.ManagementGeneral1 Stop anticoagulants and review medicati<strong>on</strong>; c<strong>on</strong>sider reversing warfarin withfresh frozen plasma (rapid) or vitamin K 5mg iv (acts in a few hours).2 C<strong>on</strong>sider replacement of blood, platelets, clotting factors, fluids.3 Treat any infecti<strong>on</strong> which may be exacerbating bleeding.4 C<strong>on</strong>sider radiotherapy when bleeding due to malignancy, especiallyhaemoptysis, haematuria or cutaneous.5 C<strong>on</strong>sider chemotherapy and palliative surgical techniques includingendoscopic laser or cautery for tumour where feasible and appropriate.6 Embolisati<strong>on</strong> is occasi<strong>on</strong>ally used for liver and renal malignancy.7 Severe terminal haemorrhage – stay with the patient; verbal reassurance andphysical touch help.If slow, use sucti<strong>on</strong> as appropriate and c<strong>on</strong>sider iv as below.If rapid, c<strong>on</strong>sider im or iv midazolam +/– diamorphine (for relief of distress).If a terminal haemorrhage is anticipated carers can be given a supply of rectaldiazepam 10 mg. Dark towels or sheets may help to mask the blood. Relativeswho witness the event will need support.8 Drug therapy:Tranexamic acid 500mg -1.5g bd - qds orally (stabilises clots); cauti<strong>on</strong> inhaematuria as may lead to clot retenti<strong>on</strong>.Etamsylate 500mg qds orally (enhances platelet adhesi<strong>on</strong> within capillaries).Specific1 Nasal bleeding: – packing and cautery.2 Oral bleeding: – sucralfate suspensi<strong>on</strong>.3 Haemoptysis: – radiotherapy often helpful in lung tumours.4 Upper GI bleeding: – c<strong>on</strong>sider stopping any NSAIDsprot<strong>on</strong> pump inhibitors.5 Lower GI bleeding: – rectal steroidstranexamic acid oral (as above) or 0.5g in 5mlswater pr bd.6 GI tumours: – thalidomide* 100 - 400mg od.7 Skin – Kaltostat dressingtopical adrenaline 1 in 1000 to soak dressings.49* indicates that this is best managed by specialists
VENOUS THROMBOEMBOLISMDiagnosis1 Some degree of venous thromboembolic disease (VTE) is extremely comm<strong>on</strong>in patients with cancer and to a lesser extent with other advanced disease.2 Suspect pulm<strong>on</strong>ary emboli in patients with episodic and otherwiseunexplained breathlessness or c<strong>on</strong>fusi<strong>on</strong>.3 Serological tests such as D-Dimers are unhelpful in advanced cancer.4 Doppler scans will reveal DVTs in large veins.5 CT pulm<strong>on</strong>ary angiography can detect even small pulm<strong>on</strong>ary emboli.6 VQ lung scan will reveal ventilati<strong>on</strong>/perfusi<strong>on</strong> mismatches but may bedifficult to interpret in the presence of other pulm<strong>on</strong>ary pathology.Causes / Risk factors1 Malignant disease.2 Recent chemotherapy or surgery.3 Immobility.4 Pelvic disease.Management1 Assess whether patient is at risk of VTE. If so, take into account any risk ofbleeding and expected prognosis; and then discuss with the patient whetherthey wish to have active prophylaxis with anti-embolism stockings and lowmolecular weight (LMW) heparin as appropriate, balancing risks and benefitsto optimise quality of life.If the patient is in the last few days or weeks of life then thromboprophylaxisis often not appropriate, and is not routine.The best evidence in favour of thromboprophylaxis is in potentially reversibleco-existing acute c<strong>on</strong>diti<strong>on</strong>s.2 If there is symptomatic or objective evidence of VTE, c<strong>on</strong>sider formalanticoagulati<strong>on</strong> with LMW heparin, the preferred opti<strong>on</strong> because it is moreeffective in VTE associated with malignancy, is less likely to cause bleedingbut requires daily injecti<strong>on</strong>s. LMW heparin followed by warfarin is cheaper,but requires blood tests and INR may be very difficult to keep stable in thosewith advanced disease and variable nutriti<strong>on</strong>al intake.3 Regularly re-assess the patient to ensure that the current <strong>management</strong> strategyis appropriate to the stage of their illness and their wishes.* indicates that this is best managed by specialists 50
HYPERCALCAEMIAHypercalcaemia is comm<strong>on</strong> in cancers with b<strong>on</strong>e metastases (eg breast, prostate,lung) or may be due to ectopic producti<strong>on</strong> of PTH-like peptides. It occurs in 10%of cancer patients and 30% of those with myeloma. Am<strong>on</strong>gst solid tumours, it ismost comm<strong>on</strong>ly associated with squamous carcinomas and breast cancers.Diagnosis1 Corrected serum calcium > 2.7 mmol/l; symptoms usually <strong>on</strong>ly becometroublesome above 2.9 mmol/l; levels > 4 mmol/l may be fatal.2 Any combinati<strong>on</strong> of the following: nausea, c<strong>on</strong>fusi<strong>on</strong>, fatigue, loss of appetiteor emoti<strong>on</strong>al disturbances, thirst, polyuria, c<strong>on</strong>stipati<strong>on</strong> and abdominal pain.Causes / Risk factors1 B<strong>on</strong>e metastases.2 PTHrP-secreting tumours, eg carcinoma of lung.3 Dehydrati<strong>on</strong>, renal impairment.4 Tamoxifen flare.Management1 Decide if further treatment is appropriate – is this a terminal event?2 Relieve associated symptoms.3 Stop thiazide diuretics, vitamin D/calcium supplements.4 Correct dehydrati<strong>on</strong> using up to 3 litres saline iv over 24 hours.5 If serum calcium >3.0mmol/l or >2.8 still symptomatic after iv rehydrati<strong>on</strong>,use iv bisphosph<strong>on</strong>ates:pamidr<strong>on</strong>ate 90mg in 500ml saline over 2 - 4 hours (first line), orzoledr<strong>on</strong>ic acid 4mg in 50ml saline over 15 mins (most potent).(In renal impairment the above doses need adjustment – see BNF; if eGFR
USE OF STEROIDSGeneral points• Dexamethas<strong>on</strong>e is the preferred drug.• Prescribe as a single or 2 morning doses to avoid sleep disturbance.• Give a 5 - 7 day trial and stop if there is no benefit.Be clear about what objective benefit is sought, and keep under review.• Discuss potential benefits and side effects with patient and give steroid card.• If benefit achieved, reduce to lowest effective dose and then review regularly.• Stop if ineffective or when benefit lost (see below).• C<strong>on</strong>sider m<strong>on</strong>itoring plasma glucose levels.• Add gastric protective if also <strong>on</strong> NSAID or l<strong>on</strong>ger-term use.• Increase (up to double) the dose if <strong>on</strong> phenytoin or carbamazepine.Indicati<strong>on</strong>s• Brain tumour, SVCO, spinal cord compressi<strong>on</strong>:• Nerve compressi<strong>on</strong> pain, liver capsule pain,intestinal obstructi<strong>on</strong>, anti-emesis, br<strong>on</strong>chialobstructi<strong>on</strong>, lymphangitis carcinomatosa,post-radiotherapy inflammati<strong>on</strong>:• Anorexia, fatigue:Initial dose, dexamethas<strong>on</strong>e8 - 16mg4 - 8mg2 - 4mgStopping steroids• Can withdraw immediately if less than 3 weeks and < 6 mg dexamethas<strong>on</strong>e.• Otherwise tail off by 2mg every 5 - 7 days until 2mg od, then by 0.5mgevery 5 - 7 days (can substitute with betamethas<strong>on</strong>e 0.5mg tabs).• After cranial irradiati<strong>on</strong> start reducing 2 weeks after completi<strong>on</strong> of treatment,eg 16 - 12 - 8 - 6 - 4 - 2mg at intervals of 3 days; if symptoms recur, returnto previous effective dose.Comm<strong>on</strong> problems (usually related to higher or l<strong>on</strong>ger-term doses)• Early: oral thrush, hyperglycaemia, heartburn, sleep disturbance, mania.• Late: proximal myopathy, skin atrophy, change in face and body shape.Steroid equivalents (approximate)Dexamethas<strong>on</strong>e Betamethas<strong>on</strong>e Prednisol<strong>on</strong>e Hydrocortis<strong>on</strong>e2mg 2mg 15mg 50mg* indicates that this is best managed by specialists 52
DIABETES MANAGEMENTAims1 Blood sugars 7 - 15 and asymptomatic.2 No hypoglycaemia, diabetic ketoacidosis, or HONK.3 Avoid unnecessary injecti<strong>on</strong>s and testing.ManagementBlood sugar testing• On oral therapy: test 18:00 (premeal)• If starting/<strong>on</strong> steroids: test 18:00 (premeal)• If worried about fasting hypoglycaemia: test before breakfastDiet c<strong>on</strong>trolled• Blood sugars 17 +/– symptoms: start sulph<strong>on</strong>ylurea (eg gliclazide,glimepiride)On oral therapy• Stop metformin and glitaz<strong>on</strong>e therapy• Blood sugars 17: add glargine 10units 08:00 (increase by 2mg every 48h if >17)Insulin c<strong>on</strong>trolled• If eating, c<strong>on</strong>tinue usual regimen or c<strong>on</strong>tact Diabetes Team• If not eating, stop short acting insulin, c<strong>on</strong>tinue l<strong>on</strong>g acting or swap toglargine 08:00 (test 18:00), c<strong>on</strong>tacting the Diabetes TeamOn/starting steroids• Single dose steroid mane. Test blood sugars 18:00 (premeal)• If blood sugars >17, add sulph<strong>on</strong>ylurea at 12:00If still >17: start short acting insulin bd eg Humulin S/Actrapid 8 - 12unitsat 12:00 & 18:00 premeal (glargine less effective & risk of fastinghypoglycaemia)Notes• Avoid bd insulin mixtures (risk of hypoglycaemia), qds regimes (multipletests and injecti<strong>on</strong>s), bd steroids (prol<strong>on</strong>ged hyperglycaemia), bolus/prnActrapid (poor c<strong>on</strong>trol, risk of hypoglycaemia), metformin, glitaz<strong>on</strong>es.• Treat hypoglycaemia with sugar eg GlucoGel, glucag<strong>on</strong> less effective if noglycogen stores.• In the last few days of life, can allow blood sugars >17 if asymptomatic.• Communicate the above basic principles to patient, family and carers.53* indicates that this is best managed by specialists
END STAGE CONDITIONSGeneral principles1. Looking ahead (see also Advance Care Planning p65):• prognostic triggers – “Would you be surprised if this patient was to diein the next year?”, repeated hospital admissi<strong>on</strong>s, increasing dependency,specific <strong>clinical</strong> prognostic indicators (see below)• to ease the transiti<strong>on</strong> from invasive treatment to supportive care• discussi<strong>on</strong> with patient (and carer as appropriate) about theirunderstanding of severity of disease and likely prognosis, preferences forfuture care and treatment, and what to do or where to go in a crisis:“Thinking ahead – what sort of future care would you want?”“What would you like to happen or not to happen?”2. Assessment of patient’s and carers’ needs for physical, psychological/emoti<strong>on</strong>al, social/financial and spiritual support (see p60).3. Symptom c<strong>on</strong>trol, for restorati<strong>on</strong> or maintenance of dignity/quality of life• optimisati<strong>on</strong> of medical <strong>management</strong> of c<strong>on</strong>diti<strong>on</strong>, treatable causes ofdeteriorati<strong>on</strong> and iatrogenic problems• disease-specific symptom palliati<strong>on</strong> (see below).4. Informati<strong>on</strong> exchange – ensure that the above informati<strong>on</strong>/choices arecommunicated to the relevant hospital team, GP, community team and supportservices etc as appropriate.5. Triggers for Specialist Palliative Care referral:• poorly c<strong>on</strong>trolled symptoms• complex needs or problems that require additi<strong>on</strong>al help• help required with issues brought up in 1 and 2 above• preferred place of terminal care is a hospice.End stage heart failureSpecific <strong>clinical</strong> prognostic indicators:Heart failure NYHA Stage III or IV, ejecti<strong>on</strong> fracti<strong>on</strong> ≤ 20%, albumin
• Nausea – avoid cyclizine as may exacerbate heart failure• Pain – cauti<strong>on</strong> with NSAIDs and steroids because of fluid retenti<strong>on</strong>• C<strong>on</strong>stipati<strong>on</strong> – magnesium hydroxide and lactulose less effective• Care of the Dying – stop warfarin, statins etc; switch off ImplantableDefibrillator.End stage kidney failureSpecific <strong>clinical</strong> prognostic indicators:eGFR
SYRINGE DRIVERSA syringe driver is a small portable battery-powered pump which administersdrugs subcutaneously by c<strong>on</strong>tinuous infusi<strong>on</strong>. It offers an alternative mode androute of drug administrati<strong>on</strong> with little impact <strong>on</strong> patient mobility orindependence. By maintaining steady plasma levels a syringe driver mayimprove symptom c<strong>on</strong>trol.Indicati<strong>on</strong>sFor administering medicati<strong>on</strong> when the oral route is difficult or inappropriate.If/when problems resolve, c<strong>on</strong>sider a return to oral medicati<strong>on</strong>.1 Severe vomiting and/or nausea.2 Dysphagia.3 Severe oral tumours, sores, or infecti<strong>on</strong>.4 Profoundly weak, unc<strong>on</strong>scious, or sedated patient.5 Poor absorpti<strong>on</strong> of orally administered medicati<strong>on</strong>.Practical points1 Syringe drivers in current use are the McKinley, the Graseby MS26 andMS16. The McKinley automatically calculates the rate (mm/hr) and thevolume remaining (ml) from the type and size of syringe. For the MS26 andMS16 the rate of infusi<strong>on</strong> has to be set manually: in mm/24hrs for the GrasebyMS26 and in mm/hr for the Graseby MS16.2 The line should be primed before calculati<strong>on</strong> or measuring length.3 Use a Luerlock syringe in syringe drivers. A 20ml syringe allows greaterdiluti<strong>on</strong> and less risk of precipitati<strong>on</strong>. For the MS16 driver, the syringe shouldbe filled to a length of 48mm.4 Label the syringe with the patient’s name, drug(s) and dose(s), nature ofdiluent and the date and time commenced.5 The syringe driver and inserti<strong>on</strong> site must be checked at least <strong>on</strong>ce a day, andpreferably every 4 hours in the hospital setting.6 The boost butt<strong>on</strong> should not be used to administer breakthrough medicati<strong>on</strong>.7 Use as few drugs in the syringe driver as possible (usually maximum of 3).8 Site inflammati<strong>on</strong> may occur as a result of irritant soluti<strong>on</strong>s or hypersensitivityto the metal cannula. Management strategies include changing the drug, thediluent, the site or the giving set (from a metal butterfly to a plastic cannula).If problems persist, seek specialist advice.9 Certain drug combinati<strong>on</strong>s may cause precipitati<strong>on</strong> within the syringe. Thismay sometimes be overcome by the following strategies, but do not assumethat lack of precipitati<strong>on</strong> necessarily implies compatibility:• using a larger syringe to allow greater diluti<strong>on</strong>• using water rather than saline for diluti<strong>on</strong>, or vice versa• separating drugs into two syringe drivers• drawing up dexamethas<strong>on</strong>e last when used in combinati<strong>on</strong>• substituting drugs with an equivalent alternative• avoiding exposure to sunlight as n<strong>on</strong>-observable reacti<strong>on</strong>s may occur.* indicates that this is best managed by specialists 56
Drugs often used in the syringe driver• All doses given are per 24 hours.• Water or normal saline may be used as diluents. We usually recommendwater, but saline is essential for diclofenac/NSAIDs.• Not all drug combinati<strong>on</strong>s are compatible: check with local Palliative CareTeam, pharmacy or the Palliative Care Formulary, www.pallcare.info (see p3).• Do not use diazepam, prochlorperazine or chlorpromazine – all irritant.Cyclizine100 - 150mgAntihistamine and antimuscarinic antiemetic which acts at the vomitingcentre. Often causes site irritati<strong>on</strong>. Limited compatibility.Dexamethas<strong>on</strong>e Up to 16mgUsed to relieve raised intracranial pressure, liver capsule and neuropathic pain,and as antiemetic. May precipitate when higher doses mixed with other drugs.Diamorphine 5 - 100mg (or higher*) for use see pp7-12More soluble (more expensive) than morphine (equivalence see p10).Diclofenac75 - 150mgUse saline as diluent. Does not mix with other drugs.Glycopyrr<strong>on</strong>ium 200mcg - 1.2mgUsed to reduce respiratory secreti<strong>on</strong>s if sedati<strong>on</strong> is undesirable.Haloperidol2.5 - 10mgAntidopaminergic antiemetic (see p19). Higher doses occasi<strong>on</strong>ally used inc<strong>on</strong>fusi<strong>on</strong> (see p41). Extrapyramidal side-effects may occur with high doses.Hyoscine butylbromide 20 - 120mg (- 240mg*)Anti-spasmodic used to relieve intestinal colic. Useful for drying secreti<strong>on</strong>sand in intestinal obstructi<strong>on</strong> through its antisecretory effect.Hyoscine hydrobromide 400mcg - 2.4mgUseful for reducing secreti<strong>on</strong>s; some smooth muscle antispasmodic activity.Can be sedative, may cause agitati<strong>on</strong> or c<strong>on</strong>fusi<strong>on</strong> (eg in elderly).Levomepromazine 5 - 25mg (antiemetic, see p19)25 - 100mg (sedative, see p41)Metoclopramide 30 - 80mgAntiemetic (see pp19, 21). Extrapyramidal effects may occur at higher doses.Midazolam5 - 60mgBenzodiazepine: sedative, antiepileptic. May be useful in neuropathic pain.Higher doses are <strong>on</strong>ly appropriate for terminal sedati<strong>on</strong>.Morphine5 - 300mg, for use see pp7-12Specialist palliative care referral recommended at the top end of dose range.Octreotide*300 - 800mcgUsed in intestinal obstructi<strong>on</strong> (see p21), and for fistulae (see p26). Expensive.Oxycod<strong>on</strong>e5 - 200mgAlternative to morphine and diamorphine (equivalence see p10).Other drugs are occasi<strong>on</strong>ally used eg alfentanil, cl<strong>on</strong>azepam, fentanyl,furosemide, ketorolac, <strong>on</strong>dansetr<strong>on</strong>, phenobarbital.57* indicates that this is best managed by specialists
<str<strong>on</strong>g>THE</str<strong>on</strong>g> LAST FEW DAYS OF LIFEPrinciples• Adopt a problem solving approach to symptom c<strong>on</strong>trol.• Review all drugs and keep <strong>on</strong>ly the essentials.• Anticipatory prescribing (see below).• Avoid all unnecessary interventi<strong>on</strong>s eg iv infusi<strong>on</strong>s.• Ensure effective communicati<strong>on</strong> am<strong>on</strong>gst all involved• Ensure practical and emoti<strong>on</strong>al support offered to family and carers• Check religious and cultural needs.Many will use a Liverpool Care Pathway or equivalent to facilitate theseprinciples.Management• Anticipate:Availability of drugs and equipment for treatment of pain, breathlessness,nausea and vomiting, c<strong>on</strong>fusi<strong>on</strong>, haemorrhage, terminal restlessness,urinary retenti<strong>on</strong>, diabetes <strong>management</strong>, mouth and skin care.Family distress and fears.Practical care requirements.• Analgesics• Antiemetics• Anxiolytics• Antisecretories• Administrati<strong>on</strong> route.This will require the use of Anticipatory Prescribing or Just In Case boxes (in thehome) for drugs and their route of administrati<strong>on</strong>.Guidance <strong>on</strong> Medicati<strong>on</strong> for Symptom C<strong>on</strong>trolPainOpioids and NSAIDs are the main analgesics.C<strong>on</strong>versi<strong>on</strong> from oral opioids to csci morphine or diamorphine is often needed:eg morphine po 3mg = 1.5mg morphine sc = 1mg diamorphine sc (see pp8-10).Prn doses of morphine (po, sc) or diamorphine (sc) should be up to 1/6th totaldaily opioid dose or 2.5 - 5mg in the opioid naïve (see p10).If <strong>on</strong> fentanyl or buprenorphine patch, keep the patch and if further analgesiarequired add opioid to syringe driver (eg fentanyl 25mcg/hr patch roughlyequivalent to csci morphine 30mg or diamorphine 20mg per 24hrs). Prn doses ofsc morphine or diamorphine are suggested <strong>on</strong> p11.* indicates that this is best managed by specialists 58
Stiffness, general aches and pains often develop with immobility – NSAID egdiclofenac po, pr or via csci often helpful, or midazolam 5 - 10mg/24h via csci.Nausea and VomitingUsually less of a problem, unless there is intestinal obstructi<strong>on</strong> (see p20).Available antiemetics should be:Metoclopramide or haloperidol and cyclizine or levomepromazine (see p19).Prn doses (po or sc): metoclopramide 10mg, haloperidol 0.5 - 1.5mg, cyclizine50mg, levomepromazine 5 - 6.25mg.Csci doses (per 24hrs): metoclopramide 30mg - 60mg, haloperidol 2.5 - 5mg,cyclizine 100 - 150mg, levomepromazine 5 - 25mg.Rarely, a nasogastric tube will be required in intestinal obstructi<strong>on</strong>.Terminal Restlessness (see also p42)Usual drugs are midazolam 2.5 - 10mg sc prn or 10 - 60mg per 24hrs via csciand/or levomepromazine 12.5 - 25mg sc prn or 25 - 150mg per 24hrs via csci.Alternatively, diazepam can be given orally 2 - 10mg or rectally 5 - 10mg.Excess/Rattling Upper Airway Secreti<strong>on</strong>sUsual drugs to be made available are hyoscine butylbromide 20mg sc prn or40 - 80mg per 24hrs via csci (also useful for colic and intestinal obstructi<strong>on</strong>) orhyoscine hydrobromide 400mcg sc prn or via csci (see p57) or glycopyrr<strong>on</strong>iumvia csci (see p57).Administrati<strong>on</strong> RouteAlternatives to the oral route are often needed. Usually drugs can be givenrectally or subcutaneously. Syringe drivers have the advantage of givingc<strong>on</strong>tinuous c<strong>on</strong>trol of symptoms and are to be preferred to multiple subcutaneousinjecti<strong>on</strong>s (see p56).Planning for the Death• To avoid inappropriate resuscitati<strong>on</strong> attempts particularly at home, checkthat this patient’s DNACPR status is known or recorded for visiting healthprofessi<strong>on</strong>als (see p64)• If the diagnosis is mesothelioma, asbestosis or other industrial disease,remember to warn the family that the Cor<strong>on</strong>er’s team will become involvedafter death• Check whether cultural or religious rituals are expected to be adhered toafter death• Provide informati<strong>on</strong> and/or c<strong>on</strong>tact numbers about procedures immediatelyafter death.59* indicates that this is best managed by specialists
PSYCHOLOGICAL, SPIRITUAL AND SOCIAL <str<strong>on</strong>g>CARE</str<strong>on</strong>g>The primary task when faced with spiritual questi<strong>on</strong>s is to help the pers<strong>on</strong>towards some resoluti<strong>on</strong>. Palliative care extends far bey<strong>on</strong>d pain relief and thealleviati<strong>on</strong> of symptoms. Psychological, spiritual and social needs of bothpatient and their family/carers should be addressed. This does not necessarilyrequire specialist help – all health professi<strong>on</strong>als should be prepared to makeinitial assessments and identify these issues.This holistic assessment is important in ensuring that the patient and family haveoptimal support in any care setting. It also ensures that discharge planning iseffective (hospital/hospice staff should check that these plans are acceptable tothe patient, family, carers and Primary Health Care Team).The framework for needs assessment should include:• Psychological needs• Spiritual issues• Social needs• Informati<strong>on</strong> needs• Carers’ needs.Many factors influence the way in which patients and families cope with theirillness and the following need to be c<strong>on</strong>sidered during an assessment:• The history of the illness and their understanding of what is happening,including their emoti<strong>on</strong>al and psychological resp<strong>on</strong>se• How the illness is affecting the pers<strong>on</strong>’s ability to carry out their role, forexample as parent, mother, lover, breadwinner etc• Family history – who is around, where are they, how important are they,how supportive are they? C<strong>on</strong>structing a family tree (genogram) is oftenhelpful both for establishing relati<strong>on</strong>ships and for use as a therapeutic toolin helping people talk about their issues• Life stresses – what is happening with regard to m<strong>on</strong>ey, jobs, housing,children, sources of support etc• Hopes and fears – what is the worst thing that can happen, what are theplans for the future, what losses and disappointments have occurred, whatunfinished business is there, and what do they still wish to accomplish?During assessment it should become apparent whether further expert professi<strong>on</strong>alhelp is required for psychological, spiritual and social care. Those available willinclude specialist palliative care staff, <strong>clinical</strong> psychologists, chaplain/spiritualadvisors, and adult and child social workers.* indicates that this is best managed by specialists 60
CULTUREIn our society there is a wide variety of people of different faiths, ethnicbackgrounds and countries of origin. Within these groups, each individual willexpress their cultural attitudes uniquely, as they are influenced by upbringing,background, envir<strong>on</strong>ment, beliefs and life experience.Cultural attitudes can particularly influence:• Language and the use of colloquialisms• The roles of the family• How symptoms or illness are described and understood• Ethical issues, including aut<strong>on</strong>omy and c<strong>on</strong>fidentiality• Attitudes towards c<strong>on</strong>venti<strong>on</strong>al Western therapies, complementary oralternative therapies, food and diet• Attitudes towards death and dying• Rituals surrounding death (see 3. below)• Preferred place of care – home, care home, hospital or hospice• Acceptance of help and support.Health professi<strong>on</strong>als should show their awareness by:• Ensuring that appropriate language interpretati<strong>on</strong> services are used• Dem<strong>on</strong>strating willingness to listen and a wish to understand culturaldifferences and implicati<strong>on</strong>s• Meeting specific requirements (such as food, privacy, opportunity topractice religious observances etc) wherever possible• Being prepared to negotiate boundaries and details of care• Ensuring that there is access to an appropriate religious advisor.Do not make assumpti<strong>on</strong>s – ASKRemember that each pers<strong>on</strong> is unique, regardless of cultural background andprofessed faith.Further reading1. Neuberger J. Care for Dying People of Different Faiths. Oxford: RadcliffeMedical Press, 2004.2. Henley Q, Schott J. Culture, Religi<strong>on</strong> and Patient Care in a MultiethnicSociety. Age C<strong>on</strong>cern Books, 1999.3. Multi-Faith Practices. In Standards for Spiritual Care (NHS Wales) 2009:Supporting Guidance p29. www.wales.nhs.uk/sites3/Documents61* indicates that this is best managed by specialists
BREAKING BAD NEWSBad news is any informati<strong>on</strong> which alters a patient’s view of their future for theworse – the bigger the gap between expectati<strong>on</strong> and reality the worse the news.Giving bad news means entering a therapeutic dialogue of listening andresp<strong>on</strong>ding which will affect how patients and families will cope. The aim is to:• maintain trust between patient, family/carer and health professi<strong>on</strong>als• enable appropriate adjustment to the reality of the situati<strong>on</strong>• encourage informed choice of <strong>management</strong> opti<strong>on</strong>s• reduce uncertainty about the future or at least acknowledge it• enable patients to regain a feeling of some c<strong>on</strong>trol over their situati<strong>on</strong>.The following framework describes <strong>on</strong>e approach.1. Preparati<strong>on</strong>• Know the facts and the potential <strong>management</strong> plan• Arrange for privacy, sufficient seating and avoidance of interrupti<strong>on</strong>s• Whenever possible offer the patient the chance to have a close familymember or friend present2. Assess understanding (may need repeating as further informati<strong>on</strong> given)• “What do you understand about your illness/what is happening?”3. Check if more informati<strong>on</strong> is wanted and at what level• “Do you want to go <strong>on</strong> or is that enough for now?”• Again, this may need to be repeated as you give further informati<strong>on</strong>4. Allow denial• Allow the patient to c<strong>on</strong>trol the pace of informati<strong>on</strong> flow, and to whom theinformati<strong>on</strong> should be given5. Sharing the informati<strong>on</strong>• Start from where the patient is, give warning shots and further informati<strong>on</strong>in small chunks. Know when to stop.• Be clear and simple, avoiding jarg<strong>on</strong>, and above all be gentle• Avoid assumpti<strong>on</strong>s about their understanding i.e. check that they haveheard what you believe you have said6. Elicit c<strong>on</strong>cerns• What is worrying the patient most?7. Resp<strong>on</strong>d to the patient’s feelings• Identify the patient’s feelings and acknowledge them• Listen for and observe the emoti<strong>on</strong>al c<strong>on</strong>tent and behaviour• Allow them time to think through the situati<strong>on</strong> and ask questi<strong>on</strong>s:“Is there anything else you’d like to say or ask me?”.* indicates that this is best managed by specialists 62
8. Summary and plan• Summarise what has been said, emphasising the positive• Outline future treatment if appropriate, using written or printed material ifpossible• Foster realistic hope, eg “We may not be able to cure you but there arethings we can do to make you feel better and cope with your illness”• Recheck their understanding9. Make arrangements for further c<strong>on</strong>tact• Ask who may be told about the diagnosis/informati<strong>on</strong>10. Ensure others are informed of what was said• Tell the General Practiti<strong>on</strong>er and other staff <strong>on</strong> duty as so<strong>on</strong> as possible• Record as exactly as possible what was said, so that it can be repeated laterand to avoid misunderstanding• Giving the patient a recording of the interview is popular and effective.Remember• Make sure the patient feels the centre of attenti<strong>on</strong>• Much of what you communicate is by n<strong>on</strong>-verbal means and behaviour• Move at the patient’s pace, giving informati<strong>on</strong> that is appropriate for thattime• If using euphemisms, try to find out what they understand by these words.• Express your humanity and warmth, and interest in their care• Breaking bad news does not have to be d<strong>on</strong>e at <strong>on</strong>e sessi<strong>on</strong>, it is often bestd<strong>on</strong>e in stages• Do not be afraid of them expressing negative feelings or crying.• Be prepared for an initial stunned silence or anger• Ensure that you are answering the questi<strong>on</strong> that you are being asked• Avoid jarg<strong>on</strong>• Do not tell lies• Some direct questi<strong>on</strong>s are best answered initially by asking “What makesyou ask that?”. This may enable them to explain the worry behind thequesti<strong>on</strong>.• It is a breach of c<strong>on</strong>fidentiality to tell relatives without the patient’sc<strong>on</strong>sent, where the patient has the capacity to agree to or refuse disclosure.Further readingBuckman R and Kas<strong>on</strong> Y (1992) How to Break Bad News: A Guide forHealthcare Professi<strong>on</strong>als, Papermac.Peter Kaye (1996) Breaking Bad News a Ten Step Approach: EPL Publicati<strong>on</strong>s.63* indicates that this is best managed by specialists
DNACPR DISCUSSIONSA DNACPR (also called DNAR or ‘Allow a Natural Death’) order can be part ofan advance decisi<strong>on</strong> made by the patient, but is more comm<strong>on</strong>ly made when thepatient is becoming more ill. Problems may arise because:• policy documents do not distinguish between an expected death and cardiopulm<strong>on</strong>aryarrest• the general public have unrealistic expectati<strong>on</strong>s of CPR’s success rate• there is a lack of understanding of how CPR can lead to adverse outcomes,even where the restorati<strong>on</strong> of cardiac output is successful• there is a misc<strong>on</strong>cepti<strong>on</strong> that there is a requirement to discuss the decisi<strong>on</strong>with patient and/or carers• there is a misc<strong>on</strong>cepti<strong>on</strong> that patients can choose whether or not they willbe resuscitated• it is a well established principle that doctors (and other healthprofessi<strong>on</strong>als) should not offer treatments which they c<strong>on</strong>sider to be futile.The following framework is suggested to overcome these difficulties:• recognise that while discussi<strong>on</strong> is best practice, it is not mandatory, andindeed should not be undertaken if it might cause harm• do not withhold informati<strong>on</strong> just because it is difficult to c<strong>on</strong>vey• discuss what care will be given, rather than what will not be d<strong>on</strong>e;emphasise (and ensure) that a DNAR decisi<strong>on</strong> <strong>on</strong>ly relates to CPR and doesnot involve withholding other appropriate treatments• emphasise that any decisi<strong>on</strong> is based <strong>on</strong> <strong>clinical</strong> judgement, not <strong>on</strong> age or‘worth’ of the patient’s life• c<strong>on</strong>sider framing any discussi<strong>on</strong> with a patient and/or their carers aroundthe fact that the illness is progressing and death will naturally happen,rather than specifically around CPR• can point out that if death occurs (heart stops) then family can stay withpatient, allowing a dignified death, rather than having to leave while CPRattempted (and unlikely to work)• be aware that discussing CPR might imply that you believe that it could besuccessful; if appropriate, explain the likely adverse outcomes of CPR• if necessary, negotiate a limited range of resuscitative interventi<strong>on</strong>s whichmay be carried out in the event of sudden collapse.Further readingBMA/Resuscitati<strong>on</strong> Council Guideline: www.resus.org.uk/pages/dnar* indicates that this is best managed by specialists 64
ADVANCE <str<strong>on</strong>g>CARE</str<strong>on</strong>g> PLANNINGAdvance Care Planning (ACP) is the process of discussi<strong>on</strong>s between anindividual and their health care professi<strong>on</strong>al about future needs. Helping apatient establish their priorities in End of Life Care enables them to plan theirfuture and prepare for death, allowing them to maintain c<strong>on</strong>trol over their wishesand preferences should they later lose mental capacity.These preferences should be communicated to all professi<strong>on</strong>als involved anddocumented appropriately (with the patient’s c<strong>on</strong>sent). It is usually helpful toencourage the patient to include family/carers in these discussi<strong>on</strong>s.ACP takes place in anticipati<strong>on</strong> (preferably) or in recogniti<strong>on</strong> of deteriorati<strong>on</strong> inc<strong>on</strong>diti<strong>on</strong>. Triggers for ACP include:• enquiry by the patient, or from care needs assessment• the Surprise Questi<strong>on</strong>: “Would I be surprised if this patient was to die inthe next year?”• <strong>clinical</strong> prompts eg repeated hospital admissi<strong>on</strong>s, shift in treatmentfocus, loss of functi<strong>on</strong>, care home admissi<strong>on</strong>.The healthcare professi<strong>on</strong>al needs to:• have sensitivity about when and how to instigate discussi<strong>on</strong>• recognise when to stop• have knowledge of likely disease events, treatment opti<strong>on</strong>s and localresources/services available• communicate them effectively.Judgement must be used as to whether ACP is likely to provide overall benefit tothe individual at that time, and no pressure should be applied to take part in ACP.Initiati<strong>on</strong> of discussi<strong>on</strong> can be aided by introducing the leaflet “Planning for yourFuture Care – A Guide” (www.endoflifecareforadults.nhs.uk).ACP discussi<strong>on</strong>s include exploring patient and carers’ insight into disease, futureexpectati<strong>on</strong>s, and future plans/choices for treatments and place of care etc.ACP spans a spectrum from open c<strong>on</strong>versati<strong>on</strong>s to formal, legally bindingdocuments. Outcomes therefore may be:• ‘no wish to discuss further at this time’• a statement of wishes and preferences• DNACPR decisi<strong>on</strong> (see previous page)• making an Advance Decisi<strong>on</strong> to Refuse Treatment• registering a Lasting Power of Attorney.Challenges – family c<strong>on</strong>flict or exclusi<strong>on</strong>, lack of support for potentialc<strong>on</strong>sequences of discussi<strong>on</strong>, denial or collusi<strong>on</strong> etc.The patient’s permissi<strong>on</strong> is required for recording the discussi<strong>on</strong>s and sharing theinformati<strong>on</strong>/documentati<strong>on</strong> with healthcare teams (and, in the future, an End ofLife Care Register) or the family.All ACP should be regularly reviewed to check that it still accords withpreferences as wishes often change with worsening c<strong>on</strong>diti<strong>on</strong>.65* indicates that this is best managed by specialists
DEALING WITH DENIAL AND COLLUSIONDenialDenial is a basic coping mechanism that allows us to c<strong>on</strong>tinue to functi<strong>on</strong> whenfaced with informati<strong>on</strong> or events with which we cannot cope. It may be practisedby the patient, family or professi<strong>on</strong>als. Denial is not necessarily unhealthy andcan be normal, as in the first stage of accepting bad news. However, if taken toextremes or creating situati<strong>on</strong>s that are harmful, such as preventing appropriatetreatment, adequate symptom c<strong>on</strong>trol or future planning for dependents, it maybe appropriate to explore the denial.Assessment• Is it healthy or unhealthy? That is, is it reducing or increasing distress?• Is there an appropriate reas<strong>on</strong> for challenging the denial?• Is it really denial? Many people have a good understanding of the situati<strong>on</strong>but do not wish to talk about it.• Is other health professi<strong>on</strong>als’ denial c<strong>on</strong>tributing?Management1. Gently explore what the pers<strong>on</strong> understands of what they have been told.2. Using the framework outlined in Breaking Bad News (see p62), gently movethe pers<strong>on</strong> towards a better understanding of reality, particularly with regardfor the particular need identified for challenging the denial. It is often helpfulto use such phrases as “What if?” or “Let’s look at the worst scenario even if itmay not happen”.3. Be prepared to modify denial in stages and as far as possible at the patient’space; and accept that it is unrealistic to expect all patients to come to termswith their mortality.4. Ensure that extra support is available following the challenging of denial.5. Support family or carers who may be finding the patient’s denial stressful.6. Alert other health professi<strong>on</strong>als involved of any changes in the patient’sunderstanding.* indicates that this is best managed by specialists 66
Collusi<strong>on</strong>Collusi<strong>on</strong> usually occurs when the family c<strong>on</strong>spire am<strong>on</strong>g themselves or withprofessi<strong>on</strong>als to withhold informati<strong>on</strong> from or lie to the patient. It is often wellintenti<strong>on</strong>ed, acting in what is believed to be the best interests of the patient.However, this inevitably creates tensi<strong>on</strong> because, ethically and legally, thepatient has the right to informati<strong>on</strong> and to authorise disclosure of informati<strong>on</strong> tothe family.Management1. Explore the family’s understanding and reas<strong>on</strong>ing:• establish whether they are trying to protect themselves or the patient• recognise that they may have valid c<strong>on</strong>cerns about the patient’s capabilitiesand past behaviour patterns• show understanding of their situati<strong>on</strong>.2. Reassurance and explanati<strong>on</strong>:• reassure that you will not walk in and impose informati<strong>on</strong>• explain that the patient has a right to informati<strong>on</strong>, if requested, and h<strong>on</strong>estyis an important part of maintaining trust in a doctor-patient relati<strong>on</strong>ship• explain the stressful c<strong>on</strong>sequences of living out an ever increasing lie• explain that if the patient asks direct questi<strong>on</strong>s, their understanding andwishes will be explored before answering the questi<strong>on</strong> appropriately andsensitively• offer to facilitate a joint c<strong>on</strong>versati<strong>on</strong> between the family and patient if theyare finding it too difficult.3. Gently explore the patient’s understanding, and assess their desire for furtherinformati<strong>on</strong>. Pass this <strong>on</strong> to the family, with the patient’s c<strong>on</strong>sent, to enablemore open communicati<strong>on</strong>.Occasi<strong>on</strong>ally patients collude with professi<strong>on</strong>als to withhold informati<strong>on</strong> fromtheir family. This is more difficult as the patient has to give permissi<strong>on</strong> fordisclosure of informati<strong>on</strong>, but the principles are the same as above – explorati<strong>on</strong>of reas<strong>on</strong>ing; explanati<strong>on</strong> about c<strong>on</strong>sequences; reassurance of sensitive handling;and offer of facilitati<strong>on</strong>.67* indicates that this is best managed by specialists
SPIRITUAL <str<strong>on</strong>g>CARE</str<strong>on</strong>g>Introducti<strong>on</strong>Spiritual care is <strong>on</strong>e of the central aspects of palliative care. It is difficult todefine, but any problem, c<strong>on</strong>versati<strong>on</strong> or c<strong>on</strong>tact may c<strong>on</strong>tain spiritual as well asphysical, psychological or social issues. Spirituality is to do with how we live,what we treasure and value, and peace of mind. Spirituality is relati<strong>on</strong>al in itsexpressi<strong>on</strong>, i.e. feeling a need to c<strong>on</strong>nect with some<strong>on</strong>e or something. Allpatients have spiritual needs while <strong>on</strong>ly some will have religious needs.Spiritual distressWhen a pers<strong>on</strong> experiences a life crisis they will look to their spiritual values,beliefs, attitudes or religious practices to make sense of it. If these do not enablethem to cope with the crisis, then they may experience spiritual distress.Expressi<strong>on</strong>s of spiritual distress include:• fear about the future, about dying and what happens after death• loss of identity or roles (parenthood, work etc)• helplessness and loss of c<strong>on</strong>trol over what is happening• anxiety about relati<strong>on</strong>ships, body image or sexuality• suffering excessively from physical symptoms, especially pain• anger• guilt or shame• hopelessness, despair, feeling al<strong>on</strong>e or unloved• explorati<strong>on</strong> of meaning and purpose of their life• breaking with religious or cultural ties.Dealing with spiritual distressThe primary task when faced with spiritual questi<strong>on</strong>s is to help the pers<strong>on</strong>towards some resoluti<strong>on</strong> and understanding. Accept that there is unlikely to be aspecific answer – it's OK not to know.Listen attentively and be prepared to face uncertainties – just by “being there”you can help the patient to make c<strong>on</strong>necti<strong>on</strong>s and embark <strong>on</strong> their own search formeaning.Do not be afraid to ask simple questi<strong>on</strong>s about their fears, losses, feelings, “thefuture”, sense of c<strong>on</strong>trol, past regrets, values, beliefs and religious needs. Offer aparticular group or pers<strong>on</strong> such as a chaplain if you feel out of your depth orthere is a requirement for a religious input.* indicates that this is best managed by specialists 68
Basic principles1. Provide a safe caring envir<strong>on</strong>ment.• Good symptom c<strong>on</strong>trol• Show willingness to listen• Value their role and appearance, and belief systems2. Attend to:• Signs of their wishing to explore spiritual issuesAsk yourself “Why am I being told this? And why now?”• Your own verbal and n<strong>on</strong>-verbal behaviour and reacti<strong>on</strong>s (patients can bereluctant to embarrass professi<strong>on</strong>als if they sense that they are causingdiscomfort)3. Listen to:• Questi<strong>on</strong>s• Expressi<strong>on</strong>s of fear, anger, loss etc• Their story4. Assess in terms of :• Past, present and future. Ask simple questi<strong>on</strong>s as outlined above.• What help is needed5. Reassure and help with:• Good physical care in illness and dying• Respect for their integrity, worth and values• Informati<strong>on</strong> as requested• “Unfinished business”• Pers<strong>on</strong>al support – “being al<strong>on</strong>gside”• Care for family and carers• Reviewing of life• Arranging provisi<strong>on</strong> of spiritual counselling if needed eg to help facemortality• Arranging provisi<strong>on</strong> of religious and sacramental care, according to faithAbove all – be there.6. Attend to yourself:• Facing intense feelings or distress can leave us feeling uncomfortable,inadequate, helpless or vulnerable. The task is to live with our ownuncertainties. It is therefore important to explore difficult issues or sharec<strong>on</strong>cerns with colleagues, eg through individual or group supervisi<strong>on</strong>.Further readingSpeck P. Being there: pastoral care in times of illness. L<strong>on</strong>d<strong>on</strong>: SPCK, 1988.Stanworth R. Recognising the spiritual needs in people who are dying. Oxford:OUP, 2004.69* indicates that this is best managed by specialists
BEREAVEMENTGrief is a natural process experienced by any<strong>on</strong>e who has to adjust to asignificant loss. An appreciati<strong>on</strong> of what is 'normal' is required in order torecognise when and what type of interventi<strong>on</strong> is needed. Parkes describesbereavement in terms of phases of grief:1 Initial shock, numbness and disbelief before emoti<strong>on</strong>al reality of the loss isfelt. Seeing the body after death, attending the funeral or visiting the grave areoften important in facilitating acceptance of the reality of the death.2 The pain of separati<strong>on</strong> which affects behaviour and emoti<strong>on</strong>s. The bereavedusually suffer overwhelming periods of sadness as they are faced with the dayto-dayreality of their loss. They may try to reduce this by avoiding remindersof the deceased. They may also find themselves ‘searching’ for the bereaved,dreaming about them or actually seeing or hearing them. Visual or auditoryhallucinati<strong>on</strong>s at this time are normal. Agitati<strong>on</strong>, restlessness and an inabilityto c<strong>on</strong>centrate can result from the c<strong>on</strong>flict between this searching and avoidingbehaviour – attempts to avoid the reality of the situati<strong>on</strong>.A range of emoti<strong>on</strong>s other than sadness may be experienced. Anxiety may bedue to loss of the familiar routine and feelings of insecurity. Anger may bedirected towards the deceased for aband<strong>on</strong>ing them, towards God, or (justly orunjustly) towards professi<strong>on</strong>als. It may simply manifest as general irritability.Feelings of guilt may occur when anger is directed internally.It is comm<strong>on</strong> for physical symptoms related to over-activity of the aut<strong>on</strong>omicnervous system to be experienced, eg palpitati<strong>on</strong>s, insomnia, diarrhoea andfatigue. A transient hypoch<strong>on</strong>driasis can occur, but it is abnormal if it persists.3 Despair or depressi<strong>on</strong>. As the pangs of grief and anxiety reduce in frequencyand severity the bereaved may lose interest and purpose in life. They feelhopeless and become withdrawn. This may last for m<strong>on</strong>ths.4 Eventually the loss is accepted and life without the deceased is adjusted to.5 The final phase of resoluti<strong>on</strong> and reorganisati<strong>on</strong> is entered as emoti<strong>on</strong>alenergy is reinvested in new relati<strong>on</strong>ships and activities, although anniversariesoften trigger renewed grief.For some, part of the work of grieving may be underg<strong>on</strong>e before the actualdeath of the deceased (anticipatory grieving). Although described insequence, bereavement reacti<strong>on</strong>s usually oscillate between phases.* indicates that this is best managed by specialists 70
For most people, no formal psychotherapeutic interventi<strong>on</strong> is needed as theirpers<strong>on</strong>ality, previous life experiences, social network and loving relati<strong>on</strong>shipwith the bereaved enables them to come to terms with their loss, and often togrow pers<strong>on</strong>ally through it. All that is often required is a watchful eye tocheck that their grief is c<strong>on</strong>tinuing normally.6 For those with unresolved/abnormal grief further interventi<strong>on</strong> is required.The needs of children and adolescents are often quite complex and they mayalso benefit from specialist support. Recogniti<strong>on</strong> of those likely to develop anabnormal grief reacti<strong>on</strong> can also allow early supportive interventi<strong>on</strong> andprevent its development. Risk factors include:• an unexpected/untimely death• an unpleasant death• an ambivalent relati<strong>on</strong>ship• an excessively dependent relati<strong>on</strong>ship• a child/adolescent (may be protected/excluded)• social isolati<strong>on</strong>• excessive use of denial, preventing anticipatory grieving• unresolved anger• previously unresolved losses• previous psychiatric illness• a history of alcoholism/drug abuse• other c<strong>on</strong>current stressful life events.For many, a trained volunteer who listens may address the need of thebereaved to recognise and express their feelings and fears, enabling them tomake sense for themselves of the events which have occurred. Reassurancethat what they are experiencing is 'normal' is extremely helpful. A chaplainmay also be helpful to those whose faith is shaken, destroyed or awakened.Some find meeting with a group of individuals who have underg<strong>on</strong>e a similarexperience can be supportive. These groups may or may not have a trainedfacilitator.Written informati<strong>on</strong> explaining what may be experienced and giving usefulc<strong>on</strong>tact numbers is often appreciated.71* indicates that this is best managed by specialists
UNRESOLVED/ABNORMAL GRIEFThere is no clear boundary between what is 'normal' and what is 'abnormal' grief,and it is often a questi<strong>on</strong> of unusual intensity, of reacti<strong>on</strong> or timing. Thefollowing guide indicates when professi<strong>on</strong>al interventi<strong>on</strong> may be required.1 Delayed grief is defined by an absence of grieving within the first weeks orm<strong>on</strong>ths after the death. It is often precipitated many years later by further loss.It is more likely to be severe and chr<strong>on</strong>ic when it finally occurs. Help is oftenneeded in emoti<strong>on</strong>ally accepting the reality of the past loss.2 Inhibited grief occurs when all reminders of the bereaved are avoided. Thismechanism of avoidance may work for some, but can present as irritability,restlessness or depressi<strong>on</strong>. Guided mourning is employed to encourage thebereaved to face the reality of the loss.3 Chr<strong>on</strong>ic grief (mummified grief) may be severe and occurs when a pers<strong>on</strong>fails to progress through all the tasks of mourning. There is no fixed timeperiod. Assistance is needed in helping the bereaved to move <strong>on</strong> in thegrieving process.4 Persistent hypoch<strong>on</strong>driasis can occur and may block grief. The bereavedmay take <strong>on</strong> the symptoms of the deceased or develop symptoms related toanxiety or depressi<strong>on</strong>. Explaining to the patient what is happening may be allthat is required. However, note that mortality and morbidity of widows andwidowers is increased in the first year after the death, mainly due tocardiovascular disease.5 Psychiatric disorder. A severe depressive illness may develop withdelusi<strong>on</strong>al ideas of guilt and suicidal intent. It can require hospitalisati<strong>on</strong>.Mania can be precipitated as can phobic disorders, and alcoholism andaddicti<strong>on</strong> to drugs, especially hypnotics.Some of these abnormal grief reacti<strong>on</strong>s can be dealt with by the primary healthcare teams, social workers or trained counsellors. In additi<strong>on</strong>, many areas havetheir own voluntary bereavement and counselling groups including branches ofCRUSE (www.crusebereavementcare.org.uk tel 08444779400). Health centres,hospitals or Citizens' <str<strong>on</strong>g>Advice</str<strong>on</strong>g> Bureaux should also have informati<strong>on</strong>, as will TheNati<strong>on</strong>al Associati<strong>on</strong> of Bereavement Services, 10 Nort<strong>on</strong> Folgate, L<strong>on</strong>d<strong>on</strong> E16DB (tel 02072471080). Others require specialist help from psychotherapists orpsychiatrists, and it is important for all professi<strong>on</strong>als to realise their own skillsand limitati<strong>on</strong>s.* indicates that this is best managed by specialists 72
INDEX OF DRUGS, DRESSINGS ETCThis list of drugs, dressings and other preparati<strong>on</strong>s recommended in thisHandbook is intended as an aid to pharmacists and others. The list is neitherexhaustive nor exclusive, and other products may be recommended or be moreappropriate in some circumstances. Often, <strong>on</strong>ly <strong>on</strong>e drug is listed from a wholeclass of compounds: this should not be taken to imply that other preparati<strong>on</strong>smay not be equally effective. Generic names are given for drugs with singlec<strong>on</strong>stituents, proprietary names for most compound formulati<strong>on</strong>s and fordressings.Acetazolamide 33Aciclovir 23Actisorb plus 45Adrenaline 45, 49Alfentanil 10, 12, 16, 55, 57Alginate dressings 45Allevyn 45Aluminium hydroxide 55Alverine 13, 21Amitriptyline 13, 14, 23, 36, 38, 44, 55Anabact 45Antacids 18, 31, 32Aquacel 45Arachis oil enema 25Aspirin 43Aspirin gargle 23Atropine 23Baclofen 14, 32Benzodiazepines (see also diazepam, midazolam etc) 14, 18, 29, 54, 55Benzoin co Tincture 31Betamethas<strong>on</strong>e 52Bethanechol 23Biotène 23Bisacodyl 25Bisphosph<strong>on</strong>ates 13, 51Botulinum toxin 23Br<strong>on</strong>chodilators 30, 31Bupivacaine 13, 31Buprenorphine 8, 11, 12, 43, 55, 58BuTrans (see buprenorphine) 1173* indicates that this is best managed by specialists
Calcit<strong>on</strong>in 51Carbocisteine 30, 31Carbamazepine 14, 33, 34Cavi-Care 45Charcoal dressings 45Chlorhexidine 22Chlorphenamine 43, 45Chlorpromazine 32, 57Cimetidine 43, 44Clinisorb 45Clomethiazole 38Cl<strong>on</strong>azepam 14, 34, 42, 55, 57Cl<strong>on</strong>idine 14, 44Co-Codamol 6Co-Danthramer 25Co-Danthrusate 25Codeine 6, 10, 26, 31Colestyramine 26, 43Colifoam 14Cre<strong>on</strong> 26Cyclizine 8, 18, 19, 21, 54, 55, 57, 59Dantrolene 14Dexamethas<strong>on</strong>e (see also Steroids) 13, 14, 18, 19, 21, 24, 27, 30, 32, 33,34, 35, 39, 41, 44, 52, 54, 56, 57Diamorphine 8-12, 16, 21, 29, 45, 49, 57, 58Diazepam 14, 29, 32, 34, 37, 42, 49, 57, 59Diclofenac (see NSAIDs)Difflam 23Docusate sodium 21, 25Domperid<strong>on</strong>e 18, 19, 21, 27, 32Dosulepin 14, 36, 38Ent<strong>on</strong>ox 16Erythromycin 18Etamsylate 49Fentanyl 8, 10-12, 16, 55, 57, 58Fluc<strong>on</strong>azole 23Flurbiprofen lozenges 23Furosemide 27, 48, 57* indicates that this is best managed by specialists 74
Gabapentin 13, 14, 43, 55Glargine 53Gliclazide 53Glimepiride 53Glitaz<strong>on</strong>es 53GlucoGel 53Glycerol suppositories 25Glyceryl trinitrate 14Glycopyrr<strong>on</strong>ium 23, 44, 57, 59Haloperidol 8, 18, 19, 21, 32, 41, 54, 55, 57, 59Heparin 50Hydrocortis<strong>on</strong>e 14, 23, 52Hydrogel 45Hydromorph<strong>on</strong>e 9, 10, 12Hyoscine butylbromide 13, 21, 23, 57, 59Hyoscine hydrobromide 18, 19, 23, 57, 59Ibandr<strong>on</strong>ic acid 51Ibuprofen (see NSAIDs) 6Insulins 53Kaltostat 45, 49Ketamine 14Ketorolac (see NSAIDs) 57Lactulose 25, 55Lamotrigine 34Levomepromazine 18, 19, 21, 32, 41, 42, 55, 57, 59Lidocaine 23Lomotil 26Loperamide 26Loratadine 43Lorazepam 29, 34, 37, 41Macrogols 21, 25Magnesium hydroxide 21, 25, 55Mebeverine 13, 21Megestrol 24Melat<strong>on</strong>in 38Menthol 2% in aqueous cream 43Menthol & eucalyptus inhalati<strong>on</strong> 31Metformin 5375* indicates that this is best managed by specialists
Methad<strong>on</strong>e 8, 9, 12, 14Methylnaltrex<strong>on</strong>e 25Methylphenidate 24, 39, 47Metoclopramide 8, 18, 19, 21, 27, 32, 55, 57, 59Metr<strong>on</strong>idazole 23, 26, 45Metr<strong>on</strong>idazole gel 45Midazolam 29, 30, 32, 34, 37, 41, 42, 49, 57, 59Mirtazapine 14, 36, 43Misoprostol 6, 18Modafinil 24Morphine 7-13, 16, 21, 29, 31, 45, 57, 58Movicol 21, 25Mugard 23Nalox<strong>on</strong>e 8Naltrex<strong>on</strong>e 43Naproxen (see NSAIDs)Neurokinin 1 antag<strong>on</strong>ists 19Nifedipine 14, 32Nitrous oxide 16NSAIDs 6, 13, 14, 23, 24, 30, 44, 45, 54, 55, 57, 59Nystatin 23Octreotide 21, 26, 57Ondansetr<strong>on</strong> 19, 43, 55, 57Oramorph (see morphine)Oxybutynin 13, 44Oxycod<strong>on</strong>e 9, 10, 12, 16, 57Oxygen 29, 41, 54Pamidr<strong>on</strong>ate 51Pancreatic enzymes 26Paracetamol 6, 27, 33, 44, 45, 55Paroxetine 43Phenobarbital 34, 42, 57Phenytoin 33, 34Phosphates enemas 25Pilocarpine 23PPIs 6, 18, 32, 49Prednisol<strong>on</strong>e (see also Steroids) 24, 52Predsol enema 14Pregabalin 14, 55Propantheline 13, 44* indicates that this is best managed by specialists 76
Propranolol 23, 37, 44Ranitidine 21, 32Rifampicin 43Saline (sodium chloride) 29-31, 45, 57Senna 25Sodium picosulfate 25Sodium Valproate 14, 34Sorbsan 45Spir<strong>on</strong>olact<strong>on</strong>e 27SSRIs 36Steroids (see also dexamethas<strong>on</strong>e, prednisol<strong>on</strong>e) 13, 14, 26, 30, 31,46, 49, 52, 55Sucralfate 23, 49Sulph<strong>on</strong>ylureas 53Temazepam 38Thalidomide 44, 49Tizanidine 14Tramadol 6, 10Tranexamic acid 49Tolterodine 13Venlafaxine 14Vitamin K 49Warfarin 50, 55Xerotin 23Zalepl<strong>on</strong> 38Zoledr<strong>on</strong>ic acid 51Zolpidem 38Zopicl<strong>on</strong>e 3877* indicates that this is best managed by specialists
ACKNOWLEDGEMENTSThis advice <strong>on</strong> <strong>clinical</strong> <strong>management</strong> is derived from the Bath District HealthAuthority Clinical standards for palliative medicine and terminal care (1991),revised by Dr Roderick MacLeod, Jane Vella-Brincat and Dr Chris Higgs,Dorothy House Foundati<strong>on</strong>, in 1993.The format and c<strong>on</strong>tent were revised for the third editi<strong>on</strong> in 1995 by Dr ChrisHiggs, Jane Vella-Brincat and Clare Spencer, Dorothy House Foundati<strong>on</strong>/StMartin’s Hospital Pharmacy, with additi<strong>on</strong>s from Dr Patricia Needham, DorothyHouse Foundati<strong>on</strong>, and Dr Christine Wood, Salisbury Palliative Care Services.For the fourth editi<strong>on</strong>, the publicati<strong>on</strong> was adopted in 1997/8 by the SpecialistPalliative Care units in Wessex. A fifth editi<strong>on</strong> was published in 2002 and a sixthediti<strong>on</strong> in 2007 by the Wessex Palliative Physicians assisted by colleagues withintheir individual multiprofessi<strong>on</strong>al teams, under the Chairmanship of Dr StephenKirkham (Poole).This editi<strong>on</strong>, the seventh, was undertaken in 2010 by Dr Chris Higgs, withsecretarial support from Julie Harris, Dorothy House Hospice, in c<strong>on</strong>juncti<strong>on</strong>with the Wessex Palliative Physicians and the Palliative Physicians in the Av<strong>on</strong>,Somerset, Wiltshire Cancer Services Network (ASWCS): Dr Julian Abel(West<strong>on</strong> Super Mare), Dr Lara Alloway (Basingstoke), Dr Lucy Boyland(Lymingt<strong>on</strong>), Dr Harriet Bush (Southampt<strong>on</strong>), Dr David Butler (Southampt<strong>on</strong>),Dr Jane Bywater (Basingstoke), Dr Ian Cairns (Isle of Wight), Dr CandidaCornish (Bristol), Dr Carole Dacombe (Bristol), Dr T<strong>on</strong>y Dancyger (Swind<strong>on</strong>),Dr Jita Das (Southampt<strong>on</strong>), Dr Carol Davis (Southampt<strong>on</strong>), Dr Saskie Dorman(Poole), Prof Karen Forbes (Bristol), Dr Ann Goggin (Southampt<strong>on</strong>), Dr HuwJ<strong>on</strong>es (Portsmouth), Dr Claire Kendal (Bristol), Dr Helen Kirk (Salisbury), DrStephen Kirkham (Poole), Dr Rachel McCoubrie (Bristol), Dr Marina Malthouse(Bath), Dr P-J Morey (Portsmouth), Dr Tricia Needham (Bath), Dr RosamundPugh (Christchurch), Dr Fi<strong>on</strong>a Randall (Christchurch), Dr Colette Reid (Bristol),Dr Alis<strong>on</strong> Rich (West<strong>on</strong> Super Mare), Dr Adrian Ruddle (Portsmouth), DrRichard Sloan (Dorchester), Dr Karen Steadman (Dorchester), Dr RebeccaTunstall (Bristol), Dr Brenda Ward (Yeovil), Dr Bridget Wood (Lymingt<strong>on</strong>).Additi<strong>on</strong>al invaluable assistance was provided by colleagues within ourindividual multiprofessi<strong>on</strong>al teams, including Geoff Allen, pharmacist, and RuthGrett<strong>on</strong> RN, Dorothy House Hospice.Printing by Hierographics Ltd, Designer House, Sandford Lane Industrial Estate,Wareham, Dorset. BH20 4DY. 01929 554454.Copyright © Wessex and ASWCS Palliative Physicians 2010* indicates that this is best managed by specialists 78
NOTES79* indicates that this is best managed by specialists
NOTES* indicates that this is best managed by specialists 80