Letter to the Editor - Cutis
Letter to the Editor - Cutis
Letter to the Editor - Cutis

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
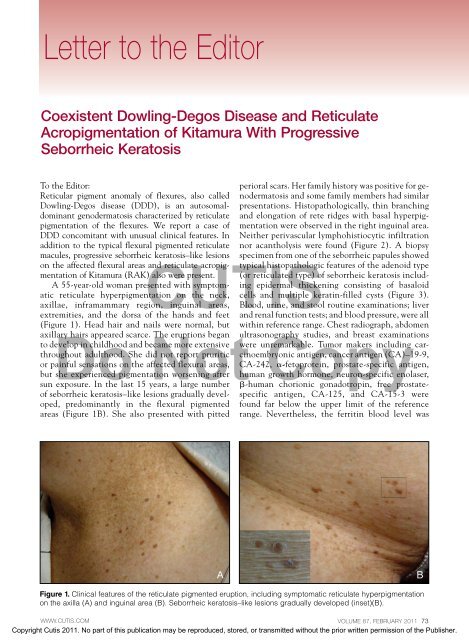
<strong>Letter</strong> <strong>to</strong> <strong>the</strong> Edi<strong>to</strong>r<strong>Letter</strong> <strong>to</strong> <strong>the</strong> Edi<strong>to</strong>rCoexistent Dowling-Degos Disease and ReticulateAcropigmentation of Kitamura With ProgressiveSeborrheic Kera<strong>to</strong>sisTo <strong>the</strong> Edi<strong>to</strong>r:Reticular pigment anomaly of flexures, also calledDowling-Degos disease (DDD), is an au<strong>to</strong>somaldominantgenoderma<strong>to</strong>sis characterized by reticulatepigmentation of <strong>the</strong> flexures. We report a case ofDDD concomitant with unusual clinical features. Inaddition <strong>to</strong> <strong>the</strong> typical flexural pigmented reticulatemacules, progressive seborrheic kera<strong>to</strong>sis–like lesionson <strong>the</strong> affected flexural areas and reticulate acropigmentationof Kitamura (RAK) also were present.A 55-year-old woman presented with symp<strong>to</strong>maticreticulate hyperpigmentation on <strong>the</strong> neck,axillae, inframammary region, inguinal areas,of seborrheic kera<strong>to</strong>sis–like lesions gradually developed,predominantly in <strong>the</strong> flexural pigmentedareas (Figure 1B). She also presented with pittedperioral scars. Her family his<strong>to</strong>ry was positive for genoderma<strong>to</strong>sisand some family members had similarpresentations. His<strong>to</strong>pathologically, thin branchingand elongation of rete ridges with basal hyperpigmentationwere observed in <strong>the</strong> right inguinal area.Nei<strong>the</strong>r perivascular lymphohistiocytic infiltrationnor acantholysis were found (Figure 2). A biopsyspecimen from one of <strong>the</strong> seborrheic papules showedtypical his<strong>to</strong>pathologic features of <strong>the</strong> adenoid type(or reticulated type) of seborrheic kera<strong>to</strong>sis includingepidermal thickening consisting of basaloidcells and multiple keratin-filled cysts (Figure 3).CUTISBlood, urine, and s<strong>to</strong>ol routine examinations; liverextremities, and <strong>the</strong> dorsa of <strong>the</strong> hands and feet and renal function tests; and blood pressure, were all(Figure 1). Head hair and nails were normal, but within reference range. Chest radiograph, abdomenaxillaryDohairs appeared scarce.NotThe eruptions began ultrasonographyCopystudies, and breast examinations<strong>to</strong> develop in childhood and became more extensive were unremarkable. Tumor makers including carcinoembryonicantigen, cancer antigen (CA)–19-9,throughout adulthood. She did not report pruriticor painful sensations on <strong>the</strong> affected flexural areas, CA-242, a-fe<strong>to</strong>protein, prostate-specific antigen,but she experienced pigmentation worsening after human growth hormone, neuron-specific enolaser,sun exposure. In <strong>the</strong> last 15 years, a large number b-human chorionic gonadotropin, free prostatespecificantigen, CA-125, and CA-15-3 werefound far below <strong>the</strong> upper limit of <strong>the</strong> referencerange. Never<strong>the</strong>less, <strong>the</strong> ferritin blood level wasABFigure 1. Clinical features of <strong>the</strong> reticulate pigmented eruption, including symp<strong>to</strong>matic reticulate hyperpigmentationon <strong>the</strong> axilla (A) and inguinal area (B). Seborrheic kera<strong>to</strong>sis–like lesions gradually developed (inset)(B).WWW.CUTIS.COM VOLUME 87, FEBRUARY 2011 73Copyright <strong>Cutis</strong> 2011. No part of this publication may be reproduced, s<strong>to</strong>red, or transmitted without <strong>the</strong> prior written permission of <strong>the</strong> Publisher.
<strong>Letter</strong> <strong>to</strong> <strong>the</strong> Edi<strong>to</strong>rCUTISDo Not CopyFigure 2. Light microscopy revealed typical thin branchingof epidermal downgrowths from one of <strong>the</strong> lesions ofreticulate hyperpigmentation (H&E, original magnification3100 [inset magnification 3400]).Figure 3. Light microscopy revealed many keratin-filledcysts from a seborrheic papule (H&E, original magnification3100 [inset magnification 3400]).250 ng/mL (reference range, 15–200 ng/mL). Theoverlap of DDD and RAK concomitant with progressiveseborrheic kera<strong>to</strong>sis was diagnosed on <strong>the</strong>basis of <strong>the</strong> clinical and his<strong>to</strong>pathologic features.Although DDD and RAK are benign conditions,<strong>the</strong>y usually cause aes<strong>the</strong>tically annoyingconsequences. 1 They are subsumed under <strong>the</strong>heading of reticulate hyperpigmentation and areinherited as a rare au<strong>to</strong>somal-dominant trait withvariable penetrance. 2 The association of <strong>the</strong>se2 conditions has suggested <strong>the</strong> existence of aclinical spectrum between <strong>the</strong> DDD and RAKpoles 3 that could represent different features of <strong>the</strong>same disease. Findings from our case streng<strong>the</strong>nthis hypo<strong>the</strong>sis.Some disorders such as multiple epidermalcysts, hidradenitis suppurativa, and squamous cellcarcinomas have been reported in association withDDD-pigmented areas. 4 The coexistence betweenDDD and seborrheic kera<strong>to</strong>sis does not seem <strong>to</strong>be coincidental in this patient because severalmembers of her family were affected by both conditions.Seborrheic kera<strong>to</strong>sis is one of <strong>the</strong> morecommon benign epidermal neoplasms; however,<strong>the</strong> association with malignancy can be useful asa cutaneous clue for diagnosis of occult internaltumors. 5 Therefore, one must emphasize <strong>the</strong> roleof correctly identifying its variants. The distinctclinical presentations in this patient concomitantwith progressive seborrheic kera<strong>to</strong>sis may representan unusual variant of DDD associated with RAKand scarce axillary hairs. These clinical featuresmay reflect simultaneous underlying defects of follicularproliferation. Fur<strong>the</strong>rmore, <strong>the</strong> comparison74 CUTIS ® WWW.CUTIS.COMCopyright <strong>Cutis</strong> 2011. No part of this publication may be reproduced, s<strong>to</strong>red, or transmitted without <strong>the</strong> prior written permission of <strong>the</strong> Publisher.
<strong>Letter</strong> <strong>to</strong> <strong>the</strong> Edi<strong>to</strong>rbetween <strong>the</strong> classic and variant forms may contribute<strong>to</strong> DDD gene mapping in special keratin genes. 6Characterization of <strong>the</strong> DDD gene will provideimportant clues <strong>to</strong> better understand <strong>the</strong> molecularmechanisms of pigmentation and would increase<strong>the</strong> hope for effective interventional strategies inclinical practice.Chongqing. Dr. San<strong>to</strong>s is from <strong>the</strong> InternalMedicine Department of <strong>the</strong> Catholic UniversityMedical Course and Armed Forces Hospital,Brasília-DF, Brazil.The authors report no conflict of interest.REFERENCESAcknowledgment—This work was partly supported 1. Müller CS, Pföhler C, Tilgen W. Changing a concept—by <strong>the</strong> National Natural Science Foundation of controversy on <strong>the</strong> confusing spectrum of <strong>the</strong> reticulateChina (No. 81072502 and 30801013) and Innovation pigmented disorders of <strong>the</strong> skin [published online ahead ofProject of Outstanding Young Scholar of Third print June 17, 2008]. J Cutan Pathol. 2009;36:44-48.Military Medical University (No. 2007XG35).2. Wu YH, Lin YC. Generalized Dowling-Degos disease. JAm Acad Derma<strong>to</strong>l. 2007;57:327-334.Sincerely,3. Al Hawsawi K, Al Aboud K, Alfadley A, et al. ReticulateZhu Shen, MD, PhDacropigmentation of Kitamura-Dowling Degos diseaseLing Chen, MDoverlap: a case report. Int J Derma<strong>to</strong>l. 2002;41:518-520.Qingyi Ye, MD4. Weber LA, Kan<strong>to</strong>r GR, Bergfeld WF. ReticulateFei Hao, MD, PhDpigmented anomaly of <strong>the</strong> flexures (Dowling-Degos disease):a case report associated with hidradenitis sup-Vi<strong>to</strong>rino Modes<strong>to</strong> dos San<strong>to</strong>s, MD, PhDXichuan Yang, MD, PhDCUTISpurativa and squamous cell carcinoma. <strong>Cutis</strong>. 1990;45:Baiyu Zhong, MD446-450.5. Heaphy MR Jr, Millns JL, Schroeter AL. The sign ofDrs. Shen, Ye, Hao, Yang, and Zhong are from <strong>the</strong> Leser-Trélat in a case of adenocarcinoma of <strong>the</strong> lung. J AmDepartment of Derma<strong>to</strong>logy, Southwest Hospital, Acad Derma<strong>to</strong>l. 2000;43(2, pt 2):386-390.Third Military Medical University, Chongqing, 6. Betz RC, Planko L, Eigelshoven S, et al. Loss-of-functionChina. Dr. Chen is from <strong>the</strong> Department of mutations in <strong>the</strong> keratin 5 gene lead <strong>to</strong> Dowling-DegosDerma<strong>to</strong>logy,DoInstitute of BattleNotSurgery, Daping diseaseCopy[published online ahead of print January 19, 2006].Hospital, Third Military Medical University, Am J Hum Genet. 2006;78:510-519.WWW.CUTIS.COM VOLUME 87, FEBRUARY 2011 75Copyright <strong>Cutis</strong> 2011. No part of this publication may be reproduced, s<strong>to</strong>red, or transmitted without <strong>the</strong> prior written permission of <strong>the</strong> Publisher.