Safe and efficientuse of the M4 safety handpiece ... - De Vos Endo BV
Safe and efficientuse of the M4 safety handpiece ... - De Vos Endo BV
Safe and efficientuse of the M4 safety handpiece ... - De Vos Endo BV
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
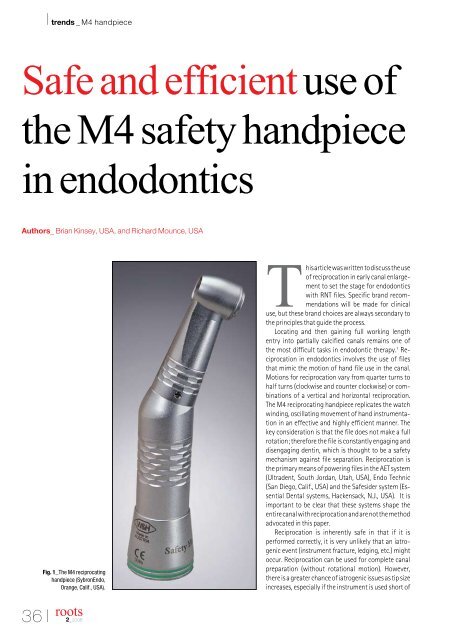
I trends _ <strong>M4</strong> h<strong>and</strong>piece<strong>Safe</strong> <strong>and</strong> efficient use <strong>of</strong><strong>the</strong> <strong>M4</strong> <strong>safety</strong> h<strong>and</strong>piecein endodonticsAuthors_ Brian Kinsey, USA, <strong>and</strong> Richard Mounce, USAFig. 1_The <strong>M4</strong> reciprocatingh<strong>and</strong>piece (Sybron<strong>Endo</strong>,Orange, Calif., USA).This article was written to discuss <strong>the</strong> use<strong>of</strong> reciprocation in early canal enlargementto set <strong>the</strong> stage for endodonticswith RNT files. Specific br<strong>and</strong> recommendationswill be made for clinicaluse, but <strong>the</strong>se br<strong>and</strong> choices are always secondary to<strong>the</strong> principles that guide <strong>the</strong> process.Locating <strong>and</strong> <strong>the</strong>n gaining full working leng<strong>the</strong>ntry into partially calcified canals remains one <strong>of</strong><strong>the</strong> most difficult tasks in endodontic <strong>the</strong>rapy. 1 Reciprocationin endodontics involves <strong>the</strong> use <strong>of</strong> filesthat mimic <strong>the</strong> motion <strong>of</strong> h<strong>and</strong> file use in <strong>the</strong> canal.Motions for reciprocation vary from quarter turns tohalf turns (clockwise <strong>and</strong> counter clockwise) or combinations<strong>of</strong> a vertical <strong>and</strong> horizontal reciprocation.The <strong>M4</strong> reciprocating h<strong>and</strong>piece replicates <strong>the</strong> watchwinding, oscillating movement <strong>of</strong> h<strong>and</strong> instrumentationin an effective <strong>and</strong> highly efficient manner. Thekey consideration is that <strong>the</strong> file does not make a fullrotation; <strong>the</strong>refore <strong>the</strong> file is constantly engaging <strong>and</strong>disengaging dentin, which is thought to be a <strong>safety</strong>mechanism against file separation. Reciprocation is<strong>the</strong> primary means <strong>of</strong> powering files in <strong>the</strong> AET system(Ultradent, South Jordan, Utah, USA), <strong>Endo</strong> Technic(San Diego, Calif., USA) <strong>and</strong> <strong>the</strong> <strong>Safe</strong>sider system (Essential<strong>De</strong>ntal systems, Hackensack, N.J., USA). It isimportant to be clear that <strong>the</strong>se systems shape <strong>the</strong>entire canal with reciprocation <strong>and</strong> are not <strong>the</strong> methodadvocated in this paper.Reciprocation is inherently safe in that if it isperformed correctly, it is very unlikely that an iatrogenicevent (instrument fracture, ledging, etc.) mightoccur. Reciprocation can be used for complete canalpreparation (without rotational motion). However,<strong>the</strong>re is a greater chance <strong>of</strong> iatrogenic issues as tip sizeincreases, especially if <strong>the</strong> instrument is used short <strong>of</strong>36 Iroots2_2008
trends _ <strong>M4</strong> h<strong>and</strong>piece IFig. 2__#6, #8, #10 h<strong>and</strong> K filesused in <strong>the</strong> <strong>M4</strong>. After use <strong>of</strong> <strong>the</strong>#10 h<strong>and</strong> K file in <strong>the</strong> <strong>M4</strong>, <strong>the</strong> canalis ready for rotary nickel titaniuminstrumentation.<strong>the</strong> MC in a multiplanar curvature. This concept willbe exp<strong>and</strong>ed upon later in <strong>the</strong> cited precautions forreciprocation techniques.The technique described within this article recommendsreciprocation for creating a minimal enlargement<strong>of</strong> <strong>the</strong> canal in order to create a reproducibleglide path to <strong>the</strong> true working length that will facilitate<strong>the</strong> safe use <strong>of</strong> RNT instruments. Said differently, a #6,#8, #10 h<strong>and</strong> file can be used with a watch windingmotion in a reciprocating h<strong>and</strong>piece such as <strong>the</strong> <strong>M4</strong>(Sybron<strong>Endo</strong>, Orange, Calif., USA) to mimic <strong>the</strong> use <strong>of</strong><strong>the</strong>se instruments by h<strong>and</strong>. These small h<strong>and</strong> files canbe placed into <strong>the</strong> <strong>M4</strong>, <strong>and</strong> once activated (within acanal, which may resist <strong>the</strong> initial insertion a h<strong>and</strong> file)can be used to create <strong>the</strong> minimal diameter needed touse RNT instruments safely <strong>and</strong> efficiently.The goals <strong>of</strong> canal enlargement remain <strong>the</strong> same,whe<strong>the</strong>r canal enlargement takes place with:1. Reciprocation — i.e., using a reciprocating h<strong>and</strong>piecewith h<strong>and</strong> files to create watch winding motionpowered by an electric motor2. Rotational forces — i.e., using a h<strong>and</strong>piece withh<strong>and</strong> files in a complete rotational motion powered byan electric motor3. H<strong>and</strong> files4. Rotary nickel titanium (RNT) files5. Gates glidden drills <strong>and</strong> h<strong>and</strong> files6. Any o<strong>the</strong>r combination <strong>of</strong> instruments, includingbut not limited to: peezo reamers, hedstrom files, h<strong>and</strong>reamers, h<strong>and</strong> K files, nickel titanium h<strong>and</strong> files, etc.The primary goals <strong>of</strong> canal instrumentationare to:1. Prepare a final canal shape that is a continuouslytapering funnel with narrowing cross sectional diametersfrom <strong>the</strong> orifice to <strong>the</strong> minor constriction (MC)<strong>of</strong> <strong>the</strong> apical foramen.2. Maintain <strong>the</strong> original canal position, only enlargedinto a continuously tapering funnel as in No.1 above.3. Maintain <strong>the</strong> original size <strong>and</strong> position <strong>of</strong> <strong>the</strong>MC <strong>of</strong> <strong>the</strong> apical foramen; <strong>the</strong> MC is not enlarged ortransported in any manner.4. Create a final canal preparation that is largeenough in taper <strong>and</strong> master apical diameter to optimizeirrigation, cone fit <strong>and</strong> obturation.Secondary considerations in canal preparationinclude:1. Canal preparation is undertaken with a viewtoward preventing iatrogenic events. The final canalpreparation is accomplished with <strong>the</strong> initial anatomy<strong>of</strong> <strong>the</strong> tooth taken into account, especially with regardto external root form <strong>and</strong> dentin wall thickness. Therisk <strong>of</strong> an iatrogenic event (or having one occur if <strong>the</strong>tooth has already been started) is carefully consideredin light <strong>of</strong> <strong>the</strong> anatomy.2. Orifice shape <strong>and</strong> canal taper should be largeFig 3_H<strong>and</strong> K files that have beenmodified by trimming. The file on <strong>the</strong>far left is a #10 21 mm h<strong>and</strong> K file.The middle file has been trimmed2 mm <strong>and</strong> <strong>the</strong> far right trimmedby 3 mm to make <strong>the</strong>m stiffer <strong>and</strong>more capable <strong>of</strong> breaking through ablockage.roots2_2008I 37
I trends _ <strong>M4</strong> h<strong>and</strong>pieceFig. 4_The Twisted File(Sybron<strong>Endo</strong>, Orange, Calif., USA).<strong>M4</strong> preparations can be blendedwith <strong>the</strong> Twisted instrument.38 Iroots2_2008enough to remove restrictive dentin coronally, maximizeirrigation, allow tactile control over instruments<strong>and</strong> optimize visualization through <strong>the</strong> surgical operatingmicroscope.General considerations to maximize <strong>M4</strong>efficiency:1. The surgical operating microscope (SOM) (GlobalSurgical, St. Louis, Mo., USA) is invaluable for visualization<strong>of</strong> <strong>the</strong> canal at all times in <strong>the</strong> process <strong>of</strong> enlargement.The SOM allows literally pinpoint accuracy incanal location <strong>and</strong> observation <strong>of</strong> <strong>the</strong> canal preparationas it unfolds. There is no substitute for <strong>the</strong> lighting,magnification <strong>and</strong> tactile control afforded by its use.2. Access must be straight line.3. The cervical dentinal triangle should be removedto help facilitate straight-line access. Files should dropinto <strong>the</strong> straightaway portion <strong>of</strong> <strong>the</strong> root without beingdeflected by <strong>the</strong> walls <strong>of</strong> <strong>the</strong> access cavity.4. The orifice <strong>of</strong> <strong>the</strong> canal should be enlargedinitially so as to allow efficient irrigation <strong>of</strong> <strong>the</strong> space<strong>and</strong> optimal tactile <strong>and</strong> visual control over <strong>the</strong> fileswhe<strong>the</strong>r h<strong>and</strong> or RNT.5. Use <strong>of</strong> <strong>the</strong> <strong>M4</strong> reciprocating h<strong>and</strong>piece presupposesthat <strong>the</strong> coronal third is ideally shaped <strong>and</strong> that<strong>the</strong> apical portion <strong>of</strong> <strong>the</strong> canal has been negotiatedsafely in <strong>the</strong> presence <strong>of</strong> a lubricant (irrigant). Thisirrigant will vary depending on whe<strong>the</strong>r <strong>the</strong> canalsare vital or necrotic or in retreatment cases. In vitalcases <strong>the</strong> irrigant <strong>of</strong> choice is sodium hypochlorite, forretreatment cases it is 2% chlorhexidine (more effectivethan NaOCl in killing E. faecalis, commonly foundin cases requiring retreatment) <strong>and</strong> in necrotic cases,ei<strong>the</strong>r sodium hypochlorite or CHX can be used. It isnoteworthy that <strong>the</strong>se two irrigants are not mixed in<strong>the</strong> canal <strong>and</strong> one must be fully flushed before using<strong>the</strong> o<strong>the</strong>r. In any event, irrigant should be in <strong>the</strong> canalat all times when using any instrument to provide bothlubrication <strong>and</strong> bactericidal irrigation.6. Use <strong>of</strong> <strong>the</strong> <strong>M4</strong> also presupposes that in vital casesthat contain a great deal <strong>of</strong> pulp in <strong>the</strong> chamber thata viscous EDTA gel (File Eze, Ultradent, South JordanUtah, USA; Slick Gel, Sybron<strong>Endo</strong>, Orange, Calif., USA)will be used to prevent pulp from being propelled <strong>and</strong>compacted into <strong>the</strong> apical half <strong>of</strong> <strong>the</strong> root. The viscousEDTA in <strong>the</strong> chamber holds <strong>the</strong> pulp in suspension <strong>and</strong>allows it to be flushed away during canal irrigation <strong>and</strong>avoid apical blockage.7. The #6, #8 <strong>and</strong> #10 h<strong>and</strong> K files are used in <strong>the</strong>initial negotiation <strong>of</strong> <strong>the</strong> canal. The clinician shouldhave enough h<strong>and</strong> K files on <strong>the</strong>ir sponge to negotiate<strong>the</strong> canal irrespective <strong>of</strong> <strong>the</strong> technical challengesthat may arise. For example, <strong>the</strong> h<strong>and</strong> K files shouldbe long enough to address <strong>the</strong> canal, but not be solong as to buckle <strong>and</strong> bend when pressure is placedupon <strong>the</strong>m. H<strong>and</strong> files can be trimmed <strong>and</strong> as manymillimeters as needed snipped <strong>of</strong>f <strong>the</strong> files with ascissors in order to custom make a h<strong>and</strong> file <strong>of</strong> <strong>the</strong>correct length <strong>and</strong> stiffness to bypass <strong>the</strong> particularblockage. H<strong>and</strong> files should be as sharp as possible<strong>and</strong> optimally used once. The clinician needs <strong>the</strong>sharpest <strong>and</strong> stiffest h<strong>and</strong> file possible to bypassledges <strong>and</strong> debris, as well as to negotiate curvatures.Empirically, many canals that at first might be difficultto negotiate can be made negotiable (safely <strong>and</strong>efficiently) by placing just enough pressure to pushpast a blockage or particular calcification. To gain <strong>the</strong>tactile sense needed to learn how much pressure can<strong>and</strong> should be placed on a h<strong>and</strong> file in such a case, <strong>the</strong>reader is encouraged to practice in extracted teeth. It isalso noteworthy that <strong>the</strong> clinician should pre curve allh<strong>and</strong> files before placement in <strong>the</strong> canal during negotiationso as to allow <strong>the</strong> curvature on <strong>the</strong> h<strong>and</strong> file t<strong>of</strong>ollow <strong>the</strong> curvature present in <strong>the</strong> root. This curvaturecan be placed on <strong>the</strong> h<strong>and</strong> file with <strong>Endo</strong>Bender pliers(Sybron<strong>Endo</strong>, Orange, Calif., USA) that allow a gentlebut precise curvature to be placed onto <strong>the</strong> apical 3–4mm <strong>of</strong> <strong>the</strong> h<strong>and</strong> file.8. Knowledge <strong>of</strong> <strong>the</strong> canal anatomy is essentialin that <strong>the</strong> manner with which an <strong>M4</strong> reciprocatingh<strong>and</strong>piece will be employed is directly related to <strong>the</strong>anatomic averages present <strong>and</strong> <strong>the</strong> degree <strong>of</strong> calcification.Specifically, <strong>the</strong> initial diameter <strong>of</strong> <strong>the</strong> averageMC <strong>of</strong> <strong>the</strong> apical foramen is approximately 0.28 mm.This is important because <strong>the</strong> h<strong>and</strong> files used with <strong>the</strong><strong>M4</strong> are much smaller than this — i.e., #6, #8 <strong>and</strong> #10.When <strong>the</strong>y are used, <strong>the</strong>se h<strong>and</strong> files are placed justslightly beyond <strong>the</strong> MC. The use <strong>of</strong> <strong>the</strong> <strong>M4</strong> is not intendedto enlarge <strong>the</strong> MC <strong>and</strong> as a result <strong>of</strong> <strong>the</strong> <strong>M4</strong> userecommended here, <strong>the</strong> clinician is only trying to createa minimal enlargement <strong>of</strong> <strong>the</strong> canal to facilitate <strong>the</strong>use <strong>of</strong> RNT by creating a glide path for <strong>the</strong>m to followto <strong>the</strong> true working length. For example, <strong>the</strong> #6–10 isplaced just beyond <strong>the</strong> MC <strong>and</strong> activated; this motionassures that <strong>the</strong> canal will not be blocked with debrisor ledged. Alternatively, using <strong>the</strong> <strong>M4</strong> short <strong>of</strong> <strong>the</strong> MCin a multiplanar pig-tailed curvature with a h<strong>and</strong> filethat is larger has <strong>the</strong> potential to create a ledge <strong>and</strong> orpossibly a debris blockage.9. It is assumed that <strong>the</strong> clinician is working under
trends _ <strong>M4</strong> h<strong>and</strong>piece Ia rubber dam.10. The <strong>M4</strong> can be used clinically with reamers, <strong>and</strong>K files made <strong>of</strong> different cross sectional blanks, includingcarbon steel instruments, etc.Irrespective <strong>of</strong> <strong>the</strong> cross sectional design <strong>of</strong> <strong>the</strong>h<strong>and</strong> file used, <strong>the</strong> <strong>M4</strong> can save significant h<strong>and</strong>fatigue relative to enlarging canals in early enlargementperformed entirely by h<strong>and</strong>. What would takeperhaps two to three minutes with <strong>the</strong> <strong>M4</strong> in glide pathcreation <strong>of</strong> a constricted canal might take six to eightminutes or longer by h<strong>and</strong>. Caution is advised, though,as <strong>the</strong> overzealous use <strong>of</strong> <strong>the</strong> <strong>M4</strong> could lead to excessdentin removal as a result <strong>of</strong> <strong>the</strong> clinician staying in <strong>the</strong>canal longer than necessary. 2 When <strong>the</strong> file attachedto <strong>the</strong> <strong>M4</strong> moves without resistance in <strong>the</strong> canal, it istime to withdraw <strong>the</strong> instrument <strong>and</strong> chose a largerone if a greater diameter is required.Principles utilizing <strong>the</strong> <strong>M4</strong> clinically:1. Always use irrigation with <strong>the</strong> <strong>M4</strong>, never activate<strong>the</strong> <strong>M4</strong> in a dry canal.2. Use <strong>of</strong> <strong>the</strong> <strong>M4</strong> with a hedstrom file should beavoided. A <strong>safety</strong> hedstrom file exists, which is designedwith <strong>the</strong> flutes removed on one side <strong>of</strong> <strong>the</strong> file<strong>and</strong> is recommended for use with a <strong>M4</strong> reciprocatingh<strong>and</strong>piece. However, it has been demonstrated that agreater potential exists for excess removal <strong>of</strong> dentinalong <strong>the</strong> inner aspect <strong>of</strong> curved canals even with <strong>the</strong><strong>safety</strong> hedstrom file. As <strong>the</strong> canal curvature increases,<strong>the</strong>re is even greater chance for excess dentin removal,possibly leading to strip perforation. 3 Taking a hedstromfile beyond <strong>the</strong> MC can rapidly <strong>and</strong> easily tear<strong>the</strong> MC <strong>of</strong> <strong>the</strong> apical foramen <strong>and</strong> destroy <strong>the</strong> naturalapical architecture that provides <strong>the</strong> barrier to extrusion<strong>of</strong> irrigants, sealer <strong>and</strong> core obturating material.Using small h<strong>and</strong> files with <strong>the</strong> <strong>M4</strong> <strong>and</strong> doing so in<strong>the</strong> manner described in this paper will avoid stripperforation. Larger <strong>and</strong> stiffer h<strong>and</strong> instruments usedincorrectly in reciprocation can cause all manner <strong>of</strong>canal transportations <strong>and</strong> should be avoided.Clinically, <strong>M4</strong> use is simple <strong>and</strong> veryefficient:1. The h<strong>and</strong> K file that allows negotiation <strong>of</strong> <strong>the</strong>root to <strong>the</strong> MC is placed into <strong>the</strong> canal. Clinically, this<strong>of</strong>ten manifest as a #6 or #8 that will allow insertionto <strong>the</strong> estimated or true working length <strong>of</strong> a MB2 canal.After taking <strong>the</strong> steps detailed in “General considerationsfor <strong>M4</strong> use” detailed above, <strong>and</strong> <strong>the</strong>n filling <strong>the</strong>chamber with irrigant, <strong>the</strong> h<strong>and</strong> K file that binds at<strong>the</strong> estimated working length is placed into <strong>the</strong> tooth<strong>and</strong> <strong>the</strong> clinician’s h<strong>and</strong>s are taken <strong>of</strong>f <strong>of</strong> <strong>the</strong> file. It isimportant to note that <strong>the</strong> h<strong>and</strong> K file is not placed into<strong>the</strong> <strong>M4</strong> <strong>and</strong> <strong>the</strong>n worked down <strong>the</strong> canal. While somecanals may allow this insertion, many will not.2. The <strong>M4</strong> is brought into <strong>the</strong> field <strong>and</strong> attached to<strong>the</strong> plastic h<strong>and</strong>le <strong>of</strong> <strong>the</strong> h<strong>and</strong> K file that is already in<strong>the</strong> canal at <strong>the</strong> estimated or true working length.3. The <strong>M4</strong> attachment fits onto an E type attachment<strong>of</strong> an electric motor such as <strong>the</strong> TCM III (Sybron<strong>Endo</strong>,Orange, Calif., USA). The electric motor is setat 900 rpm at <strong>the</strong> 18:1 setting. The torque control isturned <strong>of</strong>f.4. The file is gently moved apically <strong>and</strong> coronallyin 1–3 mm amplitude strokes (always kept in motion— ei<strong>the</strong>r insertion or withdrawal) for approximately15–30 seconds, at which time <strong>the</strong> h<strong>and</strong> file shouldmove easily within <strong>the</strong> canal to <strong>the</strong> working length.A rubber stopper can be put on <strong>the</strong> h<strong>and</strong> file, but itis not essential. The clinician can observe <strong>the</strong> relativeposition <strong>of</strong> <strong>the</strong> plastic <strong>of</strong> <strong>the</strong> h<strong>and</strong>le <strong>of</strong> <strong>the</strong> K file to areference point from which <strong>the</strong> true working lengthwas measured.5. After <strong>the</strong> #6 is removed from <strong>the</strong> canal, a #8 canFigs 5-7__Clinical cases performedblending <strong>the</strong> <strong>M4</strong> with <strong>the</strong> TwistedFile.roots2_2008I 39
I trends _ <strong>M4</strong> h<strong>and</strong>piece_Author infobe placed to <strong>the</strong> same depth as <strong>the</strong> #6 that is at or near<strong>the</strong> position <strong>of</strong> <strong>the</strong> true or estimated working length.Again, in <strong>the</strong> same manner <strong>the</strong> <strong>M4</strong> is attached <strong>and</strong> <strong>the</strong>canal enlarged through reciprocation to <strong>the</strong> point asin 4 above until that <strong>the</strong> file meets no resistance as it isused in <strong>the</strong> canal. The same enlargement occurs witha #10 h<strong>and</strong> file. After <strong>the</strong> use <strong>of</strong> <strong>the</strong> #10 h<strong>and</strong> file, <strong>the</strong>canal should be able to accept a #15 h<strong>and</strong> file easilyto <strong>the</strong> true working length <strong>and</strong> <strong>the</strong> canal is ready to beenlarged with RNT instruments.6. RNT enlargement <strong>of</strong> <strong>the</strong> canal can be performedwith any <strong>of</strong> <strong>the</strong> available systems. This said, we recommend<strong>the</strong> use <strong>of</strong> <strong>the</strong> Twisted File (Sybron<strong>Endo</strong>, Orange,Calif., USA). The TF is used crown down into <strong>the</strong> canalin which a glide path has been created. The importance<strong>of</strong> creating a reproducible glide path to <strong>the</strong> EWL or TWLcannot be overemphasized when using RNT systems.TF st<strong>and</strong>s in distinction to o<strong>the</strong>r RNT systems in that inapproximately 33% <strong>of</strong> <strong>the</strong> clinical cases encountered,<strong>the</strong> file can be used as a single file method <strong>of</strong> canalenlargement.FAQ:1. Will <strong>the</strong> use <strong>of</strong> an <strong>M4</strong> with <strong>the</strong> tip <strong>of</strong> <strong>the</strong> h<strong>and</strong> fileprotruding out <strong>of</strong> <strong>the</strong> MC cause bleeding <strong>and</strong> apicalinflammation?If performed correctly, bleeding from an extension<strong>of</strong> <strong>the</strong> h<strong>and</strong> K file 0.5–1 mm out <strong>the</strong> MC is not a commonobservation. Apical inflammation is a differentmatter as <strong>the</strong> speed with which <strong>the</strong> <strong>M4</strong> is movedvertically has an impact on how much debris can possiblybe pushed out <strong>of</strong> <strong>the</strong> MC. If <strong>the</strong> <strong>M4</strong> is insertedapically with force <strong>and</strong> rapid movement, <strong>the</strong>re is agreater tendency to extrude debris apically. This can beavoided or minimized by <strong>the</strong> clinician using <strong>the</strong> <strong>M4</strong> asdescribed, with a gentle <strong>and</strong> passive motion verticallyrootsBrian Kinsey, DMDDr. Kinsey is in private practice in Dacula, Ga., USA. Hepractices comprehensive general dentistry <strong>and</strong> has aspecial interest in endodontics. He can be contacted atbkinsey@kinseysmiles.com.Richard Mounce, DDSDr. Mounce lectures globally <strong>and</strong> is widely published.He is in private practice in endodontics in Vancouver,Wash., USA. He <strong>of</strong>fers intensive customized endodonticsingle day training programs in his <strong>of</strong>fice forsmall groups <strong>of</strong> doctors. For more information, contact<strong>De</strong>nnis at (360) 891-9111 or write RichardMounce@Mounce<strong>Endo</strong>.com.until it spins freely.2. Can I perform <strong>the</strong> entire preparation with reciprocation?While reciprocation for <strong>the</strong> entire canal preparationhas its advocates, reciprocation for <strong>the</strong> entirepreparation is not <strong>the</strong> predominant technique amongspecialists globally. Use <strong>of</strong> <strong>the</strong> <strong>M4</strong> <strong>and</strong> similar reciprocatingh<strong>and</strong>pieces in specialty practice is generallyconfined to a use that is similar to what is describedhere, using reciprocation <strong>of</strong> minimal enlargement inhighly calcified canals. As mentioned earlier, reciprocationin larger sizes risks canal transportation to agreater degree than rotary methods.3. Does reciprocation have any advantages overrotational canal enlargement in endodontics?There is one advantage to reciprocation, diminishedinstrument separation relative to RNT files.This said, <strong>the</strong> application <strong>of</strong> sound principles in RNTenlargement <strong>and</strong> use <strong>of</strong> an instrument like <strong>the</strong> TwistedFile could make fracture virtually unheard <strong>of</strong>.4. Does <strong>the</strong> <strong>M4</strong> <strong>and</strong> reciprocation have to be usedin every case?No. Cases that are more curved, calcified, complexanatomy <strong>and</strong> difficult to negotiate will be more amenableto initial early enlargement with <strong>the</strong> <strong>M4</strong>. Use <strong>of</strong><strong>the</strong> <strong>M4</strong> in larger canals <strong>and</strong> those with less curvaturemay be unneccessary.5. Will it be helpful if I place a viscous EDTA gel in<strong>the</strong> canal to help lubricate <strong>the</strong> canal during reciprocation?Use <strong>of</strong> a viscous EDTA gel during reciprocation isnot necessary. Viscous EDTA gel serves <strong>the</strong> primarypurpose <strong>of</strong> holding debris in suspension so that itmay be easily flushed from <strong>the</strong> canal during irrigation.Lubrication is adequate <strong>and</strong> provided by using liquidantibacterial solutions such as sodium hypochlorite<strong>and</strong> chlorhexidine.A clinically relevant review <strong>of</strong> reciprocation inendodontics has been presented. Emphasis has beenplaced on <strong>the</strong> use <strong>of</strong> reciprocation for early enlargement<strong>of</strong> canals to create a glide path <strong>and</strong> facilitate<strong>the</strong> safe <strong>and</strong> efficient use <strong>of</strong> rotary nickel titaniuminstruments.References1. Ann R Australas Coll <strong>De</strong>nt Surg. 1991 Oct;11:82-95. Anatomicalbarriers in endodontics. Martin AP.2. 1: Braz <strong>De</strong>nt J. 2006;17(1):10-4. NSK reciprocating h<strong>and</strong>piece: invitro comparative analysis <strong>of</strong> dentinal removal during root canalpreparation by different operators. Wagner MH, Barletta FB, ReisMde S, Mello LL, Ferreira R, Fern<strong>and</strong>es AL.3. Int <strong>Endo</strong>d J. 1997 Jan;30(1):16-24. Shaping ability <strong>of</strong> <strong>the</strong> <strong>M4</strong>h<strong>and</strong>piece <strong>and</strong> <strong>Safe</strong>ty Hedstrom files in simulated root canals.Lloyd A, Jaunberzins A, Dhopatkar A, Bryant S, Dummer PM.40 Iroots2_2008