

Immunologic changes in children with egg allergy ingesting - AInotes
Immunologic changes in children with egg allergy ingesting - AInotes
Immunologic changes in children with egg allergy ingesting - AInotes

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
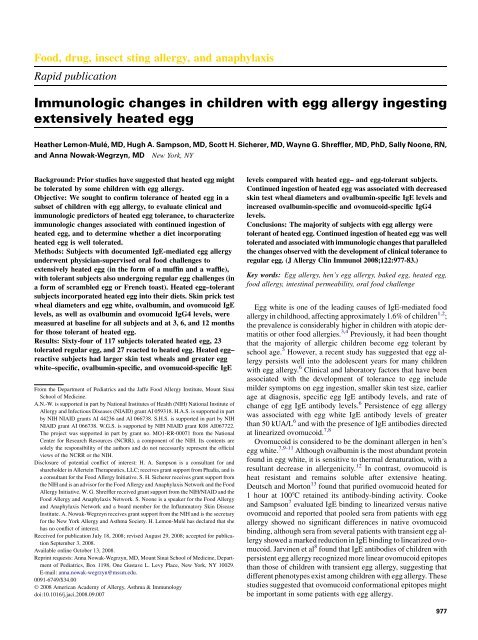
980 LEMON-MULÉ ET ALJ ALLERGY CLIN IMMUNOLNOVEMBER 2008rema<strong>in</strong><strong>in</strong>g 2 subjects, 1 discont<strong>in</strong>ued <strong>in</strong>gestion after 6 monthsbecause of parental perception of worsen<strong>in</strong>g of atopic dermatitis,although he was seen at 2 prior follow-up visits <strong>with</strong>out anobjective <strong>in</strong>crease <strong>in</strong> atopic dermatitis severity. The other childdid not like food products conta<strong>in</strong><strong>in</strong>g heated <strong>egg</strong>. These subjectsdecl<strong>in</strong>ed further follow-up <strong>with</strong><strong>in</strong> the study.FIG 2. Predicted probabilities of the heated <strong>egg</strong> challenge (oral foodchallenge) outcome and serum <strong>egg</strong> white–specific IgE concentrations andSPT responses. Logistic regression was used to calculate the probability ofreact<strong>in</strong>g dur<strong>in</strong>g heated <strong>egg</strong> oral food challenge <strong>in</strong> regard to serum ovomucoid(OVM)–specific IgE (A), serum ovalbum<strong>in</strong> (OVA)–specific IgE (B), serum<strong>egg</strong> white–specific IgE (C), and <strong>egg</strong> white–<strong>in</strong>duced SPT wheal size (D).follow-up <strong>in</strong>tervals. Ovalbum<strong>in</strong>- and ovomucoid-specific IgE/IgG4ratios were decreased from basel<strong>in</strong>e values at 3, 6, and 12 months.AnthropometricsAnthropometric parameters did not differ between the studygroups at basel<strong>in</strong>e (data not shown). In the subjects <strong>in</strong>gest<strong>in</strong>g theheated <strong>egg</strong> diet, there were no significant differences <strong>in</strong> weight,height, and body mass <strong>in</strong>dex percentiles for age and z scores betweenbasel<strong>in</strong>e and any of the follow-up times (Table IV).Intest<strong>in</strong>al permeabilityIntest<strong>in</strong>al permeability data were collected at basel<strong>in</strong>e for alltoilet-tra<strong>in</strong>ed subjects and did not differ significantly among the 3groups (not shown). LacMan values decreased compared <strong>with</strong>basel<strong>in</strong>e values <strong>in</strong> the subjects <strong>in</strong>gest<strong>in</strong>g heated <strong>egg</strong> at the 3-monthvisit (0.0255 vs 0.0203, P 5 .019) but were not significantly decreasedat the 12-month follow-up (0.0240 vs 0.0215, P 5 .9).LacMan values did not correlate <strong>with</strong> tolerance to heated and unheated<strong>egg</strong> or <strong>with</strong> the severity of reactions dur<strong>in</strong>g the oral foodchallenges to heated and unheated <strong>egg</strong>.Tolerability of a heated <strong>egg</strong> dietNone of the subjects <strong>in</strong>gest<strong>in</strong>g heated <strong>egg</strong> had documentedworsen<strong>in</strong>g of an underly<strong>in</strong>g allergic condition, such as atopicdermatitis, rh<strong>in</strong>itis, or asthma. There were no reported acuteallergic reactions to heated <strong>egg</strong> at home.WithdrawalsEighteen subjects <strong>with</strong>drew from the study after tolerat<strong>in</strong>g the<strong>in</strong>itial heated <strong>egg</strong> challenge, and all were contacted by telephone.Sixteen subjects cont<strong>in</strong>ued to <strong>in</strong>gest heated <strong>egg</strong> on a regular basis,and 1 <strong>in</strong>corporated scrambled <strong>egg</strong>s and French toast. All 16subjects cited <strong>in</strong>convenience as a reason for <strong>with</strong>drawal. Of theDISCUSSIONWe found that the majority (70%) of <strong>children</strong> <strong>with</strong> <strong>egg</strong> <strong>allergy</strong>tolerated extensively heated <strong>egg</strong> baked <strong>with</strong> wheat matrix,confirm<strong>in</strong>g prior observations that heat<strong>in</strong>g significantly dim<strong>in</strong>ishesthe allergenicity of hen’s <strong>egg</strong> white. 7,14,15 We report for thefirst time that <strong>in</strong>corporat<strong>in</strong>g extensively heated <strong>egg</strong> products <strong>in</strong>tothe daily diet is well tolerated, <strong>with</strong>out any adverse effects on underly<strong>in</strong>gallergic diseases, <strong>in</strong>test<strong>in</strong>al permeability, or normalgrowth. Furthermore, we report that regular <strong>in</strong>gestion of heated<strong>egg</strong> is associated <strong>with</strong> decreas<strong>in</strong>g SPT wheal diameters to <strong>egg</strong>white and <strong>in</strong>creas<strong>in</strong>g ovalbum<strong>in</strong>-specific and ovomucoid-specificIgG4 antibody levels. The immunologic <strong>changes</strong> occur predom<strong>in</strong>antlydur<strong>in</strong>g the first 3 months after <strong>in</strong>troduction of the heated<strong>egg</strong> and are ma<strong>in</strong>ta<strong>in</strong>ed at later time po<strong>in</strong>ts.The current standard of care for <strong>children</strong> <strong>with</strong> <strong>egg</strong> <strong>allergy</strong> isstrict dietary avoidance of <strong>egg</strong>-conta<strong>in</strong><strong>in</strong>g products. 29 However,the results of our study demonstrate that <strong>in</strong>gestion of extensivelyheated <strong>egg</strong> products is well tolerated and safe, suggest<strong>in</strong>g thatstrict dietary avoidance of heated <strong>egg</strong> might not be necessaryfor the majority of patients <strong>with</strong> <strong>egg</strong> <strong>allergy</strong>.We attempted to identify cl<strong>in</strong>ical and immunologic predictorsof tolerance to heated <strong>egg</strong>. None of the cl<strong>in</strong>ical parametersachieved high predictive value, <strong>in</strong>clud<strong>in</strong>g a history of <strong>egg</strong>-<strong>in</strong>ducedanaphylaxis. Heated <strong>egg</strong>–tolerant subjects had lower lifetimepeak <strong>egg</strong> white–specific IgE levels, smaller SPT wheal sizes, andlower <strong>egg</strong> white–, ovalbum<strong>in</strong>-, and ovomucoid-specific IgE levelsthan heated <strong>egg</strong>–reactive subjects at basel<strong>in</strong>e. However, none ofthese parameters achieved sufficiently high predictive values, andthus an oral food challenge rema<strong>in</strong>s the only conclusive test todeterm<strong>in</strong>e tolerance of heated <strong>egg</strong>.The majority of studies have identified ovomucoid to be mostimportant cl<strong>in</strong>ically, presumably because of its ability to ma<strong>in</strong>ta<strong>in</strong>allergenicity despite extensive heat<strong>in</strong>g, acid treatment, or both.Our study confirms the importance of ovomucoid because heated<strong>egg</strong>–reactive subjects had higher ovomucoid-specific IgE levelscompared <strong>with</strong> heated <strong>egg</strong>–tolerant and <strong>egg</strong>-tolerant subjects.Because ovomucoid is largely heat resistant, it follows thatsubjects <strong>with</strong> <strong>egg</strong> <strong>allergy</strong> who are tolerant of heated <strong>egg</strong> shouldhave little cl<strong>in</strong>ically significant ovomucoid-specific IgE. Theprobability curves generated for heated <strong>egg</strong> reactivity providefurther support because undetectable levels of ovomucoid-specificIgE are associated <strong>with</strong> less than a 10% chance of reactivityto heated <strong>egg</strong>. However, somewhat unexpected was the f<strong>in</strong>d<strong>in</strong>gthat only extremely <strong>in</strong>creased (>50 kUA/L) levels of ovomucoidspecificIgE were highly predictive of heated <strong>egg</strong> reactivity. Oneexplanation for this f<strong>in</strong>d<strong>in</strong>g might be the so-called matrixeffect. 30,31A recent study by Kato et al 32 demonstrated a marked decrease<strong>in</strong> the solubility of ovomucoid when <strong>egg</strong> white was mixed <strong>with</strong>wheat flour and wheat gluten and then heated at 1808C for 10 m<strong>in</strong>utes,mimick<strong>in</strong>g the process of bread mak<strong>in</strong>g. Immunoblott<strong>in</strong>gsuggested that ovomucoid polymerizes and forms high-molecular-weightcomplexes, <strong>with</strong> gluten lead<strong>in</strong>g to aggregation and
J ALLERGY CLIN IMMUNOLVOLUME 122, NUMBER 5LEMON-MULÉ ET AL 981TABLE II. Basel<strong>in</strong>e immunologic parametersHeated <strong>egg</strong> reactive Heated <strong>egg</strong> tolerant Egg tolerant P valueSPT wheal8 (6.3-9) 6 (5-8) 6 (5-6.8) .019diameter (mm)EW-specific IgE6 mo before5.7 (2.1-11.4) 1.6 (0.8-5.8) 1.1 (0.7-3.3) .001heated <strong>egg</strong> OFC (kUA/L)Egg-specific IgE (kUA/L) 5.1 (1.9-11.1) 1.3 (0.6-4.3) 1.0 (0.7-2.5) .001OVA-specific IgE (kUA/L) 7.0 (2.9-14.2) 1.6 (0.7-4.7) 1.0 (0.7-1.4)
982 LEMON-MULÉ ET ALJ ALLERGY CLIN IMMUNOLNOVEMBER 2008TABLE IV. Anthropometric parameters <strong>in</strong> <strong>children</strong> <strong>in</strong>gest<strong>in</strong>g extensively heated <strong>egg</strong>Basel<strong>in</strong>e 3 mo 6 mo 12 moHeight for age percentile 41.8 (11.1 to 75.2) 48.5 (17.6 to 80.9) 37.3 (12.7 to 73.1) 52.8 (17.5 to 77.9)Height z score 20.21 (21.2 to 0.68) 20.04 (20.9 to 0.9) 20.32 (21.1 to 0.6) 0.07 (20.9 to 0.8)Weight for age percentile 47.7 (17.3 to 69.8) 39.3 (22.7 to 68.5) 35.6 (16.6 to 73.9) 51.1 (20.8 to 76.9)Weight z score 20.06 (20.9 to 0.5) 20.28 (20.8 to 0.5) 20.37 (21.0 to 0.6) 20.03 (20.8 to 0.8)BMI percentile 47.0 (27.4 to 71.0) 46.0 (24.8 to 73.3) 47.5 (26.3 to 73.2) 51.0 (25.5 to 75.8)BMI z score 20.08 (20.6 to 0.6) 20.1 (20.7 to 0.6) 0.06 (20.6 to 0.6) 0.03 (20.7 to 0.7)BMI, Body mass <strong>in</strong>dex.All numbers represent median values <strong>with</strong> 25% to 75% <strong>in</strong>terquartile ranges provided <strong>in</strong> parentheses. No statistically significant differences were noted <strong>in</strong> any parameter (P > .05).(2.0 g), although no prior studies reported the elicit<strong>in</strong>g dose forheated <strong>egg</strong>. Similarly, the relatively high elicit<strong>in</strong>g dose ofunheated <strong>egg</strong> (1.5 g) compared <strong>with</strong> the elicit<strong>in</strong>g doses ofunheated <strong>egg</strong> reported <strong>in</strong> the literature 37 is expla<strong>in</strong>ed by ‘‘prescreen<strong>in</strong>g’’the most allergic subjects <strong>with</strong> the challenge to heated <strong>egg</strong>and by not challeng<strong>in</strong>g those <strong>with</strong> test results <strong>in</strong>dicat<strong>in</strong>g a greaterthan 95% probability of a reaction. We also excluded <strong>children</strong><strong>with</strong> a known diagnosis of eos<strong>in</strong>ophilic esophagitis because ofthe concern for the activation of the T cells <strong>with</strong> heated <strong>egg</strong> <strong>in</strong>the absence of immediate reactions.Our f<strong>in</strong>al objective was to characterize the immunologic<strong>changes</strong> associated <strong>with</strong> cont<strong>in</strong>ued <strong>in</strong>gestion of heated <strong>egg</strong>.Although we orig<strong>in</strong>ally designed the study as a randomized trial,we were unable to recruit any subjects because of the parentalconcerns of no benefit to their <strong>children</strong>. Therefore subsequentlyall <strong>children</strong> proved tolerant to extensively heated <strong>egg</strong> were put ona diet <strong>in</strong>corporat<strong>in</strong>g heated <strong>egg</strong>. As a result, we do not have acomparison group for assess<strong>in</strong>g the significance of the immunologic<strong>changes</strong> observed <strong>in</strong> <strong>children</strong> <strong>in</strong>gest<strong>in</strong>g heated <strong>egg</strong>. Nevertheless,we are encouraged by the <strong>changes</strong> of <strong>in</strong>creas<strong>in</strong>govalbum<strong>in</strong>- and ovomucoid-specific IgG4 levels and decreas<strong>in</strong>g<strong>egg</strong> white–<strong>in</strong>duced SPT wheal diameters that mimic thoseoccurr<strong>in</strong>g dur<strong>in</strong>g oral immunotherapy. 38-41 Similar to <strong>children</strong> <strong>in</strong>gest<strong>in</strong>gmilk <strong>in</strong> baked products, 33 we observed a decrease <strong>in</strong> SPTwheal diameters and an <strong>in</strong>crease <strong>in</strong> IgG4 levels <strong>with</strong><strong>in</strong> the first 3months, <strong>with</strong> no significant further <strong>changes</strong> beyond 3 months despitecont<strong>in</strong>ued <strong>in</strong>gestion of heated <strong>egg</strong>. The subjects <strong>in</strong> this studywill cont<strong>in</strong>ue to be followed cl<strong>in</strong>ically and immunologically andwill undergo oral food challenges to unheated <strong>egg</strong> to determ<strong>in</strong>ethe effect of a heated <strong>egg</strong> diet on the resolution of <strong>egg</strong> <strong>allergy</strong>.In conclusion, the results of our study <strong>in</strong>dicate that the majorityof subjects <strong>with</strong> <strong>egg</strong> <strong>allergy</strong> tolerate extensively heated (baked)<strong>egg</strong> <strong>in</strong> the food matrix and that regular <strong>in</strong>gestion of those productsis well tolerated and safe. Ingestion of heated <strong>egg</strong> by tolerantsubjects is associated <strong>with</strong> immunologic <strong>changes</strong> that can hastenthe development of tolerance to unheated <strong>egg</strong>.Currently available laboratory diagnostic tests do not reliablypredict tolerance to heated <strong>egg</strong>, and thus oral food challengesrema<strong>in</strong> the only means of establish<strong>in</strong>g a conclusive diagnosis.Oral challenges to heated <strong>egg</strong> must be undertaken under physiciansupervision <strong>with</strong> all precautions typically used for perform<strong>in</strong>gfood challenges <strong>in</strong> <strong>children</strong>. We caution strongly aga<strong>in</strong>st unsupervised<strong>in</strong>troduction of heated <strong>egg</strong> <strong>in</strong>to patients’ diets. Furtherstudies are required to determ<strong>in</strong>e whether <strong>in</strong>gest<strong>in</strong>g heated <strong>egg</strong>affects the natural history of <strong>egg</strong> <strong>allergy</strong> when compared <strong>with</strong>strict avoidance. Until such studies are completed, there rema<strong>in</strong>s<strong>in</strong>sufficient evidence to rout<strong>in</strong>ely advise the <strong>in</strong>troduction ofheated <strong>egg</strong> <strong>in</strong>to the diet of those undertak<strong>in</strong>g strict avoidance.We thank Drs Er<strong>in</strong> Thanik, Julie Wang, and Jennifer Maloney for subjectreferrals; Sheila Walsh, Beth Rob<strong>in</strong>son, and Jessica Chao for researchcoord<strong>in</strong>ation; Shideh Mofidi and Marissa Sherry for nutritional management;Ramon Bencharitiwong and Michelle Mishoe for laboratory technical assistance;Dr Jon Medd<strong>in</strong>gs (University of Alberta, Edmonton, Canada) for<strong>in</strong>test<strong>in</strong>al permeability assessment; and Dr Jim Godbold from the Mount S<strong>in</strong>aiSchool of Medic<strong>in</strong>e Department of Biostatistics and the General Cl<strong>in</strong>icalResearch Center for assistance <strong>with</strong> statistical analysis.Cl<strong>in</strong>ical implications: The majority of <strong>children</strong> <strong>with</strong> <strong>egg</strong> <strong>allergy</strong>might tolerate heated <strong>egg</strong>, but only an oral food challenge providesa def<strong>in</strong>itive diagnosis. Further studies are needed to evaluatethe effect of a heated <strong>egg</strong> diet on the resolution of <strong>egg</strong><strong>allergy</strong>.REFERENCES1. Sicherer SH, Sampson HA. 9. Food <strong>allergy</strong>. J Allergy Cl<strong>in</strong> Immunol 2006;117(suppl):S470-5.2. Eggesbo M, Botten G, Halvorsen R, Magnus P. The prevalence of <strong>allergy</strong> to <strong>egg</strong>: apopulation-based study <strong>in</strong> young <strong>children</strong>. Allergy 2001;56:403-11.3. Sampson HA, McCaskill CC. Food hypersensitivity and atopic dermatitis: evaluationof 113 patients. J Pediatr 1985;107:669-75.4. Eigenmann PA, Sicherer SH, Borkowski TA, Cohen BA, Sampson HA. Prevalenceof IgE-mediated food <strong>allergy</strong> among <strong>children</strong> <strong>with</strong> atopic dermatitis. Pediatrics1998;101:e8.5. Wood RA. The natural history of food <strong>allergy</strong>. Pediatrics 2003;111:1631-7.6. Savage JH, Matsui EC, Skripak JM, Wood RA. The natural history of <strong>egg</strong> <strong>allergy</strong>. JAllergy Cl<strong>in</strong> Immunol 2007;120:1413-7.7. Cooke SK, Sampson HA. Allergenic properties of ovomucoid <strong>in</strong> man. J Immunol1997;159:2026-32.8. Jarv<strong>in</strong>en KM, Beyer K, Vila L, Bard<strong>in</strong>a L, Mishoe M, Sampson HA. Specificity ofIgE antibodies to sequential epitopes of hen’s <strong>egg</strong> ovomucoid as a marker for persistenceof <strong>egg</strong> <strong>allergy</strong>. Allergy 2007;62:758-65.9. Bernhisel-Broadbent J, D<strong>in</strong>tzis HM, D<strong>in</strong>tzis RZ, Sampson HA. Allergenicity andantigenicity of chicken <strong>egg</strong> ovomucoid (Gal d III) compared <strong>with</strong> ovalbum<strong>in</strong>(Gal d I) <strong>in</strong> <strong>children</strong> <strong>with</strong> <strong>egg</strong> <strong>allergy</strong> and <strong>in</strong> mice. J Allergy Cl<strong>in</strong> Immunol 1994;93:1047-59.10. Hoffman DR. Immunochemical identification of the allergens <strong>in</strong> <strong>egg</strong> white. J AllergyCl<strong>in</strong> Immunol 1983;71:481-6.11. Holen E, Elsayed S. Characterization of four major allergens of hen <strong>egg</strong>-white byIEF/SDS-PAGE comb<strong>in</strong>ed <strong>with</strong> electrophoretic transfer and IgE-immunoautoradiography.Int Arch Allergy Appl Immunol 1990;91:136-41.12. Joo K, Kato Y. Assessment of allergenic activity of a heat-coagulated ovalbum<strong>in</strong>after <strong>in</strong> vivo digestion. Biosci Biotechnol Biochem 2006;70:591-7.13. Deutsch HF, Morton JI. Immunochemical properties of heated ovomucoid. ArchBiochem Biophys 1956;64:19-25.14. Urisu A, Ando H, Morita Y, Wada E, Yasaki T, Yamada K, et al. Allergenic activityof heated and ovomucoid-depleted <strong>egg</strong> white. J Allergy Cl<strong>in</strong> Immunol 1997;100:171-6.15. Des RA, Nguyen M, Paradis L, Primeau MN, S<strong>in</strong>ger S. Tolerance to cooked <strong>egg</strong> <strong>in</strong>an <strong>egg</strong> allergic population. Allergy 2006;61:900-1.16. Eigenmann PA. Anaphylactic reactions to raw <strong>egg</strong>s after negative challenges <strong>with</strong>cooked <strong>egg</strong>s. J Allergy Cl<strong>in</strong> Immunol 2000;105:587-8.17. Knight AK, Shreffler WG, Sampson HA, Sicherer SH, Noone S, Mofidi S, et al.Sk<strong>in</strong> prick test to <strong>egg</strong> white provides additional diagnostic utility to serum <strong>egg</strong>
J ALLERGY CLIN IMMUNOLVOLUME 122, NUMBER 5LEMON-MULÉ ET AL 983white-specific IgE antibody concentration <strong>in</strong> <strong>children</strong>. J Allergy Cl<strong>in</strong> Immunol2006;117:842-7.18. Boyano-Mart<strong>in</strong>ez T, Garcia-Ara C, Diaz-Pena JM, Mart<strong>in</strong>-Esteban M. Predictionof tolerance on the basis of quantification of <strong>egg</strong> white-specific IgE antibodies <strong>in</strong><strong>children</strong> <strong>with</strong> <strong>egg</strong> <strong>allergy</strong>. J Allergy Cl<strong>in</strong> Immunol 2002;110:304-9.19. Sampson HA, Ho DG. Relationship between food-specific IgE concentrations andthe risk of positive food challenges <strong>in</strong> <strong>children</strong> and adolescents. J Allergy Cl<strong>in</strong>Immunol 1997;100:444-51.20. Sampson HA. Utility of food-specific IgE concentrations <strong>in</strong> predict<strong>in</strong>g symptomaticfood <strong>allergy</strong>. J Allergy Cl<strong>in</strong> Immunol 2001;107:891-6.21. Sporik R, Hill DJ, Hosk<strong>in</strong>g CS. Specificity of allergen sk<strong>in</strong> test<strong>in</strong>g <strong>in</strong> predict<strong>in</strong>gpositive open food challenges to milk, <strong>egg</strong>, and peanut <strong>in</strong> <strong>children</strong>. Cl<strong>in</strong> ExpAllergy 2000;30:1540-6.22. Verstege A, Mehl A, Rol<strong>in</strong>ck-Wern<strong>in</strong>ghaus C, Staden U, Nocon M, Beyer K, et al.The predictive value of the sk<strong>in</strong> prick test weal size for the outcome of oral foodchallenges. Cl<strong>in</strong> Exp Allergy 2005;35:1220-6.23. A health professional’s guide to food challenges. Fairfax (VA): The Food Allergyand Anaphylaxis Network; 2004.24. Bock SA, Sampson HA, Atk<strong>in</strong>s FM, Zeiger RS, Lehrer S, Sachs M, et al. Doublebl<strong>in</strong>d,placebo-controlled food challenge (DBPCFC) as an office procedure: a manual.J Allergy Cl<strong>in</strong> Immunol 1988;82:986-97.25. Sicherer SH. Food <strong>allergy</strong>: when and how to perform oral food challenges. PediatrAllergy Immunol 1999;10:226-34.26. Dupont C, Barau E, Molkhou P, Raynaud F, Barbet JP, Dehenn<strong>in</strong> L. Food-<strong>in</strong>ducedalterations of <strong>in</strong>test<strong>in</strong>al permeability <strong>in</strong> <strong>children</strong> <strong>with</strong> cow’s milk-sensitive enteropathyand atopic dermatitis. J Pediatr Gastroenterol Nutr 1989;8:459-65.27. Bresl<strong>in</strong> NP, Nash C, Hilsden RJ, Hershfield NB, Price LM, Medd<strong>in</strong>gs JB, et al.Intest<strong>in</strong>al permeability is <strong>in</strong>creased <strong>in</strong> a proportion of spouses of patients <strong>with</strong>Crohn’s disease. Am J Gastroenterol 2001;96:2934-8.28. Sampson HA. Anaphylaxis and emergency treatment. Pediatrics 2003;111:1601-8.29. American College of Allergy, Asthma & Immunology. Food <strong>allergy</strong>: a practice parameter.Ann Allergy Asthma Immunol 2006;96(suppl):S1-68.30. Thomas K, Herouet-Guicheney C, Ladics G, Bannon G, Cockburn A, Crevel R,et al. Evaluat<strong>in</strong>g the effect of food process<strong>in</strong>g on the potential human allergenicityof novel prote<strong>in</strong>s: <strong>in</strong>ternational workshop report. Food Chem Toxicol 2007;45:1116-22.31. Teuber SS. Hypothesis: the prote<strong>in</strong> body effect and other aspects of food matrixeffects. Ann N Y Acad Sci 2002;964:111-6.32. Kato Y, Watanabe H, Matsuda T. Ovomucoid rendered <strong>in</strong>soluble by heat<strong>in</strong>g <strong>with</strong>wheat gluten but not <strong>with</strong> milk case<strong>in</strong>. Biosci Biotechnol Biochem 2000;64:198-201.33. Nowak-Wegrzyn A, Bloom KA, Sicherer SH, Shreffler WG, Noone S, Wanich N,et al. Tolerance to extensively heated milk <strong>in</strong> <strong>children</strong> <strong>with</strong> cow’s milk <strong>allergy</strong>. JAllergy Cl<strong>in</strong> Immunol 2008;122:342-7.34. Beyer K, Morrow E, Li XM, Bard<strong>in</strong>a L, Bannon GA, Burks AW, et al. Effects ofcook<strong>in</strong>g methods on peanut allergenicity. J Allergy Cl<strong>in</strong> Immunol 2001;107:1077-81.35. Maleki SJ, Chung SY, Champagne ET, Raufman JP. The effects of roast<strong>in</strong>g on theallergenic properties of peanut prote<strong>in</strong>s. J Allergy Cl<strong>in</strong> Immunol 2000;106:763-8.36. Carnes J, Ferrer A, Huertas AJ, Andreu C, Larramendi CH, Fernandez-Caldas E.The use of raw or boiled crustacean extracts for the diagnosis of seafood allergic<strong>in</strong>dividuals. Ann Allergy Asthma Immunol 2007;98:349-54.37. Patriarca G, Nucera E, Roncallo C, Pollastr<strong>in</strong>i E, Bartolozzi F, De Pasquale T, et al.Oral desensitiz<strong>in</strong>g treatment <strong>in</strong> food <strong>allergy</strong>: cl<strong>in</strong>ical and immunological results.Aliment Pharmacol Ther 2003;17:459-65.38. Taylor SL, Hefle SL, B<strong>in</strong>dslev-Jensen C, Atk<strong>in</strong>s FM, Andre C, Bruijnzeel-KoomenC, et al. A consensus protocol for the determ<strong>in</strong>ation of the threshold doses forallergenic foods: how much is too much? Cl<strong>in</strong> Exp Allergy 2004;34:689-95.39. Meglio P, Bartone E, Plantamura M, Arabito E, Giampietro PG. A protocol for oraldesensitization <strong>in</strong> <strong>children</strong> <strong>with</strong> IgE-mediated cow’s milk <strong>allergy</strong>. Allergy 2004;59:980-7.40. Buchanan AD, Green TD, Jones SM, Scurlock AM, Christie L, Althage KA, et al.Egg oral immunotherapy <strong>in</strong> nonanaphylactic <strong>children</strong> <strong>with</strong> <strong>egg</strong> <strong>allergy</strong>. J AllergyCl<strong>in</strong> Immunol 2007;119:199-205.41. Morisset M, Moneret-Vautr<strong>in</strong> DA, Guenard L, Cuny JM, Frentz P, Hatahet R, et al.Oral desensitization <strong>in</strong> <strong>children</strong> <strong>with</strong> milk and <strong>egg</strong> allergies obta<strong>in</strong>s recovery <strong>in</strong> asignificant proportion of cases. A randomized study <strong>in</strong> 60 <strong>children</strong> <strong>with</strong> cow’smilk <strong>allergy</strong> and 90 <strong>children</strong> <strong>with</strong> <strong>egg</strong> <strong>allergy</strong>. Allerg Immunol (Paris) 2007;39:12-9.
983.e1 LEMON-MULÉ ET ALJ ALLERGY CLIN IMMUNOLNOVEMBER 2008TABLE E1. Basel<strong>in</strong>e cl<strong>in</strong>ical characteristicsPatient characteristics Heated <strong>egg</strong> reactive Heated <strong>egg</strong> tolerant Egg tolerantTotal no. 27 (23%) 64 (57%) 23 (20%)Age (y), median (25th-75th <strong>in</strong>terquartile range) 5.9 (5.0-9.2) 6.0 (4.1-8.0) 6.3 (4.5-10.6)Male sex 23 (85%) 40 (63%) 14 (61%)AD, current 17 (63%) 33 (52%) 13 (57%)AD, resolved 7 (26%) 26 (41%) 9 (39%)Asthma 20 (74%) 35 (55%) 18 (78%)AR 23 (85%) 48 (75%) 19 (83%)Family history of atopy 22 (82%) 59 (92%) 21 (91%)Family history of <strong>egg</strong> <strong>allergy</strong> 3 (11%) 13 (20%) 2 (9%)Breast-fed exclusively 14 (52%) 43 (67%) 17 (74%)Time breast-fed (mo) 2 (1.5-7)* 6 (3-9) 6 (4.8-12)Age of first reaction (mo) 13 (12-24) 12 (10-36) 12 (11.3-32.3)Symptoms at first reactionCutaneous 18 (67%) 49 (77%) 12 (52%)UA 2 (7%) 9 (14%) 6 (29%)LA 0 (0%) 3 (3%) 2 (13%)GI 7 (26%) 11 (17%) 5 (22%)History of anaphylaxis to <strong>egg</strong> 2 (7%) 9 (13%) 3 (17%)History of EW-specific IgE >95% predictive of cl<strong>in</strong>ical reactivity 22 (81%) 35 (55%) 14 (61%)Never reacted to <strong>egg</strong> 5 (19%) 14 (22%) 8 (35%)Additional food allergies 26 (96%) 58 (91%) 23 (100%)Lifetime peak EW-specific IgE (kUA/L)ৠ15.4 (5.2-34.5) 6.0 (2.4-13.1) 5.9 (3.5-10.0)Time from peak EW-specific IgE to heated <strong>egg</strong> OFC (y)à 3.5 (2.6-4.8) 2.4 (1.0-4.3) 3.4 (2.2-7.2)Outgrown other food allergies 13 (48%) 17 (27%) 13 (57%)AD, Atopic dermatitis; AR, allergic rh<strong>in</strong>itis; Cutaneous (atopic dermatitis, urticaria, angioedema, pruritus, and rash); UA, upper airway (rh<strong>in</strong>orrhea, sneez<strong>in</strong>g, cough<strong>in</strong>g, and oralpruritus); LA, wheez<strong>in</strong>g; GI, gastro<strong>in</strong>test<strong>in</strong>al (nausea, vomit<strong>in</strong>g, diarrhea, and abdom<strong>in</strong>al pa<strong>in</strong>); EW, <strong>egg</strong> white; OFC, oral food challenge.*P 5 .037, heated <strong>egg</strong>–reactive versus <strong>egg</strong>-tolerant subjects.Egg white–specific IgE levels of greater than 2 kUA/L (age 2 years) or greater than 7 kUA/L (age >2 years).àNumbers expressed as medians (25th-75th <strong>in</strong>terquartile range).§P 5 .01.













