The Standard, Summer 2012 - College of Nurses of Ontario
The Standard, Summer 2012 - College of Nurses of Ontario
The Standard, Summer 2012 - College of Nurses of Ontario

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
www.cno.org/mymContact CNOUpdating your information is easier than ever!Visit the Maintain Your Membership section atwww.cno.org to:■ update your Register address■ complete membership renewal and payment■ access and complete the QA Program■ obtain a copy <strong>of</strong> your membership receiptOther resourcesEnquire about application, registrationor reinstatement matters:Customer Service Centrecno@cnomail.orgwww.cno.org/contactAsk a practice-related question:Practice Support Lineppd@cnomail.orgwww.cno.org/askVoice a concern about a nurse’sconduct:Reports and Complaintsinvestigations-intake@cnomail.orgwww.cno.org/protectSend comments to the Editor:<strong>The</strong> <strong>Standard</strong>editor@cnomail.orgwww.cno.org/standard<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong>101 Davenport Rd.Toronto, ON M5R 3P1Editor Deborah JonesManaging Editor Kristi GreenStaff Writers Eugenia Afolabi, Mitchell Brown,Bill Clarke, Tanya DaviesEditorial Associate Brooke BurnsPro<strong>of</strong>reader Roberts Ink CommunicationsContributorsAndrea Burck Decisions AdministratorJasmine Chatha InvestigatorBarbara Czerniawski, RN Outreach ConsultantAnthony Derro, RN Practice ConsultantMichael Hamilton-Jones Statistical AnalystMyra Kreick, RN Outreach ConsultantDama Lagman-Taruc AccountantLinda Levesque, RN Outreach ConsultantKatherine Smith, RN Outreach ConsultantEmily Zbieranowski Policy AnalystProduction Coordinator Susan AbrahamDesigner Paul BrandejsSubscriptions<strong>The</strong> subscription rate to members is included in theannual payment fee. Subscriptions for non-members are$22.60 (includes 13% HST) per year. U.S. subscriptionsare $22.60 per year. Other foreign and overseassubscriptions are $45.20 per year. <strong>The</strong> cost <strong>of</strong> anadditional copy <strong>of</strong> <strong>The</strong> <strong>Standard</strong> is $4.52, or $7.91 withinserts. Postage and handling charges are extra pleasecontact the <strong>College</strong> for more information.CirculationFor extra copies <strong>of</strong> an issue or missed issues, pleasecontact the Customer Service Centre at the address orphone number below.Advertising<strong>The</strong> views or opinions expressed in paid advertising arethose <strong>of</strong> the advertisers. Publication <strong>of</strong> paid advertisingin this magazine does not constitute <strong>College</strong> <strong>of</strong> <strong>Nurses</strong><strong>of</strong> <strong>Ontario</strong> endorsement <strong>of</strong>, or assumption <strong>of</strong> liability for,any claims made in the advertisement.For information about placing an advertisement,please contact Dovetail Communications Inc.Tel.: 905 886-6640<strong>The</strong> <strong>Standard</strong> is published four times a year by the<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong>. <strong>The</strong> editor welcomescomments and suggestions from readers.Email: editor@cnomail.org.ISSN 1708-9581L’Excellence est disponible en français.Copyright © <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong>, <strong>2012</strong>.Material published in <strong>The</strong> <strong>Standard</strong> may be reprintedwithout permission, provided that credit is given to thepublication and to the <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong>.<strong>The</strong> <strong>Standard</strong> is printed in Canada on recycled paper.It contains 50% recycled fibres, including 10% postconsumerwaste.Publications Mail Agreement 40062643Return undeliverable Canadian addresses to:<strong>The</strong> <strong>Standard</strong><strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong>101 Davenport Rd.Toronto, ON M5R 3P1Tel.: 416 928-0900Toll-free in <strong>Ontario</strong>: 1 800 387-5526Fax: 416 928-6507Website: www.cno.org416 928-09001 800 387-5526 (toll-free in <strong>Ontario</strong>)cno@cnomail.orgwww.cno.org
A Message from the President & Executive directorvisionLeading in regulatoryexcellencemissionRegulating nursing inthe public interestCollaboration andinnovation buildregulatory excellenceRegulating a pr<strong>of</strong>ession as large and diverse as nursing in today’s complex world requiresrobust regulatory processes and a commitment to the public interest.To excel, regulators also need to establish and nurture strong strategic partnerships andseek innovative approaches to regulatory processes.In 2011, the <strong>College</strong> provided leadership in the formation <strong>of</strong> new national organizations:■ All 12 Canadian RN regulators joined together to establish the CCRNR(Canadian Council <strong>of</strong> Registered Nurse Regulators). <strong>The</strong> CCRNR will fosterthe sharing <strong>of</strong> regulatory best practices, support collaborative initiatives andserve as a national voice for nursing’s commitment to public safety.■ <strong>The</strong> National Nursing Assessment Service will provide a consistent, centralizedapplication and assessment process for nurses from outside <strong>of</strong> Canada applyingfor registration in any Canadian jurisdiction. It will enhance fairness, access andinterprovincial mobility while maintaining a high standard for public safety.In the <strong>College</strong>’s recently released 2011 Annual Report you will find other examples <strong>of</strong>provincial, national and international collaborative initiatives that support us in meetingour regulatory commitments in new and exciting ways.<strong>The</strong> report also includes many examples <strong>of</strong> forward-thinking approaches to regulatoryprocesses. New opportunities have been created for nurses and employers to talk withus about accountability and the application <strong>of</strong> standards. <strong>The</strong> result is an enrichedunderstanding <strong>of</strong> regulation and practice realities with our stakeholders that will have alasting effect on the quality <strong>of</strong> care.We are a leader in using technology to improve and streamline our processes withnurses. For example, we are the first health regulator in <strong>Ontario</strong> to require members torenew their membership online. Not only is online renewal efficient and cost-effective, itis also essential to meeting our regulatory commitment to provide detailed data to supportthe government in health human resource planning.As the regulatory body for nurses, the <strong>College</strong> provides nurses with guidance andsupport (such as in the application <strong>of</strong> practice standards and about what constitutespr<strong>of</strong>essional misconduct) and acts on behalf <strong>of</strong> the pr<strong>of</strong>ession in the public interest. Eachnurse, by embracing her or his accountability to practise in accordance with our standards,supports public confidence in the nursing pr<strong>of</strong>ession and in its <strong>College</strong>.Download the annual report or watch a webcast <strong>of</strong> it at www.cno.org/annualreport.Kris Voycey, RNPresidentAnne Coghlan, RN, MScNExecutive Director and CEO6 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
NEWSAct addresses abuse<strong>The</strong> new Retirement Homes Act, 2010requires nurses working in retirementhomes to have increased awarenessabout what constitutes abuse.<strong>The</strong> new Act clearly outlines differentforms <strong>of</strong> abuse: emotional, sexual, verbal,physical and financial.“<strong>The</strong> Retirement Homes Act, 2010aligns the standards for care in <strong>Ontario</strong>’sretirement homes with the standardscurrently in place for other facilities,such as long-term care,” says KatherineSmith, RN, Outreach Consultant. “<strong>The</strong>Act spells out retirement home operators’obligation to provide employees withtraining to help them identify and preventclient abuse.”<strong>The</strong> Act also requires retirement homeoperators to adopt zero-tolerance policiesfor all forms <strong>of</strong> client abuse. Operatorsare expected to develop procedures forinvestigating allegations <strong>of</strong> abuse andto identify penalties for those who haveabused clients.As the Outreach Consultant for the longtermcare, retirement home and palliativecare sector, Smith builds awareness <strong>of</strong><strong>College</strong> practice documents amongpractising nurses. <strong>The</strong> <strong>The</strong>rapeutic Nurse-Client Relationship, Revised 2006, Ethicsand Restraints documents can helpnurses recognize client abuse and takesteps to stop it. <strong>The</strong> <strong>College</strong> also <strong>of</strong>fersan abuse prevention program, One isOne Too Many, which includes a DVDand self-study workbook.<strong>Nurses</strong> working in retirement homes areurged to familiarize themselves with thenew Act, which can be found on theLegislative Assembly <strong>of</strong> <strong>Ontario</strong>’s website,http://www.ontla.on.ca. SExecutive Directorleads RN council<strong>The</strong> Executive Director and CEO <strong>of</strong> the<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> has beenelected the first president <strong>of</strong> the CCRNR(Canadian Council <strong>of</strong> Registered NurseRegulators).“It is an honour to be elected aspresident,” says Anne Coghlan, RN. “<strong>The</strong>CCRNR’s members share a long history<strong>of</strong> collaborating effectively with eachother. Formalizing our commitment toexcellence in nursing regulation is veryexciting.”Elected as vice-president is Karen Eisler,RN. Eisler is the executive director <strong>of</strong>the Saskatchewan Registered <strong>Nurses</strong>’Association.Last year, 12 Canadian nursing regulatorybodies formed the CCRNR to act as anational forum and unified voice oninterprovincial, national and internationalregulatory matters. <strong>The</strong> council promotesbest practices, harmonizes approachesto nursing regulation, monitors trends,identifies issues related to nursingregulation and undertakes projects thatpromote excellence in nursing regulation.For more information on CCRNRactivities, see the spring <strong>2012</strong> issue <strong>of</strong><strong>The</strong> <strong>Standard</strong>, email info@ccrnr.ca or call613 447-5253. S8 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
news You can useNew RN entry-topracticeexamLast December, the <strong>College</strong> joined nineother Canadian RN regulators in makinga decision to move to a state-<strong>of</strong>-the-art,computerized exam for RN applicants.Beginning in 2015, applicants forregistration with the <strong>College</strong> will writethe NCLEX ® -RN exam. <strong>The</strong> exam willassess Canadian entry-to-practicecompetencies and continue to supportthe <strong>College</strong>’s accountability to ensurethat individuals entering the nursingpr<strong>of</strong>ession are competent to provide safenursing care to the <strong>Ontario</strong> public.<strong>The</strong> <strong>College</strong> is excited about theopportunity to lead an innovation inregulation and engage new members inembracing advances in technology.<strong>The</strong> new exam has many advantages forwriters, such as allowing them to writethe exam at any time <strong>of</strong> the year andreceiving exam results more quickly. Inaddition, the exam is highly secure andcost-effective because it uses the mostadvanced testing technology.Over the next few years, many RNs willhave opportunities to contribute theirknowledge and expertise to the exam bywriting questions, reviewing questionsfor cultural or language bias, andparticipating in practice analyses.In the coming months, the <strong>College</strong>will engage with educators to ensurethat students have the information andresources they need to prepare for theexam. For more information, read theQ&As at www.cno.org/newRNexam. SResults fromthe<strong>2012</strong>Councilelection are in!New Council membershave been elected inthe Southwestern,Central Western andCentral/Toronto districts.Visitwww.cno.org/electionsto see the results.QAGo onlineto the<strong>2012</strong>Watch the tutorial and learn howto create, save and review your learning goalsin one secure place.ProgramGo to www.cno.org/qa for all your QA tools andresources, including FAQs, sample learning goals anda webcast.<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>9
Feature<strong>The</strong> following scenarios provide guidance on three differentcommunication issues.SCENARIO 1: Non-verbal cuesWhenever Ricki, a novice nurse, comments at care reviewsessions, Karla, a more experienced nurse, turns away orstarts working on something else. Eventually, Ricki stopsspeaking up.As a more experienced nurse, Karla might feel she doesn’tneed to listen to new nurses’ feedback. However, as amentor, she can help new staff integrate into the practicesetting. Karla’s use <strong>of</strong> non-verbal communication is opento misinterpretation — in this case, it is counterproductiveto the team’s goals because it makes Ricki feel devalued,thus decreasing communication among team members.Feedback is also important for effective communicationto occur. In this case, Ricki must give feedback immediatelyinstead <strong>of</strong> burying hurt feelings. Buried feelings can worsenover time and will hinder the health care team’s ability toprovide the best possible client care. First, Ricki shouldbring her concern to Karla. If that doesn’t help, then sheshould discuss it with a nurse leader who might be able tohelp Karla reflect on how her behaviour affects others.Bibi F. Verwayne, RN, who practises at AlexanderPlace in Waterdown, has seen how vague non-verbalcues can create misunderstanding in a group. “A groupcannot be successful if members do not feel comfortableenough to share and know that they will be heard andappreciated,” she explains. “A team that practises goodcommunication allows everyone to share ideas and providefeedback, knowing that failure to do so leads to conflict,misunderstanding and poor client or staff outcomes.”See the Pr<strong>of</strong>essional <strong>Standard</strong>s, Revised 2002 practicedocument for information about establishing andmaintaining collegial relationships.SCENARIO 2: Systems supportA long-term care unit is transitioning to an electronicdocumentation system. During the transition, nurses use bothpaper and electronic client records. However, the nurses feelthat client information may be lost with this dual system.Communication problems can result from ineffectivesupport systems such as outdated or conflicting policiesand processes. In this situation, nurses can advocate byspeaking to colleagues in leadership positions to helpdevelop policies and procedures to address their concerns.For instance, a new interim policy could require nursesto write on the paper chart when they have electronicallyrecorded part <strong>of</strong> a client’s health information, and viceversa. <strong>The</strong> long-term goal would be to have an integratedhealth record system to avoid duplication.<strong>The</strong> responsibility for preventing or solving this type<strong>of</strong> communication breakdown does not lie solely withthe individuals involved. “It is more complex than that,”Nadine Janes, RN, explains. “Success is achieved througha combination <strong>of</strong> good communication practices betweennurses and other health care pr<strong>of</strong>essionals, and supportfrom structure and systems provided by the facility throughemployers and nurses in formal leadership positions.”SCENARIO 3: Language barriersA client who speaks only Spanish likes the light in his roomturned <strong>of</strong>f during the day, but the nurses leave it on.When one nurse notices that the client is trying to tell hersomething, she asks the client’s son to translate. However,the son is reluctant to tell the nurse because he is concernedabout <strong>of</strong>fending her.When a client is unable to speak for himself during theprovision <strong>of</strong> care, it reflects an imbalance in power andaffects the therapeutic relationship. <strong>The</strong> Culturally SensitiveCare practice document provides guidelines for dealing withchallenges nurses can face in multicultural or multilingualpractice settings. For instance, when language barriers exist,nurses can use non-verbal communication such as gestures,pictures, body language that shows openness, and vocaltones that convey warmth and compassion.To resolve this situation, the nurse should approachthe son in an open manner. She could emphasize herwillingness to understand what his father is trying to say,or if the son prefers, the nurse should find an interpreterfor them. Once she has clarified the client’s wishes, thenurse should share them with the other nurses and includea note in his plan <strong>of</strong> care.Louise Carreau, RN, regularly deals with English- andFrench-speaking clients and their families in the complexcare setting. “Language barriers can impact the therapeuticrelationship when a client fears that the caregiver does notunderstand them,” says Carreau.She adds, “When clients become incapable, familymembers or substitute decision-makers may take over. Thismakes it harder to have a ‘direct’ therapeutic relationshipwith the client. In such situations, if a nurse notices thatthe client’s best interest may be at risk, the nurse shouldnot be afraid to speak out and advocate on behalf <strong>of</strong> theclient based on the plan <strong>of</strong> care.” SHave a comment about this article?Send an email to editor@cnomail.org.<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>13
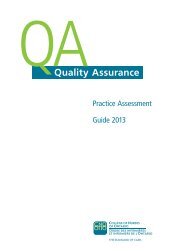
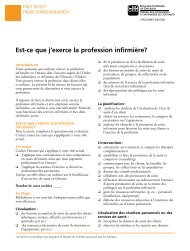
FeatureSurvey Says...<strong>Nurses</strong> weigh in on social mediaand pr<strong>of</strong>essionalism.A growing number <strong>of</strong> nurses use social media forpr<strong>of</strong>essional purposes such as networking, informationsharingand pr<strong>of</strong>essional development.This past spring, the <strong>College</strong> conducted a surveyto explore nurses’ use <strong>of</strong> social media and its effect ontheir practice and pr<strong>of</strong>essionalism. A total <strong>of</strong> 711 nursesparticipated in the survey. Participants included nurseswho work in the community and public health, acute care,academia and paediatric practice sectors.<strong>The</strong> <strong>College</strong> first explored members’ use <strong>of</strong> socialmedia in a 2008 survey, which focused on personaland pr<strong>of</strong>essional use. Since then, these means <strong>of</strong> socialinteraction have become increasingly popular. (See Figure 1on page 15 to see how many nurses currently report usingsocial media and for what purpose.)“Since the initial survey in 2008, we have beenexploring avenues for educating nurses aboutpr<strong>of</strong>essionalism while using social media,” says BarbaraCzerniawski, RN, Outreach Consultant for the academicand paediatric sectors. “We hope this survey will give usideas for developing new ways to support nurses so theycan maintain their regulatory obligations when usingsocial media.”Myth-buster<strong>The</strong> survey challenged the myth that interest in socialmedia is exclusive to younger people. While it’s notsurprising that younger nurses in the survey sample(88 per cent <strong>of</strong> 18- to 24-year-olds) reported using socialWhat is social media?Social media is a set <strong>of</strong> web-based andmobile technologies that allow peopleto monitor, create, share or manipulatetext, audio, photos or video, with others.Examples include Facebook, Twitter,Google+, Blogs and LinkedIn.Source: Canadian Medical Association. (2011). Social mediaand Canadian physicians - issues and rules <strong>of</strong> engagement.Retrieved May 1, <strong>2012</strong>, from http://www.cma.ca/advocacy/social-media-canadian-physicians.14 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
FeatureFigure 1: Do you use any social media?media, it is noteworthy that social media is used by67 per cent <strong>of</strong> nurses who are aged 55 years or older. Ofthe nurses who use social media, more than 50 per centsaid it is either critical or important to their practice.<strong>Nurses</strong> use social media for a variety <strong>of</strong> purposessuch as researching information, education and healthpromotion. However, nurses in the community and publichealth sectors are more likely to use social media for clienteducation, health promotion, debriefing colleagues andconsulting nursing specialists, than they are for research.Myra Kreick, RN, Outreach Consultant for thecommunity and public health sector, is not entirelysurprised by this finding. “Social media fits nicely withthe role <strong>of</strong> nurses in community and public health, whosepractice focuses on health promotion, protection andpreservation. <strong>The</strong>y use it for support programs, suchas smoking cessation, and as a communication optionwhen working with youth, families or hard-to-reachpopulations.”Maintaining public confidenceMany <strong>of</strong> the nurses said they were mindful <strong>of</strong> howinformation they post online might affect the public’sperception <strong>of</strong> the nursing pr<strong>of</strong>ession.“It is important for this attitude to extend beyondusing social media for pr<strong>of</strong>essional purposes,” says LindaLevesque, RN, Outreach Consultant for the acutecare — adult sector. “Even when using it for personalpurposes, nurses should pay particular attention to howtheir online conduct can impact their pr<strong>of</strong>essional image,employer reputation and collegial relationships.”Czerniawski agrees, “As regulated pr<strong>of</strong>essionals, nurseshave a responsibility to protect the public interest byavoiding social media situations that could hinder thepublic’s trust and respect for the pr<strong>of</strong>ession. Misuse <strong>of</strong>social media could also have a negative impact on thetherapeutic nurse-client relationship.”Although not many <strong>of</strong> the nurses said they hadexperienced negative consequences from using socialmedia, there is general concern about its potential riskssuch as identity theft and breaching client or workplaceconfidentiality. Interestingly, 31 per cent indicated thatthey had observed another nurse using social mediain ways that caused them to question the other nurse’spr<strong>of</strong>essionalism.Yesfor personaland nursingpracticerelateduse31.4%Yesfor nursing practicerelateduse only2.5%No22.4%Yesfor personaluse only43.7%Social media support<strong>The</strong> <strong>College</strong>’s practice documents can be applied to socialmedia activities. <strong>The</strong>y contain information that can helpnurses make good decisions when using social media.<strong>The</strong>y also help nurses avoid making poor choices suchas breaching the confidentiality <strong>of</strong> client information orescalating workplace conflict.<strong>The</strong> nurses surveyed said they would apply the<strong>College</strong>’s practice documents to their use <strong>of</strong> socialmedia. In particular, they said the Confidentiality andPrivacy — Personal Health Information; Ethics; Pr<strong>of</strong>essional<strong>Standard</strong>s, Revised 2002; <strong>The</strong>rapeutic Nurse-ClientRelationship, Revised 2006 and Consent documents wereparticularly relevant. (See the fall 2011 issue <strong>of</strong> <strong>The</strong><strong>Standard</strong> for more information on using the standards inthe social media context.)In addition to these documents, nurses can look forguidance from their own workplace policies. Nearly 50per cent <strong>of</strong> the nurses surveyed said their workplaces haveorganizational policies related to personal and pr<strong>of</strong>essionaluse <strong>of</strong> social media. “<strong>Nurses</strong> who do not have thesepolicies should advocate for them,” says Levesque.<strong>The</strong> <strong>College</strong> is now working with the OutreachAdvisory Groups to examine how the practice documentsapply to social media activities. For more informationabout the Outreach Advisory Groups, visit www.cno.org/outreach. SHave a comment about this article?Send an email to editor@cnomail.org.<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>15
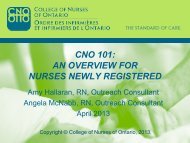
Feature<strong>College</strong> Fundsat WorkThis year, the $175.15 ($155 + 13% HST) annualmembership fee that renewing members pay accountsfor approximately 77 per cent <strong>of</strong> the <strong>College</strong>’s revenue.<strong>The</strong> <strong>College</strong> uses your membership fee and revenuegenerated from other sources (such as application feesand advertisements in <strong>The</strong> <strong>Standard</strong>) to guide thepr<strong>of</strong>ession, protect the public and complete other workrequired by legislation. This includes assessing andregistering applicants, developing practice documents,<strong>College</strong> expenses for <strong>2012</strong>Council and Committees (1%)Supports the cost <strong>of</strong> Council and committee meetings andelections.Executive Office (3%)Provides strategic leadership to <strong>College</strong> operations, andsupport to Council and committees.Practice and Regulatory Policy (11%)Develops and articulates standards <strong>of</strong> practice and entryto-practicecompetencies, and provides policy support onregulatory issues. Provides member consultation services.Administers the QA Program.Pr<strong>of</strong>essional Conduct (20%)Responds to issues about nurses’ practice, conduct orhealth via resolution or investigation processes, andsupports the prosecution <strong>of</strong> the most serious cases <strong>of</strong>pr<strong>of</strong>essional misconduct at public discipline hearings.Monitors compliance with committee orders and ensuresthat the <strong>College</strong>’s register is up-to-date.and administering a QA (Quality Assurance) Programand other programs that provide information aboutpractice and address concerns about conduct.In <strong>2012</strong>, a portion <strong>of</strong> <strong>College</strong> resources will beallotted to preparing for the implementation <strong>of</strong> therevised Registration Regulation and the jurisprudenceexamination. See the pie charts on page 17 for abreakdown <strong>of</strong> <strong>2012</strong> revenues and <strong>College</strong> expenses. SKnowledge Management (21%)Generates and shares knowledge, includingcommunication with members, employers, the public andthe media through publications and the website. Maintainsthe <strong>College</strong>’s records, produces membership statistics andconducts statistical analyses. Implements and maintainsthe s<strong>of</strong>tware and technological infrastructure to support<strong>College</strong> functions.Applicant Services (22%)Assesses applicants, administers examinations and registersthose who qualify.Corporate Services (22%)Provides customer service to members, applicantsand the public. Supports <strong>College</strong> operations throughbuilding maintenance, finance, <strong>of</strong>fice services, hearings,administration and human resources.16 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
Feature<strong>2012</strong> revenues <strong>College</strong> expensesExecutive<strong>of</strong>fice3%Interestincome1%Membership fees77%Applicantservices22%Corporateservices22%Applicantfees20%Pr<strong>of</strong>essionalconduct20%Knowledgemanagement21%Practice andregulatorypolicy11%Salesrevenue1%Otherrevenue1%Council andcommittees1%CONTRIBUTE TO NURSING REGULATIONJoinan OutreachADVISORYGroup<strong>The</strong> <strong>College</strong> will be looking for nurses to participate inits Advisory Groups.Each group focuses on regulatory issues based onpractice sectors.Visit www.cno.org/outreach for details.<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>17
Annual Report SummaryReport <strong>of</strong> the Independent Auditor on theSummary Financial StatementsTo the Council <strong>of</strong> the<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong><strong>The</strong> accompanying summary financial statements, which comprise the summary statement <strong>of</strong> financial positionas at December 31, 2011, the summary statement <strong>of</strong> operations and summary statement <strong>of</strong> changes in net assetsfor the year then ended, and related note, are derived from the audited financial statements <strong>of</strong> the <strong>College</strong> <strong>of</strong><strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> for the year ended December 31, 2011. We expressed an unmodified audit opinion on thosefinancial statements in our report dated June 7, <strong>2012</strong>.<strong>The</strong> summary financial statements do not contain all the disclosures required by Canadian accountingstandards for not-for-pr<strong>of</strong>it organizations. Reading the summary financial statements, therefore, is not asubstitute for reading the audited financial statements <strong>of</strong> the <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong>.Management’s Responsibility for the Summary Financial StatementsManagement is responsible for the preparation <strong>of</strong> a summary <strong>of</strong> the audited financial statements on the basisdescribed in the note to the summary financial statements.Auditor’s ResponsibilityOur responsibility is to express an opinion on the summary financial statements based on our procedures,which were conducted in accordance with Canadian Auditing <strong>Standard</strong> (CAS) 810, “Engagements to Report onSummary Financial Statements”.OpinionIn our opinion, the summary financial statements derived from the audited financial statements <strong>of</strong> the <strong>College</strong><strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> for the year ended December 31, 2011 are a fair summary <strong>of</strong> those financial statements, onthe basis described in the note to the summary financial statements.Toronto, <strong>Ontario</strong>June 7, <strong>2012</strong>Chartered AccountantsLicensed Public Accountants18 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
Annual Report SummarySummary Statement <strong>of</strong> Financial PositionDecember 31 2011 2010$ $ASSETSCurrent AssetsCash 10,386,976 13,861,699Investments 11,694,521 11,632,122Sundry receivables 157,228 156,328Prepaid expenses 279,046 307,97222,517,771 25,958,121Investments 8,898,586 1,834,147Capital assets 8,935,069 8,643,735Intangible assets 1,113,010 1,302,26918,946,665 11,780,151LIABILITIES41,464,436 37,738,272Current LiabilitiesAccounts payable and accrued liabilities 4,947,803 3,530,451Deferred membership and examination fees 23,341,074 17,250,16328,288,877 20,780,614Accrued pension liability 186,064 408,51128,474,941 21,189,125NET ASSETSInvested in capital and intangible assets 10,048,079 9,946,004Unrestricted 2,941,416 6,603,14312,989,495 16,549,14741,464,436 37,738,272<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong> 19
Annual Report SummarySummary Statement <strong>of</strong> OperationsYear ended December 31 2011 2010$ $RevenuesMembership fees 19,833,788 19,521,840Credential evaluations, endorsements and transcripts 2,645,321 1,530,154Examinations 4,118,724 3,224,032Publications 328,309 364,721Investment income 354,219 595,837Other 252,789 244,85427,533,150 25,481,438ExpensesPractice and regulatory policy 5,332,249 5,258,387Pr<strong>of</strong>essional conduct 6,577,208 5,535,922Council and committees 187,894 329,294Executive 1,849,123 1,893,192Knowledge management 5,950,778 6,003,007Corporate services 11,195,550 9,908,87131,092,802 28,928,673Excess <strong>of</strong> expenses over revenues for year (3,559,652) (3,447,235)Summary Statement <strong>of</strong> Changes in Net AssetsYear ended December 31Invested inCapital and20112010Intangible Assets$Unrestricted$Total$Total$Balance, beginning <strong>of</strong> year 9,946,004 6,603,143 16,549,147 19,996,382Excess <strong>of</strong> expenses over revenues foryear (1,301,719) (2,257,933) (3,559,652) (3,447,235)Purchase <strong>of</strong> capital assets 1,120,323 (1,120,323) - -Purchase <strong>of</strong> intangible assets 283,471 (283,471) - -Balance, end <strong>of</strong> year 10,048,079 2,941,416 12,989,495 16,549,147Note to Summary Financial StatementsDecember 31, 20111. Basis <strong>of</strong> presentation<strong>The</strong>se summary financial statements have been prepared from the audited financial statements <strong>of</strong> the<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> (the “<strong>College</strong>”) for the year ended December 31, 2011, on a basis that isconsistent, in all material respects, with the audited financial statements <strong>of</strong> the <strong>College</strong> and reduces cashflow information and information disclosed in the notes to the financial statements.Complete audited financial statements are available upon request from the <strong>College</strong>.20 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
Councilmeetings<strong>The</strong> draft minutes <strong>of</strong>the June Council meetingwill be posted atwww.cno.org/agendasin early July.Council meetings areAd removed forweb publishingopen to the public. Toattend, contact JennaH<strong>of</strong>bauer, Council AffairsCoordinator, at416 928-0900, ext. 7566;1 800 387-5526, ext. 7566(toll-free in <strong>Ontario</strong>); orjh<strong>of</strong>bauer@cnomail.org.Upcoming meetings:Sept. 27, <strong>2012</strong>Dec. 5, <strong>2012</strong>For more information onCouncil, visitwww.cno.org/council.
ToolsTo LearnToolsTo Succeed<strong>Nurses</strong> use a lot <strong>of</strong> tools in theirLearning ModulesOnline self-study sessions for reviewingpractice standards.Go nowAsk PracticeQuestions from nurses, answeredby nurses.Go nowTeleconferencesInteractive forums on importantnursing issues.Go nowAbuse PreventionVideos and study materials onstopping abuse.Go nowday-to-day practice, but perhapsnone is more important than theirability to learn.That’s why the <strong>College</strong> <strong>of</strong>fers avariety <strong>of</strong> educational tools to helpnurses better understand and testtheir knowledge <strong>of</strong> the practicedocuments.Visit www.cno.org/learning today
Ad removed forweb publishing
QuizQuiz answers from page 22No Delegation and directives are two different1 authorizing mechanisms. Delegation is a formalprocess by which a regulated health pr<strong>of</strong>essional withthe legislated authority and competence to perform acontrolled act procedure transfers the authority to performthe procedure to an individual who otherwise wouldnot have the authority to perform it. Delegation is onlyrequired if the directive includes a procedure that is notwithin the legal scope <strong>of</strong> nursing practice.A directive is an order for a number <strong>of</strong> clients whencertain conditions exist. Delegation provides the legalauthority to perform a controlled act, whereas an orderoutlines what to perform. Directives are always written,and they may or may not refer to delegation.Because RNs do not have the legislated authority todispense, they need delegation to acquire the authority,even if a directive is in place. According to the <strong>College</strong>,delegation and orders are two distinct authorizingmechanisms. However, not all health pr<strong>of</strong>ession acts(including medicine) make this distinction.Because RNs and RPNs do not have the authority toperform the controlled act <strong>of</strong> dispensing, they requiredelegation. So, RNs in this ED can use a directive toperform dispensing if they have also been delegated thiscontrolled act.Delegating and accepting delegation carry specificaccountabilities. See page 11 <strong>of</strong> the AuthorizingMechanisms practice document at www.cno.org/docs toreview your accountabilities for delegation.2No Orders for narcotics must be client-specific;therefore, directives cannot be used. Prescribing andadministering narcotics is subject to the Controlled Drugsand Substances Act, 1996 and Narcotic Control Regulations.<strong>The</strong> latter legislation defines a narcotic prescription as “anauthorization given by a practitioner that a stated amount<strong>of</strong> the narcotic be dispensed for the person named in theprescription.” Consequently, orders for narcotics must beclient-specific. A directive, which is used for a group <strong>of</strong>clients, does not fulfil the legislative requirements.To facilitate timely access to narcotics, Lucy couldconsider using a preprinted order form for narcotics.If a nurse receives an order for a narcotic by way <strong>of</strong> adirective, then the nurse should remind the prescriber <strong>of</strong>the requirement for a client-specific order.3Yes When a nurse transcribes a prescriptionin accordance with a directive, the nurse is notprescribing the medication. <strong>The</strong> directive is an orderfrom the physician or NP who authorized it and who isultimately responsible for the prescription. RNs and RPNsare not permitted to prescribe, but they can implement thedirective and transcribe the prescription.<strong>The</strong> nurses should work with members <strong>of</strong> the healthcare team to ensure that directives meet the <strong>College</strong>’sexpectations, and that prescriptions are transcribed ina manner that clearly identifies the directive, the nurseimplementing the directive and the prescribing physician.<strong>Nurses</strong> who implement directives are responsible forassessing clients to determine if the conditions in thedirective are met. <strong>Nurses</strong> must also have the knowledge,skill and judgment to implement the directive safely.4Yes <strong>The</strong> RN or RPN who administers themedication according to the directive is notprescribing it. Mark, the NP, is prescribing the drugthrough a directive. <strong>The</strong>refore, when the RNs and RPNsimplement Mark’s directive, they are assessing the clientto determine that the conditions and criteria specified inthe directive apply, and, if so, administering the vaccinein accordance with Mark’s order, which is in the form <strong>of</strong>a directive.If Mark authorizes the directive, he is not delegatingprescribing by doing so. Delegation is the transfer <strong>of</strong>authority to perform a controlled act from a regulatedhealth care pr<strong>of</strong>essional who has the legislated authority toperform the act to an individual without the authority.As the prescribing NP, Mark is responsible for thedirective. He needs to ensure that the directive isconsistent with the <strong>College</strong>’s expectations. (See theDirectives practice document at www.cno.org/docs.)<strong>The</strong>se expectations include specifying the clinicalconditions and circumstances that clients must meet, andidentifying any contraindications.<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>27
YouAskedUs<strong>The</strong> title “nurse”Dispensing drugsamplesCo-signingdocumentationTelepracticeoutside <strong>Ontario</strong>QI practise in a retirement homewhere I’m responsible forsupervising UCPs (unregulated careproviders). Recently, my employerpointed out that many <strong>of</strong> our clientsdon’t understand what a UCP is.To help these clients identify UCPsas caregivers, my employer askedme to instruct the UCPs to refer tothemselves as nurses. Should I tell theUCPs to call themselves nurses?ANo. In <strong>Ontario</strong>, only members<strong>of</strong> the <strong>College</strong> can use the titlenurse, Registered Nurse, RegisteredPractical Nurse or Nurse Practitioner.People who are not registeredwith the <strong>College</strong> and who refer tothemselves as nurses or attempt toobtain employment as nurses in<strong>Ontario</strong> are illegal practitioners. <strong>The</strong>ycan be prosecuted under the NursingAct, 1991 and Regulated HealthPr<strong>of</strong>essions Act, 1991.Appropriate use <strong>of</strong> the protectedtitle <strong>of</strong> nurse demonstrates nurses’accountability as regulated healthpr<strong>of</strong>essionals, and allows clients andthe public to hold nurses accountablefor their pr<strong>of</strong>essional conduct.Accountability is an essential aspect<strong>of</strong> pr<strong>of</strong>essional regulation, andnurses are accountable to the client,the <strong>College</strong> and their employer.Unregulated care providers are notregulated by a health regulatorycollege; they are accountable to theiremployer.For more information, read AnIntroduction to the Nursing Act, 1991at www.cno.org/docs.QI’m an RPN who just startedpractising at a walk-in clinic.During orientation, my employer saidthe clinic nurses dispense medicationsthrough delegation and orders fromphysicians. Some <strong>of</strong> these medicationsare samples <strong>of</strong> prescriptionmedications. Are nurses allowed todispense drug samples?A<strong>The</strong> Food and Drugs Act, 1985states that medication samplescan only be distributed to physicians,dentists, veterinary surgeons andpharmacists.If the physicians in your clinicagree that the nurses can dispensethe drug samples they have received,then the nurses may dispense themto clients when appropriate. However,the nurses also require delegationfrom the physicians before theycan dispense the medication. Thisis because RNs and RPNs are notauthorized to perform the controlledact <strong>of</strong> dispensing. In addition, RNsand RPNs need either a directclient order or a directive fromthe physician to dispense the drugsamples.As with any medication, nursesmust use their knowledge, skilland judgment to assess whether amedication is appropriate for a client.As well, the clinic must have systemsand structures in place that supportsafe medication practice.Under the Food and Drugsregulations, certain drugs cannotbe distributed as samples. <strong>The</strong>seinclude narcotics, controlled drugs28 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
Reflect on Pr<strong>of</strong>essional Conduct<strong>The</strong> <strong>College</strong> responds to concerns received from the public,employers and other sources through its complaints andreports processes. <strong>The</strong> goal is to enhance the quality <strong>of</strong>nursing care and ensure public protection by reinforcing the<strong>College</strong>’s standards <strong>of</strong> practice, and by providing nurses withopportunities to reflect on and improve their practice.This column is intended to help nurses understand and reflecton commonly raised concerns, as well as the <strong>College</strong>’s overallapproach to resolving those concerns.<strong>The</strong> scenarios are based on actual complaints or reports. Allnames, locations and identifying characteristics have beenchanged to protect confidentiality.A Facility Resolution<strong>The</strong> complaint<strong>The</strong> <strong>College</strong> received a letter from Sameena about nursesworking at the retirement home where her elderly motherhad been living for six months. Sameena wrote:It was hard for me to place my mother in a retirementhome. She has Alzheimer’s disease, which causes her to beforgetful and have emotional outbursts such as crying oryelling at people.When I told the nurse manager that I was very worriedthat my mother would be lonely and upset at the home, shesaid that I could participate in my mother’s care. She workedwith me to create a daily schedule for bathing and feeding herso that I could help the nurses with these duties.Unfortunately, many times when I arrive at the scheduledtime, I find that my mother has already been bathed or fed.Whenever I complain about this to a nurse, I’m told, “It’s hardfor staff to stick to the schedule.” No one has contacted me withan explanation or to reassure me that this problem will stop. Idon’t know why nurses can’t simply follow the schedule.<strong>The</strong> <strong>College</strong> respondsIn her letter to the <strong>College</strong>, Sameena did not name aspecific nurse or nurses. Instead, her concerns focused onthe nursing staff in general at the retirement home overa period <strong>of</strong> months. In addition to her worries about hermother’s care, Sameena felt that nurses had not addressedher concerns; they did not explain why her mother’sschedule wasn’t always followed or how they could preventthis problem from happening in the future.<strong>The</strong> <strong>College</strong> considered Sameena’s complaint to be30 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
Reflect on Pr<strong>of</strong>essional ConductQuestions:■■How would you have addressed Sameena’s concerns?Which indicators in the <strong>The</strong>rapeutic Nurse-Client Relationship, Revised2006 practice document could you use to improve this situation?suitable for its resolution program. This would involveSameena and the director <strong>of</strong> the retirement home signinga resolution agreement. <strong>The</strong> resolution agreement said thatthe <strong>College</strong> would hold an educational in-service sessionfor the nursing staff. This educational session wouldprovide the nurses with an opportunity to learn and reflecton their practice by specifically addressing the issues inSameena’s letter.<strong>The</strong> facility respondsSameena, the <strong>College</strong> and the director <strong>of</strong> the retirementhome entered into a resolution agreement together. <strong>The</strong>director believed that the <strong>College</strong>’s educational sessionwould give nurses an opportunity to reflect on theirpractice experience at the retirement home, and to sharestrategies for addressing challenging situations, such as theone Sameena described in her letter.Two representatives <strong>of</strong> the <strong>College</strong> visited the facility topresent an educational session, which approximately 25nurses and administrators attended. <strong>The</strong> representativesreviewed the <strong>College</strong>’s complaints process and thenursing issues that Sameena raised. <strong>The</strong>y also reviewedthe <strong>The</strong>rapeutic Nurse-Client Relationship, Revised 2006practice document, which was relevant to the issues.Finally, the representatives led the participants in areflective discussion about the complaint, focusing on howthe nursing issues relate to the practice standards.Reflecting on the complaintSeveral nurses reflected on the daily challenges they face intheir practice setting. <strong>The</strong>y described the retirement homeas being a unique facility where they juggle competingresponsibilities. For example, while nurses are usuallyassigned to care for specific residents, they <strong>of</strong>ten have toaddress urgent situations, such as when another residentexperiences a medical emergency. Also, some duties takelonger to perform than others, depending on each client’sneeds. Sometimes nurses acquire additional responsibilitiesif a colleague is away sick or when covering breaks. All<strong>of</strong> these factors make it difficult for nurses to followschedules exactly. <strong>The</strong> nurses also discussed how thesechallenges affect clients and family members.Following these reflections, the participants shared ideasabout how to meet the expectations <strong>of</strong> clients and theirfamily members, and address their concerns in a timelymanner. For this particular case, the nurses decided itwould help to meet with Sameena to discuss why nursescan’t always follow exact timelines for her mother’s bathingand feeding, and consider more flexible time frames.<strong>The</strong> <strong>College</strong> representatives examined the <strong>The</strong>rapeuticNurse-Client Relationship document with the participants,focusing on the key indicators for meeting the standards intheir particular practice setting. <strong>The</strong> nurses said that theyshould have communicated with Sameena immediatelyto address her concerns. <strong>The</strong>y agreed to be more aware<strong>of</strong> how their communication style is perceived by others.While many participants emphasized their commitmentto providing client-centred care on a daily basis, theysaid they sometimes underestimate the importance <strong>of</strong>establishing and maintaining therapeutic relationshipswith residents’ family members as well.Facility resolutions give nurses who work togetheran opportunity to reflect on their practice and sharetheir nursing expertise with each other. In this case, thenurses used Sameena’s complaint to develop strategies foraddressing similar situations in the future and to improvetheir overall practice. S<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong> 31
Ad removed forweb publishing
Ad removed forweb publishing
<strong>The</strong> followingdecisions and reasons<strong>of</strong> the DisciplineCommittee formpart <strong>of</strong> the <strong>College</strong>’sSummarizedDiscipline DecisionsAnnual Report and arepublished as a requirement <strong>of</strong>the Regulated Health Pr<strong>of</strong>essionsAct, 1991. By publishing thesedecisions, the <strong>College</strong> educatesnurses and informs the publicabout what constitutespr<strong>of</strong>essional misconduct andincompetence. <strong>The</strong>se decisionsalso provide direction to RNs,RPNs and NPs on practicestandards and pr<strong>of</strong>essionalbehaviour, if they findthemselves in similar situations.<strong>The</strong> name <strong>of</strong> the Member whois the subject <strong>of</strong> the hearingmay or may not be included,as required by law. Informationrevealing the names <strong>of</strong> witnessesand clients has been removed.For copies <strong>of</strong> full decisions,visit the website atwww.cno.org/decisions, orcontact Bill Clarke at1 800 387-5526, ext. 7590 (tollfreein <strong>Ontario</strong>) or 416 928-0900,ext. 7590.Eduardo Azevedo9026899/HG10329Allegations and plea<strong>The</strong> <strong>College</strong> alleged that the Memberaccessed and administered controlledsubstances, contrary to an order<strong>of</strong> the Discipline Committee, andthat he falsified copies <strong>of</strong> his APCs(Annual Payment Cards) by deletingreferences to the terms, conditionsand limitations.<strong>The</strong> Member admitted to theallegations, and the <strong>College</strong> andthe Member submitted a writtenstatement to the Panel in which theyagreed to the following facts.Agreed factsAt a hearing before the DisciplineCommittee in 1994, the Memberadmitted to medication and recordkeepingerrors and changing anothernurse’s documentation. <strong>The</strong> Memberwas found to have committedpr<strong>of</strong>essional misconduct and as aresult, his Certificate <strong>of</strong> Registrationwas restricted, so he could only accessand administer controlled substancesunder the supervision <strong>of</strong> another RN.<strong>The</strong> Member was employed withthe organization from 1999 untilhe was terminated in 2010. <strong>The</strong>restriction on his certificate remainedin effect throughout the period <strong>of</strong> hisemployment.Upon being hired, the Membernotified the <strong>College</strong> about hisemployer and advised that his roledid not require him to administercontrolled substances. However,he did access and administermedications, including controlledsubstances, during the normal course<strong>of</strong> his duties. Although this practicewas discontinued by the organizationin early 2001, the Member dispensednarcotics on numerous occasionsin 1999 and 2000, without beingsupervised by an RN.As a term <strong>of</strong> his employment withthe organization, the Member wasrequired to provide annual pro<strong>of</strong><strong>of</strong> registration with the <strong>College</strong>.He provided a copy <strong>of</strong> his APC,which he had altered to concealthe restriction on his practice. <strong>The</strong>organization discovered this in late2009. By that time, the organizationonly had the Member’s APCs for2008 and 2009 on file. Whenconfronted by the organizationabout the practice restriction andhis failure to disclose it, the Memberadmitted that he had contravened theDiscipline Committee order.Finding<strong>The</strong> Panel found that the factssupported a finding <strong>of</strong> pr<strong>of</strong>essionalmisconduct as alleged. <strong>The</strong>Member contravened an order <strong>of</strong>the Discipline Committee, falsifiedcopies <strong>of</strong> his APCs and otherdocumentation, signed or issueddocuments containing a false ormisleading statement, and engagedin conduct that would be regarded34 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
Discipline decisionsas disgraceful, dishonourable andunpr<strong>of</strong>essional. <strong>The</strong> Memberdemonstrated a persistent pattern <strong>of</strong>deception over several years.Submissions on order<strong>The</strong> <strong>College</strong> and the Member soughtan oral reprimand and a two-monthsuspension. <strong>The</strong> Member wouldbe required to complete specifiedremediation activities in preparationfor a meeting with a nursing expert.For 12 months after returning topractice, the Member would berequired to advise the <strong>College</strong> <strong>of</strong>his employers, provide employerswith a copy <strong>of</strong> the Panel’s decisionand reasons, and only practise foran employer who agreed to advisethe <strong>College</strong> if the Member breachedthe standards <strong>of</strong> practice <strong>of</strong> thepr<strong>of</strong>ession.Panel order<strong>The</strong> Panel accepted the jointsubmission as reasonable and inthe public interest. <strong>The</strong> Memberaccepted responsibility for hisactions and cooperated with the<strong>College</strong> by agreeing to the facts.<strong>The</strong> order addresses specific andgeneral deterrence, remediationand rehabilitation; ensures publicprotection; and maintains publicconfidence in the pr<strong>of</strong>ession’s abilityto regulate itself.D’Arcie Hunter9500844Allegations and plea<strong>The</strong> <strong>College</strong> alleged that theMember held the client’s hands inan aggressive manner, pushed theclient’s wheelchair and caused theclient’s arm to hyperextend, madeinappropriate remarks, left theclient alone in a dark room, failedto document appropriately, failed torespond to a call bell and was foundsleeping while on duty.<strong>The</strong> Member admitted to theallegations, and the <strong>College</strong> andthe Member submitted a writtenstatement to the Panel in which theyagreed to the following facts.Agreed facts<strong>The</strong> Member worked on the chroniccare/rehabilitation unit <strong>of</strong> a hospital.One morning, after telling herco-worker that she felt unwell andcould not deliver care to a client,the Member could not be locatedfor an hour and 20 minutes. Shewas found sleeping on the couch ina multipurpose room, with a chairplaced against the door to block theentrance. <strong>The</strong> Member went on sickleave for several months after thisincident.After her return to work, theMember was working a night shift.Two other nurses were providing carewhen they heard call bells ringing.<strong>The</strong> bells rang for some time. One <strong>of</strong>the nurses went to the lounge door tocall the Member, who was sleepingin a chair. <strong>The</strong> nurse kicked the back<strong>of</strong> the chair and called the Member’sname, at which point the Memberjumped up.On another occasion, a client wasrestrained in a chair with a table trayand an alarmed lap belt restraint.<strong>The</strong> client tried to remove the lapbelt and an RPN tried to reattachit. <strong>The</strong> Member went over to help.She aggressively held the client’shand into his chest for longer thannecessary, and taunted him withstatements such as, “You are messingwith the wrong girl” and, “You liketo hit girls, don’t you?” <strong>The</strong> Memberroughly took the client’s wheelchairand pushed him into a multipurposeroom. As she pushed himthrough the door, the client’s armhyperextended backwards and theMember let go <strong>of</strong> the chair, whichrolled into the room. She turned <strong>of</strong>fthe light, closed the door and left theclient alone in the dark. Her chartingindicated that the client becamecombative, attempted to strike staffand grabbed her wrists. <strong>The</strong> Memberincluded no further details, suchas placement <strong>of</strong> the client in themultipurpose room.Finding<strong>The</strong> Panel found that the factssupported a finding <strong>of</strong> pr<strong>of</strong>essionalmisconduct as alleged. <strong>The</strong> Panelfound the Member’s conduct tobe disgraceful, dishonourable andunpr<strong>of</strong>essional. <strong>The</strong> Member’s actionsregarding the client were aggressive,rough and inappropriate. <strong>The</strong>conduct shamed the Member and thepr<strong>of</strong>ession.Submissions on order<strong>The</strong> <strong>College</strong> and the Member soughtan oral reprimand and a two-monthsuspension. <strong>The</strong> Member wouldbe required to complete specifiedremediation activities in preparationfor a meeting with a nursing expert.For 12 months after returning topractice, the Member would berequired to advise the <strong>College</strong> <strong>of</strong>her employers, provide employerswith a copy <strong>of</strong> the Panel’s decisionand reasons, and only practise foran employer who agreed to advisethe <strong>College</strong> if the Member breachedthe standards <strong>of</strong> practice <strong>of</strong> thepr<strong>of</strong>ession.Panel order<strong>The</strong> Panel accepted the jointsubmission as reasonable and inthe public interest. <strong>The</strong> Memberaccepted responsibility for her actionsand cooperated with the <strong>College</strong> byagreeing to the facts.<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>35
Christine JacksonIE03822Allegations and plea<strong>The</strong> <strong>College</strong> alleged that the Memberintervened contrary to a physician’sorder, failed to record accuratelythe administration <strong>of</strong> medication,failed to administer medicationand was dishonest in response toquestions regarding the medication,administration and documentation.<strong>The</strong> Member admitted to theallegations, and the <strong>College</strong> andthe Member submitted a writtenstatement to the Panel in which theyagreed to the following facts.Agreed facts<strong>The</strong> Member worked in acutecare at a hospital. She had beenterminated from her position in2006 and was reinstated in 2008.Upon her return to work, shewas required to undergo trainingwith a PPL (pr<strong>of</strong>essional practiceleader) regarding IV (intravenous)medication administration.As part <strong>of</strong> her training, the Memberwas given 12 hours <strong>of</strong> instruction andthen asked to identify opportunities toobserve other nurses performing theskill. <strong>The</strong> Member was to call the PPLwhen administration opportunitiesarose so that the PPL could observeand assess her skills. <strong>The</strong> Member wasadvised that she could not perform theskill until the PPL had signed <strong>of</strong>f onfive administrations. <strong>The</strong> Member didnot contact the PPL at all on the dayin question.A chart review indicated that theMember had initialled client C’smedication administration record(MAR) two days earlier as though shehad administered an IV medication.At a meeting to discuss the issue, theMember insisted that she had notadministered the drug in the PPL’sabsence, but had asked a colleagueto administer the medication for her.<strong>The</strong> colleague denied having beenasked to administer the drug anddenied having administered it. ClientC did not receive her medication asprescribed.Client B was receiving dialysistreatment. After the Memberperformed client B’s dialysis exchangeone evening, client B reported thatthe Member had failed to open orfully open the drainage clamp. After15 minutes, client B noticed that thebag was still empty and he openedthe clamp himself.Client A had a physician’s orderto discontinue the sodium chlorideIV if test results indicated that thecreatinine level was less than 125umol/L. Blood test results printedat 1331 hrs indicated that client A’screatinine level was 202 umol/L.Despite this result, the Memberdiscontinued client A’s IV medicationat 1440 hrs.Finding<strong>The</strong> Panel found that the factssupported findings <strong>of</strong> pr<strong>of</strong>essionalmisconduct as alleged, and foundthe Member’s conduct to beunpr<strong>of</strong>essional.Submissions on order<strong>The</strong> <strong>College</strong> and the Member soughtan oral reprimand and a one-monthsuspension. <strong>The</strong> Member wouldbe required to complete specifiedremediation activities in preparationfor a meeting with the Director <strong>of</strong>Pr<strong>of</strong>essional Conduct and a meetingwith a regulatory expert. <strong>The</strong>Member would also be required tosuccessfully complete an approvedcommunity college course related tomedication administration. For 12months after returning to practice,the Member would be required toadvise the <strong>College</strong> <strong>of</strong> her employers,provide employers with a copy <strong>of</strong> thePanel’s decision and reasons, and onlypractise for an employer who agreedto advise the <strong>College</strong> if the Memberbreached the standards <strong>of</strong> practice <strong>of</strong>the pr<strong>of</strong>ession.Panel order<strong>The</strong> Panel accepted the jointsubmission as reasonable and in thepublic interest. It provides for anin-depth remediation program. <strong>The</strong>Member accepted responsibility forher actions; her demeanour showedremorse for her actions and respectfor the process.Sherri MacKenzie(formerly Deiter)9405499Allegations and plea<strong>The</strong> <strong>College</strong> alleged that the Membermisappropriated and used orattempted to use a deceased client’scredit cards and bank access card.<strong>The</strong> Member admitted to theallegations, and the <strong>College</strong> andthe Member submitted a writtenstatement to the Panel in which theyagreed to the following facts.Agreed facts<strong>The</strong> client had been receiving dialysistreatment at the facility approximatelyfour times a week since 2003. <strong>The</strong>Member provided the client withdirect nursing care on numerousoccasions over the years, including atleast 20 occasions in 2007 and at leastone occasion in 2008.<strong>The</strong> client died in July 2008.Police initiated an investigation afterlearning that transactions continuedto be posted to his credit card afterhis death. <strong>The</strong> investigation revealedthat the Member had the client’sbank access card and two creditcards. <strong>The</strong>re were multiple attemptsto withdraw funds from the client’s36 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
Discipline decisionsbank account using his access card,and to make purchases and cashadvances on the credit cards. <strong>The</strong>attempted bank machine withdrawalswere unsuccessful, and the attemptedpurchases on one <strong>of</strong> the cards weredeclined.<strong>The</strong> police laid one charge <strong>of</strong> fraudagainst the Member, encompassingall <strong>of</strong> the fraudulent credit cardtransactions. Purchases includedcosmetic surgery, services and hairproducts at a beauty salon; a lady’sblazer; payment <strong>of</strong> a veterinary billand payment <strong>of</strong> the Member’s annualmembership fee to the <strong>College</strong>. <strong>The</strong>total amount <strong>of</strong> the 135 transactionswas more than $47,000. Approvedtransactions totalled $27,286.21. Notall <strong>of</strong> these transactions were postedby the associated merchant. <strong>The</strong> totalloss suffered by the issuing financialinstitution was $14,801.40.<strong>The</strong> Member pleaded guilty to acharge <strong>of</strong> fraud exceeding $5,000.If the Member were to testify, thenshe would say that she and the clientshared a friendship, that he gave herhis credit card for safe-keeping forseveral weeks at a time, that he gaveher permission to use the card andthat she had used it in the past.During the criminal proceedings,the Member claimed she had accessto the client’s cards before his death(which could not be confirmed),but she could not explain why thespending patterns before the client’sdeath were inconsistent with thespending patterns after his death.Finding<strong>The</strong> Panel found that the factssupported findings <strong>of</strong> pr<strong>of</strong>essionalmisconduct: failing to meet standards<strong>of</strong> practice; misappropriation <strong>of</strong> funds;finding <strong>of</strong> guilt for a criminal <strong>of</strong>fencerelevant to suitability to practise;and disgraceful, dishonourable andunpr<strong>of</strong>essional conduct.Submissions on order<strong>The</strong> <strong>College</strong> and the Member soughtan oral reprimand and a five-monthsuspension. <strong>The</strong> Member wouldbe required to complete specifiedremediation activities in preparationfor at least three meetings with aregulatory expert. For 18 monthsafter returning to practice, theMember could not engage inindependent practice, and wouldbe required to advise the <strong>College</strong> <strong>of</strong>her employers, provide employerswith a copy <strong>of</strong> the Panel’s decisionand reasons, and only practise foran employer who confirmed thatthe Member would not have controlover finances <strong>of</strong> the employer orclients, and who agreed to advisethe <strong>College</strong> if the Member breachedthe standards <strong>of</strong> practice <strong>of</strong> thepr<strong>of</strong>ession.Panel order<strong>The</strong> Panel considered theaggravating factors: the volume <strong>of</strong>the transactions; the number <strong>of</strong>attempted transactions; the amount<strong>of</strong> money involved; the vulnerability<strong>of</strong> the client, who was deceasedand unable to protect himself; andthe nature <strong>of</strong> the purchases. <strong>The</strong>Panel also considered the mitigatingfactors: the Member’s lack <strong>of</strong> adisciplinary history with the <strong>College</strong>;her admission; that she had sufferedrepercussions through the criminalproceedings; that she made fullrestitution to the financial institution;her assertion that the proceedingshad a pr<strong>of</strong>ound and significantimpact on her; and that she has notbeen employed in nursing since 2009.<strong>The</strong> Panel accepted the jointsubmission as reasonable and inthe public interest. <strong>The</strong> Memberaccepted responsibility for her actionsand cooperated with the <strong>College</strong> byagreeing to the facts.Anthony MorrisIB12606Allegations and plea<strong>The</strong> <strong>College</strong> alleged that the Memberwas found guilty <strong>of</strong> criminal<strong>of</strong>fences relevant to his suitability topractise; held himself out as a nurseand engaged in nursing practicewhile his Certificate <strong>of</strong> Registrationwas suspended; provided false ormisleading information to the<strong>College</strong>; and made medication errorsin connection with 11 clients.<strong>The</strong> Member was neither presentnor represented by counsel at thehearing. <strong>The</strong> hearing proceeded onthe basis that the Member denied theallegations.Evidence<strong>The</strong> Panel heard from 10 witnesses.<strong>The</strong> Member’s certificate wassuspended for nonpayment <strong>of</strong> feesbetween May 1995 and October1999, April and June 2003, May2004 and September 2008, andfrom April 2009 on. <strong>The</strong> Membersigned his 2008 reinstatement formindicating that he had not practisednursing during the time <strong>of</strong> thesuspension and provided false dates<strong>of</strong> employment with facility B. Healso signed his 2008 annual renewalform without indicating that he hadprior criminal convictions.In April 2009, the Memberpleaded guilty to criminal charges <strong>of</strong>breaking and entering, and assault.According to court transcripts, theMember forced his way into anapartment and punched, kneed andchoked the victim. He also stole a cellphone. <strong>The</strong> assault may have been inretaliation for having been asked toleave a party.<strong>The</strong> court transcript also showedthat the Member worked duringthe periods that his certificate wassuspended. This was confirmed by<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>37
the testimony <strong>of</strong> the director <strong>of</strong> care atfacility A and the owner <strong>of</strong> facility B.Several witnesses from facility Atestified to incidents <strong>of</strong> medicationerrors, which were documented. Anexpert witness was given hypotheticalscenarios regarding each medicationincident report and testified that inall but one case, standards <strong>of</strong> practicewere not met. <strong>The</strong> expert also notedthat documentation was inadequate,as the Medication AdministrationRecords were pre-signed. She opinedthat the Member’s practices were adanger to the public.Finding<strong>The</strong> Panel found that the evidencesupported findings <strong>of</strong> pr<strong>of</strong>essionalmisconduct as alleged, except withrespect to two medication errors. <strong>The</strong>Panel also found that the Member’sconduct would be considereddisgraceful, dishonourable andunpr<strong>of</strong>essional. <strong>The</strong> public relies onnurses to document honestly, andthe Member’s repeated instances <strong>of</strong>falsifying documents and records,and <strong>of</strong> failing to disclose criminalconvictions, cast doubt on hiswillingness to discharge the moralobligation that is expected <strong>of</strong> a nurse.<strong>The</strong> medication errors, whichincluded failing to administermedications, administeringmedications to the wrong clients andsigning that he had administeredmedications when he had not, werebreaches <strong>of</strong> the standards <strong>of</strong> practice.Finally, the Member was found guilty<strong>of</strong> criminal <strong>of</strong>fences that are relevantto his suitability to practise.Submissions on order<strong>The</strong> Member had a history with the<strong>College</strong>. He received recommendationsfrom the Complaints Committeein 1993 regarding medicationadministration; a letter <strong>of</strong> cautionfrom the President <strong>of</strong> the <strong>College</strong>about medication administrationin 2004; and a letter from theExecutive Director <strong>of</strong> the <strong>College</strong>regarding 11 incidents in 2002 aboutunpr<strong>of</strong>essional communication andfailure to administer medications.In 2010, a panel <strong>of</strong> the DisciplineCommittee found that he hadcommitted pr<strong>of</strong>essional misconductwhen he was found guilty <strong>of</strong> <strong>of</strong>fencesrelevant to his suitability to practise(assault and theft) and had failed todisclose those findings to the <strong>College</strong>.<strong>The</strong> <strong>College</strong> sought immediaterevocation <strong>of</strong> the Member’scertificate.Panel order<strong>The</strong> Panel accepted the <strong>College</strong>’ssubmission. <strong>The</strong> Member’s actionsshow him to be ungovernable andthey violate the cornerstones <strong>of</strong>the nursing pr<strong>of</strong>ession — honesty,integrity and trustworthiness. <strong>The</strong>Member’s absence from the hearingand his many unreported criminalconvictions show his disrespectfor both the law and the <strong>College</strong>’sprocesses.Revocation is fair and appropriatein the circumstances. <strong>The</strong> orderprotects the public and sends a strongmessage to the membership thatthis type <strong>of</strong> behaviour will not betolerated.Paula Pontin9914862Allegations and plea<strong>The</strong> <strong>College</strong> alleged that theMember held herself out as a nurseand engaged in nursing practicewith four different facilities whileher Certificate <strong>of</strong> Registration wassuspended; falsified her APC (AnnualPayment Card); misappropriatedfunds from an employer; forgedprescriptions for Oxycontin; told astaff member to provide her with aurine sample that she could submitas her own; and engaged in conductthat would be deemed disgraceful,dishonourable and unpr<strong>of</strong>essional.<strong>The</strong> Member was neither presentnor represented by counsel at thehearing. <strong>The</strong> hearing proceeded onthe basis that the Member denied theallegations.Evidence<strong>The</strong> Panel heard from 10 witnesses,including staff from the fourfacilities, pharmacy staff, an employee<strong>of</strong> the <strong>College</strong> and an expert witness.<strong>The</strong> Member’s certificate wassuspended in May 2006 fornonpayment <strong>of</strong> fees. BetweenMay 2006 and January 2008, theMember sought employment and wasemployed as an RN. She representedherself as a nurse to four differentfacilities, in her resumé and ininterviews.While employed at facility A, theMember falsified prescriptions forOxycontin and misappropriatedmore than $15,500. She subsequentlypleaded guilty to the followingcriminal <strong>of</strong>fences: forging aprescription, forging a cheque, usinga credit card in facility A’s name andstealing money from facility A.<strong>The</strong> Member was later hired byfacility C through facility B. Whenshe was unable to provide a currentAPC, her position was terminated.She was then hired as a nurseadministrator by facility D. Shewas terminated when she asked acolleague for a urine sample for herown use. Upon advising the <strong>College</strong><strong>of</strong> the Member’s termination, facilityD learned that her registration hadbeen suspended and that the APCshe had provided had been falsified.<strong>The</strong> expert opined that theMember’s behaviour and practices38 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
Discipline decisionscontravened the standards <strong>of</strong>practice, and that her behaviourwould be deemed to be disgraceful,dishonourable and unpr<strong>of</strong>essional.Finding<strong>The</strong> Panel found that the evidencesupported findings <strong>of</strong> pr<strong>of</strong>essionalmisconduct as alleged, includingthat the Member’s conduct would beconsidered disgraceful, dishonourableand unpr<strong>of</strong>essional. <strong>The</strong> evidence wasclear, cogent and convincing, and thewitnesses were credible.<strong>The</strong> Panel described the Member’sbehaviour as highly deceitful andcriminal, reflecting a betrayal <strong>of</strong> thepublic trust and an abuse <strong>of</strong> power <strong>of</strong>her position.Submissions on order<strong>The</strong> <strong>College</strong> sought revocation <strong>of</strong>the Member’s certificate, as hermisconduct was among the mostserious categories <strong>of</strong> misconduct.<strong>The</strong>re was an extended pattern <strong>of</strong>criminal behaviour over two years,and she misrepresented her status asan RN to four separate employers.<strong>College</strong> counsel submitted that therewere no mitigating factors. Given theMember’s absence, it is not knownwhether she is interested in or capable<strong>of</strong> rehabilitation. In this instance,deterrence is the main issue, ratherthan rehabilitation.Panel order<strong>The</strong> Panel accepted the <strong>College</strong>’ssubmission. No mitigatingcircumstances were presented,and the Panel was unable to assesswhether the Member had anyfeelings <strong>of</strong> remorse or propensity forrehabilitation or remediation.Revocation provides specific andgeneral deterrence, protection <strong>of</strong>the public interest, assurance thatpublic trust in the pr<strong>of</strong>ession will bemaintained, and recognition thatcrimes <strong>of</strong> fraud, deceit, dishonestyand deliberate abuse <strong>of</strong> power willnot be tolerated.Patricia Ann Tennant9101049Allegations and plea<strong>The</strong> <strong>College</strong> alleged that the Memberfailed to provide adequate trainingand supervision and inappropriatelydelegated nursing tasks to UCPs(unregulated care providers), failed todocument, inappropriately restraineda client, directed or allowed staff toabuse a client, failed to maintainproper sanitation and hygiene at thefacility, failed to provide appropriatefood to clients, allowed clients toshare or use needles, failed to providefor appropriate supervision <strong>of</strong> clientswith dementia, and failed to reportpromptly a fire in the facility to thefire department. <strong>The</strong> <strong>College</strong> alsoalleged that the Member held herselfout as a nurse and engaged in nursingpractice while her Certificate <strong>of</strong>Registration was suspended.<strong>The</strong> Member was neither presentnor represented by counsel at thehearing. <strong>The</strong> hearing proceeded onthe basis that the Member denied theallegations.Evidence<strong>The</strong> Panel heard from 10 witnesses,including staff at the facility, anemployee <strong>of</strong> the <strong>College</strong>, an expertwitness, the family member <strong>of</strong> aclient at the facility, a public healthinspector and the president <strong>of</strong>another facility where the Memberwas employed.From October 2008 to June 2009,the Member assumed all nursing andadministrative duties at a retirementfacility for clients with complex needsrequiring ongoing care. Although hercertificate had been suspended sinceApril 2007, the Member representedherself as a nurse to staff at thefacility, introduced herself as a nurseand performed controlled acts.UCP A was assigned to orienta new staff member to the facilityand to teach the skills required forthe PSW (personal support worker)position. UCP A had no postsecondaryeducation or training, andthe Member knew that she had n<strong>of</strong>ormal experience caring for clients ina retirement facility. Three other staffmembers were also hired as PSWs.<strong>The</strong>ir training came from UCP Aand UCP B, neither <strong>of</strong> whom had anyformal training. <strong>The</strong> Member wasfrequently absent and provided noon-site training or supervision <strong>of</strong> staff.All problems were to be reported toUCP A.Client B fell twice in his roomwithin two days. After the secondfall, UCP A tried to contact theMember for an hour before theMember arrived. <strong>The</strong> Member didnot complete a thorough physicalassessment. Before the ambulancearrived, the Member asked staff toapply a dressing to the skin tearson client B’s arms; on admission tohospital, it was discovered that clientB had also fractured his hip.When asked to assess client C,who had been vomiting, the Memberdid not take vital signs or documenther assessment. Client C had said shewas fasting because <strong>of</strong> her religiousbeliefs, and the Member told staff toignore her because she was attentionseeking.<strong>The</strong> Member did not permitstaff to access client charts andtold UCP A to record everythingin the log book. Staff received noinstruction on what or how to chart.<strong>The</strong> Member examined client Das part <strong>of</strong> a demonstration <strong>of</strong> theprocedure for checking for evidence<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>39
Ad removed forweb publishing
<strong>The</strong> <strong>College</strong> welcomes letters commending outstandingnursing care. Please send original signed letters from clientsor family members. Facilities or agencies can also forwardoriginal signed letters, along with a copy <strong>of</strong> the author’sletter and the author’s permission to publish. Letters maybe edited for publication.In Praise<strong>of</strong> <strong>Nurses</strong>Holistic health careMy mother, Margaret Haynes, was afrequent client at Groves MemorialCommunity Hospital in Fergus untilshe passed away.During her last hospitalization,she was transferred to Guelph forcorrective surgery <strong>of</strong> a broken hip.When she returned to Groves, thenursing staff on the second floorwelcomed her and treated her withtender care and dignity, even thoughshe was confused, agitated and notcompletely cooperative.<strong>The</strong> reception my father and therest <strong>of</strong> our family received from thenurses was also unlike anythingI have seen elsewhere. <strong>The</strong> nurseswere very pr<strong>of</strong>essional, but alsocompassionate and supportive. <strong>The</strong>ybrought comfort during a verydifficult time for our family.I am truly glad that my mothercame home to Groves for her finaldays. I’m sure she knew that she wassurrounded by love during this time.I want to express how thankful weare for the way the staff cared for all<strong>of</strong> us. It was truly holistic health care!Gillian FedericoDignity in dyingMy grandfather passed away in his90th year. During his final days, thenurses at Northland Pointe in PortColborne showed me that there canbe dignity in dying.My grandparents moved toNorthland Pointe after mygrandmother had a stroke and mygrandfather started to decline withAlzheimer’s. While the move wasn’teasy, the staff made it much moretolerable.My grandfather had a witty andsarcastic sense <strong>of</strong> humour, and whilehe may have become forgetful, hehad certainly not lost his wit. Onsome <strong>of</strong> his more difficult, stubborndays, the nurses appealed to his jokeynature and could usually get him tocome around.In his final days, the same nurseswho had joked with him made himcomfortable, sat with him and spokequietly to him. <strong>The</strong>y also took goodcare <strong>of</strong> our family—bringing usmeals, ensuring we knew what washappening and checking in to makesure we were OK. And on the nightthat he passed, a nurse stayed withour family and said goodbye with us.<strong>The</strong> nurses at Northland Pointedeserve much praise. <strong>The</strong>y arecompassionate people who genuinelycare for their clients and treat themlike family. It was comforting toknow that my grandfather was welltaken care <strong>of</strong> and loved by suchamazing staff. We can never thankthem enough.Jenn Green and the Overholt family42 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
IN Prase <strong>of</strong> <strong>Nurses</strong>Commendable careI am writing to comment on theexemplary care my father, StanleyStevenson, received while he wasa client at St. Mary’s <strong>of</strong> the LakeHospital in Kingston.Dad was admitted for six weeks <strong>of</strong>rehabilitation therapy. During thistime, he developed bleeding froman enlarged prostate gland requiringirrigation. <strong>The</strong> nurses who caredfor him on Gibson 3 demonstratedthe “Philosophy <strong>of</strong> Nursing Practiceat Providence Care” by giving Dadautonomy, and listening to andadvocating for our family’s concernsabout Dad’s acute health. <strong>The</strong>occupational therapist and other staffwere also wonderful. Everyone wasvery respectful and helpful.My mother, brothers and I wouldlike to convey our deepest gratitudefor this quality care. I hope that Iprovide my clients with the kind<strong>of</strong> nursing care, compassion andhope for recovery that my fatherexperienced from the Gibson 3 staff.Thank you,Sandra Monroe, RNA kind spiritI’m writing this letter in praise <strong>of</strong>Debbie Ferguson, RPN.When my Dad was about to turn80, he was listed as palliative in thecomplex care unit at GeorgetownHospital. I told his nurse, Debbie,that his birthday was coming up andfound out that she was going to beworking with him for most <strong>of</strong> theweek. In the days leading up to hisbirthday, I asked her if it would bepossible to have him up in a chair forthe event because some <strong>of</strong> his familywould be visiting.When the day came, I arrived atthe hospital to find my Dad washed,dressed and ready for his big day,awake and alert. Debbie truly tookthe time to get my Dad ready,finding pyjamas and even socks!He got to spend the afternoon andevening with his family and evenwent outside on the patio for a partyin his honour.I write this letter to acknowledgeone <strong>of</strong> the loveliest, mostcompassionate nurses I’ve met. Debbieis a dedicated and caring person whobrings such a kind spirit to her work.This was evident in the way she tooktime to sit with and talk to my Dadand the other clients in the unit. Shealso eased the worries and concerns <strong>of</strong>family members with a compassionatetouch. And she always did her jobwith a smile on her face!Tracy O’Donnell, RNPatients come firstI would like to comment on theexcellent care I received when Iwas admitted to Belleville GeneralHospital for knee replacement surgery.I have had many hospital staysthroughout my life, but I honestlybelieve that the care and concernshown by the sixth-floor nurses atBelleville General has never beenbeat. <strong>The</strong> wonderful treatment Ireceived showed me that the patientis most important.All <strong>of</strong> the nurses who cared for mecertainly deserve a very big round <strong>of</strong>applause.Wendy AveyInspirational careMy mother was a frequent patientat Northumberland Hills Hospitalin Cobourg where she was treatedfor chronic obstructive pulmonarydisease. <strong>The</strong> emergency departmentand ICU nurses were always patientand kind. As an ICU nurse myself,I know how busy it can be during a12-hour shift. <strong>The</strong> nurses were gentleand soothing, and really helped easethe stress <strong>of</strong> the situation. <strong>The</strong>irpr<strong>of</strong>essionalism was inspirational.My mother spent her last daysin the palliative care unit. Whilenothing could have prepared usfor her passing, the amazing staffhelped make it a positive, serene andpeaceful experience for my motherand our family. <strong>The</strong> nurses in theunit are angels, to say the least.<strong>The</strong>y made my mother’s last days ascomfortable as possible. <strong>The</strong>y werequick with smiles and tender care,and were advocates for pain control.Being in the position <strong>of</strong> familymember rather than nurse hasopened my eyes to the kind <strong>of</strong> carethat nurses can and do provide fortheir clients. <strong>The</strong> nurses who caredfor my mother have inspired me andmade me proud to be part <strong>of</strong> thenursing pr<strong>of</strong>ession.Sincerely,Karen Honey, RN, and familySend your letters to:InPraiseOf<strong>Nurses</strong>@cnomail.org or<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong>101 Davenport Rd.Toronto, ON M5R 3P1<strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong> 43
Careers Careers Careers Careers Careers Careers Careers CareersAd removed forweb publishing44 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
Pursuea Career at Your <strong>College</strong>Are you looking for aworkplace that valuesleadership, integrityand collaboration?Do you want to workfor an employerthat recognizes theimportance <strong>of</strong> apositive work/lifebalance? Do youappreciate workingwith pr<strong>of</strong>essional andtalented colleagues?If so, the <strong>College</strong> <strong>of</strong><strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> may<strong>The</strong> <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> is a dynamic leader innursing self-regulation. As the regulator for nursing in<strong>Ontario</strong>, the <strong>College</strong>’s mission is to regulate nursing in thepublic interest.Benefits:Work with teams <strong>of</strong> committed nursing colleagues,as well as a wide range <strong>of</strong> enthusiastic pr<strong>of</strong>essionals.Competitive benefit and compensation packages.Opportunities for ongoing pr<strong>of</strong>essional development.An active social committee.Easily accessible downtown Toronto location.Career opportunities in practice consulting, policydevelopment, investigations and other fields are posted onthe <strong>College</strong>’s website as they become available.Visit www.cno.org/hr for more information about growingyour career at the <strong>College</strong>.have the career you’vebeen looking for.
“A nurse demonstrates the standardby advocating for quality practiceimprovements in the workplace.”– from Pr<strong>of</strong>essional <strong>Standard</strong>s<strong>The</strong> <strong>Standard</strong> <strong>of</strong> Care.Photo: Heather LatterJoanne Ogden, RN, doesn’t let geographystop her from providing optimal home care. Joanneworks with three other RNs, two RPNs and one personalsupport worker at Fort Frances Tribal Area HealthServices. Together the team serves 10 First Nationscommunities scattered over 50,000 km 2 .When Ogden became the manager <strong>of</strong> home andcommunity care in 2003, she immediately identified ahigh need for addressing wound care in clients. “Close to70 per cent <strong>of</strong> our clients have diabetes,” she says.Ogden began by advocating for education. “We can’tprovide good care if our team members aren’t educatedin the areas that have the most need. All our staff arecertified in wound care, anticoagulation therapy, skinperfusion pressures and chronic disease management. Westrive to stay updated with the most advanced practiceapplicable to our population.”Ogden, a former critical care nurse, also advocated forbetter equipment. “You don’t use outdated equipment inthe ICU, so why should you have to use it in home care?”she asks. By looking for one-time funding opportunities,the team acquired digital skin thermography, bedsideDoppler ultrasound, and the technology to measure skinperfusion and pulse volume recording. “This allows usto better treat clients with wound care at the bedside,decreasing the number <strong>of</strong> clients that have to leave hometo see specialists for this testing. We can upload thisinformation to a vascular surgeon to review and expeditethe process for referral <strong>of</strong> clients who are in high need.”In the past, the team had challenges acquiring woundcare supplies, including waiting for approval <strong>of</strong> clients’health benefits. But, by advocating for an improvedprocess, Ogden is now part <strong>of</strong> a pilot program in whichsupplies are approved quickly—usually within the sameday. No wait time for the client and no delay in thewound-healing process.“Our first year <strong>of</strong> service, over 15 clients receivedamputations in one year; this past year, only one,” saysOgden, reflecting on the team’s preventive measures.“We must be doing something right!” SAt the <strong>College</strong>, the phrase “the standard <strong>of</strong> care” is more than atag line for the logo; it’s about setting the bar for safe, effectiveand ethical nursing care through the practice standards andguidelines. This page features nurses who have raised the baron the standard <strong>of</strong> care they provide their clients.46 <strong>College</strong> <strong>of</strong> <strong>Nurses</strong> <strong>of</strong> <strong>Ontario</strong> the standard summer <strong>2012</strong>
Ad removed forweb publishing
Ad removed forweb publishing