SPAP Prescription Verification - US Virgin Islands DHS
SPAP Prescription Verification - US Virgin Islands DHS
SPAP Prescription Verification - US Virgin Islands DHS

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
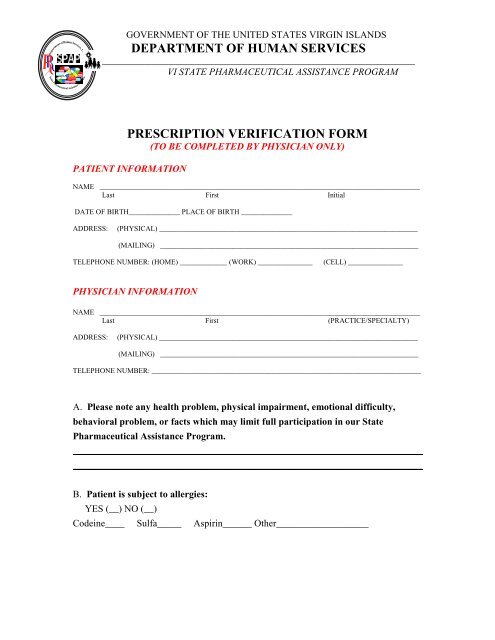
GOVERNMENT OF THE UNITED STATES VIRGIN ISLANDSDEPARTMENT OF HUMAN SERVICES_________________________________________________________________VI STATE PHARMACEUTICAL ASSISTANCE PROGRAMPRESCRIPTION VERIFICATION FORM(TO BE COMPLETED BY PHYSICIAN ONLY)PATIENT INFORMATIONNAME ________________________________________________________________________________________Last First InitialDATE OF BIRTH______________ PLACE OF BIRTH ______________ADDRESS:(PHYSICAL) _______________________________________________________________________(MAILING) _______________________________________________________________________TELEPHONE NUMBER: (HOME) _____________ (WORK) _______________(CELL) _______________PHYSICIAN INFORMATIONNAME ________________________________________________________________________________________Last First (PRACTICE/SPECIALTY)ADDRESS:(PHYSICAL) _______________________________________________________________________(MAILING) _______________________________________________________________________TELEPHONE NUMBER: __________________________________________________________________________A. Please note any health problem, physical impairment, emotional difficulty,behavioral problem, or facts which may limit full participation in our StatePharmaceutical Assistance Program.________________________________________________________________________________________________________________________________________________B. Patient is subject to allergies:YES (__) NO (__)Codeine____ Sulfa_____ Aspirin______ Other___________________
C. Patient is subject to:__ asthma__ sensitive skin__ sleepwalking__ nosebleed__ ear ache__ sinus trouble__ convulsions__ high blood pressure__ fainting__ frequent colds__ headache__ motion sickness__ tonsillitis__ nightmares__ bed wetting__ allergies__ eye infection__ bronchitis__ kidney problem(describe)_____________D. Patient wears contact lenses (__) or glasses (___)Medical Conditions and Diagnosis: (Check all that apply)High Blood Pressure _____ Diabetes _____ Arthritis _____Cancer _____ Heart Lung _____Other ___________________________________________________________________________________________________________E. To ensure that all patients comply with their medication regimen in a cost contained manner,please provide a list of the patient’s CURRENT prescribed medication and the indication for itsuse.Medication Strength(mg)SIGDirectionsPrescribingDoctorDoctorPhone #PharmacyCompanyDateNOTE: THE <strong>SPAP</strong> PROVIDES MEDICATION ASSISTANCE TO SENIORSAGE 60 AND ABOVE; TO ENSURE THAT WE PROVIDE ADEQUATECOVERAGE, WE ENCOURAGE PHYSICIANS TO PRESCIBE GENERICSUNLESS BRAND IS ABSOLUTELY NECESSARY!!!