Community dialogue forum on TB in Mwea PDF - Kelin
Community dialogue forum on TB in Mwea PDF - Kelin
Community dialogue forum on TB in Mwea PDF - Kelin
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
ABBREVIATIONSAIDS . . . . . . . . . . . Acquired Immune Deficiency SyndromeARV . . . . . . . . . . . AntiretroviralCACC . . . . . . . . . . C<strong>on</strong>stituency AIDS C<strong>on</strong>trol CommitteeCBO . . . . . . . . . . . <str<strong>on</strong>g>Community</str<strong>on</strong>g> Based Organisati<strong>on</strong>CSO . . . . . . . . . . . Civil Society Organisati<strong>on</strong>DASCO . . . . . . . . . . District AIDS Coord<strong>in</strong>at<strong>in</strong>g OfficeDOTS. . . . . . . . . . Directly Observed TherapyDTLC . . . . . . . . . . District <strong>TB</strong> and Leprosy Coord<strong>in</strong>atorGIPA . . . . . . . . . . . Greater Involvement of People liv<strong>in</strong>g and/or affected with HIV/AIDSGoK . . . . . . . . . . . Government of KenyaHIV . . . . . . . . . . . Human Immuno-deficiency VirusKCM . . . . . . . . . . . Global Fund Nati<strong>on</strong>al Oversight Committee of Kenya Coord<strong>in</strong>at<strong>in</strong>g MechanismKELIN . . . . . . . . . . Kenya Legal & Ethical Issues Network <strong>on</strong> HIV and AIDSLAHI . . . . . . . . . . . Law and Health InitiativeMDGs . . . . . . . . . . Millennium Development GoalsMSM . . . . . . . . . . . Men who have sex with MenNACC . . . . . . . . . . Nati<strong>on</strong>al AIDS C<strong>on</strong>trol CouncilNEPHAK . . . . . . . . . Nati<strong>on</strong>al Empowerment Network of People Liv<strong>in</strong>g with HIV and AIDS <strong>in</strong> KenyaNGO . . . . . . . . . . . N<strong>on</strong>-governmental Organisati<strong>on</strong>OSIEA . . . . . . . . . . Open Society Initiative East AfricaPHO . . . . . . . . . . . Public Health Officer, Public Health DepartmentPLHIV . . . . . . . . . . Pers<strong>on</strong>s liv<strong>in</strong>g with HIVPMTCT . . . . . . . . . . Preventi<strong>on</strong> of Mother to Child Transmissi<strong>on</strong><strong>TB</strong> . . . . . . . . . . . . TuberculosisCover photograph: Melba Kat<strong>in</strong>di (KELIN Advocacy and Tra<strong>in</strong><strong>in</strong>g Officer) takes participants through a sessi<strong>on</strong>2
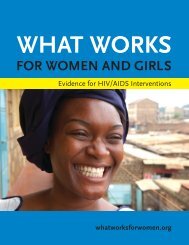
1.0 EXECUTIVE SUMMARYThe Kenya Legal and Ethical Issues Network <strong>on</strong> HIV & AIDS (KELIN) is <strong>on</strong>e of the few organisati<strong>on</strong>s <strong>in</strong> Kenya and East Africa work<strong>in</strong>g <strong>on</strong> legal and humanrights issues <strong>in</strong> relati<strong>on</strong> to health and HIV. KELIN’s goal is to undertake advocacy and provide leadership <strong>in</strong> ensur<strong>in</strong>g an enhanced rights based approach <strong>in</strong>health and HIV strategies and programmes.The Nati<strong>on</strong>al Empowerment Network of People Liv<strong>in</strong>g with HIV and AIDS <strong>in</strong> Kenya (NEPHAK) is an NGO that unites support groups of People Liv<strong>in</strong>gwith HIV/AIDS (PLHIV) and <strong>in</strong>dividual PLWHAs <strong>in</strong>to a nati<strong>on</strong>al and formidable force to counter the impact of HIV and AIDS <strong>on</strong> their lives and that oftheir loved <strong>on</strong>es <strong>in</strong> Kenya.Follow<strong>in</strong>g <strong>in</strong>creas<strong>in</strong>g reports of arrests of <strong>TB</strong> patients <strong>in</strong> and around <strong>Mwea</strong>, KELIN and NEPHAK, with support of the Open Society Foundati<strong>on</strong>, collaborated todeliver a <strong>on</strong>e day <str<strong>on</strong>g>Community</str<strong>on</strong>g> Dialogue Forum <strong>in</strong> <strong>Mwea</strong> <strong>on</strong> the effective c<strong>on</strong>trol, management and care of <strong>TB</strong> with a focus <strong>on</strong> PLHIV. The <str<strong>on</strong>g>forum</str<strong>on</strong>g> was held <strong>on</strong>27th May 2011 at Green Ficus Hotel. The aim of the <str<strong>on</strong>g>forum</str<strong>on</strong>g> was to mobilize complementary acti<strong>on</strong> by all stakeholders <strong>in</strong> the effective management of <strong>TB</strong> <strong>in</strong> thearea.Key stakeholders <strong>in</strong> <strong>TB</strong> management at community level were <strong>in</strong>vited <strong>in</strong>clud<strong>in</strong>g representatives of key Government organs work<strong>in</strong>g <strong>on</strong> health issuesespecially <strong>TB</strong> & HIV, Magistrates, community health workers (CSWs), local CBOs and <str<strong>on</strong>g>Community</str<strong>on</strong>g> Support groups of <strong>TB</strong> patients & PLHIV and mediahouses. Unfortunately neither the Prov<strong>in</strong>cial <strong>TB</strong> and Leprosy Coord<strong>in</strong>ator (PTLC) nor the District <strong>TB</strong> and Leprosy Coord<strong>in</strong>ator (DTLC) were represented.There were 39 participants dur<strong>in</strong>g the <str<strong>on</strong>g>forum</str<strong>on</strong>g>. The attendees shared views and perspectives <strong>on</strong> various issues hamper<strong>in</strong>g effective <strong>TB</strong> diagnosis andtreatment adherence <strong>in</strong> the area.The <str<strong>on</strong>g>forum</str<strong>on</strong>g> begun with general PowerPo<strong>in</strong>t presentati<strong>on</strong>s facilitated by Allan Maleche, Melba Kat<strong>in</strong>di, Mr. Nels<strong>on</strong> Otwoma and Ms. Lucy Ghati of KELIN andNEPHAK respectively. Deliberati<strong>on</strong>s followed thereafter <strong>on</strong> the topics presented <strong>on</strong> <strong>in</strong>clud<strong>in</strong>g issues relat<strong>in</strong>g to <strong>TB</strong>, HIV and relevant Legal provisi<strong>on</strong>s. Severalparticipants shared pers<strong>on</strong>al testim<strong>on</strong>ies highlight<strong>in</strong>g their experiences as <strong>TB</strong> patients. There were numerous questi<strong>on</strong>s raised <strong>in</strong> relati<strong>on</strong> to <strong>TB</strong> treatmentespecially <strong>in</strong> children who were HIV positive. The misc<strong>on</strong>cepti<strong>on</strong>s around <strong>TB</strong> epidemic were discussed br<strong>in</strong>g<strong>in</strong>g out numerous cultural beliefs that discouragedmany suspected <strong>TB</strong> patients from seek<strong>in</strong>g <strong>TB</strong> screen<strong>in</strong>g. One major issue brought out that c<strong>on</strong>tributed to n<strong>on</strong>-adherence was the l<strong>on</strong>g durati<strong>on</strong> of <strong>TB</strong>treatment which was unsusta<strong>in</strong>able dur<strong>in</strong>g weekends and l<strong>on</strong>g holidays when the health centres rema<strong>in</strong>ed closed and hospital pers<strong>on</strong>nel unavailable. Thepris<strong>on</strong> representatives raised c<strong>on</strong>cerns with regard to <strong>TB</strong> diagnosis with<strong>in</strong> the Pris<strong>on</strong>s sight<strong>in</strong>g understaffed laboratories and the difficulty <strong>in</strong> screen<strong>in</strong>g newdeta<strong>in</strong>ees.Back to the top4
• To understand the law• To learn about our rights• To address community problems <strong>on</strong> <strong>TB</strong> treatment• To ga<strong>in</strong> knowledge to be able to share with others• To know how to go about the challenges of my work <strong>in</strong> pris<strong>on</strong> and foster<strong>in</strong>g cooperati<strong>on</strong> with community members <strong>in</strong> support<strong>in</strong>g releasedpris<strong>on</strong>ers still undergo<strong>in</strong>g <strong>TB</strong> treatment.• To know the systems <strong>in</strong> place and encourage community referral mechanisms• How to give support <strong>in</strong> terms of elim<strong>in</strong>at<strong>in</strong>g <strong>TB</strong> and HIV related stigma• Understand the role of the community <strong>in</strong> support<strong>in</strong>g patience dur<strong>in</strong>g treatmentSESSION ONE: Summary of Presentati<strong>on</strong>si. Introducti<strong>on</strong> and overview of KELINMr. Allan Maleche, the Coord<strong>in</strong>ator at KELIN, familiarized the participants with KELIN. He menti<strong>on</strong>ed KELIN’s objective, missi<strong>on</strong> and visi<strong>on</strong>. Allan expla<strong>in</strong>edthat KELIN was <strong>in</strong> the bus<strong>in</strong>ess of health and human rights because majority of ord<strong>in</strong>ary citizens <strong>in</strong> Kenya are ignorant of their rights and cannot hence accesshealth related rights. He expla<strong>in</strong>ed that the stigma and discrim<strong>in</strong>ati<strong>on</strong> associated with HIV and other related diseases like <strong>TB</strong> pose a major challenge <strong>in</strong> theirpreventi<strong>on</strong>, c<strong>on</strong>trol and management. He expla<strong>in</strong>ed the need for <strong>in</strong>tegrati<strong>on</strong> of human rights <strong>in</strong> programmes and strategies <strong>on</strong> health, HIV and <strong>TB</strong>.He further enlightened the participants <strong>on</strong> KELIN’s <strong>in</strong>volvement <strong>in</strong> <strong>TB</strong> and HIV programm<strong>in</strong>g. He expla<strong>in</strong>ed that KELIN was <strong>in</strong>volved <strong>in</strong> sensitizati<strong>on</strong>and capacity build<strong>in</strong>g which <strong>in</strong>volves the educati<strong>on</strong> of members of the community <strong>on</strong> the various human rights comp<strong>on</strong>ents relat<strong>in</strong>g to health andHIV and <strong>TB</strong>. He <strong>in</strong>formed them of the recent tra<strong>in</strong><strong>in</strong>gs KELIN c<strong>on</strong>ducted <strong>in</strong> Kapsabet <strong>in</strong> partnership with NEPHAK which were aimed at enabl<strong>in</strong>gan understand<strong>in</strong>g of the balance between public health and human rights <strong>in</strong> the c<strong>on</strong>text of <strong>TB</strong> and HIV. He then expla<strong>in</strong>ed the litigati<strong>on</strong> and legalsupport that KELIN offers <strong>on</strong> pro b<strong>on</strong>o basis <strong>in</strong> order to provide redress to PLHIV <strong>in</strong> respect of the various legal & ethical c<strong>on</strong>cerns or human rightsviolati<strong>on</strong>s encountered. He expla<strong>in</strong>ed KELIN’s <strong>in</strong>volvement <strong>in</strong> case of the impris<strong>on</strong>ment of three <strong>TB</strong> patients <strong>in</strong> Kapsabet who had allegedly defaulted<strong>on</strong> their <strong>TB</strong> treatment. He also drew their attenti<strong>on</strong> to KELIN’s <strong>on</strong>go<strong>in</strong>g enquiries <strong>in</strong>to the case of Sim<strong>on</strong> Maregwa <strong>in</strong> <strong>Mwea</strong> which is similar. F<strong>in</strong>ally heexpla<strong>in</strong>ed that KELIN hopes to develop detailed reports and share with policy makers <strong>in</strong> an effort to strengthen advocacy and lobby<strong>in</strong>g for effective <strong>TB</strong>management nati<strong>on</strong>al and operati<strong>on</strong>al policy that are rights based, people centred and less punitive for the achievement of better results with<strong>in</strong> thecommunity.Back to the top7
He expla<strong>in</strong>ed that his expectati<strong>on</strong> for the <str<strong>on</strong>g>forum</str<strong>on</strong>g> was the participants would be enlightened <strong>on</strong> <strong>TB</strong> and related human rights to enable them report violati<strong>on</strong>sand claim the health rights guaranteed to them under the provisi<strong>on</strong>s of the C<strong>on</strong>stituti<strong>on</strong>.A member of the community posses a questi<strong>on</strong> at the <str<strong>on</strong>g>forum</str<strong>on</strong>g>ii. Introducti<strong>on</strong> and overview of NEPHAKThe participants were generally familiar with NEPHAK. Mr. Nels<strong>on</strong> Otwoma, the Nati<strong>on</strong>al Coord<strong>in</strong>ator at NEPHAK gave them a further detailed <strong>in</strong>sight <strong>in</strong>tothe work of the organizati<strong>on</strong>. He began by expla<strong>in</strong><strong>in</strong>g that NEPHAK was nati<strong>on</strong>al network that not <strong>on</strong>ly united PLHIV but also those affected by <strong>TB</strong> throughsupport groups, post-test clubs, women and youth groups, CBOs, NGOs and other networks. After stat<strong>in</strong>g NEPHAK’s missi<strong>on</strong> and visi<strong>on</strong>, he expla<strong>in</strong>ed thatthrough NEPHAK and its partners, Greater Involvement of People liv<strong>in</strong>g and/or affected with HIV&AIDS (GIPA) can be achieved. He expla<strong>in</strong>ed NEPHAK’s role<strong>in</strong> identify<strong>in</strong>g and br<strong>in</strong>g<strong>in</strong>g the <strong>TB</strong> cases to that attenti<strong>on</strong> of KELIN for legal and probable litigati<strong>on</strong> support. He expla<strong>in</strong>ed that majority of the cases identifiedby them <strong>in</strong>volv<strong>in</strong>g violati<strong>on</strong> of rights of PLHIV are referred to KELIN and encouraged report<strong>in</strong>g of any violati<strong>on</strong>s with<strong>in</strong> <strong>Mwea</strong> and its envir<strong>on</strong>s. F<strong>in</strong>ally, heexpla<strong>in</strong>ed that <strong>on</strong> the Nati<strong>on</strong>al platform NEPHAK served as the voice of PLHIV and enhanced their <strong>in</strong>volvement <strong>in</strong> the HIV resp<strong>on</strong>se through representati<strong>on</strong> <strong>in</strong>the Nati<strong>on</strong>al Oversight Committee of Kenya Coord<strong>in</strong>at<strong>in</strong>g Mechanism (KCM) – Global Fund, Kenya Stop <strong>TB</strong> Partnership and the <strong>TB</strong> Interagency Coord<strong>in</strong>at<strong>in</strong>gCommittee.Back to the top8
He c<strong>on</strong>cluded by expla<strong>in</strong><strong>in</strong>g that the overall goal of NEPHAK is to work to improve the quality of life of PLHIV and that dictates <strong>in</strong>volvement <strong>in</strong>empowerment of its membership <strong>on</strong> <strong>TB</strong> care and its management.iii. HIV and <strong>TB</strong> collaborati<strong>on</strong>The objective of this presentati<strong>on</strong> was to facilitate an understand<strong>in</strong>g of the l<strong>in</strong>k between <strong>TB</strong> and HIV. Lucy Ghati, Programme Officer at NEPHAK facilitated thesessi<strong>on</strong>. She began by bra<strong>in</strong> storm<strong>in</strong>g with the participants <strong>on</strong> their knoweleddge <strong>on</strong> <strong>TB</strong> issues. Besides some comm<strong>on</strong> symptoms the participants did not havea lot of <strong>in</strong>formati<strong>on</strong> regard<strong>in</strong>g <strong>TB</strong>. Ms. Ghati proceeded to give an overview of the causes of <strong>TB</strong>, how <strong>on</strong>e gets <strong>in</strong>fected and additi<strong>on</strong>al signs and symptoms. Shehighlighted the epidemiology of <strong>TB</strong> and HIV and their c<strong>on</strong>necti<strong>on</strong>.The participants identified the possible factors that cause delay <strong>in</strong> <strong>TB</strong> diagnosis as l<strong>on</strong>g distances to health centres, HIV related stigma, patient’spreference for traditi<strong>on</strong>al healers and prayers before seek<strong>in</strong>g treatment, communicati<strong>on</strong> barriers between health workers and clients and ignorance ofthe facts <strong>on</strong> <strong>TB</strong>. She briefly expla<strong>in</strong>ed the treatment drugs which were dependant <strong>on</strong> each <strong>in</strong>dividual case.After reiterat<strong>in</strong>g the importance of adher<strong>in</strong>g to <strong>TB</strong> treatment Lucy <strong>in</strong>quired from the participants community misc<strong>on</strong>cepti<strong>on</strong>s around <strong>TB</strong> that hamperedtreatment adherence.“One of my colleagues at work passed away after be<strong>in</strong>g diagnosed with <strong>TB</strong>. Interrogati<strong>on</strong> of the circumstances surround<strong>in</strong>g his death revealed that due to self stigma, the deceased hadnot been tak<strong>in</strong>g his medic<strong>in</strong>es but was simply discard<strong>in</strong>g them under his bed.”Lucy expla<strong>in</strong>ed that both HIV and <strong>TB</strong> related stigma results <strong>in</strong> numerous unnecessary deaths.“Villagers <strong>in</strong> my area believe that <strong>TB</strong> is a curse that is hereditary that is why it is comm<strong>on</strong> am<strong>on</strong>g members of the same family”Lucy expla<strong>in</strong>ed that <strong>TB</strong> be<strong>in</strong>g airborne was likely to be easily passed <strong>on</strong> from <strong>on</strong>e member of the family who is <strong>in</strong>fected to the others. She clarified that it wasnot a curse or related to witchcraft as comm<strong>on</strong>ly alleged.Several other misc<strong>on</strong>cepti<strong>on</strong>s were addressed. The participants were enlightened <strong>on</strong> the causes of MDR <strong>TB</strong> and c<strong>on</strong>cluded with a lengthy discussi<strong>on</strong> <strong>on</strong> therole of the community <strong>in</strong> <strong>TB</strong> management. Dur<strong>in</strong>g this sessi<strong>on</strong> there arose uncerta<strong>in</strong>ty as to whether BCG should be adm<strong>in</strong>istered to HIV positive babies.iv. Legal and Ethical issues <strong>in</strong> <strong>TB</strong> managementThe objective of the presentati<strong>on</strong> was to enable an understand<strong>in</strong>g of the balance between Public health and Human rights <strong>in</strong> the c<strong>on</strong>text of <strong>TB</strong> and HIV. M/sMelba Kat<strong>in</strong>di, Advocacy and Tra<strong>in</strong><strong>in</strong>g Officer at KELIN delivered the presentati<strong>on</strong>. She began the sessi<strong>on</strong>s by <strong>in</strong>quir<strong>in</strong>g whether the participants had everdiscrim<strong>in</strong>ated aga<strong>in</strong>st some<strong>on</strong>e with either <strong>TB</strong> or HIV. After <strong>in</strong>terest<strong>in</strong>g deliberati<strong>on</strong>s by the participants as to what c<strong>on</strong>stituted discrim<strong>in</strong>ati<strong>on</strong> and what didn’tBack to the top9
she expla<strong>in</strong>ed what legal and ethical issues were and expla<strong>in</strong>ed the role of stigma and discrim<strong>in</strong>ati<strong>on</strong>. Her presentati<strong>on</strong> focused <strong>on</strong> Test<strong>in</strong>g, C<strong>on</strong>fidentiality andCrim<strong>in</strong>alizati<strong>on</strong>.She expla<strong>in</strong>ed briefly the provisi<strong>on</strong>s of The C<strong>on</strong>stituti<strong>on</strong> and The HIV and AIDS preventi<strong>on</strong> and c<strong>on</strong>trol Act, 2006. Dur<strong>in</strong>g discussi<strong>on</strong>s <strong>on</strong> test<strong>in</strong>g andc<strong>on</strong>fidentiality, the participants expressed differ<strong>in</strong>g op<strong>in</strong>i<strong>on</strong>s <strong>on</strong> the issue of partner notificati<strong>on</strong> of HIV+ results.On crim<strong>in</strong>alizati<strong>on</strong>, Melba expla<strong>in</strong>ed summarily the provisi<strong>on</strong>s of Secti<strong>on</strong> 24 of the HIV and AIDS (preventi<strong>on</strong> and c<strong>on</strong>trol) Act, 2006 and secti<strong>on</strong> 27 ofthe sexual offences Act, 2003 that crim<strong>in</strong>alize <strong>in</strong>tenti<strong>on</strong>al transmissi<strong>on</strong> of HIV. She further elaborated <strong>on</strong> secti<strong>on</strong> 27 of the public health act that allowsfor the detenti<strong>on</strong> of pers<strong>on</strong>s suspected of hav<strong>in</strong>g an <strong>in</strong>fectious disease up<strong>on</strong> an applicati<strong>on</strong> by a Public Health Officer <strong>in</strong> the <strong>in</strong>terest of protecti<strong>on</strong> ofpublic health. The issue of crim<strong>in</strong>alizati<strong>on</strong> sparked off a heated debate <strong>on</strong> appropriateness and effectiveness of the provisi<strong>on</strong>s both <strong>in</strong> relati<strong>on</strong> to HIVand <strong>TB</strong>.Melba c<strong>on</strong>cluded by reiterat<strong>in</strong>g the significance of embrac<strong>in</strong>g the Rights Based Approach <strong>in</strong> deal<strong>in</strong>g with health issues.SESSION TWO: Experience Shar<strong>in</strong>gExperiential stories are a powerful tool <strong>in</strong> enhanc<strong>in</strong>g learn<strong>in</strong>g, performance, cohesiveness and understand<strong>in</strong>g. The objective of this sessi<strong>on</strong> was to highlightboth positive and negative aspects relat<strong>in</strong>g to <strong>TB</strong> management as pers<strong>on</strong>ally experienced by community members.WaitheraMark“I was <strong>on</strong> <strong>TB</strong> treatment for 5 m<strong>on</strong>ths. In that period I was made to believe that I had received div<strong>in</strong>e heal<strong>in</strong>g. Sadly, shortly after I stopped tak<strong>in</strong>g my medicati<strong>on</strong> I got really sick. Asa result of my relapse when I was <strong>in</strong>itiated back <strong>on</strong> treatment I had to have 60 <strong>in</strong>jecti<strong>on</strong>s adm<strong>in</strong>istered daily. This was really tough <strong>on</strong> my hav<strong>in</strong>g to travel daily to the health centre.The difficulty was mostly <strong>on</strong> weekends when the centres were all closed and medical pers<strong>on</strong>nel unavailable. I had to pay a government Doctor who lived next to my home to adm<strong>in</strong>isterthe <strong>in</strong>jecti<strong>on</strong>s for me over the weekends so that I d<strong>on</strong>’t risk relapse aga<strong>in</strong>! ”“My wife and children were diagnosed with <strong>TB</strong> before I was. We all received treatment. My wife however who was HIV positive at the time was secretly us<strong>in</strong>g herbal treatment. We<strong>on</strong>ly discovered after she was paralysed. Despite all efforts to save her life, she passed away. As a result of this traumatiz<strong>in</strong>g experience I am actively <strong>in</strong>volved <strong>in</strong> <strong>TB</strong> and HIV literacywith<strong>in</strong> my community.”Gachoki“Had previously suffered from <strong>TB</strong> and got re-<strong>in</strong>fected. When I was put <strong>on</strong> treatment, the treatment really weakened me and I was unable to fend for myself. I was too weak to work ordo anyth<strong>in</strong>g and liv<strong>in</strong>g <strong>in</strong> the city, there was no-<strong>on</strong>e to assist me <strong>in</strong> cook<strong>in</strong>g, look<strong>in</strong>g for clean water and basic groom<strong>in</strong>g. Inevitably, I defaulted. I got sicker and sicker and eventuallyBack to the top10
esorted to go<strong>in</strong>g back to my village to seek necessary family support that encouraged me to complete my medicati<strong>on</strong>. It was tough but I am now liv<strong>in</strong>g healthy, free from <strong>TB</strong>.”Wambui“I was diagnosed with <strong>TB</strong> at the age of 23 after undergo<strong>in</strong>g so many <strong>in</strong>c<strong>on</strong>clusive tests. <strong>TB</strong> is often associated with HIV and my loss of weight <strong>on</strong>ly fuelled the rumours. Self stigmaand fear of discrim<strong>in</strong>ati<strong>on</strong> by family made me move away from my home. Despite be<strong>in</strong>g negative, I felt mov<strong>in</strong>g would allow me to complete my medicati<strong>on</strong> without any<strong>on</strong>e f<strong>in</strong>d<strong>in</strong>gout. I advocate for strengthened community support systems for <strong>TB</strong> patients to encourage adherence without fear of double stigma related to <strong>TB</strong> and HIV. ”PLENARYDur<strong>in</strong>g the Plenary, the CACC Coord<strong>in</strong>ator expla<strong>in</strong>ed that there is great effort <strong>in</strong> the county to foster <strong>TB</strong>-HIV collaborati<strong>on</strong>. He recognized the need for<strong>in</strong>creased health educati<strong>on</strong> <strong>on</strong> <strong>TB</strong> management and treatments <strong>in</strong>clud<strong>in</strong>g community awareness <strong>on</strong> the l<strong>in</strong>k between <strong>TB</strong> and HIV. He appreciated the roleof the community health workers and emphasized the need for strengthen<strong>in</strong>g the referral system from the community to the health facilities and vice versa.Success <strong>in</strong> defaulter trac<strong>in</strong>g is highly dependent <strong>on</strong> this. He expla<strong>in</strong>ed that the pressure aris<strong>in</strong>g from the strict policy of zero defaulters is forc<strong>in</strong>g public healthofficers to rush <strong>in</strong> seek<strong>in</strong>g detenti<strong>on</strong> of defaulters as opposed to try<strong>in</strong>g to address the problem. This way they avoid answer<strong>in</strong>g to their superiors as there will beno defaulters <strong>on</strong> record. He says lack of recogniti<strong>on</strong> and lack of remunerati<strong>on</strong> for CHW and other community structures is discourag<strong>in</strong>g their good work.A community health volunteer expla<strong>in</strong>ed that whenever a <strong>TB</strong> suspect is identified, referral to health centres are normally frustrated by the l<strong>on</strong>gdistance which would impose numerous travel costs for the patients.A community peer educator was c<strong>on</strong>cerned that defaulter tracers are most of the time ignorant of the special circumstances h<strong>in</strong>der<strong>in</strong>g adherence such as lackof food, clean water and m<strong>on</strong>ey to travel to the health centres as often as is required.Back to the top11
From left to right: Ms. Mary Ngunji (NEPHAK <strong>TB</strong> Ambassador) and Ms. Kisanet Yemen(KELIN volunteer lawyer) listen to the proceed<strong>in</strong>gs at the <str<strong>on</strong>g>forum</str<strong>on</strong>g>The pris<strong>on</strong> representatives unanimously raised c<strong>on</strong>cern with regard to the ignored nutriti<strong>on</strong>al needs of both <strong>TB</strong> and HIV patients <strong>in</strong> pris<strong>on</strong>s. He expla<strong>in</strong>edthat neither the Public Health Officers nor the patients themselves request for special diets while <strong>in</strong> the pris<strong>on</strong>s. Further the courts rema<strong>in</strong> ignorant <strong>on</strong> thesignificance of factor<strong>in</strong>g <strong>in</strong> dietary needs <strong>in</strong> successful medical <strong>in</strong>terventi<strong>on</strong>s. They also stressed <strong>on</strong> the need of special hold<strong>in</strong>g cells for all new pris<strong>on</strong>ersfor screen<strong>in</strong>g before jo<strong>in</strong><strong>in</strong>g the general pris<strong>on</strong> populati<strong>on</strong>. This will greatly reduce the chances of <strong>in</strong>fecti<strong>on</strong> with<strong>in</strong> the pris<strong>on</strong>s. Additi<strong>on</strong>ally the pris<strong>on</strong>representatives observed that failure rate <strong>in</strong> drug adherence of released pris<strong>on</strong>ers is very high. There needs to be a follow-up mechanism to ensure theirsuccess with<strong>in</strong> the community.The NEPHAK community representative restated the lack of community awareness <strong>on</strong> <strong>TB</strong> and health related rights. Government has failed <strong>in</strong>educat<strong>in</strong>g the public <strong>on</strong> health issues. She proposed that just as <strong>in</strong> HIV treatment adherence, counsell<strong>in</strong>g of <strong>TB</strong> patients needs to play a significant roleif <strong>TB</strong> treatment adherence is to improve.Back to the top12
3.0. METHODOLOGYThe Forum comprised a participatory approach which <strong>in</strong>cluded structured presentati<strong>on</strong>s, Questi<strong>on</strong> & Answer sessi<strong>on</strong>s, experience shar<strong>in</strong>g, and healthydebates am<strong>on</strong>g the participants. The presentati<strong>on</strong>s were made through PowerPo<strong>in</strong>t and handouts. For efficient deliberati<strong>on</strong>s the facilitators felt it wasimportant to deliver an overall presentati<strong>on</strong> to cover basics of <strong>TB</strong> and the relevant legal provisi<strong>on</strong>s. This was d<strong>on</strong>e <strong>in</strong> an attempt to address exist<strong>in</strong>gpresumpti<strong>on</strong>s that may have arisen dur<strong>in</strong>g the deliberati<strong>on</strong>s and promote accurate and <strong>in</strong>formed c<strong>on</strong>tributi<strong>on</strong>s from the participants.4.0 CHALLENGES1. The participants were unfamiliar with basic facts of <strong>TB</strong> and the law. The coverage of the modules was rushed and the case studies could not be<strong>in</strong>terrogated <strong>in</strong> detail.2. Due to lack of previous tra<strong>in</strong><strong>in</strong>g, the participants raised numerous questi<strong>on</strong>s and clarificati<strong>on</strong>s which ate <strong>in</strong>to the presentati<strong>on</strong> time. The numerousquesti<strong>on</strong>s that arose could not be exhaustively discussed <strong>in</strong> the limited time that was allocated for community deliberati<strong>on</strong>s.3. The sessi<strong>on</strong>s started late as a result of the participant’s late arrival; this posed the challenge of hav<strong>in</strong>g detailed presentati<strong>on</strong>s and discussi<strong>on</strong>s.4. Power cuts dur<strong>in</strong>g the tra<strong>in</strong><strong>in</strong>g <strong>in</strong>terrupted the sessi<strong>on</strong>s and blew KELIN’s electr<strong>on</strong>ic equipments <strong>in</strong>clud<strong>in</strong>g laptop cables and the LCD that was be<strong>in</strong>gused for the presentati<strong>on</strong>s. We were unable to share the visual aids prepared <strong>in</strong>clud<strong>in</strong>g images and videos.5.0 RECOMMENDATIONS1. In future, it would be best if a general tra<strong>in</strong><strong>in</strong>g for purposes of <strong>in</strong>formati<strong>on</strong> dissem<strong>in</strong>ati<strong>on</strong> and capacity build<strong>in</strong>g would be c<strong>on</strong>ducted beforeundertak<strong>in</strong>g a community <str<strong>on</strong>g>dialogue</str<strong>on</strong>g> <str<strong>on</strong>g>forum</str<strong>on</strong>g>. This will greatly benefit participants and c<strong>on</strong>tribute to more <strong>in</strong>formed deliberati<strong>on</strong>s.2. A simplified handbook c<strong>on</strong>ta<strong>in</strong><strong>in</strong>g legal provisi<strong>on</strong>s highlight<strong>in</strong>g rights and obligati<strong>on</strong>s <strong>in</strong> relati<strong>on</strong> to the enjoyment of the Right to Health would be auseful tool <strong>in</strong> dissem<strong>in</strong>at<strong>in</strong>g the much needed <strong>in</strong>formati<strong>on</strong>.Back to the top13
APPENDIX I: LIST OF PARTICIPANTSNo. Name Sex Organizati<strong>on</strong>1. John M. Kanja M Peer Educator Kimbimbo SDH2. Moses Gachoki M Christian <str<strong>on</strong>g>Community</str<strong>on</strong>g> <strong>Mwea</strong> (CCS Ngurubari) <strong>TB</strong> Patient3. Naomi W Riura F <str<strong>on</strong>g>Community</str<strong>on</strong>g> Health Volunteer (Anti stigma Support Group)4. David Munithi M Christian <str<strong>on</strong>g>Community</str<strong>on</strong>g> <strong>Mwea</strong> (CCS Ngurubari) <strong>TB</strong> Patient5. Ejidio W Wjoka M6. Emily Wangeci F Mwienderi Self Group7. Mark Gathumiano M DIFFATHAS PLWHAS Group8. Edita Wangari F Christian <str<strong>on</strong>g>Community</str<strong>on</strong>g> <strong>Mwea</strong> CCS Support Group9. Alice Muth<strong>on</strong>i F Christian <str<strong>on</strong>g>Community</str<strong>on</strong>g> <strong>Mwea</strong> CCS TAIBA10. Joseph Muntike M KIMBIMBI Support Group11. James Liy<strong>in</strong>gi M <strong>Mwea</strong> Hope <strong>in</strong> Life12. Michael Wamboi M Discovery Artists Youth Group “Advocacy Group”13. Elizabeth Kan<strong>in</strong>i F MWIRERI Support Group14. Agnes Wanjiku F MWIRERI Support Group15, Rose Waithira F Former <strong>TB</strong> Patient16. Emily Wanjiru F Peer Educator (YPENLO Self help group)17. Florence Mwangi F Mugumo Support Group18. Susan Kavumbu F <strong>Mwea</strong> Hope <strong>in</strong> Life19. Kemau Kibe M Christian <str<strong>on</strong>g>Community</str<strong>on</strong>g> <strong>Mwea</strong>: Former <strong>TB</strong> patient20. Nazario Karuk M PLWHIV21. Francis Muiruri MOur Lady of LordsFormer <strong>TB</strong> Patient22. Sarah Wangech F Kimbimbi Support Group23. Charles Nauni M Embu Pris<strong>on</strong>, Prov<strong>in</strong>cial <strong>TB</strong>/HIV Program Coord<strong>in</strong>ator24. Josphat Myaga M <strong>Mwea</strong> Hope <strong>in</strong> Life25. Nancy M. Gratobi F MUGUMO Support Group26. Peters<strong>on</strong> Wat<strong>in</strong>au M CALL Coord<strong>in</strong>ator27. Charles Isimuitu M Kagio Support Group28. Aar<strong>on</strong> Mutumga M Paralegal Coord<strong>in</strong>ator Southern Z<strong>on</strong>e Support Group29. Sim<strong>on</strong> Mati M <strong>Mwea</strong> Pris<strong>on</strong>30. Mary Mg<strong>on</strong>eyi F <strong>TB</strong> Ambassador Kerugova31. Elizabeth Wanji F32. Esther Wambi F PLWA Representative33. Zipporah Kisilo F <strong>Mwea</strong> NEPHAK Representative34. Lucy Gheli F NPHAK35. Kisanet Yemane F KELIN36. Allan Maleche M KELIN37. Joy Obuya F Eyeris Pictures38. Nels<strong>on</strong> J.Otwoma M NEPHAK39. Melba Katidi F KELINBack to the top14