Download PDF - The Dermatologist
Download PDF - The Dermatologist
Download PDF - The Dermatologist

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Volume 5, Number 1 Spring 2006dermResident Expert:<strong>The</strong> OutpatientSurgical SuiteItch—An Update onPathophysiology andNew Treatment StrategiesManaging Cases of Chronic,Moderate-to-Severe PlaquePsoriasis Involving the Handsand Feet with RAPTIVA ®(efalizumab)R E S I D E N T
Welcome Residents!We’re pleased to bring you the latest issue of Derm Resident, a quarterly newsletter createdto help answer your questions as you move toward full-time practice.We hope the articles help you address the challenges you’ll face. <strong>The</strong>se articles provide you witheasy-to-follow advice to ease your transition from resident to practicing dermatologist.We bring you “Resident Expert,” a column written by well-known practitioner and practicemanagement expert, Dr. Phillip M. Williford, Associate Professor of Dermatology at WakeForest University School of Medicine, Winston-Salem, NC. Continuing with his guidance onsetting up a successful outpatient surgical suite, Dr. Williford focuses on quality assurance—a subject crucial to the establishment of a premier surgical practice.In this issue’s cover story, Dr. Gil Yosipovitch, Associate Professor, Departments of Dermatology,Neurobiology & Anatomy, and Regenerative Medicine, Wake Forest University Baptist MedicalCenter, Winston-Salem, NC, discusses the pathophysiology and new treatment strategies of itch.In addition, Scott Fretzin, MD, describes the use of RAPTIVA ® in chronic, moderate-to-severeplaque psoriasis involving the hands and feet.We hope you’ll find information in this newsletter that you can use in your everyday practicenow, and in the future.If you know of any of your colleagues who are not receiving Derm Resident and wouldlike to receive it for free, please call the Publisher, Joe Morris, at (800) 237-7285, ext. 204,or e-mail him at jmorris@hmpcommunications.com.Best regards,Ivor Caro, MDFellow of the American Academy of DermatologyMedical Director, Dermatology, Genentech
Resident ExpertThis established practitioner, professor, andpractice management expert answersyour most important questions.By Phillip M. Williford, MD<strong>The</strong> Outpatient Surgical Suiteare theQ.Whatmost importantconsiderations in creating asuccessful surgical practicesuite?A.In the Spring, Summer, andFall issues of DermResident, I reviewed the key points concerningdesign of space, budget, supplycosts, and time efficiency in creating a successfuloutpatient surgical suite. In thisissue, I will explore a subject crucial to theestablishment of a premier surgical practice:quality assurance. While I recognizethat there may not always be agreementon what this entails, there are aspects ofthe mission for continued quality improvementthat are common to the lexicon of allsurgeons.First, one must begin by recognizingthat at the completion of your new practiceor surgical space, the effort for qualityassurance is just beginning. While the successfuloffice builds on established qualityand plans, the new facility must draft anorganized, well-conceived blueprint toaugment patterns of behavior, and implementtools that lead to improved care,which lessens the risk of mortality or morbiditywith any surgical exposure.Fortunately, in dermatology, the risk ofdeath related to the procedures performedin the office setting is extremely low.However, it should be recognized that evenin dermatology, procedures carry risk.Quality improvement is about loweringthat risk as well as improving the overalldelivery of care to patients.So, where should you focus yourefforts? Begin by looking at those areaswhere crucial attention to detail is necessaryday in and day out, and expand yourpurview to all arenas that offer somepotential for improved patient safety andservice. While quality assurance beginswith attention to the details of deliveringsurgical services, it extends to record keeping,billing, procedural documentation,and even patient privacy. This articleexamines only a few of those arenas thatwill eventually require your attention.Remember, first, your most importanttime-saver, people, and assign the designationof Quality Assurance Officer to oneor more of your staff. Try to incorporatetheir skill strengths so that the certified histotechnicianmay be responsible for aspectsof the lab, and a registered nurse may beresponsible for infection control. On day1, create a record of every biopsy, excision,Mohs procedure, or other procedurewhere specimens are submitted for pathologicevaluation. In every instance, somenotation recognizing the report, acknowledgingthe need for further care, if indicated,and the date of those plans shouldbe entered. Lost specimens and lostreports unrelated to your care will occur.You need to be aware of these issuesbefore a patient calls 6 months later forthe report that you never received, butwas read as invasive melanoma Clarklevel 4. Consider personally initialing yourspecimen bottles, and having a nurse confirmthe tissue in the bottle before apatient leaves the office. Inform thepathology lab that you are making thiseffort. It will reduce calls that the bottlewas received without a specimen.Whenever a complication such asinfection occurs, re-create the circumstances.Was this avoidable? What roomwas used for the procedure? Has thatroom been associated with other patients’infections? Were preoperative antibioticmedications used? Is the infecting organismlikely to be community-acquired?Which personnel were involved in thecare of that patient? Should the staff becultured for carrier status? Ensure thatyour cleaning service recognizes theunique needs for intensive cleaning of alltable tops, light handles, and other surfacesdaily. Follow up to ensure that thecleaning staff understands, are usingappropriate products, and are complyingwith your requests. Establish regular testingfor adequacy of sterilization techniques.Use commercially available testingmedia. Create a regular schedule of trainingon resuscitative equipment, checkdaily that these devices are in workingorder, and keep a log confirming this.Don’t try to reinvent the wheel. Requesthelp from national groups specializing inoutpatient surgical suites’ quality assuranceprograms and incorporate thoseideas, but modify your plans to meet yourown particular needs. Finally, the qualityassurance journey—much like a crosswordpuzzle for you aficionados—whensolved, can be lot of fun. ●●●<strong>The</strong> opinions expressed in this article arethose of the author and are not necessarilythose of Genentech, Inc.3
—An Update onPathophysiologyand New Treatment StrategiesBy Gil Yosipovitch, MDItch was defined more than 340 years agoby Samuel Hafenreffer as an “unpleasantsensation provoking the desire to scratch.”This definition does not cover all the aspects ofthis subjective symptom, but provides a simpleand accurate description of itch.Itch declared its independence from pain ina pivotal study by Schmelz et al 1 in 1997, whoused direct nerve recordings in awake humans,and demonstrated that itch is transmitted bydedicated C neurons distinct from the classical“polymodal nociceptors,” which are involved inpain processing. <strong>The</strong>se “itch” neurons can beidentified by their lasting response to histamineapplication and are characterized by their slowconduction velocities and extensive terminalbranching. In a recent study, the same C fibershave shown spontaneous activity in a patientsuffering from chronic itch. 2 However, it shouldbe made clear that there is no single specializeditch receptor on peripheral nerve endings.Since itch can be induced by mechanical stimulisuch as contact with wool, C nerve fibers,which are mechanical sensitive, may beinvolved in itch transmission, especially inchronic itch.<strong>The</strong> supraspinal processing of itch and itscorresponding scratch response have recentlybeen investigated in humans by functionalpositron emission tomography (PET) as well asfunctional magnetic resonance imaging(fMRI). 3,4 Induction of itch by intradermal histamineinjections and histamine skin prick elicitsco-activation of sensory as well as motorareas in the brain. <strong>The</strong> significant co-activationof the motor area supports the clinicalobservation that itch is inherently linked to adesire to scratch.MEDIATORS FOR ITCH OTHERTHAN HISTAMINEHistamine is the archetypal mediator ofitch. It clearly is an important mediator ofitch in urticaria and insect bite reaction;however, in itch related to chronic pruritusassociated with other skin inflammatory diseasessuch as atopic eczema and in systemicdiseases, its role is very limited. Thisexplains the weak therapeutic efficacy ofantihistamines as antipruritics.Recent studies have shown that activationof the mast cell releases a proteinase namedtryptase, which in turn activates a proteinaseactivatedreceptor-2 (PAR-2) localized on Cfiber nerve terminals as well as keratinocytes. 5<strong>The</strong> activated C fibers will transmit this informationto the central nervous system (CNS),inducing the sensation of itch. Steinhoff et al 6demonstrated enhanced tryptase immunoreactivityin lesions of patients with atopic dermatitisin comparison to healthy controls.Accordingly, the PAR-2 receptor for tryptasewas markedly enhanced.Recent data suggest that neuromediatorssuch as nerve growth factor and neurotrophin-3are involved in localized itch andatopic eczema; these mediators are alsoimportant in pain. 7 Vanilloid receptors andcannabinoid receptors may also have a rolein attenuating the itch response. 8 Other receptorsbelonging to the ion channel proteins,such as cold receptors like transient receptorpotential-M8 (TRP-M8), which respond tomenthol, can suppress itch.Opiates and itch. Opiates have a direct centraland peripheral itch-producing activity. Lowdoses of intradermal morphine produce itch,and the effect is independent of mast celldegranulation. This effect is probably causedby mu-opiate receptors, as it has been reportedthat the mu-opiate receptor antagonist naltrexonesuppresses these itch sensations. Inaddition, it was recently reported that the activationof kappa-opiate receptor antagonizesvarious mu-opiate receptor–mediated actions. 5Cytokines and pruritus. Cytokines have beenproposed as mediators of nonhistamineinduceditch. Only interleukin (IL)-2 shows a4direct pruritogenic effect when it is injectedintradermally. 2,9 Although tumor necrosis factor(TNF)-alpha does not have any direct pruritogeniceffect, it is elevated in many pruriticdermatoses; antipruritic medications such asthalidomide may exert their antipruritic effectby lowering TNF-alpha levels. Recent studieshave shown that the role of IL-6 and IL-31 areimportant in the elicitation of itch.Prostaglandins. Prostaglandins do not have adirect pruritogenic effect on itch, but are knownto lower the skin threshold for itch induced byhistamine, and probably other mediators. 5MANAGEMENT<strong>The</strong>re are different types of itch.Dermatologic itch originates from skin diseasessuch as atopic eczema, psoriasis, and skindryness. Neuropathic itch is due to pathologyto nerve fibers along the afferent pathways(eg, postherpetic neuralgic itch, brachioradialitch, and itch in multiple sclerosis). Systemicitch is associated with mediators that induceitch without skin inflammation, such as uremiaand itch of cholestasis. Psychogenic itch isassociated with psychological abnormalities(eg, delusions of parasitosis and itch associatedwith depression). <strong>The</strong>se recent definitionsmay help us to evaluate and treat pruritus in amore meaningful way, both for the individualpatient and for the comparison of potentialtherapies in studies.Better understanding of the pathophysiologyof itch and the different types of itch has ledto advances in treatment of itch. 9,10 Amongtreatment strategies for itch are drugs that canblock the neuropathic afferent pathway. Forexample, gabapentin, which is a structuralanalog of the neurotransmitter gammaaminobutyric acid, has been reported to beeffective for treatment of neuropathic itch and,in recent case series, of generalized pruritus.11 Drugs that can reduce itch intensity inthe CNS, such as selective serotonin reuptakeContinued on page 6
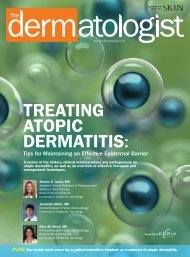
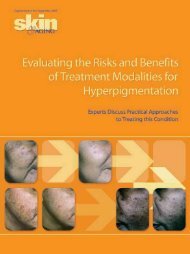
Managing Cases of Chronic, Moderateto-SeverePlaque Psoriasis Involving theHands and Feet with RAPTIVA ®By Scott Fretzin, MDPsoriasis plaques commonly occur on theelbows, knees, scalp, and trunk of thebody; however, they may occur anywhere,including the hands and feet. Psoriasisthat appears on the hands and feet may be aplaque-type form or a pustular form, and pustulesare frequently present in a predominantlyplaque-type presentation. As many as 15-25% of patients who suffer from plaque psoriasisalso present with psoriasis that involvesthe hands and feet. 1 Thus, it is always importantto carry out a head-to-toe inspection ofany patient upon presentation and at followupexams.Psoriasis involving the hands and feet isoften recurrent and frequently challenging totreat effectively. Conventional psoriasis treatmentoptions, including topical steroids, phototherapy,and systemic agents (eg,methotrexate and acitretin), have demonstratedlimited efficacy for management of thisform of the disease. In many cases, thickenedskin on the palms and soles may act as aphysical barrier that limits efficient delivery oftopical agents. In addition, short duration ofresponse, inconvenient or unpleasant topicalformulations, toxicity, and intolerability associatedwith many traditional treatmentapproaches present further limitations to effectivetreatment. 2 In order to develop a treatmentplan appropriately tailored to a patient,Figure 1. Jane’s feet and legs.A. Before treatment with RAPTIVA.Individual results may vary. Photos from phase 3 clinical trials.a complete understanding of his or her medicaland treatment history is necessary.Biologic therapies, such as efalizumab (RAP-TIVA ® , Genentech, Inc.), may offer an effectivealternative to conventional treatments for handand-footplaque psoriasis. RAPTIVA is a recombinant,humanized, monoclonal immunoglobulinG 1(IgG 1) antibody that targets many of theT-cell interactions associated with theimmunopathogenesis of psoriasis. Because of itspositive safety and efficacy record in multiplephase 3 clinical trials, 3 RAPTIVA has beenapproved by the Food and Drug Administration(FDA) for the treatment of adults with chronic,moderate-to-severe plaque psoriasis who arecandidates for systemic or phototherapy. It isimportant to note that the long-term efficacy ofRAPTIVA has been supported with up to 3 yearsof clinical experience. 4 <strong>The</strong> most serious adversereactions observed during treatment with RAP-TIVA were serious infections, malignancies,immune-mediated thrombocytopenia, immunemediatedhemolytic anemia, arthritis events,and psoriasis worsening and variants. Seriousinfections and immune-mediated thrombocytopeniahave been reported during post-marketingsurveillance. <strong>The</strong> most common adversereactions associated with RAPTIVA were asymptom complex that included headache,chills, fever, nausea, and myalgia within 48hours following the first two injections.B. After 6 months of RAPTIVA1 mg/kg/wk subcutaneously.5When we think of plaque psoriasis involvingthe hands and feet, we often expect lesionsof the palms and soles, but hand-and-foot psoriasisincludes lesions localized to the dorsalsurfaces of the hands and feet as well. <strong>The</strong> followingcase study shows Jane, a 52-year-oldCaucasian woman who has had a 41-year historyof plaque psoriasis. Jane also has a historyof type 2 diabetes mellitus and hypercholesterolemia.She presented with an affected bodysurface area (BSA) of 18%, with lesions on herlower extremities (Figure 1A). <strong>The</strong> dorsal surfacesof her feet, particularly her toes and heels,were affected. Jane’s psoriasis had been treatedpreviously with methotrexate, but she had todiscontinue taking the drug after developingmethotrexate-induced liver fibrosis. Sheenrolled in a 6-month RAPTIVA clinical trial andinitiated RAPTIVA treatment. Jane took an initialconditioning dose of 0.7 mg/kg and proceededwith 1 mg/kg administered subcutaneously(SC) every week. Her psoriasis responded rapidlyto RAPTIVA, and at 2 months her BSA hadimproved to 4%. She continued to improve withweekly therapy, and at 3 months her BSA hadimproved to 1.5%. At the end of the 6-monthstudy, Jane had achieved 90% improvementfrom baseline (Figure 1B).<strong>The</strong> severity of psoriasis is measured bymultiple parameters. Generally, psoriasis thataffects more than 10% BSA is consideredsevere, and that which affects 3-10% BSA isconsidered moderate. Psoriasis can severelyimpact a patient’s quality of life by affectingphysical, psychological, social, sexual, andoccupational well-being. 5 It is the patient withhand and foot involvement who often experiencesexcessive pain, distress, disability, andinterference with daily function beyond thatcaused by psoriasis anywhere else on thebody. 6 Although many patients with plaquepsoriasis involving the hands and feet havesevere disease, it is not uncommon for patientsto have more moderate forms of the disease.<strong>The</strong> management of moderate hand-and-footplaque psoriasis should not be undervaluedbecause the physical location of the diseaseincreases a patient’s vulnerability to environmentallyinduced trauma (eg, inclement weather,exposure to water, restrictive footwear),which may lead to exacerbation of disease. 7Continued on page 6
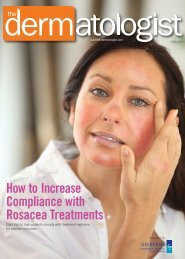
“Itch” continued from page 4inhibitors (SSRIs), have beneficial response topsychogenic itch. <strong>The</strong> new class of SSRIs thatare both noradrenergic and serotoninenhancers, such as mirtazapine, has beenshown in low doses of 15 mg at nighttime toreduce itch intensity of different types, includingsystemic and dermatologic itch.Another target of treatment is inhibitionof itch transmission based on the directincreased opioidergic tone in the spinalcord and pruritus. Intravenous naloxoneand oral naltrexone have been used formore than a decade as antipruritics, mainlyin cholestatic itch. Naltrexone 50 mgdaily has shown a significant therapeuticresponse for itch of different types.Unfortunately, these medications have severalside effects and are contraindicatedin patients who are addicted to opiates orare chronically taking opioid-containingmedicines. Drugs that are kappa agoniststhat inhibit the mu agonists have showngreat promise in phase 3 studies in uremicpruritus. Drugs on the horizon with potentialto be antipruritics are proteaseinhibitors, as well as vanilloid andcannabinoid receptor agonists.Given the large number of mediatorsknown to be involved in itch, developing anideal drug that will abolish all types of itchmay be a difficult task. Targeting the neuralsystem, the common pathway for itch transmission,seems a promising venue. A combinationof centrally acting drugs and topicallyacting drugs that counteract inflammationand mediators involved in itch inductionseems to be a rational strategy in amelioratingpruritus. ●●●Dr. Yosipovitch is an AssociateProfessor, Departments ofDermatology, Neurobiology& Anatomy, and RegenerativeMedicine, Wake ForestUniversity Baptist MedicalCenter, Winston-Salem, NC.<strong>The</strong> opinions expressed in this article arethose of the author and are not necessarilythose of Genentech, Inc.References1. Schmelz M, Schmidt R, Bickel A, et al. Specific Creceptors for itch in human skin. J Neurosci1997;17:8003-8008.2. Schmelz M, Hilliges M, Schmidt R, et al. Active “itchfibers” in chronic pruritus. Neurology 2003;26;61:564-566.3. Darsow U, Drzezga A, Frisch M, et al. Processing ofhistamine- induced itch in the human cerebral cortex: Acorrelation analysis with dermal reactions. J InvestDermatol 2000;115:1029-1033.4. McGlone F, Rukwied R, Hitchcock D, et al. Histamineinduced discriminative and affective responses revealedby functional MRI. In: Yosipovitch G, Greaves MW,Fleischer AB Jr, McGlone F, eds. Itch: Basic Mechanismsand <strong>The</strong>rapy. Marcel Dekker; 2004:51-61.5. Yosipovitch G, Greaves MW, Schmelz M. Itch. Lancet2003;361:690-694.6. Steinhoff M, Neisius U, Ikoma A, et al. Proteinaseactivatedreceptor-2 mediates itch: A novel pathway forpruritus in human skin. J Neurosci 2003;23:6176-6180.7. Toyoda M, Nakamura M, Makino T, et al. Nervegrowth factor and substance P are useful plasma markersof disease activity in atopic dermatitis. Br J Dermatol2002;147:71-79.8. Stander S, Steinhoff M, Schmelz M, et al.Neurophysiology of pruritus: Cutaneous elicitation ofitch. Arch Dermatol 2003;139:1463-1470.9. Yosipovitch G. Pruritus: An update. Current ProblDermatol 2003;15:135-164.10. Summey B Jr, Yosipovitch G. Pharmacologicadvances in the systemic treatment of itch. Dermatol <strong>The</strong>r2005;18:328-332.11. Yesudian PD, Wilson NJ. Efficacy of gabapentin inthe management of pruritus of unknown origin. ArchDermatol 2005;141:1507-1509.“Plaque Psoriasis” continued from page 5Figure 2. Henry’s hands.Dr. Fretzin is a board-certifieddermatologist practicing atDawes Fretzin DermatologyGroup, LLC; and a ClinicalAssistant Professor at IndianaUniversity School of Medicine,Indianapolis.<strong>The</strong> opinions expressed in this article are thoseof the author and are not necessarily those ofGenentech, Inc.Case information and photos courtesy ofKenton Busch, DO, and phase 3 clinical trials.A. Prior to RAPTIVA therapy.Individual results may vary. Photos courtesy of Kenton Busch, DO.<strong>The</strong> case of Henry, a 48-year-old man witha 2-year history of psoriasis with hand and footinvolvement, describes a patient with moderatedisease who benefited from RAPTIVA therapy.Henry has a history of hypertension and obesity.Because he preferred not to use methotrexate,cyclosporine, or acitretin, Henry had beentreating his psoriasis with topical steroids,which achieved only limited improvement. Atinitiation of RAPTIVA therapy, he had an affectedBSA of 5% (Figure 2A). After 2 months oftaking RAPTIVA 1 mg/kg/wk SC, he hadachieved approximately 50% improvement ofhis BSA. He continued to improve, and by 3months his BSA had improved to 0.5% (90%B. After 6 months of RAPTIVA1 mg/kg/wk subcutaneously.improvement). After 6 months of continuoustherapy, Henry’s hands are clear (Figure 2B).<strong>The</strong>se case studies show the responses oftwo patients to treatment with RAPTIVA. <strong>The</strong>secases should be used to assist health care professionalsin assessing the appropriateness ofRAPTIVA, and are not to be used as a substitutefor independent professional medicaljudgment. <strong>The</strong> treatment of each patient withplaque psoriasis involving the hands and feetwho enters the dermatology clinic needs to beevaluated on an individual basis. Patients whosuffer from chronic, moderate-to-severeplaque psoriasis involving the hands and feetmay benefit from RAPTIVA treatment. ●●●References1. Farber EM, Nall L. Nonpustular palmoplantar psoriasis.Cutis 1992;50(6):407-410.2. Spuls PI, Hadi S, Rivera L, Lebwohl M. Retrospectiveanalysis of the treatment of psoriasis of the palms andsoles. J Dermatolog Treat 2003;14 Suppl 2:21-25.3. RAPTIVA ® (efalizumab) [package insert]. South SanFrancisco, CA: Genentech, Inc.; June 2005.4. Gottlieb AB, Gordon KB, Hamilton TK, et al.Maintenance of efficacy and safety with continuous efalizumabtherapy in patients with moderate to severe chronicplaque psoriasis: Final Phase IIIb study results. Poster presentedat: 63rd Annual Meeting of American Academy ofDermatology; February 18-22, 2005; New Orleans, LA.5. Kimball AB, Jacobson C, Weiss S, et al. <strong>The</strong> psychosocialburden of psoriasis. Am J Clin Dermatol 2005;6(6):383-392.6. Pettey AA, Balkrishnan R, Rapp SR, et al. Patients with palmoplantarpsoriasis have more physical disability and discomfortthan patients with other forms of psoriasis: Implications forclinical practice. J Am Acad Dermatol 2003;49(2):271-275.7. Eyre RW, Krueger GG. Response to injury of skininvolved and uninvolved with psoriasis, and its relationto disease activity: Koebner and ‘reverse’ Koebner reactions.Br J Dermatol 1982;106(2):153-159.Please see www.raptiva.com or call1-877-RAPTIVA for full prescribing information.6
83 General Warren Blvd. • Suite 100Malvern, PA 19355LQ1215-7638004PRSRT STDUS POSTAGEPAIDBENSALEM, PAPERMIT #182