AETNA ARIZONA MERCY CARE PLAN (MEDICAID) Suboxone ...
AETNA ARIZONA MERCY CARE PLAN (MEDICAID) Suboxone ...
AETNA ARIZONA MERCY CARE PLAN (MEDICAID) Suboxone ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
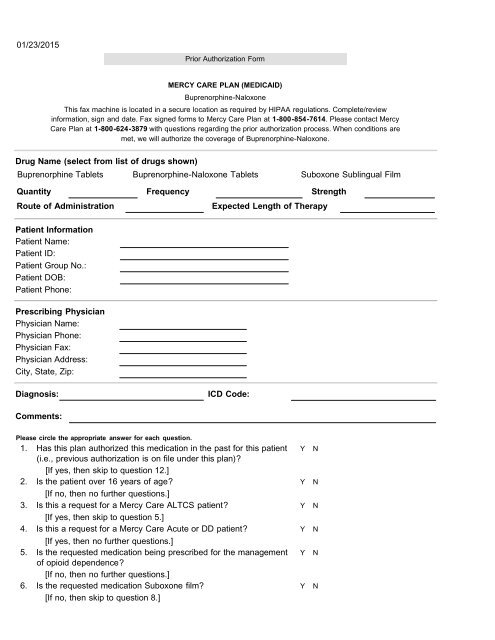
01/23/2015Prior Authorization Form<strong>MERCY</strong> <strong>CARE</strong> <strong>PLAN</strong> (<strong>MEDICAID</strong>)Buprenorphine-NaloxoneThis fax machine is located in a secure location as required by HIPAA regulations. Complete/reviewinformation, sign and date. Fax signed forms to Mercy Care Plan at 1-800 -854 -7614. Please contact MercyCare Plan at 1-800 -624 -3879 with questions regarding the prior authorization process. When conditions aremet, we will authorize the coverage of Buprenorphine-Naloxone.Drug Name (select from list of drugs shown)Buprenorphine Tablets Buprenorphine-Naloxone Tablets <strong>Suboxone</strong> Sublingual FilmQuantity Frequency StrengthRoute of AdministrationExpected Length of TherapyPatient InformationPatient Name:Patient ID:Patient Group No.:Patient DOB:Patient Phone:Prescribing PhysicianPhysician Name:Physician Phone:Physician Fax:Physician Address:City, State, Zip:Diagnosis:ICD Code:Comments:Please circle the appropriate answer for each question.1. Has this plan authorized this medication in the past for this patient Y N(i.e., previous authorization is on file under this plan)?[If yes, then skip to question 12.]2. Is the patient over 16 years of age? Y N[If no, then no further questions.]3. Is this a request for a Mercy Care ALTCS patient? Y N[If yes, then skip to question 5.]4. Is this a request for a Mercy Care Acute or DD patient? Y N[If yes, then no further questions.]5. Is the requested medication being prescribed for the management Y Nof opioid dependence?[If no, then no further questions.]6. Is the requested medication <strong>Suboxone</strong> film? Y N[If no, then skip to question 8.]
7. Has the patient experienced intolerance to Y Nbuprenorphine/naloxone tablets? Please provide details ofintolerance:[If no, then no further questions.]8. Does the prescriber possess a DATA 2000 waiver (is SAMHSA Y Ncertified)?[If no, then no further questions.]9. Does the prescriber have expertise in the treatment of addiction Y N(qualifications can include: Certificate in Addiction Psychiatry fromthe American Board of Psychiatry and Neurology, or Certified bythe American Board of Addiction Medicine, or Certificate inAddiction Medicine from the American Osteopathic Association)?Please note qualifications10. Has a comprehensive assessment for co-morbid substance Y Nabuse/dependence behaviors, including previous treatmentreceived and outcome been completed?[If no, then no further questions.]11. Is there a comprehensive substance abuse treatment plan Y Nincluding an opioid contract, psychosocial counseling, assessmentand treatment of other abuse/dependence behaviors and mentalhealth disorders, and random urine drug screens documented inthe patient’s medical record?[No further questions.]12. Has a urine drug screen been performed within the last 30-days Y Nand positive results other than buprenorphine (e.g.,benzodiazepines, amphetamines, illicit drugs, other opioids) areaddressed in the treatment plan?[If no, then no further questions.]13. Has the provider checked the Arizona Controlled Substances Y NDatabase (CSPMP) AND addressed any Opioid Contractviolations?[If no, then no further questions.]14. Is the patient continuing psychosocial counseling? Y N[If no, then no further questions.]15. Is the request for continuation of a daily dose of buprenorphine Y Nthat exceeds 24 mg per day? If yes, please provide the rationaleto support the necessity of this dose:I affirm that the information given on this form is true and accurate as of this date.Prescriber (Or Authorized) Signature and Date