Brief Cognitive-Behavioural Therapy for Children with Anxiety ...
Brief Cognitive-Behavioural Therapy for Children with Anxiety ...
Brief Cognitive-Behavioural Therapy for Children with Anxiety ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>years, participant 3, 10-year-old boy, participant 4, 11-year-old girl. Participants 2and 3 above average academic per<strong>for</strong>mance, participants 1 and 4 average per<strong>for</strong>manceat school. All participants were New Zealand European and came from twoparent families.MeasuresA comprehensive, multimethod assessment was carried out as recommended in thechild therapy and research literature (Kendall & Morris, 1991; Ronan, 1996). Theinstruments selected <strong>for</strong> the present study have known reliability and validity, andare extensively used in the treatment of anxiety disorders in children. These measureshave also demonstrated sensitivity to the effects of the treatment program onwhich this program is based (Kendall et al., 1992; Ronan & Deane, 1998). Theinterview and measures were administered by an independent and trained graduatestudent in clinical psychology.<strong>Anxiety</strong> Disorders Interview Schedule For <strong>Children</strong>A structured clinical interview, the <strong>Anxiety</strong> Disorders Interview Schedule <strong>for</strong><strong>Children</strong> (ADIS-C; Silverman, 1987), and the parallel version <strong>for</strong> parents (ADIS-P), were administered to assess <strong>for</strong> any anxiety disorder diagnoses. The interviewhas the advantage of gaining in<strong>for</strong>mation about the child’s developmental historyand current problems from the perspective of both the child and the parents(Kendall et al., 1992). The ADIS-C has undergone revisions to make it compatible<strong>with</strong> DSM IV and to improve its usefulness <strong>with</strong> younger children (Silverman,1994). The measure is increasingly used by childhood anxiety researchers, due to itshigh reliability, its structure that helps enhance rapport, and its ability to providespecific in-depth in<strong>for</strong>mation on childhood anxiety (Ronan, 1996). In terms ofdiagnostic reliability, all four initial interviews across children and parents (8 intotal) were audiotaped and blindly assessed by another rater (a trained graduate studentin clinical psychology). Across anxiety and other diagnoses, diagnostic agreementwas found to be 100%.Revised <strong>Children</strong>’s Manifest <strong>Anxiety</strong> Scale (RCMAS)The Revised <strong>Children</strong>’s Manifest <strong>Anxiety</strong> scale (RCMAS; Reynolds & Richmond,1978) is designed to measure generalised, nonspecific anxiety in children and adolescentsbetween the ages of 6 and 19 years (Gresham, 1989). The RCMAS contains37 yes/no items, <strong>with</strong> a Total <strong>Anxiety</strong> score made up of 28 items, and theremaining 9 items comprising a Lie scale. Internal consistency coefficients <strong>for</strong> theRCMAS range from .78 to .85 across age, and test retest reliability coefficients rangefrom .68 (nine months) to .98 (3 weeks) (James, Reynolds, & Dunbar, 1994). TheRCMAS has correlated .85 <strong>with</strong> the State-Trait <strong>Anxiety</strong> Inventory <strong>for</strong> <strong>Children</strong>,Trait <strong>Anxiety</strong> subscale (STAIC-T).31State-Trait <strong>Anxiety</strong> Inventory <strong>for</strong> <strong>Children</strong> (STAIC)The State Trait <strong>Anxiety</strong> Inventory <strong>for</strong> <strong>Children</strong> (STAIC; Spielberger, 1973) wasused to assess situational and temporal variations in perceived anxiety (state), aswell as more enduring anxiety tendencies (trait) in the participants. The STAICwas developed by Spielberger (1973) to measure both acute (state) and chronicBehaviour Change
Robyn D. Girling-Butcher and Kevin R. Ronan(trait) anxiety in children between the ages of 9 to 12 years. Normative data areavailable (Spielberger, 1973).<strong>Children</strong>’s Depression Inventory (CDI)The Child Depression Inventory (CDI; Kovacs, 1981) is a 27-item self-report measurerelated to the cognitive, behavioural, and affective signs of depression. It isdesigned to measure the severity of depressive symptoms in children and adolescentsbetween the ages of 8 and 17 (Kovacs, 1992). A total CDI score is obtained, as wellas a number of subscale scores; negative mood, interpersonal problems, ineffectiveness,anhedonia, and negative self-esteem (Kovacs, 1992).Coping Questionnaire – Child (CQ-C)The coping ability of the children in specific anxiety-provoking situations wasmeasured using the Coping Questionnaire-Child (CQ-C; Kendall et al., 1992). TheCQ-C assesses a child’s self-perceived ability to cope <strong>with</strong> personally anxiety producingsituations that appear to be particularly problematic. Three situations identifiedin the parent and child interviews as being most distressing to the child arelisted on the Coping Questionnaire. The child rates each situation on a 1 to 7 pointscale ranging from Not at all able to help myself (1) to Completely able to help myselffeel com<strong>for</strong>table (7). The average of the three ratings provides a measure of thechild’s perceived coping ability (Howard & Kendall, 1996). Over a 2-month interval,test–retest reliability <strong>for</strong> 20 participants <strong>with</strong> anxiety disorders was reported tobe .46 (Kendall, 1994). Another study (Ronan, 1997) using the same three situationsrelating to coping <strong>with</strong> a natural disaster found the alpha reliability to be .70(see also Ronan & Johnston, 1999).Negative Affect Self-Statement Questionnaire (NASSQ)<strong>Cognitive</strong> features were measured using the Negative Affect Self-StatementQuestionnaire (NASSQ; Ronan, Kendall, & Rowe, 1994). The NASSQ is designedto assess self-statements related to negative affect in children and young adolescentsaged 7 to 15 years. <strong>Children</strong> are asked to endorse self-statements on a scale rangingfrom Not at all (1) to All the time (5), which represents the frequency <strong>with</strong> whicheach thought occurred during the past week (Ronan et al., 1994; Ronan & Kendall,1997). The NASSQ is comprised of two separate scales of anxious self-talk: one <strong>for</strong>7- to 10-year-olds (14 items), and one <strong>for</strong> 11- to 15-year-olds (39 items). Kendall etal. (1997) report the NASSQ to be internally reliable, <strong>with</strong> a retest reliability of .73over a 2-month interval.32Child Behaviour Checklist/4–18 — Parent Form (CBCL/4–18)General aspects of childhood functioning in the participants were assessed usingthe Child Behaviour Checklist <strong>for</strong> Ages 4 to 18 (CBCL/4–18; Achenbach, 1991a).The purpose of the instrument is to measure in a standardised <strong>for</strong>mat, parents’reports of their child’s competencies, emotional functioning, and behaviour problems(Christenson, 1992). The CBCL/4–18 consists of two major sections: socialcompetencies, and problematic behaviours. The 20 social competence items assessthe amount and quality of the child’s participation in areas such as sports, hobbies,friendships, and social interaction. The 118 problem items provide scores <strong>for</strong> thefollowing scales: Total Problems, Internalising, Externalising, Withdrawn, SomaticComplaints, Anxious/Depressed, Social Problems, Thought Problems, AttentionBehaviour Change
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>Problems, Delinquent Behaviour, Aggressive Behaviour (Achenbach, 1991a).Parents are asked to rate their child on the problem items using a 3-point scale 0–2.The CBCL/4–18 can be scored on a profile that shows the items and raw scores <strong>for</strong>each scale, plus percentiles and normalised T scores, based on norms of each sex ineach age range (Achenbach, 1991a).State-Trait <strong>Anxiety</strong> Inventory <strong>for</strong> <strong>Children</strong> — Modification of TraitVersion <strong>for</strong> Parents (STAIC-T-P)Chronic or more enduring anxiety tendencies in the participants were alsoassessed by the parents filling out the State-Trait <strong>Anxiety</strong> Inventory <strong>for</strong> <strong>Children</strong>-Modifica tion of Trait Version <strong>for</strong> Parents (STAIC-T-P; Strauss, 1987). The STAIC-T-P is a modification of the trait version of Spielberger’s (1973) STAIC, and isdesigned to be used as a parent rating of the child’s trait anxiety. The STAIC-T-Phas adequate psychometric properties (Kendall & Southam-Gerow, 1996).Coping Questionnaire — Parent (CQ-P)The CQ-P parallels the CQ-C described previously. In this version, parents rate thechild’s ability to cope in the same three anxiety-provoking situations identifiedduring the diagnostic interview (Kendall, 1994). The child’s coping ability in eachsituation is rated on the same 1- to 7-point scale that is used in the CQ-C. An averageof the three ratings provides an overall rating of the child’s coping ability fromthe parents’ perspective.Child Behaviour Checklist —Teacher Report Form (TRF).The Child Behaviour Checklist — Teacher Report Form (TRF; Achenbach, 1991b)was used to assess participants’ problems and competencies in the social/emotionalarea, <strong>with</strong>in the school setting. This assessment instrument mirrors the parent versionof the CBCL, and provides in<strong>for</strong>mation on the child’s academic per<strong>for</strong>mance,adaptive functioning, and behavioural/emotional problems as rated by the child’sprimary teacher (Achenbach, 1991b). The TRF was administered at pre- and posttreatmentonly. Following treatment, all children changed teachers. While administrationof the TRF is done in these circumstances in group studies, it was notconsidered here owing to increased potential <strong>for</strong> sampling bias problems as a functionof a low sample size.ProcedureInitial contact <strong>with</strong> participants was gained through individuals contacting theresearcher by telephone call, in response to advertisements in a local communityaccess newspaper or local school newsletters. Once potential participants and theirparents consented to be involved in the study, the children undertook a screeningprocedure to ensure that they met the criteria of a primary diagnosis of a childhoodanxiety disorder. The intake evaluation involved both the parents and the childrenparticipating in structured diagnostic interviews and completing the relevant assessmentmeasures. The TRF was completed by the child’s primary teacher and wasreturned to the clinic by the parents. <strong>Children</strong> who did not meet the research criteriawere provided feedback and referred appropriately.The structured diagnostic interviews, child self-report, and parent report measureswere administered pretreatment and posttreatment. All assessments were conducted33Behaviour Change
Robyn D. Girling-Butcher and Kevin R. Ronanby a trained independent assessor (a graduate student training as clinical psychologist)who was also working <strong>with</strong>in this clinic (while this clinician did the assessment<strong>for</strong> this project, a ‘buddy system’ resulted in the senior author providingindependent evaluation services in return <strong>for</strong> this clinician’s PhD project). In addition,at every therapy session, anxiety features were assessed by child self-reportusing the STAIC-T. The parents completed the STAIC-T-P each week. Weeklyparent and child reports of the child’s coping skills were assessed using the CQ-Cand the CQ-P. Additionally, 3-month and 12-month follow-up assessments wereconducted once treatment finished, using measures administered in the pretreatmentand posttreatment evaluations.All children and parents participated in eight sessions. Typically, sessions wereheld once a week, <strong>with</strong> variations being made (holidays, conflicting schedules) asneeded. Based on additional need, two children and their parents participated in anadditional two sessions. The programs took place over 10 sessions <strong>for</strong> these two childrento enable them to complete exposure practices and work through some specificanxiety concerns.Setting and TherapistTreatment took place at the university Psychology Clinic, <strong>with</strong> several of theexposure situations carried out in the children’s natural environments. <strong>Therapy</strong>was provided by the senior author in the final stages of her training as a clinicalpsychologist.34Treatment Manual and Materials<strong>Therapy</strong> followed a 46-page manual (Girling-Butcher & Ronan, 2002) and is ashortened version of a cognitive–behavioural treatment program developed byKendall et al. (1992). The manual used in the present study outlines specific sessionobjectives and describes goals and strategies to be implemented in each of eighttreatment sessions. As recommended in the literature, a flexible and clinically sensitiveapplication of the program was applied (Kendall & Chu, 2000; Kendall,Kortlander, Chansky, & Brady, 1992). For example, it was important to consider theparticipant’s age, cognitive and social development, specific anxieties, and familyfactors, including the amount of family support, and the family’s capacity to assistthe child <strong>with</strong> mastering new situations (Howard & Kendall, 1996). A number ofprogram resources and stimulus materials were used to facilitate and rein<strong>for</strong>ce treatmentgoals and strategies, such as the recognition of anxious cues, modification ofanxious self-talk, the development of coping plans, and the provision of rewards.<strong>Children</strong> were also given a workbook (Girling-Butcher & Ronan, 2002) that outlinedimportant concepts taught, and required the child to complete a range ofexercises related to the therapy sessions. To rein<strong>for</strong>ce and generalise the copingstrategies taught, children were assigned homework tasks (referred to as STIC tasks— Show That I Can) to be completed outside of therapy.InterventionThe participants took part in 8 to 10 sessions of cognitive–behavioural therapy,which involved helping them recognise anxious cognitions, and develop anxietymanagement strategies to cope <strong>with</strong> anxiety-provoking situations. Strategiesemployed that make up the ‘FEAR Plan’ (Ronan & Deane, 1998; see also KendallBehaviour Change
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>et al., 1992) included: (a) recognising anxious feelings and somatic reactions, (b)cognitive restructuring in anxiety-provoking situations, (c) developing problemsolving steps to manage anxious reactions, and (d) self-evaluating per<strong>for</strong>mance andadministering self-rein<strong>for</strong>cement. <strong>Behavioural</strong> techniques such as relaxation, modelling,role play, exposure, and contingent rein<strong>for</strong>cement are also used. Of note,exposure began in Session 3, following introduction of the FEAR coping plan. Thedetails of the treatment program are provided in the treatment manual (Girling-Butcher & Ronan, 2002).Approximately 30 to 40 minutes of each session was spent <strong>with</strong> the therapistworking <strong>with</strong> the child only, and 10 to 20 minutes was spent <strong>with</strong> the parents only.In addition, approximately 10 to 20 minutes of each session involved the therapistworking <strong>with</strong> the parents and the child together. During this time, the strategiestaught to the child were demonstrated and rein<strong>for</strong>ced in front of the parents.Parents were also encouraged to model and coach their children outside of the therapysessions using contingency rein<strong>for</strong>cement methods. Contingency managementincorporated strategies that included praise, rewards and privileges, and plannedignoring (see also Barrett et al., 1996). The planned ignoring strategy involved theparents immediately prompting the child to engage in coping strategies (that werebeing taught in therapy) when they observed their child engaging in anxiousbehaviour. Parents were then to <strong>with</strong>draw attention from the child until the anxiousbehaviour ceased. To help parents become more involved, and as described inthe treatment manual, parent training in how to reward courageous behaviour andhelp extinguish excessive anxiety experienced by the child was carried out in thepart of each session that included the parents only.Treatment FidelityAn assessment of treatment fidelity was conducted via audiotapes. A senior clinicalpsychologist familiar <strong>with</strong>, but independent from, the treatment program listened tofour randomly selected sessions. A treatment integrity checklist was used to assesswhether the intervention objectives and procedures in the manual were followed.No protocol violations were assessed; that is, treatment was assessed to be carriedout in accord <strong>with</strong> the manual’s instructions.ResultsThe major research goal of the study was that children would no longer qualify <strong>for</strong>an anxiety disorder following the intervention. Of course, all participants received aprimary anxiety disorder diagnosis at pretreatment (see Table 1). Table 1 also showsthat all four participants no longer received a child anxiety diagnosis at posttreatmentand 3- and 12- month follow-up intervals.Child ReportChild reports are presented in Table 2. The coping ability of the participants asmeasured by the CQ-C indicated positive behaviour change over time. Childcoping skills (scores averaged across the child’s three target complaints) showed substantialchanges from pre- to posttreatment. There was a significant increase inchild reported coping ability following treatment <strong>for</strong> all participants. Scores on theRCMAS suggest a reduction in chronic anxiety <strong>for</strong> three of the four participants. Inparticular, a marked reduction in anxiety symptoms was seen in the results of35Behaviour Change
Robyn D. Girling-Butcher and Kevin R. RonanTABLE 1Diagnoses Over TimeAssessment pointsPretreatment Posttreatment 3-month 12-monthfollow-upfollow-upParticipant <strong>Anxiety</strong> diagnosis <strong>Anxiety</strong> diagnosis <strong>Anxiety</strong> diagnosis <strong>Anxiety</strong> diagnosis1 SP No diagnosis No diagnosis No diagnosisSpecific PGAD2 SP No diagnosis No diagnosis No diagnosisGAD3 GAD No diagnosis No diagnosis No diagnosisSPSpecific P4 SAD No diagnosis No diagnosis No diagnosisGADNote: SP = Social Phobia; Specific P = Specific Phobia; GAD = Generalised <strong>Anxiety</strong> Disorder;SAD = Separation <strong>Anxiety</strong> Disorder. The primary anxiety diagnosis <strong>for</strong> each participantis noted in bold. Participant 1: 8-year-old female; 2: 8-year-old female; 3: 11-year-old male;4: 10-year-old female.Participants 2 and 4. Participant 1 entered the program initially denying anxietyproblems as indicated by a T score of 35, although from the parent report and assessorand therapist observations, the child appeared to be experiencing excessive anxietyconcerns, especially in relation to social situations. Scores on the STAIC-Sshowed that <strong>for</strong> three participants there was a reduction in self-reported state anxietyfollowing treatment. In contrast, Participant 1 reported an increase in state anxietyafter treatment though both scores were in the normal range. However, therewere also beneficial changes reported in trait anxiety at posttreatment as measuredby the STAIC-T <strong>for</strong> all participants, <strong>with</strong> Participants 2, 3, and 4 showing substantialreductions.Two of the four participants reported moderate levels of depressive symptoms(CDI ≥ 13; Cole, Peeke, Martin, Truglio, & Seroczynski, 1998) at pretreatment.Following treatment, CDI scores <strong>for</strong> all participants were below this level.Reductions in depressive symptoms appeared to parallel reductions in self-reportedanxiety. In addition, there were substantial changes reported on the NASSQ aftertreatment <strong>for</strong> three of the four participants. The scores of Participant 1 were quitelow at pretreatment and remained unchanged after treatment.36Parent’s ReportsParent’s reports overall reflected improvement after treatment. Parent’s reports oftheir child’s coping, internalising and externalising behaviours are presented inTable 3. The coping ability of the participants as rated by their parents using theCQ-P indicated positive behaviour change over time. Parents reports of their child’scoping (scores averaged across the child’s three target complaints) showed substantialchanges from pre- to posttreatment (see Table 3). There was a marked increasein parent’s perception of the child’s coping skills following treatment <strong>for</strong> all participants.Specifically, parent reports of the child’s trait anxiety using the STAIC-C-PBehaviour Change
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>TABLE 2Child Self-Report Scores on Outcome MeasuresAssessment pointsMeasure Participant Pretreatment Posttreatment 3-month 12-monthfollow-up follow-upCQ-C (mean) 1 5.0 5.7 5.3 6.02 2.7 6.0 6.3 6.03 2.7 6.5 6.0 4.74 1.0 3.3 5.7 3.7STAIC-T 1 57 44 47 41(T score) 2 40 21 21 213 58 26 37 444 76 22 21 21STAIC-S 1 50 56 37 37(T score) 2 52 49 36 373 55 52 44 554 71 48 46 57RCMAS 1 35 49 37 31(T score) 2 52 32 27 313 45 44 13 394 68 41 33 33NASSQ 1 15 15 14 16(Total) 2 60 44 40 403 39 16 17 194 46 14 14 15CDI (total) 1 3 3 3 12 3 0 0 03 15 12 3 64 25 4 2 3Note: RCMAS = Revised <strong>Children</strong>’s Manifest <strong>Anxiety</strong> scale; STAIC-S = State Trait <strong>Anxiety</strong> Inventory <strong>for</strong><strong>Children</strong> – State; STAIC-T = State Trait <strong>Anxiety</strong> Inventory <strong>for</strong> <strong>Children</strong> – Trait; CDI = <strong>Children</strong>’sDepression Inventory; NASSQ = Negative Affect Self-Statement Questionnaire; CQ-C = CopingQuestionnaire <strong>for</strong> <strong>Children</strong>.showed noticeable reductions from pre- to posttreatment. All parents reporteddecreases in their child’s trait anxiety following treatment.Parent reports of the child’s internalising and externalising problems as measuredby the CBCL-4-18 showed improvement over treatment. The results of theCBCL ratings are presented in Table 3. Three participants had internalising Tscores in the clinical range at pretreatment (T ≥ 64). In contrast, these participants’scores were reduced to <strong>with</strong>in the normative range at posttreatment. T-Scores onthe anxiety/depression scale on the CBCL remained the same <strong>for</strong> one participantand decreased <strong>for</strong> three participants following the intervention. Results were asfollows: Participant 1, pre = 59, post = 59; Participant 2, pre = 70, post = 54;Participant 3, pre = 63, post = 56; Participant 4, pre = 70, post = 61. Furthermore,although all participants had externalising T scores <strong>with</strong>in normal limits at bothpre- and posttreatment, scores decreased following the intervention suggesting thatsome externalising behaviours decreased following treatment (e.g., at home actingout after school).37Behaviour Change
Robyn D. Girling-Butcher and Kevin R. RonanTABLE 3Parent Scores on Child Outcome MeasuresAssessment pointsMeasure Participant Pretreatment Posttreatment 3-month 12-monthfollow-up follow-upParent ReportCQ-P 1 2.7 5 4.3 4.3(mean) 2 2.3 6.0 5.7 6.03 2.7 6.5 6.0 7.04 2.7 5.3 6.0 5.0STAIC-T-P 1 36 30 42 41(Raw score) 2 53 31 28 333 53 31 46 314 62 52 38 33CBCL 1 55 55 52 57(Int. T) 2 77 59 55 453 65 52 54 464 72 62 64 52CBCL 1 52 46 37 46(Ext. T) 2 49 38 44 373 40 32 37 324 52 50 56 56Note: STAIC-T-P = State Trait <strong>Anxiety</strong> Inventory <strong>for</strong> <strong>Children</strong> – Trait, Parent version; CQ-P = CopingQuestionnaire – Parent report; CBCL (Int. T) = Child Behaviour .Checklist (Internalising T score);CBCL (Ext. T) = Child Behaviour Checklist (Externalising T-score). TRF (Int. T) = Teacher ReportForm (Internalising T score); TRF (Ext. T) = Teacher Report Form (Externalising T score).Teacher’s ReportsTeacher’s reports of the child’s internalising and externalising problems as measuredby the TRF remained the same or showed improvement after treatment. The TRF<strong>for</strong> two participants was unable to be completed by the children’s classroom teacherat the end of treatment due to treatment sessions continuing after the end of theschool year. Thus, the TRF <strong>for</strong> these participants was obtained following Session 7in their treatment. Results are presented in Table 4. Overall, internalising T scores<strong>for</strong> two participants remained relatively unchanged while two participants hadreduced scores following treatment. After treatment, the internalising behaviourscore <strong>for</strong> Participant 3 had decreased markedly. Finally, already low externalising Tscores remained unchanged <strong>for</strong> three of four participants.38Follow-UpOverall, changes on child self-report measures indicated that the gains made in therapywere maintained at 3-month and 12-month follow-up assessments. Specifically,changes made over the treatment time in child coping skills were maintained. Inrelation to self-reported anxiety, participants’ scores on these measures stayed <strong>with</strong>inthe normal range at follow-up intervals. Scores on other self and parent report measuresalso were maintained <strong>with</strong> the exception of Participant 1’s STAIC-T-P scores.In relation to the CBCL, the parents scored their children’s internalising andexternalising symptoms <strong>with</strong>in the normal range at 3-month follow-up <strong>with</strong> theBehaviour Change
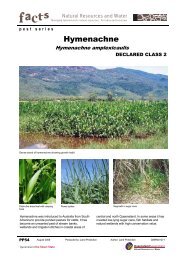
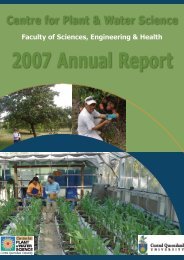
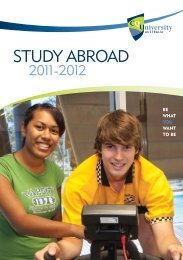
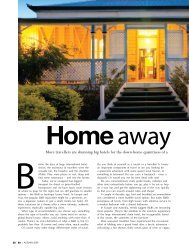
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>TABLE 4Teacher Scores on Child Outcome MeasuresAssessment PointsMeasure Participant Pretreatment PosttreatmentTeacherTRF 1 37 37(Int. T) 2 56 513 63 374 63 62TRF 1 42 42(Ext. T) 2 46 393 42 424 42 42Note: CBCL (Ext. T) = Child Behaviour Checklist (Externalising T score); TRF (Int. T) – Teacher ReportForm (Internalising T score); TRF Ext. T) – Teacher Report Form (Externalising T score).exception of Participant 4. The parent of Participant 4 scored their child just <strong>with</strong>inthe clinical range at 3-month follow-up. Their score did not differ markedly fromposttreatment, but was decreased from that of the pretreatment assessment. However,by 12-month follow-up, this score had reduced to near the normative mean.Finally, all children no longer qualified <strong>for</strong> an anxiety (or any other) diagnosis atboth follow-up intervals.Ongoing EvaluationResults indicated that parent and child reports of coping skills, and parent and childreports of the child’s trait anxiety, tended to remain stable during the baselineperiod and improved during and following treatment. The results of the coping andtrait anxiety measures are presented in Figures 1–12.Coping Skills of the ChildAs seen in Figures 1 to 4, weekly coping scores remained relatively constant duringthe baseline period (<strong>with</strong> the exception of Participant 1, the child’s report went upslightly, and the parent’s report down slightly), and steadily increased through treatment.Participant 1 reported an initially high self-reported coping rating; however,this was seen as being consistent <strong>with</strong> her lack of endorsement of anxiety symptomsacross most measures at pretreatment (see Figure 5). The child demonstrated strongavoidant behaviours early on in treatment; however, a number of obvious physicalsymptoms of anxiety, such as talking rapidly, flushed cheeks, having difficulty makingeye contact, and not being able to sit still were evident. It is noted that in this casecoping scores of the child and parent regressed towards their combined mean acrossbaseline and both remained at the same level through the first half of treatment.39Trait <strong>Anxiety</strong>As seen in Figures 5 to 12, <strong>for</strong> each child, STAIC-T-P reports remained relativelystable during baseline and as the treatment was introduced, there was a decrease inparents reports of child trait anxiety across treatment. Furthermore, on the STAIC-T the levels of child reported trait anxiety also remained relatively stable duringBehaviour Change
Robyn D. Girling-Butcher and Kevin R. Ronanbaseline (<strong>with</strong> the exception of Participant 2 whose score decreased; however, theparents STAIC-T-P score increased over baseline) and decreased over treatment.These findings suggest that during baseline, initial monitoring produced littlechange in these measures; however, once children attended the program, features oftheir anxiety improved over the course of treatment.Single Case Evaluation Criteria and Clinical SignificanceAll indices assessed across baseline and treatment were assessed against criteria usedto evaluate change in single case research (Kazdin, 2003). This included whatKazdin refers to as mean, level, slope, and latency. Of the 16 separate indicesassessed (i.e., four criteria × four separate child and parent measures), 13 were seento reasonably reflect these criteria, reflecting relative stability across baseline andchange being a function of treatment implementation. The other three (see Figures1 and 9) showed some fluctuation across baseline. However, in these cases (and aswould be expected in the program) relative stability was established across the firstcouple of sessions of treatment, prior to the beginning of exposure. Thus, concernsabout causality are reduced somewhat in these instances.Consistent <strong>with</strong> Kendall and Grove (1988; see also Sheldrick, Kendall, &Heimberg, 2001), one index of clinically significant improvement in the presentresearch was defined as change to <strong>with</strong>in normal limits on measures <strong>for</strong> which normativein<strong>for</strong>mation was provided. In the present study, clinically significant changewas evaluated using the normative mean appropriate <strong>for</strong> each participant’s age onthe relevant measures. On the parent CBCL Internalising scale, T scores followingtreatment <strong>for</strong> the three participants whose initial T scores were in the clinical range(≥ 64) were <strong>with</strong>in normal limits. On child report measures, <strong>for</strong> Participant 4, initialT scores on the RCMAS, STAIC-S, and STAIC-T were in the clinical range.Results after treatment showed clinically significant change on all three measures.In addition, and in terms of the other major index of clinically significant change,all four participants no longer met diagnostic criteria <strong>for</strong> anxiety or other disordersfollowing treatment, at 3-month follow-up, and at 1 year follow-up.40DiscussionTaken together, the present results provide support <strong>for</strong> the effectiveness of a briefversion of an established cognitive-behavioural intervention in the treatment ofanxiety disorders in children. The results of the current study are consistent <strong>with</strong>previous studies (e.g., Barrett et al., 1996; Feather & Ronan, 2006; Howard &Kendall, 1996) using various adaptations of our manualised program <strong>for</strong> treatingyouth <strong>with</strong> anxiety disorders (Kendall et al., 1992; Ronan & Deane, 1998).Multimethod assessment using diagnostic status, child-self-reports, and parentreports indicated beneficial gains <strong>for</strong> all participants from pre- to posttreatmentusing single case evaluation criteria. Moreover, further support <strong>for</strong> the interventionwas provided by the determination of clinically significant change <strong>for</strong> participantson all measures where this was possible. Importantly, all children were diagnosis freefollowing treatment and one year following treatment. The results indicated thatthe intervention was successful in eliminating both primary and secondary diagnoses<strong>for</strong> the four participants. Given the overall findings combined <strong>with</strong> thebrevity of the program, there appears to be potential <strong>for</strong> this program in outpatientchild clinic settings.Behaviour Change
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>Coping Questionnaire76ChildParentLevel of Coping54321PT B2 1 2 3 4 5 6 7 PT 3m 12mWeekly AssessmentFIGURE 1Changes in parent-reported and child-reported child coping skills (*average of scores <strong>for</strong>three target complaints across assessment and treatment sessions) <strong>for</strong> Participant 1.Coping Questionnaire76ChildParentLevel of Coping54321PT B2 B3 1 2 3 4 5 6 7 8 9 PT 3m 12mWeekly AssessmentFIGURE 2Changes in parent-reported and child-reported child coping skills (*average of scores <strong>for</strong>three target complaints across assessment and treatment sessions) <strong>for</strong> Participant 2.41Behaviour Change
Robyn D. Girling-Butcher and Kevin R. RonanCoping Questionnaire76ChildParentLevel of Coping54321PT B2 1 2 3 4 5 6 7 PT 3m 12mWeekly AssessmentFIGURE 3Changes in parent-reported and child-reported child coping skills (*average of scores <strong>for</strong>three target complaints across assessment and treatment sessions) <strong>for</strong> Participant 3.Coping Questionnaire76ChildParentLevel of Coping54321PT B2 B3 1 2 3 4 5 6 7 8 9 PT 3m 12mWeekly Assessment42FIGURE 4Changes in parent-reported and child-reported child coping skills (*average of scores <strong>for</strong>three target complaints across assessment and treatment sessions) <strong>for</strong> Participant 4.Behaviour Change
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>FIGURE 5Changes in trait anxiety (T scores) across assessment and treatment sessions <strong>for</strong>Participant 1.Trait7Level of <strong>Anxiety</strong>6654STAIC-P-32PTB21 2 3 4 5 6 7 PWeeklyT3m 1243FIGURE 6Changes in parent ratings of child trait anxiety across assessment and treatment sessions<strong>for</strong> Participant 1.Behaviour Change
Robyn D. Girling-Butcher and Kevin R. RonanFIGURE 7Changes in trait anxiety (T scores) across assessment and treatment sessions <strong>for</strong>Participant 2.44FIGURE 8Changes in parent ratings of child trait anxiety across assessment and treatment sessions<strong>for</strong> Participant 2.Behaviour Change
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>FIGURE 9Changes in trait anxiety (T scores) across assessment and treatment sessions <strong>for</strong>Participant 3.45FIGURE 10Changes in parent ratings of child trait anxiety across assessment and treatment sessions<strong>for</strong> Participant 3.Behaviour Change
Robyn D. Girling-Butcher and Kevin R. RonanFIGURE 11Changes in trait anxiety (T scores) across assessment and treatment sessions <strong>for</strong>Participant 4.46FIGURE 12Changes in parent ratings of child trait anxiety across assessment and treatment sessions<strong>for</strong> Participant 4.Behaviour Change
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>Results of the present study are similar to those reported by Kane and Kendall(1989), Kendall (1994), Kendall et al. (1997), and others (e.g., Barrett et al., 1996;Howard & Kendall, 1996). Child and parent reports on several measures providedsupport <strong>for</strong> the beneficial effects of the program across a range of functioning areas.Specifically, in the present study, improvement was shown on child reported anxiety,depressive symptoms, and self-statements related to negative affect <strong>for</strong> three ofthe four participants. In contrast, the fourth participant initially denied anxietyproblems and reported more anxiety at post-treatment on one measure (RCMAS)<strong>with</strong> his level of self-reported anxiety following treatment being in the normalrange. For this participant, the combination of no disorder at posttreatment combined<strong>with</strong> reduced denial of anxiety on self-report was encouraging.Positive changes on parent reports also followed the intervention. Using normativecomparisons, treatment returned participants to <strong>with</strong>in the normal range of functioning.For example, the three participants who had CBCL internalising ratings inthe clinical range at pretreatment had scores reduced to <strong>with</strong>in the normative rangeat posttreatment. This level of functioning was maintained at follow-up intervals.As predicted, parent and child ongoing reports of the child’s anxiety symptomsand ability to cope <strong>with</strong> individualised anxiety-provoking situations remained relativelystable at baseline and improved during treatment. Specifically, as treatmentprogressed, parents and children tended to report continuing reductions in children’strait anxiety. Similarly, anxiety-related coping ability targeted during treatment alsoshowed positive change as treatment progressed. Substantial improvements werereported from pre- to posttreatment by both children and parents.A major aspect of the present research related to the use of parents to facilitateand encourage coping behaviour in their children. Anecdotally, there were anumber of positive effects from increased parental involvement observed in the presentstudy. Specifically, the way in which parents responded to their child’s anxietyappeared to change over the course of the intervention. Parents appeared to developmore tolerance of their child’s anxiety and no longer appeared as willing to supporttheir child’s avoidant behaviours. Additionally, as the children began to manageanxious situations, parent’s positive perceptions of their child’s ability to cope andsuccessfully deal <strong>with</strong> anxious experiences clearly increased and appeared to encouragefurther involvement. With the skills that the parents were learning, they wereperhaps better able to support and coach their child to attempt a number of exposure-basedtasks outside of the therapy sessions. This appeared to facilitate more efficienttreatment delivery involving fewer sessions compared <strong>with</strong> those reported inthe United States (Kendall et al., 1992) and other Australian programs (e.g., Barrettet al., 1996). However, the exact mechanisms by which parents contributed to theprogress that their child made during the program is unknown. Furthermore,although there was an increase in exposure practice, workbook activities, and STICtasks per session compared to the original program (Kendall et al., 1992), there wasno examination made of the effects of these increases in the present study.Alternatively, whether including parents directly in this anxiety program is necessary<strong>for</strong> enhancing treatment effectiveness remains an empirical question. Thiswould involve implementing controlled treatment studies that would directlymanipulate, or assess <strong>for</strong>, varying levels of parent involvement while keeping theskills and treatment strategies of the program the same. If it is established thatactive parent involvement is related to positive outcome, research can then investigatewhich specific parent components increase effectiveness. For example, is it the47Behaviour Change
Robyn D. Girling-Butcher and Kevin R. Ronan48coping skills taught to the child and demonstrated to the parents that enhancestreatment outcome? Or is it direct parent involvement in the in vivo exposure activitiesthat is critical? The current evidence is mixed <strong>with</strong> support <strong>for</strong> increased parentinvolvement (Barrett et al., 1996; Howard & Kendall, 1996; Ronan et al., 2009)but no differences between an individual and family focused approach over the longterm (Barrett et al., 2001; see also Ronan et al., 2009). Additional research includinglong term follow-up of treatment gains is also needed.In contrast to previous studies using the manualised program (Howard &Kendall, 1996; Kendall et al., 1997), the present study incorporated both the educationaland graduated exposure components of treatment simultaneously. The resultsdemonstrate that the education component of the program does not exclusivelyneed to precede graduated exposure in order to produce positive changes in children’sability to manage anxious situations. However, the study was not designed toassess which specific aspects of our intervention were responsible <strong>for</strong> the success ofthe program. Additional research investigating the effectiveness of the specific componentsof the program would need to be undertaken to clarify that issue. With thatsaid, inspection of the figures suggests that from early sessions, the slope and magnitudeof change became more substantial. Given that exposure occurs in earlier sessionscompared to some other protocols, emphasising this component from earlieron may indeed have value (Ronan et al., 2009).Adding the exposure element earlier also has the added value of providingsome protection against at least three clinical realities: (1) the tendency <strong>for</strong> familiesto be seen <strong>for</strong> 10 sessions or fewer, including early drop-out, (2) parents wantingimmediate results, and (3) managed care session limits (Weisz & Addis, 2006).Consequently, combined <strong>with</strong> the use of a straight<strong>for</strong>ward single case strategy, thisintervention has potential to help committed clinicians and agencies better realisethe ideal of the local clinical scientist while keeping an eye on some of the realitiesthey face every day. With that said, we do acknowledge that some of the methodologicalfeatures included in this study — reflecting our commitment to evidencebasedpractice (APA Task Force on Evidence-Based Practice, 2006) — may not beseen as easy to implement (e.g., independent evaluation, multiple in<strong>for</strong>mant assessment,ongoing and follow-up evaluation). However, as we have experienced in ourown clinical work <strong>with</strong> anxious children and families (e.g., community familymental health centre), these features can be incorporated <strong>with</strong> clinician advocacy,agency commitment, and <strong>with</strong> some planning and coordination. For example, as inthis study, colleagues ‘buddying up’ to do assessment and intervention, respectively,can quite easily be done. Similarly, trained administrative assistants can be used tohelp collect data be<strong>for</strong>e treatment sessions. However, we would add that given thereality that many clinical settings do not engage in any evaluation, it is not ourintention here to provide blanket recommendations <strong>for</strong> methodologies that simplywill not be used (see Stricker & Trierweiler, 2006). Rather, this study is intendedto be an illustration that the use of a shortened evidence-supported protocol thathas some evaluation included is a much preferred state of affairs compared to anintervention <strong>with</strong> little focus and no evaluation. However, as a final word here, wewould finish by saying that the extent to which some advanced methodologicalfeatures can be incorporated should be able to be translated into clinical andorganisational benefits (APA Task Force, 2006; Weisz & Addis, 2006).A number of limitations were evident in the present study. A disadvantage ofusing a single case design is that it is not known whether results from these casesBehaviour Change
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>can be generalised to other cases. In addition, using a multiple baseline design doesnot allow <strong>for</strong> the identification of specific strategies/components that are central tosuccessful treatment outcome. Although observed effects were associated <strong>with</strong> theintervention, it is difficult to unravel a multifaceted treatment program designed totreat complex disorders such as anxiety (see also Howard & Kendall, 1996).Additionally, the minimum number of baselines and baseline assessment intervalsrecommended in the literature (Kazdin, 2003) were used prior to the start of treatment.Thus, while it would have been preferable to use a larger number of baselinesand baseline assessment intervals, this limitation is balanced against the needreflected in clinical settings to begin treatment soon after an initial visit. Withthat said, inspection of the figures prior to the implementation of treatment suggesteda reasonable level of baseline stability was achieved even <strong>with</strong> the minimumnumber of intervals used. Additionally, in terms of the two baselines used, ourapproach was to use a replication strategy to reflect clinic setting pragmatics.Initial findings across two participants were replicated across the second two.Finally, the use of a single case evaluation strategy (Kazdin, 2003) confirmedchanges across several criteria (mean, level, trend, latency). Thus, while there aredefinite limitations in the single case approach, overall we feel the approach takenhere had enough empirically based protection so as not to compromise theintegrity of the overall findings. Of course, single case findings need to be replicatedthrough group designs, including controlled trials.As all four participants had comorbid anxiety disorders, the study did not permitan examination of treatment effects <strong>for</strong> children presenting <strong>with</strong> an anxiety disordercomorbid <strong>with</strong> another psychological disorder, not an uncommon condition in children<strong>with</strong> anxiety diagnoses (Anderson, 1994; Connolly & Bernstein, 2007). Theparticipants in the present study had a primary as well as at least one secondary anxietydiagnosis at pretreatment. Both primary and secondary anxiety diagnoses wereno longer present at posttreatment, suggesting that the intervention was useful ineliminating a range of anxiety disorders in children. However, while the impact oftreatment on self-reported depression was encouraging, research is required toexamine the effects on comorbid diagnoses other than anxiety. Future studies needto investigate whether children <strong>with</strong> secondary comorbid disorders would benefitfrom the current integrated treatment package or whether more specialised interventionsthat target secondary disorders would be necessary.Future research needs to address the issue of transporting manual-based treatmentsfrom research clinics to service clinics. Bridging the gap between researchand practice requires studying the similarities and differences between researchbasedinterventions and service-based treatments (e.g., Weisz et al., 2006). Forexample, in research settings, the routine use of focused and monitored treatment(e.g., treatment manuals, audio taping sessions in order to rate treatment integrity)carried out by highly trained therapists (e.g., Curtis, Ronan, & Borduin, 2004) maysimply not be possible or realistic in a day-to-day setting (e.g., Curtis, Ronan,Heiblum, & Crellin, 2009; Hengeller, 2004). As also noted by Kendall andSoutham-Gerow (1995), the role of close and focused supervision and pre, post, andfollow-up assessment, along <strong>with</strong> additional organisation supports (Hengeller,2004), needs to be investigated in future studies (see also Weisz et al., 2006). Inaddition, further investigation into client and therapist factors involved in researchbasedversus service-based treatments is also required to close the gap. However,despite caveats, this program, and the use of pragmatic single case evaluation,49Behaviour Change
Robyn D. Girling-Butcher and Kevin R. Ronanappear to have potential in real world settings. Research into the merits of the programas well as organisational buy-in would be worthwhile.Additional research using this program <strong>with</strong> large and diverse groups of childrenfrom various ethnic backgrounds is needed. While initial indications appear promising(e.g., Kendall, 1994), future studies need to examine whether CBT programs aresuitable or effective <strong>for</strong> children from ethnic minorities, including those in countriesother than the United States (e.g., Feather, Ronan, Murupaenga, Berking, &Crellin, 2009). Culturally relevant considerations need to include the examinationof whether parents from cultural minorities view this type of treatment in clinic settingsas being appropriate <strong>for</strong> their culture. Combined <strong>with</strong> the mode of servicedelivery, consideration of cultural differences in definitions of fear-provokingobjects or events, modes of coping, and parent management style/skills appear to beparticularly important.In conclusion, <strong>with</strong> additional outcome support (e.g., RCT’s), identifying thecomponents that are necessary and effective in producing long term change, theissue of comorbidity, and the precise role of parents and family processes in the ameliorationof anxiety problems in children are all areas that need further examination.In addition, the value of early intervention programs (e.g., Dadds et al., 1997),the possible differential effects of anxiety programs in relation to age and developmentallevel (e.g., Barrett et al., 1996), and efficient modes of delivery (e.g., Rapeeet al., 2006; Spence et al., 2006) require further investigation. In relation to thecurrent findings, the challenge <strong>for</strong> researchers and practitioners is whether brieftherapy can effectively address the pragmatic and cost related issues of clinical practicewhile meeting the needs of anxious children and their families.AcknowledgmentsThe research presented in this paper <strong>for</strong>med part of the Masters thesis of the firstauthor.50ReferencesAchenbach, T.M. (1991a). Manual <strong>for</strong> the Child Behavior Checklists/4–18 and 1991 profile.Burlington: University of Vermont.Achenbach, T.M. (1991b). Manual <strong>for</strong> the Teacher’s Report Form and 1991 Profile. Burlington:University of Vermont.American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders (4thed.). Washington, DC: Author.Anderson, J.C. (1994). Epidemiological issues. In T.H. Ollendick, N.J. King, & W. Yule (Eds.),International handbook of phobic and anxiety disorders in children and adolescents (pp. 43–65). NewYork, NY: Plenum Press.APA Presidential Task Force on Evidence-Based Practice (2006). Evidence-based practice in psychology.American Psychologist, 61, 271–285.Barlow, D.H., & Hersen, M. (1984). Single case experimental designs: Strategies <strong>for</strong> studying behaviorchange (2nd ed.). New York: Pergamon Press.Barrett, P.M., Dadds, M.R., & Rapee, R.M. (1996). Family treatment of childhood anxiety: A controlledtrial. Journal of Consulting and Clinical Psychology, 64, 333–342.Barrett, P.M., Duffy, A.L., Dadds, M.R., & Rapee, R.M. (2001).<strong>Cognitive</strong>-behavioral treatment ofanxiety disorders in children: Long-term (6-year) follow-up. Journal of Consulting and ClinicalPsychology, 69, 135–141.Barrett, P.M. Rapee, R.M. Dadds, M.M., & Ryan, S.M. (1996). Family enhancement of cognitivestyle in anxious and aggressive children. Journal of Abnormal Child Psychology, 24, 187–203.Behaviour Change
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>Bernstein, G.A., & Borchardt, C.M. (1991). <strong>Anxiety</strong> disorders of childhood and adolescence: Acritical review. Journal of the American Academy of Child and Adolescent Psychiatry, 30, 519–532.Blampied, N.M. (1999). A legacy neglected: Restating the case <strong>for</strong> single-case research in cognitivebehaviortherapy. Behaviour Change, 16, 89–104.Blampied, N.M. (2000). Single-case research designs: A neglected alternative. AmericanPsychologist, 55, 960.Christenson, S.L. (1992). Review of the Child Behavior Checklist. In J.J. Kramer, & J.C. Conoley(Eds.), The eleventh mental measurements yearbook (pp. 164–166). Lincoln, Nebraska: BurosInstitute of Mental Measurements.Cole, D.A., Peeke, L.G., Martin, J.M., Truglio, R., & Seroczynski, A.D. (1998). A longitudinallook at the relation between depression and anxiety in children and adolescents. Journal ofConsulting and Clinical Psychology, 66, 451–460.Connolly, S.D. & Bernstein, G.A. (2007). Practice parameters <strong>for</strong> the assessment and treatment ofchildren and adolescents <strong>with</strong> anxiety disorders. Journal of the American Academy of Child andAdolescent Psychiatry, 46, 267–283.Curtis, N.M., Ronan, K.R., & Borduin, C.M. (2004). Multisystemic treatment: A meta-analysis ofoutcome studies. Journal of Family Psychology, 18, 411–419.Curtis, N.M., Ronan, K.R., Heiblum, N., & Crellin. K. (2009). Dissemination and effectivenessof multisystemic treatment in New Zealand: A benchmarking study. Journal of FamilyPsychology, 23(2), 119–129.Dadds, M.R., Spence, S.H., Holland, D.E., Barrett, P.M., & Laurens, K.R. (1997). Prevention andearly intervention <strong>for</strong> anxiety disorders: A controlled trial. Journal of Consulting and ClinicalPsychology, 65, 627–635.Feather, J., & Ronan, K.R. (2006). Trauma-focused <strong>Cognitive</strong> Behavioral <strong>Therapy</strong> <strong>for</strong> abused children<strong>with</strong> Post-traumatic Stress Disorder: A pilot study. New Zealand Journal of Psychology, 35,132–145.Feather, J.S., Ronan, K.R., Murupaenga, P., Berking, T., & Crellin, K. (2009). Trauma focused cognitive-behaviouraltherapy <strong>for</strong> Maori and Samoan children <strong>with</strong> multiple-abuse and PTSD in aNew Zealand child protection setting: A single-case multiple-baseline study. Manuscript inpreparation.Ginsburg, G.S., Siqueland, L., Masia-Warner, C., & Hedtke, K.A. (2004). <strong>Anxiety</strong> disorders inchildren: Family matters. <strong>Cognitive</strong> and Behavioral Practice, 11, 28–43.Girling-Butcher, R. & Ronan, K.R. (2002). <strong>Brief</strong> cognitive-behavioural therapy <strong>for</strong> anxious children:The Coping Kiwi treatment manual (2nd ed). Massey University, New Zealand: Authors.Gresham, F.M. (1989). Review of the Revised <strong>Children</strong>’s Manifest <strong>Anxiety</strong> Scale. In J.C, Conoley,& J.J. Kramer (Eds.), The tenth mental measurements yearbook (pp. 695–699). Lincoln, Nebraska:Buros Institute of Mental Measurements.Hayes, S.C. (1981). Single-case research designs and empirical clinical practice. Journal of Consultingand Clinical Psychology, 49, 193–211.Hengeller, S.W. (2004). Decreasing effect sizes <strong>for</strong> effectiveness studies — Implications <strong>for</strong> thetransport of evidence-based treatments: Comment on Curtis, Ronan and Borduin (2004).Journal of Family Psychology, 18, 420–423.Howard, B.L. & Kendall, P.C. (1996). <strong>Cognitive</strong>-behavioral family therapy <strong>for</strong> anxiety-disorderedchildren: A multiple-baseline evaluation. <strong>Cognitive</strong> <strong>Therapy</strong> and Research, 20, 423–443.James, E.M., Reynolds, C.R., & Dunbar, J. (1994). Selfreport instruments. In T.H. Ollendick, N.J.King, & W. Yule (Eds.), International handbook of phobic and anxiety disorders in children and adolescents.New York: Plenum Press.Kane, M.T., & Kendall, P.C. (1989). <strong>Anxiety</strong> disorders in children: A multiple-baseline evaluationof a cognitive-behavioral treatment. Behavior <strong>Therapy</strong>, 20, 499–508.Kashani, J.H., & Orvaschel, H. (1988). <strong>Anxiety</strong> disorders in mid-adolescence: A communitysample. American Journal of Psychiatry, 145, 960–964.Kashani, J.H., & Orvaschel, H. (1990). A community study of anxiety in children and adolescents.American Journal of Psychiatry, 147, 313–318.51Behaviour Change
Robyn D. Girling-Butcher and Kevin R. Ronan52Kazdin, A.E. (2003). Research design in clinical psychology (4th ed.). Needham Heights: Allyn &Bacon.Kazdin, A.E., & Weisz, J.R. (1998). Identifying and developing empirically supported child andadolescent treatments. Journal of Consulting and Clinical Psychology, 66, 19–36.Kendall, P.C. (1994). Treating anxiety disorders in children: Results of a randomised clinical trial.Journal of Consulting and Clinical Psychology, 62, 100–110.Kendall, P.C., Chansky, T.E., Kane, M.T., Kim, R.S., Kortlander, E., Ronan, K.R., et al. (1992).<strong>Anxiety</strong> disorders in youth: <strong>Cognitive</strong> behavioral interventions. Needham Heights, MA: Allyn &Bacon.Kendall, P.C., Chu, B.C. (2000). Retropective self-reports of therapist flexibility in a manual-basedtreatment <strong>for</strong> youths <strong>with</strong> anxiety disorders. Journal of Clinical Child Psychology, 29, 209–220.Kendall, P.C., Flannry-Schroeder, E., Panichelli-Mindel, S.M., Southam-Gerow, M., Henin, A., &Warman, M. (1997). <strong>Therapy</strong> <strong>for</strong> youths <strong>with</strong> anxiety disorders: A second randomised clinicaltrial. Journal of Consulting and Clinical Psychology, 65, 366–380.Kendall, P.C., & Grove, W.M. (1988). Normative comparisons in therapy outcome. BehavioralAssessment, 10, 147–158.Kendall, P.C., Kane, M., Howard, B., & Siqueland, L. (1990). <strong>Cognitive</strong>–behavioral treatment of anxiouschildren: Treatment manual. [Available from Phillip C. Kendall, Department of Psychology,Temple University, Philadelphia, PA 19122].Kendall. P.C., Kortlander, E., Chansky, T.E., & Brady, E.U. (1992). Comorbidity of anxiety anddepression in youth: Treatment implications. Journal of Consulting and Clinical Psychology, 60,869–880.Kendall, P.C., & Morris, R. (1991). Child therapy: Issues and recommendations. Journal of Consultingand Clinical Psychology, 59, 77–84.Kendall, P.C. & Southam-Gerow, M.A. (1995). Issues in the transportability of treatment: Thecase of anxiety disorders in youths. Journal of Consulting and Clinical Psychology, 63, 702–708.Kendall, P.C., & Southam-Gerow, M.A. (1996). Long-term follow-up of a cognitive-behavioraltherapy <strong>for</strong> anxiety-disordered youth. Journal of Consulting and Clinical Psychology, 64, 724–730.Kovacs, M. (1981). Rating scales to assess depression in children. Acta Paedopsychiatrica, 46,305–315.Kovacs, M. (1992). <strong>Children</strong>’s Depression Inventory. New York: Multi-Health Systems.Lambert, M.J. (2004). Bergin and Garfield’s handbook of psychotherapy and behavior change. NewYork: John Wiley & Sons Inc.Nock, M.K., & Kazdin, A.E. (2005). Randomized controlled trial of a brief intervention <strong>for</strong>increasing participation in parent management training. Journal of Consulting and ClinicalPsychology, 73, 872–879.Rapee, R.M., Abbott M.J., & Lyneham, H.J. (2006). Bibliotherapy <strong>for</strong> children <strong>with</strong> anxiety disordersusing written materials <strong>for</strong> parents: A randomized Controlled Trial. Journal of Consultingand Clinical Psychology, 74, 436–444.Reynolds, C.R., & Richmond, B.O. (1978). ‘What I Think and Feel’: A revised measure of children’smanifest anxiety. Journal of Abnormal Child Psychology, 6, 271–280.Ronan, K.R. (1996). Building a reasonable bridge in childhood anxiety assessment: A practitioner’sresource guide. <strong>Cognitive</strong> and Behavioral Practice, 3, 63–90.Ronan, K.R. (1997). The effects of a series of volcanic eruptions on emotional and behavioralfunctioning in children <strong>with</strong> Asthma. New Zealand Medical Journal, 110, 11–13.Ronan, K.R., Crellin, K., & McMurray, K. (2009). Childhood anxiety treatment: A comprehensivemeta-analysis and review. Manuscript in preparation <strong>for</strong> submission.Ronan. K.R., & Deane, F. (1998). <strong>Anxiety</strong> disorders. In P. Graham (Ed.), <strong>Cognitive</strong> behavior therapy<strong>for</strong> children and families: Cambridge monograph series in child and adolescent psychiatry (pp. 74–94).Cambridge: Cambridge University Press.Ronan, K.R., & Johnston, D. (1999). Behaviorally-based interventions <strong>for</strong> children following volcaniceruptions: An evaluation of effectiveness. Disaster Prevention and Management: AnInternational Journal, 8, 169–176.Behaviour Change
Treatment of <strong>Anxiety</strong> in <strong>Children</strong>Ronan, K.R. & Kendall, P.C. (1997). Self-talk in distressed youth: States-of-mind and contentspecificity. Journal of Clinical Child Psychology, 26, 330–337.Ronan, K.R., Kendall, P.C., & Rowe, M. (1994). Negative affectivity in children: Developmentand validation of a self-statement questionnaire. <strong>Cognitive</strong> <strong>Therapy</strong> and Research, 18, 509–528.Sheldrick, R.C., Kendall, P.C., Heimberb, R.G. (2001). The clinical significance of treatments: Acomparison of three treatments <strong>for</strong> conduct disordered children. Clinical Psychology Science andPractice, 8, 418–430.Silverman, W.K. (1987). <strong>Anxiety</strong> Disorders Interview <strong>for</strong> <strong>Children</strong>. State University of New Yorkat Albany: Graywind Publications.Silverman, W.K. (1994). Structured diagnostic interviews. In T.H. Ollendick, N.J., King & W.Yule (Eds.), International handbook of phobic and anxiety disorders in children and adolescents (pp.293–315). New York: Plenum Press.Spence, S.H., Holmes, J.M., March, S., & Lipp, O. (2006). The feasibility and outcome of clinicplus internet delivery of cognitive-behavior therapy <strong>for</strong> childhood anxiety. Journal of Consultingand Clinical Psychology, 74, 614–621.Spielberger, C. (1973). Manual <strong>for</strong> State-Trait <strong>Anxiety</strong> Inventory <strong>for</strong> <strong>Children</strong>. Palo Alto, CA:Consulting Psychologists Press.Strauss, C.C. (1987). Modification of trait portion of State-Trait <strong>Anxiety</strong> Inventory <strong>for</strong> <strong>Children</strong>-Parent <strong>for</strong>m. University of Florida, Grainesville. (Available from the author).Strauss, C.C. (1994). Overanxious disorder. In T.H. Ollendick, N.J., King & W. Yule (Eds.),International handbook of phobic and anxiety disorders in children and adolescents (pp. 43–66). NewYork: Plenum Press.Strauss, C.C., Lease, C.A., Last, C.G., & Francis, G. (1988). Overanxious disorder: An examinationof developmental differences. Journal of Abnormal Child Psychology, 16, 433–443.Stricker, G. (2007). The local clinical scientist. In S.G. Hofman & J. Weinberger (Eds.), The artand science of psychotherapy (pp. 85–99). New York: Routledge/Taylor & Francis Group.Stricker, G., & Trierweiler, S.J. (2006). The local clinical scientist: A bridge between science andpractice. Training and Education in Professional Psychology, S, 37–46.Weisz, J.R., & Addis, M.E. (2006). The Research-Practice Tango and other choriographic challenges:Using and testing evidence-based psychotherapies in clinical care settings. In C.D.Goodheart, A.E. Kazdin & R.J. Sternberg (Eds.), Evidence-based psychotherapy: Where practiceand research meet (pp. 179–206). Washington, DC: American Psychological Association.Weisz, J.J., Jensen-Doss, A., & Hawley, K.M. (2006). Evidence-based youth psycholotherapiesversus usual clinical care. American Psychologist, 61, 671–689.Weisz, J.R., & Weiss, B. (1989). Assessing the effects of clinic-based psychotherapy <strong>with</strong> childrenand adolescents. Journal of Consulting and Clinical Psychology, 57, 741–746.53Behaviour Change