Community resources: - Christiana Care Health System
Community resources: - Christiana Care Health System
Community resources: - Christiana Care Health System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
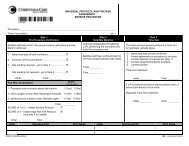
PATIENT NOTIFICATION of SERVICE & FINANCIAL RESPONSIBILITYHome health agencies have a responsibility to advise patients, in advance, about the services ordered by the physician and the extentto which payment is expected from insurance carriers or other sources, including the patient. This information is listed below.Patient’s name ID SSNSubscriber nameEmployerInsurance name HIC GroupDeductible amountCo-insurance co-payOther insurance nameThe checks below ACKNOWLEDGE MY RECEIPT AND ACCEPTANCE OF THE DOCUMENTS LISTED. These documentshave been fully explained to me and I agree to be an active participant in my plan for care at home. Consent & Information form OASIS Privacy Rights Notice of Privacy Practices Patient Rights & ResponsibilitiesADVANCE DIRECTIVES: Check the following based on patient/caregiver report and professional review of content withpatient/caregiver:I have an Advance Directive in the form of: Living will. I have not executed an Advance Directive. Durable Power of Attorney. I want more information. The Advance Directive includes a Do Not Resuscitate. Information providedCopy obtained for agency? Yes No Document location:Physician has a copy? Yes No Physician name:Name of Durable Power of Attorney: Phone #:TRADITIONAL MEDICARE or MEDICAIDEligibility Requirements Your Payment Responsibility VNA’s Responsibility to Bill Services VisitsCheck each requirement asWill bill your insurance DisciplineNo charge for services.presented to the patient.company. You require intermittent skilled careSkilled NursingFrequency& Duration Your doctor determined your need for home care & certifies a plan of care for youPhysical Therapy You are essentially confined to your home for the following reasons:Occupational Therapy Absences from home are medically contraindicatedSpeech Therapy Absences from home are for medical treatment which cannot be provided in the home. Social Work Leaving the home is short in duration, infrequent, requires considerable taxing effort, Home <strong>Health</strong> Aidassistance of another person(s) and/or assistive device.Initial Visit ApprovalALL OTHER INSURANCESSkilled NursingType of Coverage Your Payment Responsibility VNA’s Responsibility to BillPhysical TherapyOccupational TherapySpeech TherapyManaged MedicareorManaged MedicaidCoinsurance (amount you will pay afterpaying your deductible)Copayments (set amount you pay for eachvisit for each medical service)Bill sent to your insurance carrier tocalculate your coinsurance and to tellthe VNA the stated amount ofcopayment that you must pay.Social WorkHome <strong>Health</strong> AideOther health insuranceprovidersAny and all deductibles, coinsurance and/orcopayments as written in your insurancecontract.Bill sent to your insurance carrier tocalculate your coinsurance and to tellthe VNA the state amount ofcopayment that you must pay.______________________________ _________________ __________________________________ ________________Patient signature Date Responsible person/legal guardian Date______________________________ _________________ ______________________________________________________Witness signature Date Printed name & relationship of responsible persona/legal guardian