APTI ijopp - Indian Journal of Pharmacy Practice
APTI ijopp - Indian Journal of Pharmacy Practice APTI ijopp - Indian Journal of Pharmacy Practice
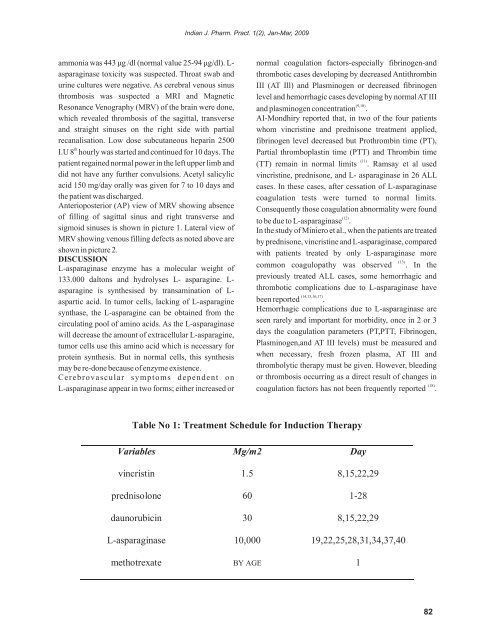
Indian J. Pharm. Pract. 1(2), Jan-Mar, 2009ammonia was 443 ìg /dl (normal value 25-94 ìg/dl). L- normal coagulation factors-especially fibrinogen-andasparaginase toxicity was suspected. Throat swab and thrombotic cases developing by decreased Antithrombinurine cultures were negative. As cerebral venous sinus III (AT Ill) and Plasminogen or decreased fibrinogenthrombosis was suspected a MRI and Magnetic level and hemorrhagic cases developing by normal AT IIIResonance Venography (MRV) of the brain were done,(9,10)and plasminogen concentration .which revealed thrombosis of the sagittal, transverse AI-Mondhiry reported that, in two of the four patientsand straight sinuses on the right side with partial whom vincristine and prednisone treatment applied,recanalisation. Low dose subcutaneous heparin 2500 fibrinogen level decreased but Prothrombin time (PT),thI.U 8 hourly was started and continued for 10 days. The Partial thromboplastin time (PTT) and Thrombin timepatient regained normal power in the left upper limb and(11)(TT) remain in normal limits . Ramsay et al useddid not have any further convulsions. Acetyl salicylic vincristine, prednisone, and L- asparaginase in 26 ALLacid 150 mg/day orally was given for 7 to 10 days and cases. In these cases, after cessation of L-asparaginasethe patient was discharged.coagulation tests were turned to normal limits.Anterioposterior (AP) view of MRV showing absenceConsequently those coagulation abnormality were foundof filling of sagittal sinus and right transverse and (12)to be due to L-asparaginase .sigmoid sinuses is shown in picture 1. Lateral view of In the study of Miniero et al., when the patients are treatedMRV showing venous filling defects as noted above are by prednisone, vincristine and L-asparaginase, comparedshown in picture 2.with patients treated by only L-asparaginase moreDISCUSSION(13)L-asparaginase enzyme has a molecular weight ofcommon coagulopathy was observed . In the133.000 daltons and hydrolyses L- asparagine. L-previously treated ALL cases, some hemorrhagic andasparagine is synthesised by transamination of L- thrombotic complications due to L-asparaginase have(14,15,16,17)aspartic acid. In tumor cells, lacking of L-asparagine been reported .synthase, the L-asparagine can be obtained from theHemorrhagic complications due to L-asparaginase arecirculating pool of amino acids. As the L-asparaginaseseen rarely and important for morbidity, once in 2 or 3will decrease the amount of extracellular L-asparagine,days the coagulation parameters (PT,PTT, Fibrinogen,tumor cells use this amino acid which is necessary forPlasminogen,and AT III levels) must be measured andprotein synthesis. But in normal cells, this synthesis when necessary, fresh frozen plasma, AT III andmay be re-done because of enzyme existence.thrombolytic therapy must be given. However, bleedingCerebrovascular symptoms dependent on or thrombosis occurring as a direct result of changes inL-asparaginase appear in two forms; either increased or(18)coagulation factors has not been frequently reported .Table No 1: Treatment Schedule for Induction TherapyVariables Mg/m2 Dayvincristin 1.5 8,15,22,29prednisolone 60 1-28daunorubicin 30 8,15,22,29L-asparaginase 10,000 19,22,25,28,31,34,37,40methotrexate BY AGE 182
Indian J. Pharm. Pract. 1(2), Jan-Mar, 2009Figure no.1: AP view of MR Venogram showing absence of filling of Sagittal sinus andright transverse and sigmoid sinuses.Figure no.2: Lateral view of MR venogram showing venous filling defects as noted above.83
- Page 37 and 38: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 39 and 40: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 41 and 42: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 43 and 44: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 45 and 46: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 47 and 48: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 49 and 50: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 51 and 52: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 53 and 54: pivotal to the rational use of medi
- Page 55 and 56: .leadership” (Cohen, 1984). A stu
- Page 57 and 58: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 59 and 60: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 61 and 62: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 63 and 64: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 65 and 66: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 67 and 68: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 69 and 70: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 71 and 72: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 73 and 74: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 75 and 76: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 77 and 78: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 79 and 80: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 81 and 82: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 83 and 84: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 85 and 86: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 87: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 91 and 92: Indian J. Pharm. Pract. 1(2), Jan-M
- Page 93 and 94: Indian J. Pharm. Pract. 1(2), Jan-M
<strong>Indian</strong> J. Pharm. Pract. 1(2), Jan-Mar, 2009ammonia was 443 ìg /dl (normal value 25-94 ìg/dl). L- normal coagulation factors-especially fibrinogen-andasparaginase toxicity was suspected. Throat swab and thrombotic cases developing by decreased Antithrombinurine cultures were negative. As cerebral venous sinus III (AT Ill) and Plasminogen or decreased fibrinogenthrombosis was suspected a MRI and Magnetic level and hemorrhagic cases developing by normal AT IIIResonance Venography (MRV) <strong>of</strong> the brain were done,(9,10)and plasminogen concentration .which revealed thrombosis <strong>of</strong> the sagittal, transverse AI-Mondhiry reported that, in two <strong>of</strong> the four patientsand straight sinuses on the right side with partial whom vincristine and prednisone treatment applied,recanalisation. Low dose subcutaneous heparin 2500 fibrinogen level decreased but Prothrombin time (PT),thI.U 8 hourly was started and continued for 10 days. The Partial thromboplastin time (PTT) and Thrombin timepatient regained normal power in the left upper limb and(11)(TT) remain in normal limits . Ramsay et al useddid not have any further convulsions. Acetyl salicylic vincristine, prednisone, and L- asparaginase in 26 ALLacid 150 mg/day orally was given for 7 to 10 days and cases. In these cases, after cessation <strong>of</strong> L-asparaginasethe patient was discharged.coagulation tests were turned to normal limits.Anterioposterior (AP) view <strong>of</strong> MRV showing absenceConsequently those coagulation abnormality were found<strong>of</strong> filling <strong>of</strong> sagittal sinus and right transverse and (12)to be due to L-asparaginase .sigmoid sinuses is shown in picture 1. Lateral view <strong>of</strong> In the study <strong>of</strong> Miniero et al., when the patients are treatedMRV showing venous filling defects as noted above are by prednisone, vincristine and L-asparaginase, comparedshown in picture 2.with patients treated by only L-asparaginase moreDISCUSSION(13)L-asparaginase enzyme has a molecular weight <strong>of</strong>common coagulopathy was observed . In the133.000 daltons and hydrolyses L- asparagine. L-previously treated ALL cases, some hemorrhagic andasparagine is synthesised by transamination <strong>of</strong> L- thrombotic complications due to L-asparaginase have(14,15,16,17)aspartic acid. In tumor cells, lacking <strong>of</strong> L-asparagine been reported .synthase, the L-asparagine can be obtained from theHemorrhagic complications due to L-asparaginase arecirculating pool <strong>of</strong> amino acids. As the L-asparaginaseseen rarely and important for morbidity, once in 2 or 3will decrease the amount <strong>of</strong> extracellular L-asparagine,days the coagulation parameters (PT,PTT, Fibrinogen,tumor cells use this amino acid which is necessary forPlasminogen,and AT III levels) must be measured andprotein synthesis. But in normal cells, this synthesis when necessary, fresh frozen plasma, AT III andmay be re-done because <strong>of</strong> enzyme existence.thrombolytic therapy must be given. However, bleedingCerebrovascular symptoms dependent on or thrombosis occurring as a direct result <strong>of</strong> changes inL-asparaginase appear in two forms; either increased or(18)coagulation factors has not been frequently reported .Table No 1: Treatment Schedule for Induction TherapyVariables Mg/m2 Dayvincristin 1.5 8,15,22,29prednisolone 60 1-28daunorubicin 30 8,15,22,29L-asparaginase 10,000 19,22,25,28,31,34,37,40methotrexate BY AGE 182


