Spring 2013 - Ontario Midwives
Spring 2013 - Ontario Midwives
Spring 2013 - Ontario Midwives
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Spring</strong> <strong>2013</strong>Association of <strong>Ontario</strong> <strong>Midwives</strong>02<strong>Midwives</strong>: providingcare across <strong>Ontario</strong>04-05Birth as a normalprocess: lowc-section rates08Breastfeeding success:supporting new moms09Baby Kristen’s story:midwife makeslife-saving call10Home birth in ruralcommunities: safetyand comfort withmidwivesQuality and Value<strong>Midwives</strong> provide primary care that leads to quality outcomes for moms and babies. The midwifery model ofcare means rates of interventions, like c-sections, are low (about half the provincial average) – bringing value to<strong>Ontario</strong>’s health care system as whole.
Midwifery Care: Quality and Value<strong>Ontario</strong> needs a health care system thatprovides quality and value for maternaland newborn health and midwives delivernothing short of that.Two years ago, a landmark study aboutwomen’s reproductive health in <strong>Ontario</strong>found that one in three women give birthby c-section (source POWER study). Thestudy focused on trends in the provincewith regards to pregnancy, childbirthand postpartum care. While the studydemonstrated positive birth outcomes, italso demonstrated high intervention rates.<strong>Midwives</strong> are skilled at managing andsupporting normal birth. Our approachis evidence-based and uses technologyjudiciously – meaning that when care ismanaged by a midwife, interventionsrates are low and outcomes areexcellent. That’s why a comparison ofc-sections rates for women in midwiferycare is half of the provincial average.A low intervention approach allows usto give women the quality care they’vecome to expect from midwives and it’sthe reason why midwives are in suchhigh demand.According to the Ministry of Healthand Long-Term Care, it costs a hospitalabout $4,237 to provide a c-section, butonly $2,739 to provide a vaginal birth.Based on these estimates, it’s predicteda reduction in c-section rates from thecurrent provincial average of 28.4% to22.8%, could result in savings of nearly$11.6 million for hospitals. <strong>Midwives</strong> arecritical in turning the tide on medicallyunnecessary interventions and onpromoting normal birth. By contrast, forexample, a home birth takes no toll onhospital resources whatsoever.The midwifery approach to care deliversboth value and quality. <strong>Midwives</strong> areleaders in maternal and newbornhealth. We have a strong vision that cancontribute to building a sustainable andresponsive health care system in <strong>Ontario</strong>during these challenging times.Lisa M. Weston, RM“A reduction in c-section rates from thecurrent provincial average of 28.4% to22.8%, could result in savings of nearly$11.6 million for hospitals.”Lisa M. Weston, AOM PresidentCost savings by reducing c-sections2010/11 <strong>Ontario</strong> overallc-section rate at 28.4%Simulated projectionat 22.8%Simulated projectionat 15%28.4%C-section costs:$188 millionTotal cost:$506 million22.8%C-section costs:$151 millionTotal cost:$494 million15%C-section costs:$99 millionTotal cost:$477 millionC-section rateVaginal delivery rateCost of c-sectionsTotal cost (vaginal birth and c-sections)Estimated savingsof $12 millionEstimated savingsof $29 millionSource: Stewart, M. C-Sections in <strong>Ontario</strong> [slide presentation]. Presentation toHQO’s Caesarean Section Expert Advisory Panel. <strong>2013</strong> Jan 21. Ministry of Health andLong-Term Care, Health Quality Branch; <strong>2013</strong>.www.aom.on.ca 3
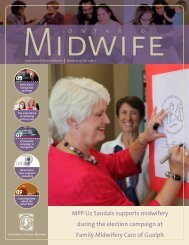
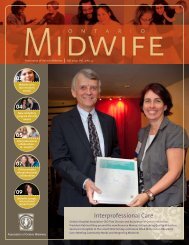
<strong>Midwives</strong>’ expertise includes VBAC births<strong>Midwives</strong> are experts in normalpregnancy, birth and newborn care.This includes vaginal birth after acaesarean section (VBAC). VBAC birthscan be complex but midwives areskilled in managing VBACs and havehigh rates of success helping womenavoid subsequent c-sections.Released in 2011, ECHO’s Project foran <strong>Ontario</strong> Women’s Health Evidence-Based Report (POWER study) showedthat 28%, or more than one in fourbabies in <strong>Ontario</strong> are born via c-section.VBAC can be a safe choice for mostwomen who havepreviously had ac-section and 75%of women whoattempt a VBAC aresuccessful accordingto a study publishedin the medicaljournal EvidenceReport/TechnologyPETERBOROUGHAssessment. VBAC is apreferable choice formany women becauseit can mean shorter hospital stays,less chance of complications relatedto surgery and greater breastfeedingsuccess.Peterborough mother Shanda Chamboknew right from the start she wantedto attempt a VBAC with her second son.“That was the reason I chosemidwifery care,” Chambo says.And although having a VBAC ultimatelyproved harder than Chambo thought,she’s glad she had her midwives thereto manage her care.Chambo now has three sons, all ofwhom were healthy but small inutero. Because of her babies’ smallsize, Chambo underwent additionaltests and follow-up throughout herpregnancies. While labouring with hersecond son, Liam, Chambo’s midwifewas able to put Chambo on fetalmonitors to confirm the baby wasdoing well and it was safe to proceedwith the VBAC.“She was able to explain that (mybaby was fine), and that’s what Iwanted and needed her to do for me,”Chambo says.Chambo’s midwife, Kathy Balazs ofKawartha Community <strong>Midwives</strong>says it is important for midwives toadvocate for clients as health careprofessionals and to be able to talk tophysicians and nurses about the clientand the clinical details of the individualsituation. <strong>Midwives</strong> can offer safealternatives and options, and cometo an agreement with other healthcare providers about how to proceedclinically and provide quality care.In the end, Chambo was able to avoida second c-section.Chambo says her birth story couldhave ended differently if it hadn’t beenfor midwifery care and is grateful forthe clinical care, advocacy and supportshe received in achieving her VBAC.For more information and decisionmakingtools regarding VBAC, visitbit.ly/WSPmJoIf 100 women plana VBAC10080Rate of repeat c-sectionin <strong>Ontario</strong>6084.3%75%4025%2046.1%75% will have a VBAC25% will have another c-section0Repeat c-section rate in<strong>Ontario</strong>(2006/07 OPSS)repeat c-section rateamong midwifery clients(2003-2008)Data source: Guise JM, Eden K, Emeis C, Denman MA, Marshall N, Fu RR, etal. Vaginal birth after cesarean: new insights. Evid Rep Technol As sess (FullRep) 2010 Mar;(191)(191):1-397.Data source: Darling L. Vaginal Birth After Cesarean Section: Outcomesof Women Receiving Midwifery Care in <strong>Ontario</strong>. Canadian Journal ofMidwifery Research and Practice. 2011;10(1):9-19.4ontario midwife • <strong>Spring</strong> <strong>2013</strong>
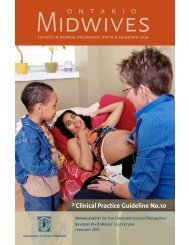
Julie Chester’s first babywas born by c-section. Butwhen she learned she waspregnant a second timearound, she opted for amidwife, hoping to be able toavoid another c-section.Even though Julie Chester’s baby Elaina was bornvia c-section, her midwife ensured they hadskin-to-skin contact as soon as possible.Change of plans: when a c-section is neededAlthough Chester was able to findmidwifery care, she was not able toavoid a second c-section. Despite thischange of plans, Chester says havingOttawa midwife Jackie Whiteheadallowed her to make every possibleeffort to avoid a c-section and itallowed her to be able to still accessmidwifery support even when hercare was transferred to a physician forthe surgery.“This time, because Jackie was there, Iwasn’t nervous,” says Chester. “She waswith me while I was in surgery and wasthere through the whole thing, talkingto me and supporting me.”Provincially, 15% of midwifery clientshave a c-section but following surgery,midwives continue to be primarycare providers for both mother andbaby. These clients still benefit fromsix weeks of postpartum care that allmidwifery clients receive.Whitehead says that even thougha transfer of care was necessary forthe c-section and a physician becamethe most responsible care providerfor Chester, once her baby was born,the baby was under midwifery careand Whitehead was responsible forproviding primary care to the baby.So when Chester’s daughter Elainacame into the world, Whitehead wasright there to receive her.“Until mom goes to the recovery room,I facilitate her having as much contactwith the baby as possible. As soon asthey hook her up to the blood pressuremonitor in the recovery room, I put thebaby skin-to-skin with her so she canstart breastfeeding. I try my best toget the baby on the breast within anhour after the birth,” says Whitehead.When mom and baby arrived onthe postpartum floor, the baby wasWhitehead’s patient. “I gave a reportto the postpartum nurses on thebaby’s health and the birth unit nursereported on Julie’s health,” explainsWhitehead.Because she was being discharged intothe care of her midwife, a primary careprovider who was available to her bypager 24/7, Chester was able leave thehospital on the second day. This meantshe could rest, heal and get to knowher new baby in her own home whilestill receiving follow-up care from hermidwife.Early discharge makes efficient useof hospital resources while stillbeing safe for women becausethey continue to receivehigh-quality midwifery care inthe community. This providesvalue to women and the <strong>Ontario</strong>40health care system as a whole.30Chester really appreciatedreceiving care from Whitehead at 20her home. The midwifery modelof postpartum care meant she 10didn’t have to leave the housewith her newborn and toddler 0while recovering from surgery.“You don’t have to packeveryone up and go.You’re more relaxed. Ihealed faster being athome. Jackie checkedmy incision andchanged my bandage,”Chester says.Whitehead sayspostpartum visits are an important timefor educating and assessing clients.Today Chester and eight-month-oldElaina are happy and healthy. Chestersays being in midwifery care for hersecond pregnancy and second c-sectionwas a very positive experience.“It almost didn’t matter that I had ac-section because I had a midwife,”she says. Chester says even though herplans might have changed, she hada positive birth experience becauseshe still had her midwife with her toprovide care and support throughouther journey.50Provincial c-section rate*28%Provincial rate15%Midwifery rateOTTAWA*Data source: Ministry of Health and Long-Term Care <strong>Ontario</strong> Midwifery Program, Midwifery Outcomes Report, 2010-2011.Highlights from the BORN <strong>Ontario</strong> LHIN Region Reports for 2009-2010; August 2011.www.aom.on.ca 5
<strong>Ontario</strong> <strong>Midwives</strong>: Quality & Value<strong>Midwives</strong> provide primary care that leads to quality outcomes formoms and babies. The midwifery model of care means that rates ofinterventions, like c-sections, are low (about half the provincialaverage) – bringing value to <strong>Ontario</strong>’s health care system as whole.Prenatal careCare during birthPostpartum carePregnant? Get a midwife!There are more than 600 registeredmidwives in <strong>Ontario</strong> serving communitiesin about 100 clinics across the province.Midwifery services are funded by theMinistry of Health and Long-Term Care, sofamilies do not pay for care out of pocket.Women do not need a referral from aphysician to access midwifery care.Routine prenatal tests<strong>Midwives</strong> arrange all routine prenatal testing includingblood tests, ultrasounds and genetic screenings as well asstandard laboratory and diagnostic tests.KETONE TEST STRIPSTest resultsmidwifery appointments1 month 2 months 3 months 4 months 5 months 6 monthsRegular visits withyour midwifeWomen will have about 12 prenatal visits with amidwife before their baby is born. Appointmentslast 30 to 45 minutes.calling...MIDWIFE<strong>Midwives</strong> on call 24/7Throughout midwifery care,midwives are on call 24 hours aday, 7 days a week, reducingemergency room visits.* Ministry of Health and Long-Term Care <strong>Ontario</strong> Midwifery Program, Midwifery Outcomes Report.† Ministry of Health and Long-Term Care <strong>Ontario</strong> Midwifery Program, Midwifery Outcomes Report, 2010-2011. Highlights from the BORN <strong>Ontario</strong> LHIN Region Reports for 2009-2010; August 2011.‡ Ministry of Health and Long-Term Care <strong>Ontario</strong> Midwifery Program, Midwifery Outcomes Report 2005-2006. Highlights from the BORN <strong>Ontario</strong> LHIN Region Reports for 2009-2010; August 2011.6 ontario midwife • <strong>Spring</strong> <strong>2013</strong>
35,000Since 1994 more than 150,000<strong>Ontario</strong> babies have beenborn under midwifery care*Choice of birthplace115,000 Home birthsHospital births<strong>Midwives</strong> in <strong>Ontario</strong> are trained inhospital and out-of-hospital birth,including birth at home and birthcentres (to open in late <strong>2013</strong>).Birth CentresUNDERCONSTRUCTIONLow intervention ratesThe c-section rate among midwifery clients in<strong>Ontario</strong> is 15%, compared to the provincial rate of28%. This represents a significant savings for thehealth care system.50403020100Provincialrate28%<strong>Ontario</strong> c-section rate†2009-10Midwiferyrate15%3 home visitsin week 17 months 8months 9 monthsweek 1 weeks 2-6The first six weeks after birth<strong>Midwives</strong> provide care to bothmom and baby for six weeks afterbirth. Over 90% of midwiferyclients are breastfeeding after sixweeks, compared with a provincialaverage of about 60% of womenon discharge from from hospitalfollowing birth.Breastfeeding rate at 6 weeks‡Overall breastfeedingrate at hospital discharge59%Midwifery breastfeeding rateat 6 weeks postpartum91%0 20 40 60 80 100www.aom.on.ca 7
Breastfeeding success: supporting new momsAfter a difficult and stressfulexperience trying to breastfeed herfirst son, Margaret So was determinedto make things different the next timearound and chose midwifery care forher second pregnancy.“Although I was armed with a lot ofinformation, it is really what happenson the ground at the critical momentthat makes breastfeeding work,” shesays. “My midwives were my lifeline.”Clients in midwifery care haveexcellent breastfeeding rates, whichlead to long-term value for the healthcare system. At birth, 96%of midwifery clientsinitiate breastfeedingand 91% are stillbreastfeeding atdischarge from carewhen baby is sixweeks old. Data fromBORN <strong>Ontario</strong> showsthat in 2009/10, theLONDONoverall provincial rateof breastfeeding at thetime women dischargedfrom hospital was 59%.Though So wanted to breastfeed heroldest son, she was not prepared forhow challenging that would be. Animproper latch right from the startresulted in her baby not getting muchmilk and increasing frustration forboth mom and baby.Last fall, Health Canada, the CanadianPaediatric Society, Dietitians of Canadaand the Breastfeeding Committeefor Canada issued a joint statementpromoting exclusive breastfeedingfor the first six months and continuedbreastfeeding for up to two yearsor beyond largely due to the healthbenefits conferred to both mom andbaby, which can last a lifetime.Health Canada states that breastfedbabies have been shown to havefewer respiratory and gastrointestinalillnesses. The first milk that comesin – called colostrum – coats thebaby’s digestive system and preventsbacterial infection. Studies havefound breastfed babies also havefewer instances of ear infections andasthma.From left: Midwife Kathi Wilson holding baby Hart, midwives Shawn Bawden and Julie Serrador, andmidwifery student Katherine Puchala.Women also benefitfrom breastfeeding.Breastfeeding triggersuterine contractions afterbirth, helping to reducethe risk of excessivepostpartum bleeding. ThePublic Health Agency ofCanada states that womenwho breastfeed are alsoless likely to develop breastcancer.Right after So’s secondson, Hart, arrived, hermidwives provided thequality care she needed toget him properly latchedand nursing minutes after hewas born.“Part of breastfeeding success isreassuring the mom they’re doing agood job. When they hear that they canrelax and the whole experience can gobetter,” says Kathi Wilson of ThamesValley <strong>Midwives</strong> in London, ON who wasone of So’s midwives.<strong>Midwives</strong> provide primary care formothers at home after the baby isborn, which gives them a uniqueopportunity to check that their clientsaren’t too overwhelmed by otherdemands, Wilson says.“We have the expertise to getbreastfeeding established and makewomen feel they can ask for help,”she says.<strong>Ontario</strong> breastfeeding ratesOverall breastfeedingrate at hospital discharge59%Midwifery breastfeeding rateat 6 weeks postpartum91%0 20 40 60 80 100Data source: Ministry of Health and Long-Term Care <strong>Ontario</strong>Midwifery Program, Midwifery Outcomes Report 2005-2006.Highlights from the BORN <strong>Ontario</strong> LHIN Region Reports for2009-2010; August 2011.So’s midwives visited her every day thefirst few days she was home to ensureshe had the support and informationshe needed to successfully breastfeedand at each visit checked that Hartwas latching well and appropriatelygaining weight. They also gave Soinstruction on different breastfeedingpositions.“The midwives told me to keep going,”she says. “I knew they were comingthe next day to check on us. It wasreally reassuring. They gave me theconfidence to hang in there and thenby day four, suddenly I heard a wetsound – my milk had come in! Hartwas drinking! We’d turned a corner…and all because my midwives werethere for me and Hart in those criticalfirst few days.”8ontario midwife • <strong>Spring</strong> <strong>2013</strong>
Baby Kristen’s story: midwife makes life saving callWhen little Kristen Seal was born,no one knew she had a heartdefect. In fact, she had two holes inher heart, which could have beenlife-threatening had it not been forquick detection and action from hermidwives during postpartum care.“We owe Kristen’s life to the midwivesfirst and foremost because they werethe ones who found it,” says momJamie Seal. “If it wasn’t for them,we don’t know when Kristen’s heartissues would have been identified.”<strong>Midwives</strong> are experts in pregnancycare, birth and postpartum care.Not everyone realizes that midwivesprovide six weeks of primary careafter the birth to both mother andnewborn.At postpartum visits at home and inmidwifery clinics, midwives checknewborns for growth, hydration,and watch for jaundice. They checkan infant’s umbilical stump, heart,lungs, hearing and overall physicaldevelopment. Skilled at providingcare, if anything is outside of normal,midwives provide appropriate care orrefer to a specialist, as was the case forKristen.<strong>Midwives</strong> also monitor and managethe mother’s health, checking herrecovery after the birth both physicallyand emotionally, and working with themother to establish breastfeeding.Kristen was only 13 days old whenmidwives Sarah Golledge and MarieSmith-Lutz made a routine home visitto check up on her and Jamie. As isnormal for midwifery care, midwiveshad seen mother and baby at homeseveral times in the previous twoweeks, but this time was different.“I do remember it quite well,” saysGolledge. “Basically when I came in,Kristen was on her mom’s lap andbefore I even picked her up, I could tellsomething wasn’t right. Her breathingwas increased and abnormal. Welistened to baby’s heart and could hearthe murmur straight away.”Golledge says it’s more common tohear an infant heart murmur on dayone and then it heals up, but none hadbeen heard inKristen’s othercheck-ups untilthis point. Shelater learnedfrom a specialistthat with thiskind of heartabnormality, itdoesn’t presentuntil the baby isa bit older.Golledgeimmediatelyphonedthe on-callpediatrician atRoyal VictoriaHospital in<strong>Midwives</strong> Sarah Golledge and Marie Smith-Lutz with 13-day-oldKristen Seal.Barrie and set up an appointment forKristen.“We were new parents. We noticedshe was breathing fast but we didn’tthink anything of it,” says Andrew Seal,Kristen’s dad. “The midwives kept uscalm. They said, ‘we hear a lot of heartmurmurs, but you’ll feel better gettingthis checked out today.’ At the hospitalthey put Kristen on oxygen right awayand later I heard the triage nurse didn’tthink she was going to make it.”Kristen was moved to Sick Kidshospital in Toronto and care continuedin and out of hospital with drugs,feeding tubes and finally, surgery.Today, Kristen is ahappy, healthy3-year-old.“We are trained todetect things that areabnormal,” Golledgesays. “Babies inmidwifery care getfrequent assessments.In circumstances likethis, it can make a realdifference.”The Seals say they will be forevergrateful to their midwives fordetecting their daughter’s heartmurmur, ensuring she expedientlyreceived the life-saving treatment sheneeded while continuing to provideprimary care to Jamie.“The midwives explained everythingto us and helped us follow up withspecialists,” says Jamie. “But the bestpart was how they genuinely caredfor us and for our daughter Kristen. Itsaved her life.”<strong>Midwives</strong> provide six weeks ofprimary care to both motherand baby after the birthBARRIEwww.aom.on.ca 9
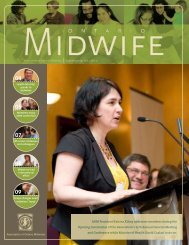
Rural family chooses home birthHome births aren’t a commonoccurrence in Espanola, a town of justover 5,000 people located 70 km westof Sudbury on the Spanish River. Mostwomen travel to Sudbury so they cangive birth in hospital. So when Danaand Melisa Rancourt announced theywere planning to have their baby athome with a midwife, their friendswere shocked and worried.“Everybody thought I was crazy,”remembers Dana. “They asked me‘What’s going to happen to the baby?’”The couple wasn’t surprised by theway people reacted to theirnews. “I think a lot ofpeople, when they firsthear about home birth,they think of LittleHouse on the Prairie,”says Melisa. “Youknow, you run downESPANOLAand get the neighbourand they boil waterand pull out sometowels.”While home birth may be unusualin Espanola, thousands of womenacross <strong>Ontario</strong> have safely givenbirth at home with midwives. Sincemidwifery becamea regulated healthprofession in1994, more than35,000 babieshave been born athome.Home birthown environment.”attended by amidwife is a safeMelisa Rancourtoption for womenwith healthypregnancies. <strong>Midwives</strong> are the onlyhealth care providers specificallytrained in home birth.In spite of the apprehension expressedby those around them, the Rancourtsnever doubted their decision.“The more we researched it, we cameto the conclusion that birth is a naturalthing. And given the fact that Dana’spregnancy was healthy and there didn’tappear to be any risk factors, we choseto have our baby in our own home, inour own environment,” says Melisa.A 2009 researchstudy conductedby Dr. EileenHutton,midwife,researcher andthe Director ofthe MidwiferyEducationProgram atMcMasterUniversity,demonstratesthat a plannedhome birth isat least as safeas a hospitalbirth forhealthy women“And given the fact that Dana’spregnancy was healthy and there didn’tappear to be any risk factors, we chose tohave our baby in our own home, in ourDana Rancourt labours in the birth pool in her home, supported by her partnerMelisa Rancourt.attended by trained midwives who arewell-integrated into the health caresystem.<strong>Midwives</strong> are trained to provideall the necessary care needed for ahome birth and they are trained inemergency care. The equipment theybring with them to home births isequivalent to what would be foundin a community hospital, includingoxygen, medications to stop bleedingand sterile instruments.Research wasn’tthe only factorthat gave thecouple confidencein their decision.Their son Lincoln(now 2) was bornat home withmidwives whenthe couple lived inBarrie. They alsohad complete trustin the knowledge and skills of theirmidwife Christina Therrien. She hasbeen a solo midwife with a full-timepractice on nearby Manitoulin Islandsince 2007. The couple say they wereimpressed by the information andexplanations Therrien provided inresponse to their questions, her quietconfidence, and the fact that she wasavailable to them 24/7.On July 16, 2012, little PresleyRancourt came into the world inexactly the way her parents planned,in a birthing pool in their own homewith Therrien providing care. Melisawas right there to support her partnerduring labour and so was Dana’smother. Lincoln was upstairs withDana’s father and brother.Melisa says that having their babyat home with a midwife meant thefamily had lots of time to enjoy thefirst miraculous minutes with theirnew daughter. “Christina put Presleyon Dana’s chest and we just sat therestaring at her. We had some quiet timeto get to know her,” says Melisa.Later, Melisa took her upstairs to meether Poppa, uncle and brother.Dana says being able to give birth athome under the care of a midwife wasan amazing experience. “It was theright choice for us,” she says.20% of midwifery clinicsare in rural or remotecommunities20%RuralUrbanSource: AOM membership department <strong>2013</strong>.10ontario midwife • <strong>Spring</strong> <strong>2013</strong>
Caring for newcomers and their Canadian babiesImmigrants and refugees in <strong>Ontario</strong>may struggle with issues relatedto poverty, trauma, social isolation,culture shock, language barriers andprecarious housing. In addition, theymay not have health insurance. Forfemale newcomers who are pregnant,navigating an unfamiliar health caresystem to find affordable care optionscan significantly add to their stress.But in <strong>Ontario</strong>, midwifery care is freeto all residents, allowing newcomersto access essential prenatal care.Karen Hayhoe is one of the midwives atThe Midwife Clinic, where more than 50% ofthe clients are newcomers to Canada.<strong>Ontario</strong> Midwife is published threetimes a year by the Association of<strong>Ontario</strong> <strong>Midwives</strong> and is availableonline at <strong>Ontario</strong><strong>Midwives</strong>.ca or youmay request a printed copy.We welcome your feedback. Pleasecontact joanna.zuk@aom.on.caAssociation of <strong>Ontario</strong> <strong>Midwives</strong>365 Bloor St. E., Suite 301Toronto, ON M4W 3L4Follow @<strong>Ontario</strong><strong>Midwives</strong> for dailynews and updates.Newcomer women are referred toclinics by community health centres ororganizations that provide services toimmigrants and refugees.Due to complicated life circumstancesor the fact they have arrived inthe country quite recently, someimmigrant and refugee women arenot able to seek care early in theirpregnancies.“We often meet clients who havehad no prenatal care or peoplewho’ve had patchwork prenatal care,”explains Manavi Handa, a midwife atWest End <strong>Midwives</strong>, which providescare to women living in Etobicoke,Rexdale and West Toronto. She saysthat before finding a midwife, clientsmay have visited a walk-in clinic orhospital ER department for a problemduring pregnancy. Some women seephysicians for prenatal care but stopattending appointments when theycan no longer afford to pay out ofpocket.Handa says that when midwivesbegin caring for women, they havethe opportunity to discover healthconditions suchas hypertensionor gestationaldiabetesthat couldall of health care.”complicate theirpregnanciesManavi Handa, RMand deliveries,and are ableto manage their care and provideappropriate treatments or referrals.Finding and treating issues early leadsto healthier mothers and babies,and means less stress on emergencyhospital resources and the health caresystem down the road.Barb Heathcote is a midwife at TheMidwife Clinic, which serves womenin East Mississauga and SouthwestEtobicoke. She has also been involvedin prenatal assessments and earlyinterventions that have ensured thesafety of women and their babies.“One client had placenta previa, acondition where the placenta is tooclose to the cervix, so it’s a requiredc-section. She wouldn’t necessarilyhave known that ifshe hadn’t been ourclient because shecouldn’t otherwiseafford prenatal care.Due to some otherfactors, she qualifiedfor financial coverageunder the communityhealth centre and hada hospital c-section,” saysHeathcote.“We know that prenatal care is one ofthe most cost effective interventions inToronto midwife Manavi Handa provides care toimmigrant and refugee women.GREATER TORONTO AREAIn both clinics,newcomers make upmore than 50% oftheir clients.Ensuring that thenewest residentsof <strong>Ontario</strong> haveaccess to appropriateprenatal care notonly protects the women and theirbabies, it also provides great value tothe health care system as a whole.“Adequate prenatal care leads tobabies that are less likely to bepremature, less likely to be small, lesslikely to be sick,” says Handa. “Small,early babies cost our health systemmassive amounts of money. A day ina neonatal intensive care unit costsour system thousands of dollars – anda preemie can be there for weeks ormonths.”“At the end of the day, these womenare having Canadian children and weknow that prenatal care is one of themost cost-effective interventions in allof health care,” says Handa.www.aom.on.ca 11
<strong>2013</strong> Association of <strong>Ontario</strong> <strong>Midwives</strong> AGM and Annual ConferenceMay 6-8, <strong>2013</strong>Hockley Valley ResortTheBalancingSustaining MidwiferyActFeatured SpeakersJust announced!Pre-conference workshopon Monday, May 6Caring for Your Clients,Caring for YourselfCindy-Lee Dennis, PhDCanada Research Chair in PerinatalCommunity Health and Professor,Lawrence S. Bloomberg Facultyof Nursing, University of TorontoTed Bober, MSW, RSWCase Manager with OMA Physicianand Professionals Health ProgramWendy KatherineManager, Women’s and Family Health,Ministry of Health and Long-Term CareOpening Ceremonies KeynoteNora SpinksCEO, Vanier Institute of the FamilyOpening KeynotePat CampbellPresident & CEO,<strong>Ontario</strong> Hospital AssociationClosing KeynoteRetreat, reconnect, renew.Register at aom.on.ca