


Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
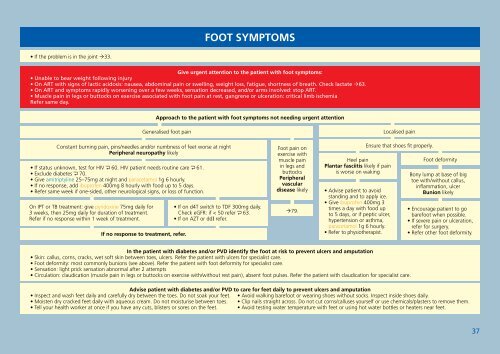
FOOT SYMPTOMS• If the problem is in the joint 33.Give urgent attention to the patient with foot symptoms:• Unable to bear weight following injury• On ART with signs of lactic acidosis: nausea, abdominal pain or swelling, weight loss, fatigue, shortness of breath. Check lactate 63.• On ART and symptoms rapidly worsening over a few weeks, sensation decreased, and/or arms involved: stop ART.• Muscle pain in legs or buttocks on exercise associated with foot pain at rest, gangrene or ulceration: critical limb ischemiaRefer same day.Approach to the patient with foot symptoms not needing urgent attentionGeneralised foot painConstant burning pain, pins/needles and/or numbness of feet worse at nightPeripheral neuropathy likely• If status unknown, test for HIV 60. HIV patient needs routine care 61.• Exclude diabetes 70.• Give amitriptyline 25–75mg at night and paracetamol 1g 6 hourly.• If no response, add ibuprofen 400mg 8 hourly with food up to 5 days.• Refer same week if one-sided, other neurological signs, or loss of function.On IPT or TB treatment: give pyridoxine 75mg daily for3 weeks, then 25mg daily for duration of treatment.Refer if no response within 1 week of treatment.If no response to treatment, refer.• If on d4T switch to TDF 300mg daily.Check eGFR: if < 50 refer 63.• If on AZT or ddI refer.Foot pain onexercise withmuscle painin legs andbuttocksPeripheralvasculardisease likely79.Heel painPlantar fasciitis likely if painis worse on waking• Advise patient to avoidstanding and to apply ice.• Give ibuprofen 400mg 3times a day with food upto 5 days, or if peptic ulcer,hypertension or asthma,paracetamol 1g 6 hourly.• Refer to physiotherapist.Localised painEnsure that shoes fit properly.Foot deformityBony lump at base of bigtoe with/without callus,inflammation, ulcerBunion likely• Encourage patient to gobarefoot when possible.• If severe pain or ulceration,refer for surgery.• Refer other foot deformity.In the patient with diabetes and/or PVD identify the foot at risk to prevent ulcers and amputation• Skin: callus, corns, cracks, wet soft skin between toes, ulcers. Refer the patient with ulcers for specialist care.• Foot deformity: most commonly bunions (see above). Refer the patient with foot deformity for specialist care.• Sensation: light prick sensation abnormal after 2 attempts• Circulation: claudication (muscle pain in legs or buttocks on exercise with/without rest pain), absent foot pulses. Refer the patient with claudication for specialist care.Advise patient with diabetes and/or PVD to care for feet daily to prevent ulcers and amputation• Inspect and wash feet daily and carefully dry between the toes. Do not soak your feet.• Moisten dry cracked feet daily with aqueous cream. Do not moisturise between toes.• Tell your health worker at once if you have any cuts, blisters or sores on the feet.• Avoid walking barefoot or wearing shoes without socks. Inspect inside shoes daily.• Clip nails straight across. Do not cut corns/calluses yourself or use chemicals/plasters to remove them.• Avoid testing water temperature with feet or using hot water bottles or heaters near feet.37
