Strategija primarne zdravstvene zaštite
Strategija primarne zdravstvene zaštite
Strategija primarne zdravstvene zaštite
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Ministarstvo zdravlja i socijalne zaštite Republike SrpskeMinistry of Health and Social Welfare Republic of Srpska<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštiteThe Primary Health Care Strategy
Vlada Republike Srpske Republic of Srpska GovernmentMINISTARSTVO ZDRAVLJA I SOCIJALNE ZAŠTITE MINISTRY OF HEALTH AND SOCIAL WELFAREwww.vladars.net
Liječenje počinje osmijehomTreatment start with a smile
UvodPolazna osnova za utvrđivanje Strategije <strong>primarne</strong><strong>zdravstvene</strong> zaštite (u daljem tekstu: PZZ) u RepubliciSrpskoj je njen Ustav, po kome se pravo na zdravlje izdravstvenu zaštitu definišu kao osnovna ljudska prava.To pravo pretpostavlja da svi raspoloživi resursi društvabudu iskorišteni u obezbjeđivanju dostupne, efikasne ikvalitetne <strong>zdravstvene</strong> zaštite, koja odgovara potrebamagrađana Republike Srpske.Najnovija istraživanja koja je objavila Evropska komisijapokazuju ekonomsku važnost zdravlja, a ne samo<strong>zdravstvene</strong> zaštite, u smislu održivog ekonomskog razvojai socijalne kohezije. Zdravlje se mora posmatratikao ekonomski potencijal i kao dio ljudskog kapitala, tekao sredstvo povećanja produktivnosti i smanjenja javnihtroškova liječenja; zdravo stanovništvo radi bolje iproizvodi više.Istraživanja i analize Svjetske banke pokazuju širokorasprostranjeno, apsolutno i relativno, siromaštvou Republici Srpskoj, Bosni i Hercegovini i zemljamaregiona. Siromaštvo predstavlja izazov za stvaranje uslovaza dugoročan i održiv ekonomski razvoj, čime bi se<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštiteBackgroundThe underlying grounds for developing the Strategyof Primary Health Care (hereinafter referred to as:PHC) in the Republic of Srpska is its Constitution,whereby the right to health and health care is definedas a fundamental human right. This right implies that allavailable resources of a society should be exploited inorder to provide accessible, efficient and quality healthcare tailored to the needs of the citizens of the Republicof Srpska.The latest research results published by the EuropeanCommission point to the economic significance ofhealth, and not only of health care, in relation to sustainableeconomic development and social cohesion. Healthmust be viewed as economic potential and an ingredientof human resources, as well as a tool for increasingproductivity and decreasing public expenditures relatedto treatment; a healthy population works better and producesmore.Studies and analysis of the World Bank demonstratewidely spread, both absolute and relative povertyin the Republic of Srpska, Bosnia and Herzegovina andThe Primary Health Care Strategy
značajno uticalo na smanjenje siromaštva. Jedan od posljednjihizvještaja Svjetske banke zagovara tezu da unapređenjezdravlja u značajnoj mjeri doprinosi postizanjuovih ciljeva.Unapređenje zdravlja umnogome zavisi od efikasnostii uspješnosti zdravstvenog sistema. Efikasnost i uspješnostzdravstvenog sistema mogu se ojačati kroz razvojPZZ u čijem je centru model porodične medicine.Reforma zdravstvenog sistema Republike Srpske jeorijentisana na:■■■■■■■Uvođenje modela porodičnog doktora;Uspostavljanje efikasnog ulaza u zdravstvenisistem;Obnavljanje infrastrukture PZZ;Slobodan izbor doktora;Uspostavljanje novih mehanizama raspodjelesredstava za zdravstvenu zaštitu i uvođenje novihmehanizama plaćanja davalaca usluga;Unapređenje organizacije, planiranja imenadžmenta u zdravstvenim ustanovama;Razvijanje i implementaciju nacionalnih zdravstvenihpolitika, strategija i programa.Reforma zdravstvenog sistema Republike Srpske, uproteklih devet godina bila je, sadržajno, ispunjena definisanjem,razvojem i usvajanjem značajnog broja dokumenata,koji su bili od izuzetne važnosti za usmjeravanje ivođenje ukupnog reformskog procesa.Najvažniji dokumenti koji su definisali početak itok reforme zdravstvenog sistema Republike Srpske su:■■<strong>Strategija</strong> razvoja <strong>zdravstvene</strong> zaštite u Republici Srpskojdo 2000. g. (Narodna skupština RS, 1996. g.);Strateški plan za reformu i rekonstrukciju zdravstvenogsistema 1997-2000. g. (Vlada RS, 1997. g.);other countries in the region. Poverty represents a challengefor ensuring conditions for a long-term and sustainableeconomic development that would significantlycontribute to the reduction of poverty. One of the latestreports of the World Bank upholds the assumption thatbetter health considerably contributes to the attainmentof these goals.Better health markedly depends on the efficiencyand success of a health system. Efficiency and successof a health system may be strengthened through developingPHC that is based on the family medicine model.The health care reform in the Republic of Srpskaaims to:■■■■■■■Introduce the family medicine model;Establish an efficient entry point into the healthsystem;Rehabilitate the PHC infrastructure;Allow a free choice of a doctor;Establish new mechanism for health care resourceallocation and introduce new provider paymentmechanisms;Enhance the organisation, planning and managementof health institutions;Develop and implement national health policies,strategies and programmes.Over the past 9 years, the health care reform in theRepublic of Srpska has abounded in definitions, developmentand adoption of a large number of documentsthat have been of particular importance for streamliningand management of the overall reform processes.Key documents, which defined the initiation andcourse of the health care reform of the Republic of Srpska,are as follows:<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštiteThe Primary Health Care Strategy
■ Zakon o zdravstvenoj zaštiti RS i Zakon ozdravstvenom osiguranju RS (Narodna skupštinaRS, 1999. g.);■ Pravilnik o specijalizaciji iz porodične medicine(Vlada RS, 1999. g.);■ Zakon o lijekovima RS (Narodna skupština RS,2001. g.);■ Zakon o zdravstvenim komorama (Narodnaskupština RS, 2001. g.);■ Plan mreže zdravstvenih ustanova RS (Vlada RS,2001. g.);■ Program politike i strategije za zdravlje u RepubliciSrpskoj do 2010. g. (Narodna skupština RS,2002. g.);■ Pravilnik o referalnom sistemu u zdravstvenojzaštiti RS (Vlada RS, 2002. g.);■ Pravilnik o dodatnoj edukaciji iz porodične medicine(Vlada RS, 2003. g.);■ Odluka o donošenju glavnih <strong>Strategija</strong> za zdravljeu Republici Srpskoj (Vlada RS, 2003. g.):1. <strong>Strategija</strong> za smanjenje razlika u zdravstvenom stanjui dostupnosti <strong>zdravstvene</strong> zaštite stanovništva;2. <strong>Strategija</strong> za reorjentaciju <strong>zdravstvene</strong> zaštite i reorganizaciju<strong>zdravstvene</strong> službe;3. <strong>Strategija</strong> za povećanje efikasnosti i kvaliteta radazdravstvenih ustanova;4. <strong>Strategija</strong> prevencije i kontrole nezaraznih bolesti.Kao operativna realizacija reforme zdravstvenogsistema Republike Srpske realizovani su, pored drugih,i sledeći projekti:■■Projekat osnovnog zdravstva (BHP);Program specijalizacije i dodatne edukacije izporodične medicine;■■■■■■■■■■■Strategy for Health Care Development in theRepublic of Srpska by the year 2000 (RS NationalAssembly, 1996);Strategic Plan for the Reform and Reconstructionof the Health System 1997-2000 (RS Government,1997);RS Health Care Act and RS Health Insurance Act(RS National Assembly, 1999);Rules on Family Medicine Specialisation (RS Government,1999);RS Pharmaceuticals Act (RS National Assembly,2001);Medical Chambers Act (RS National Assembly,2001);Plan of the RS Health Institutions Network (RSGovernment, 2001);Health Policy and Strategy Program in the Republicof Srpska by the year 2010 (RS NationalAssembly, 2002);Rules on the Referral System in RS Health Care(RS Government, 2002);Rules on Additional Training in Family Medicine(RS Government, 2003);Decision on Development of Key Health Strategiesin the Republic of Srpska (RS Government, 2003);1. Strategy for Reduction of Inequality in terms ofHealth Status and Access to Health Services;2. Strategy for Reorientation of Health Care andReorganisation of Health Services;3. Strategy for Improving Efficacy and PerformanceQuality of Health Institutions;4. Strategy for Prevention and Control of Non-Communicable Diseases.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštiteThe Primary Health Care Strategy
■■■■■■Projekat osnovnih bolničkih usluga (EHSP);Unaprećenje fizikalne rehabilitacije u zajednici(CBR);Unapređenje mentalnog zdravlja u zajednici;Podrška reformi zdravstvenog sektora EU/SZO;Opremanje domova zdravlja medicinskom opremom(tri faze);Projekat tehničke pomoći socijalnom osiguranju(SITAP).Ministarstvo zdravlja i socijalne zaštite RepublikeSrpske ima čvrstu opredjeljenost i namjeru da ustraje uprovođenju započete reforme zdravstvenog sistema RepublikeSrpske i da je dovede do kraja.Razvoj PZZ, koja će se bazirati na modelu porodičnemedicine, ima centralnu ulogu u provođenju reformezdravstvenog sistema Republike Srpske.U tom smislu, ova <strong>Strategija</strong> definiše osnovne ciljeve,pravce i aktivnosti u daljem razvoju PZZ u RepubliciSrpskoj, u narednom petogodišnjem periodu (2006– 2010. g.).Polazište i načela <strong>primarne</strong><strong>zdravstvene</strong> zaštitePolazište za Strategiju PZZ u Republici Srpskoj jeDeklaracija koja je usvojena na međunarodnoj konferencijio PZZ, održanoj u Alma Ati septembra 1978. g. u organizacijiSvjetske <strong>zdravstvene</strong> organizacije i UNICEF-a.Prema Deklaraciji iz Alma Ate, PZZ se definišekao:“Esencijalna zdravstvena zaštita, zasnovana napraktičnim, naučno ispravnim i društveno prihvatljivimmetodama i tehnologiji, opšte pristupačna pojedincima i<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštiteThe following projects, amongst others, have beenrealised as operative implementation of the health carereform of the Republic of Srpska:■■■■■■■■Basic Health Project (BHP);Program for specialisation and additional trainingin family medicine;Essential Hospital Services Project (EHSP);Improvement of Community-Based Rehabilitation;Improvement of Community-Based Mental Health;EU/WHO Support to the Health Sector Reform;Equipping of health centres with medical equipment(three stages);Social Insurance Technical Assistance Project(SITAP).The Ministry of Health and Social Welfare of theRepublic of Srpska is strongly committed and intend topursue the implementation of the launched health carereform of the Republic of Srpska.PHC development, which will be based on the familymedicine model, has a central role in the implementationof the RS health care reform.To this end, the Strategy defines fundamental goals,directions and activities to be pursued in the developmentof primary health care in the Republic of Srpskain the next five-year period (2006 – 2010).Foundation and principles ofprimary health careThe foundation of the PHC Strategy of the Republicof Srpska is the Declaration adopted at the internationalconference on PHC, which was held in AlmaThe Primary Health Care Strategy
porodicama u zajednici uz njihovo puno učešće, po cijenikoju ta zajednica i zemlja mogu da podnesu u svakojfazi njihovog razvoja, u duhu oslanjanja na sopstvenemogućnosti i samo-odlučivanje. Ona istovremeno predstavljaintegralni dio zdravstvenog sistema zemlje, čija jecentralna funkcija i glavno žarište i sveukupnog socijalnogi ekonomskog razvoja zajednice. Ona je prvi nivokontakta pojedinca, porodice i zajednice sa nacionalnimzdravstvenim sistemom, približavajući zdravstvenu zaštitušto je moguće više mjestu gdje ljudi žive i rade, konstituišućiprvi element u kontinuiranom procesu <strong>zdravstvene</strong>zaštite”.Primarna zdravstvena zaštita predstavlja osnovcjelokupnog sistema <strong>zdravstvene</strong> zaštite, a to znači dase u okviru <strong>primarne</strong> <strong>zdravstvene</strong> zaštite putem kostefektivnihintervencija kao što su: promocija zdravlja,prevencija bolesti, rano otkrivanje bolesti blagovremenitretman i rehabilitacija, rješava najveći dio zdravstvenihproblema i zdravstvenih potreba stanovništva uz aktivnupodršku pojedinaca, porodice i zajednice u cjelini.Primarna zdravstvena zaštita treba da ima centralnomjesto i ulogu u strategijama razvoja zdravstvenihsistema.Primarna zdravstvena zaštita se ne poistovjećuje saporodičnom medicinom niti sa vanbolničkom službom,iako se najveći dio zdravstvenih potreba i najveći broj mjera<strong>primarne</strong> <strong>zdravstvene</strong> zaštite ostvaruje preko timova porodičnemedicine, zbog čega primarna zdravstvena zaštitatreba da bude osposobljena kadrovski i materijalno kakobi mogla u potpunosti ostvariti svoje mjesto i ulogu.Tim porodične medicine je u središtu zdravstvenogsistema, a institucionalno je predstavljen preko ambulantiporodične medicine, grupne prakse ili doma zdravlja.Ata in September 1978 under the auspices of the WorldHealth Organisation and UNICEF.The Declaration of Alma Ata views primary healthcare as follows:Primary health care is essential health care based onpractical, scientifically sound and socially acceptable methodsand technology made universally accessible to individualsand families in the community through their full participationand at a cost that the community and countrycan afford to maintain at every stage of their developmentin the spirit of self-reliance and self-determination. At thesame time, it forms and integral part both of the country’shealth system, of which it is the central function and mainfocus, and of the overall social and economic developmentof the community. It is the first level of contact ofindividuals, the family and community with the nationalhealth system bringing health care as close as possible towhere people live and work, and constitutes the first elementof a continuing health care process.Primary health care constitutes the foundation ofthe overall health care system, which means that primaryhealth care, relying of cost-effective interventions, suchas health promotion, illness prevention, early detectionof diseases, timely treatment and rehabilitation, will resolvethe majority of health problems and health needsof the population with the active support of individuals,family and community as a whole.Primary health care should have the central roleand place in strategies of health system development.Primary health care is not identical with familymedicine or outpatient services, although the majorityof health needs and primary health care measures aredealt with and implemented through family medicine<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštiteThe Primary Health Care Strategy
Dom zdravlja ostaje kao institucionalni oblik organizovanja,ali se mora organizaciono prilagoditi modeluporodične medicine i biti nosilac <strong>primarne</strong> <strong>zdravstvene</strong>zaštite. Nova uloga doma zdravlja je logistička podrškatimu porodične medicine bez obzira na to ko je osnivač,putem konsultativno-specijalističkih ambulanti i dijagnostičkihslužbi. Dom zdravlja koordinira rad ambulantiporodične medicine.Na PZZ se gleda kao na “integralni, permanentnii sveobuhvatni dio formalnog sistema <strong>zdravstvene</strong>zaštite u svim državama”, odnosno ona se shvata kao“sredstvo kojim se balansiraju dva osnovna cilja sistema<strong>zdravstvene</strong> zaštite – optimizacija i uravnoteženost u distribucijizdravstvenih usluga”. Njen cilj je rješavanje uobičajenihproblema u zajednici putem pružanja promotivnih,preventivnih, kurativnih i rehabilitacionih usluga,koje unapređuju zdravlje i dobrobit stanovništva. Onaintegriše <strong>zdravstvene</strong> usluge u slučaju postojanja jednogi/ili više zdravstvenih problema i u koštac se hvata sakontekstom u kojem se određeno oboljenje pojavljujei utiče na ljude u smislu njihovog odgovora na njihove<strong>zdravstvene</strong> probleme. PZZ je zdravstvena zaštita kojaorganizuje i racionalizuje angažman resursa, osnovnih ispecijalističkih, koji su usmjereni ka promociji, održavanjui unapređenju zdravlja.Primarna zdravstvena zaštita kao nivoPZZ kao nivo <strong>zdravstvene</strong> zaštite predstavlja mjestogdje se ostvaruje prvi kontakt građana sa zdravstvenimsistemom. To je, dakle, mjesto ulaska u zdravstvenisistem ili, simbolično rečeno, to su “vrata” zdravstvenogsistema. U tom smislu se doktori PZZ odnosno doktori<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite10teams, which is why primary health care should be capacitatedin terms of staffing and resources, to fully fulfilits role and place.The family medicine team is the focus of the healthsystem and is represented, in institutional terms, by familymedicine clinics, shared practices or health centres.The health centre will remain as an institutional organisationalform, but will need to adapt to the familymedicine model and function as a tier of primary healthcare. The new role of the health centre will be logisticalsupport to family medicine teams irrespective of whois its founder, through consultative-specialist clinics anddiagnostic services. The health centre will coordinate thework family medicine clinics.PHC is viewed as “an integral, continuing and comprehensivepart of the country’s formal health system”, i.e. it is conceived as “a tool for balancing two major goalsof health care - optimising and equal distribution ofhealth services”. It aims to address the main health problemsin the community, providing promotive, preventive,curative and rehabilitative services accordingly, that improvehealth and welfare of the population. It integrateshealth services where one and/or more health problemsemerge and deals with the context in which a disease appearsand affects the people in terms of their response totheir health problems. PHC is health care that organisesand rations the employment of resources, both fundamentaland specialist, which are oriented towards promotion,preservation and improvement of health.Primary health care as a levelAs a health care level, PHC constitutes the first levelof contact of individuals and with the health system.The Primary Health Care Strategy
porodične medicine nazivaju “čuvarima vrata” (od engl.“gate keeper”). PZZ treba biti osposobljena da rješavanajmanje 80% svih zdravstvenih problema.Sveobuhvatna primarna zdravstvena zaštitaKoncept “sveobuhvatne PZZ” u velikoj mjeri koristise u mnogim razvijenim državama, i sastoji se od širokograspona <strong>zdravstvene</strong> edukacije, promocije zdravlja,prevencije bolesti, liječenja i rehabilitacije.Primarna zdravstvena zaštita kao ključni procesPZZ je ključni proces u okviru zdravstvenog sistema.Podrazumijeva prvi kontakt, filter za ulazak u zdravstvenisistem, kontinuitet, sveobuhvatnost i koordinaciju.Prvi kontakt koji pacijent ostvaruje, omogućen je utrenutku kada se za njim ukaže potreba; kontinuitet sefokusira na dugoročno zdravlje građana, a ne samo nakratko trajanje oboljenja; sveobuhvatnost predstavaljaodređeni raspon usluga, koje su odgovarajuće u smisluzajedničkih zdravstvenih problema stanovništva, kojesu dostupne na nivou PZZ i gdje ne postoji podjela postarosti, polu i bolesti; koordinacija u PZZ podrazumijevaplanirani put pacijenta kroz više nivoe zdravstvenogsistema u kome ključnu ulogu igraju doktori porodičnemedicine.Tim porodične medicine u primarnojzdravstvenoj zaštitiOsnovna organizaciona struktura koja će biti nosilacposlova i aktivnosti na nivou PZZ je tim porodičnemedicine.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite11Therefore, it is an entry point of the health system, or,in symbolic terms, the “gate” of the health system. Inthis sense, PHC doctors, i. e. family medicine doctors arecalled “gate-keepers”. PHC should be capable of resolvinga minimum of 80% of all health problems.Comprehensive primary health careThe concept of “comprehensive PHC” is generallyused in many developed countries and entails a widerange of health education, health promotion, preventionof diseases, treatment and rehabilitation.Primary health care as the major processPHC is the major process within a health system. Itimplies the first level of contact, an entry filter of the healthsystem, continuity, comprehensiveness and coordination.The first level of contact of a patient is made possiblewhen a need for it arises; continuity focuses on long-lastinghealth of citizens, not only on short-lasting treatment;comprehensiveness constitutes a range of services that areadequate in terms of common health problems of the population,which are accessible at the PHC level and wherethere is no discrimination as to age, sex and health problems;PHC coordination refers to the planned pathway of apatient to the upper levels of the health system, where thecentral role is played by family medicine doctors.Family medicine team in primary health careThe basic organisational structure that will be theagent of tasks and activities at the PHC level is the familymedicine team.The Primary Health Care Strategy
U prelaznom periodu tim porodične medicine sesastoji od specijaliste porodične medicine ili doktora medicinesa završenom dodatnom edukacijom ili specijalistedruge grane medicine sa završenom dodatnom edukacijomi dvije medicinske sestre/tehničara.Dugoročno, od 2010. godine, tim porodične medicinesastojaće se: od doktora - specijaliste porodične medicineili specijaliste druge grane medicine sa završenom dodatnomedukacijom i dvije medicinske sestre/tehničara.Porodični doktor, kao vođa tima, je kliničar kojitreba da obavlja sljedeće poslove: promociju zdravlja iprevenciju bolesti, predsimptomatsko otkrivanje bolesti,ranu dijagnozu, konačnu dijagnozu, upravljanje bolestima,upravljanje komplikacijama kod bolesti, oporavakpacijenta, palijativnu njegu i savjetovanje porodice u vanrednimokolnostima.Razlozi za reformu <strong>primarne</strong><strong>zdravstvene</strong> zaštiteNejednak pristup zdravstvenoj zaštitiNejednak pristup zdravstvenoj zaštiti uzrokovan jevisokom stopom zdravstveno neosiguranih građana. Visokje nivo direktnog plaćanja zdravstvenih usluga (“plaćanjeiz džepa”), čime se stvaraju dodatne barijere pristupui povećava nejednakost, što dovodi do povećanjavulnerabilnosti građana na posljedice bolesti.Bolja zaštita najugroženijih kategorija stanovništvaod zdravstvenih rizika i rješavanje nejednakosti u pristupuzdravstvenoj zaštiti ključ su za smanjenje siromaštva ipoboljšanje socijalne kohezije.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite12The family medicine team consists of a doctor - familymedicine specialist and two nurses/medical technicians.The family doctor, as the team leader, is the onlyclinician that should perform the following tasks: healthpromotion and disease prevention, pre-symptomatic detectionof diseases, early diagnostics, final diagnosis, diseasemanagement, disease complications management,recovery of patients, palliative care, and consulting offamilies in extraordinary circumstances.Reasons for the primary healthcare reformKey health care issues to be considered by the RSPHC Strategy may be summarised as follows:■ Unequal access to health care,■ Inefficient delivery of health care services,■ Inadequate health care financing,■ Inadequate structure of human resources,■ Ageing population.Unequal access to health careUnequal access to health care is caused by a highnumber of individuals with no health care insurance.The level of direct payment for health services (”out-ofpocket”payment) is quite high, thus constituting an additionalbarrier to the access and aggravating inequality,which renders individuals more vulnerable to the effectsof a disease.A better protection of the most vulnerable groupsof the population from health risks, and dealing withThe Primary Health Care Strategy
Neefikasno pružanje uslugaNaslijeđena PZZ okrenuta je bolesti i terapiji, epizodnojzaštiti i pasivnom prijemu pacijenata, većem korišćenjukonsultativno-specijalističkih i dijagnostičkih usluga,te bolničkog liječenja.Postoji fragmentacija prvog kontakta građana sazdravstvenim sistemom uz ograničenu ulogu “vratara”,a kontinuitetu <strong>zdravstvene</strong> zaštite posvećuje se neodgovarajućapažnja. Na nivou PZZ usluge se i dalje,u najvećem broju domova zdravlja, pružaju na osnovusta rosne dobi, pola ili vrste bolesti u specijalizovanim dispanzerimai službama, što nije najefikasniji način korišćenjaraspoloživih resursa.Neefikasnost u aranžmanima pružanja zdravstvenihusluga jasno je vidljiva kada se prikažu rashodi u zdravstvu,gdje se naglasak i dalje stavlja na sekundarnu itercijarnu zdravstvenu zaštitu, a na štetu PZZ.Neadekvatno finansiranje <strong>zdravstvene</strong> zaštiteGlavni nedostaci sistema finansiranja <strong>zdravstvene</strong>zaštite u Republici Srpskoj su sljedeći:■ Nesrazmjer između raspoloživih finansijskih sredstavai garantovanih prava;■ Nesrazmjer između ukupnog kapaciteta zdravstvenogsistema i raspoloživih finansijskih sredstava;■ Neefektivno uključivanje samozaposlenih i poljoprivednikau obavezno zdravstveno osiguranje;■ Veliki broj korisnika, koji su isključeni iz plaćanjaličnog doprinosa, nema zdravstveno osiguranjejer oni koji bi trebali da uplaćuju doprinos za ovekategorije to uglavnom ne rade (vanbudžetskifondovi i vladin budžet);<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite13inequality in access to health care is the key to povertyreduction and enhanced social cohesion.Inefficient delivery of health care servicesThe PHC we inherited focuses on disease and therapy,episodic care and passive admission of patients, ahigher utilisation rate of consultative-specialist and diagnosticservices and hospital treatment.The first level of contact of individuals with thehealth system is fragmented, where the gate-keeping roleis limited and insufficient attention is paid to the continuityof health care. At the PHC level, in the majorityof health centres, services are still delivered according toage, sex or type of disease, by specialised departmentsor services, which does not constitute the most efficientway of utilisation of available resources.Inefficiency of health services delivery is evidencedby health expenditures, where an emphasis remains onthe secondary and tertiary health care to the detrimentof primary health care.Inadequate health care financingThe core shortcomings of the RS health financingare as follows:■ Disproportion of available funds and guaranteedentitlements;■ Disproportion of the aggregate capacities of thehealth system and available funds;■ Ineffective involvement of the self-employedand farmers into the mandatory health insurancescheme;The Primary Health Care Strategy
■■Niske stope ubiranja doprinosa;Visoki ukupni troškovi u zdravstvu.Konačan rezultat je taj da znatan dio građana jošuvijek nije pokriven šemom obaveznog zdravstvenog osiguranja,koja je zamišljena da obezbijedi univerzalno pokrićei pristup zdravstvenoj zaštiti.Neadekvatna struktura ljudskih resursaU zdravstvenom sistemu Republike Srpske ne postojistrategija na polju ljudskih resursa. Neophodno jeizraditi takvu strategiju koja će identifikovati postojećei buduće potrebe, planove za implementaciju, te finansijskeimplikacije kroz primjenu ove strategije.Trenutni broj doktora i medicinskih sestara / tehničarana nivou PZZ nije dovoljan kako bi se provelareforma PZZ prema modelu porodične medicine.Na nivou PZZ se nalazi velik broj doktora-specijalistarazličitih grana medicine, koji je naslijeđen iz prethodnogsistema. Ovakva struktura doktora na primarnomnivou otežava provođenje reforme i uvođenje modelaporodične medicine.Starenje populacijeUz stanovništvo koje ubrzano stari, opterećenjeposljedičnim bolestima će se i dalje povećavati. Najvećiizazov za javno zdravstvo u Republici Srpskoj predstavljakontrola epidemije masovnih nezaraznih bolesti.Prilagođavanje zdravstvenog sistema značajnim demografskim,epidemiološkim i sociološkim promjenama,njegovo osposobljavanje da se suoči sa predviđenim dodatnimopterećenjem i novonastalim potrebama, i njego■■■A large number of health care users who areexempted from paying social contributions and arenot members of the health insurance fund, sincethe institutions responsible for paying the said contributionsfor these categories generally fail to do it(extra-budgetary funds and Government’s Budget);Low rates of contribution collection;High total health care costs.The ultimate result is that a considerable numberof people still remain outside the mandatory health insurancescheme, which is conceived in such a way as toensure universal coverage and access to health care.Inadequate structure of human resourcesIn the RS health system, not a single strategy dealswith human resources. It is necessary to develop such astrategy, which will identify the current and future needs,implementation plans, as well as financial implicationsof its application.The current number of doctors and nurses/medicaltechnicians at the PHC level does not suffice for the implementationof the family medicine-based PHC reform.At the PHC level, there is a large number of doctors- specialists in various branches of medicine, whichis a legacy of the previous system. Such a profile of doctorsat the primary health care level impedes the implementationof the reform and introduction of the familymedicine model.Ageing populationWith the rapidly ageing population, the burden ofdisease will continue to grow. In the RS the main public<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite14The Primary Health Care Strategy
va bolja reakcija na očekivanja stanovništva predstavljajuglavne izazove u narednim godinama.Ciljevi Strategije <strong>primarne</strong><strong>zdravstvene</strong> zaštiteOsnovni, strateški cilj je razvoj PZZ u kojoj će centralnomjesto imati model porodične medicine i koja ćese bazirati na pružanju dostupnih, efikasnih, kvalitetnih iisplativih usluga, intervencija i programa.Strateški cilj će biti ostvaren kroz realizaciju specifičnihciljeva i to:■■■■■■■■■■■■Izmjene i dopune postojeće regulative u cilju jačanjaPZZ;Jačanje planiranja i organizacije u PZZ;Uspostavljanje neophodnih upravljačkih mehanizama;Širenje modela porodične medicine na cjelokupnojteritoriji Republike Srpske;Uspostavljanje efikasnog sistema pružanja usluga;Transformacija postojećih službi doma zdravlja iusklađivanje sa modelom porodične medicine;Razvoj, testiranje i uvođenje novog ugovora imehanizama plaćanja davalaca usluga;Stvaranje adekvatnog profila zdravstvenih radnika;Uvođenje i primjena standarda kvaliteta s ciljemunapređenja, osiguranja i kontrole kvaliteta;Razvoj i implementacija informacionog sistema;Razvoj i implementacija sistema praćenja i vrednovanja.Jačanje učešća lokalne zajednice u obezbjeđivanju<strong>primarne</strong> <strong>zdravstvene</strong> zaštite<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite15health challenge is control of outbreaks of mass noncommunicablediseases.Adjusting the health system to these significant demographic,epidemiological and sociologic changes, makingit able to cope with the foreseen additional burdenand emerging needs and making it more responsive tothe population expectations constitutes major challengesin the years to come.Goals of the primary healthcare reformThe core strategic goal is development of primaryhealth care focused on family medicine, which will bebased upon delivery of accessible, efficient, quality andcost-effective services, interventions and programmes.The strategic goal will be attained through the realisationof specific objectives, such as:■■■■■■■changes and amendments to the existing regulationswith a view to strengthening primary healthcare;strengthening of PHC planning and organisation;establishment of required management mechanisms;Expansion of the family medicine model to coverthe whole territory of the Republic of Srpska;Establishment of an efficient system of servicedelivery;Transformation of the existing service of healthcentres and adjustment to the family medicinemodel;Development, piloting and introduction of newcontracting and provider payment mechanisms;The Primary Health Care Strategy
Sadržaj reforme <strong>primarne</strong><strong>zdravstvene</strong> zaštiteCilj 1. Izmjene i dopune postojeće regulativeu cilju jačanja PZZU narednom periodu, potrebno je izvrštiti revizijupostojeće zakonske i podzakonske regulative i utvrditikoje je izmjene i dopune neophodno napraviti kako bi sepozicija PZZ u zdravstvenom sistemu Republike Srpskekonačno učvrstila.Za određene segmente PZZ koji nisu dovoljno ilinisu nikako pokriveni postojećim zakonima i/ili pod-zakonskimaktima, potrebno je pristupiti izradi novih zakonskihi/ili podzakonskih rješenja.■■■■■■■Da bi se ovaj cilj ostvario potrebno je:Revidirati postojeću zakonsku i pod-zakonskuregulativu;Izraditi, eventualne, izmjene i dopune postojećeregulative;Usvojiti izmjene i dopune postojeće regulative;Implementirati izmjene i dopune;Izraditi nova zakonska i/ili pod-zakonska rješenja;Usvojiti nova zakonska i/ili pod-zakonskarješenja;Implementirati nova zakonska i/ili pod-zakonskarješenja.Ovaj posao treba da urade ekspertski timovi kojeće, po potrebi, formirati Ministarstvo zdravlja i socijalnezaštite.■■■■■Building adequate profiles of health workers;Introduction and application of quality standardswith a view to quality enhancement, assurance andcontrol;Development and implementation of an informationsystem;Development and implementation of monitoringand evaluation systems;Better involvement of the local community in theprovision of primary health care.Contents of the primary healthcare reformGoal 1. Changes and amendments ofthe existing legislation with a view tostrengthening primary health careIn the forthcoming period, it will be necessary toreview the existing laws and by-laws and identify changesand amendments to be made in order to finally strengthenthe position of primary health care in the health systemof the Republic of Srpska.With regard to certain PHC segments that are notadequately or at all provided for by the established lawsand/or by-laws, it will be necessary to initiate formulationof new laws and/or by-laws.■■In order to attain this goal, it will be necessary to:review the established laws and by-laws;develop possible changes and amendments of thecurrent regulations;<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite16The Primary Health Care Strategy
Cilj 2. Jačanje planiranja i organizacije u PZZPlaniranjeU cilju jačanja funkcija planiranja, kao jedne od četiriglavne sekundarne funkcije menadžmenta u zdravstvenimustanovama, potrebno je u sve domove zdravljauvesti strateško i poslovno planiranje i osposobiti postojećei buduće menadžere domova zdravlja, u vezi usvajanjamodernih tehnika planiranja.Da bi se ovaj cilj ostvario potrebno je:■ Revidirati i dopuniti postojeći program za kratkekurseve iz oblasti zdravstvenog menadžmenta;■ Odrediti ciljne grupe u PZZ koje moraju biti edukovanei obučene iz oblasti strateškog i poslovnogplaniranja;■ Planirati i organizovati program edukacije i obukeiz oblasti strateškog i poslovnog planiranja;■ Angažovati međunarodne i lokalne eksperte, kaopredavače, iz oblasti strateškog i poslovnog planiranja;■ Uvesti program edukacije i obuke iz oblastistrateškog i poslovnog planiranja za ciljne grupe;■ Vrednovati program edukacije i obuke iz oblastistrateškog i poslovnog planiranja i njegov učinakna uvođenje i održavanje strateškog i poslovnogplaniranja u ustanove PZZ.Institut za zdravstveni menadžment Medicinskogfakulteta Univerziteta u Banjoj Luci biće glavni nosilacaktivnosti u vezi sa sprovođenjem programa i obuke izzdravstvenog menadžmenta.■■■■■adopt changes and amendments to the existingregulations;implement the changes and amendments;Develop new laws and/or by-laws;Adopt the new laws and/or by-laws;implement the new laws and/or by-laws;This responsibility needs to be vested with expertteams, which will as necessary be appointed by the Ministryof Health and Social Welfare.Goal 2. Strengthening of PHC planning andorganisationPlanningWith a view to strengthening the planning functionas one of the four core secondary functions of healthmanagement, it is necessary to introduce strategic andoperative planning into all health centres, as well as totrain both existing and future health centre managers toenable them to acquire modern planning techniques.In order to attain this goal, it will be necessary to:■ review and amend the current curriculum forshort-term courses in the filed of health management;■ identify target groups in primary health care thatneed to be educated and trained in the field ofstrategic and operative planning;■ plan and organise a programme of education andtraining in the field of strategic and operativeplanning;■ involve international and local experts as trainersin the field of strategic and business planning;<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite17The Primary Health Care Strategy
Organizacioni obliciOsnovni organizacioni oblik u PZZ Republici Srpskojje tim porodične medicine. Pored tima porodičnemedicine ova strategija definiše još dva organizacionaoblika PZZ: grupnu praksu porodične medicine i domzdravlja.Tim porodične medicine sastoji se od doktorai dvije medicinske sestre/tehničara porodične medicine.Tim može registrovati između 1.500 i 2.500 građana.Grupna praksa porodične medicine sastoji se od4 do 10 timova porodične medicine, koji zajedno mogupokriti najviše do 25.000 građana.Dom zdravlja sastoji se od timova porodične medicine,grupnih praksi porodične medicine i ostalih organizacionihjedinica koje mogu činiti dom zdravlja, apokriva preko 25.000 građana.Tim porodične medicine i grupna praksa porodičnemedicine mogu biti u javnom i privatnom vlasništvu, dokdom zdravlja može biti isključivo u javnom vlasništvuUsluge, ugovaranje i mehanizmi plaćanjaOrganizacioni oblici PZZ pružaće usluge iz paketakoji su prikazani u tabeli 1.Ugovaranje i mehanizmi plaćanjaSa timovima porodične medicine, grupnim praksamaporodične medicine i domovima zdravlja biće zaključivaniugovori, koji će definisati obim i strukturu uslugaiz tri različita, gorenavedena, paketa.Ugovori neće biti automatski, već će se zaključivatiu skladu sa definisanim kriterijumima.Pored toga, timovi porodične medicine, grupnapraksa porodične medicine i domovi zdravlja koji budu■ implement and organise a programme of educationand training in the field of strategic andoperative planning;■ evaluate the programme of education and trainingin the field of strategic and business planning andits effects on the introduction and sustainability ofstrategic and operative planning in PHC institutions;The Health Management Institute of Banja LukaUniversity’s School of Medicine will be the main agentof the activities related to the implementation of theprogramme and training in health management.Organisational formsThe core organisational form of primary health carein the Republic of Srpska is the family medicine team.In addition to the family medicine team, the Strategy definesanother two organisational PHC forms: collectivefamily medicine practice and health centres.The family medicine team consists of a doctor- family medicine specialist and two nurses/medicaltechnicians. 1,500 to 2,500 individuals can be registeredwith a team.Collective family medicine practice consists of4 to 10 family medicine teams, which can collectively covera maximum of 25,000 people.A Health Centre gathers family medicine teams,shared practices and other organisational units whichmay constitute a health centre, and covers over 25,000people.Family medicine teams and shared practices may beeither publicly or privately owned, while health centresmay be exclusively privately owned.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite18The Primary Health Care Strategy
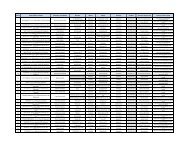
Tabela 1. Paketi usluga koje će pružati organizacioni oblici PZZTable 1. Service packages to be provided by PHCorganisational formsPaket / PackageOsnovni paket PZZPHC basic servicesProšireni paket PZZExpanded PHC packageIntegralni paket PZZIntegral PHC packageUsluge / ServicesEsencijalne usluge (uključujući obaveznu imunizaciju)Essential services (including mandatory immunisation)Esencijalne usluge + dodatne usluge / Essential services + supplementary services- Manji hiruški zahvati / Minor surgical interventions- Promocija zdravlja / Health promotion- Prevencija bolesti / Disease prevention- Upravljanje hroničnim bolestima / Chronic diseases management- Planiranje porodice / Family planning- Kućne posjete / Home visitsEsencijalne usluge + dodatne usluge + / Essential services + supplementary services +- Rehabilitacija u zajednici / Community-based rehabilitation- Mentalno zdravlje / Mental Health- Bolnica kod kuće / Hospital at Home- Palijativna njega Palliative care- Dječija i preventivna stomatologija / Child and preventive stomatology- Dijagnostičke usluge / Diagnostic services- Higijensko-epidemiološki poslovi / Hygienic – epidemiological services* lista i opis usluga biće dodatno definisani podzakonskim aktom / the list and description of services will be additionally defined in by-lawsakreditovani imaće prioritet prilikom sklapanja ugovorasa Fondom zdravstvenog osiguranja i moći će ostvarivatiodređena bonus plaćanja.Paket osnovnih usluga sastoji se od esencijalnih uslugaPZZ. Sadržaj paketa odrediće Ministarstvo zdravljai socijalne zaštite. Usluge u paketu su za sve starosne grupei oba pola.Usluge iz ovog paketa plaćaju se per capita. Potrebnoje prilagoditi postojeću formulu plaćanja timova po rodičnemedicine, u koju bi bio uključen segment plaćanjausluga iz domena obavezne imunizacije.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite19Services, contracting and payment mechanismsPHC organisational forms will provide servicesfrom the packages as given in Table 1 below.Contracting and provider payment mechanismsFamily medicine teams, shared practices and healthcentres will sign contracts whereby the volume andstructure of services for three different, aforementioned,packages will be defined.Contracting will not be a matter-of-course but willbe made in line with the established criteria.The Primary Health Care Strategy
Prošireni paket PZZ nadovezuje se na Paket osnovnihusluga, kojim se proširuje obim i struktura usluga.Usluge iz ovog paketa mogu se plaćati kombinovano:■■Per capita za osnovne usluge, iPo obavljenoj usluzi za dodatne usluge.Integralni paket PZZ se, u suštini, nadovezuje naProšireni paket PZZ, koji ima za cilj stvaranje uslova zarazvoj koncepta sveobuhvatne PZZ. Primjenom ovogPaketa podstaklo bi se prenošenje zdravstvenih usluga,koje se tradicionalno pružaju na sekundarnom nivou, naPZZ.Usluge iz ovog paketa mogu se plaćati kombinovano:■■■Per capita za osnovne usluge,Po obavljenoj usluzi za dodatne usluge, iProspektivnim budžetom za stavke navedene utabeli 1. pod proširenom PZZ.U ugovore za timove porodične medicine koji radeu ruralnim ambulantama treba ugraditi bonus plaćanja,kao mehanizme stimulacije za rad i ostanak timova porodičnemedicine u takvim područjima.In addition, FM teams, FM shared practices andhealth centres that are accredited will be treated as prioritiesfor contracting with HIF and will be eligible forbonus payments.Basic Services Package consists of PHC essentialservices. The contents of the package will be identifiedby the Ministry of Health and Social Welfare. The BasicServices Package covers all age and sex groups.Services of this package are paid through capitation.It will be necessary to adjust the current paymentformulas for family medicine teams, which should incorporatepayment of services related to mandatory immunisation.Expanded PHC package supplements the BasicServices Package with expanded volume and structureof services.Services of this package are paid through a mix of:■ capitation for basic services, and■ fee-for-service payment for supplementary services.The PHC Integral Package in principle adds to theExpanded Package aimed at creating conditions for theTabela 2. Ugovaranje paketa usluga PZZ / Table 2. Contracting of PHC Service PackagesOrganizacioni obliciOrganisational formsTim porodične medicineFamily medicine teamGrupna praksa porodične medicineCollective family medicine practiceOsnovni paket PZZBasic PHC PackageXXProšireni paket PZZExpanded PHC PackageXIntegralni paket PZZIntegral PHC PackageDom zdravlja / Health centre X X X* sadržaj paketa biće dodatno definisani podzakonskim aktom / the contents of the packages will be defined in by-lawsX<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite20The Primary Health Care Strategy
Cilj 3. Uspostavljanje neophodnihupravljačkih mehanizamaU cilju transformacije doma zdravlja i uvođenja modelaporodične medicine neophodno je proizvesti edukovane<strong>zdravstvene</strong> menadžere koji bi bili osposobljeni zaprofesionalno upravljanje reformskim procesima.Da bi se ovaj cilj ostvario potrebno je:■ Stvoriti okruženje koje će pružati podsticaj ikontrolne mehanizme za uvođenje i korišćenjemodernih menadžerskih tehnika u organizacionimstrukturama PZZ;■ Izvršiti profesionalizaciju zanimanja zdravstvenogmenadžera;■ Stvoriti uslove za nesmetano obavljanje edukacijei obuke menadžera iz oblasti zdravstvenogmenadžmenta;■ Planirati, organizovati, permanentno sprovoditi ivrednovati edukaciju i obuku menadžera iz oblastizdravstvenog menadžmenta;■ Planirati, organizovati, permanentno provoditi ivrednovati obuku iz upravljanja promjenama;■ Razviti strukture i puteve napredovanja zanimanjazdravstvenog menadžera;■ Razviti mehanizme stimulacije za vrednovanjekvalitetnog rada zdravstvenih menadžera.Ključnu ulogu u ostvarenju definisanih ciljeva razvojai profesionalizacije zdravstvenog menadžmenta uRepublici Srpskoj treba da odigra Institut za zdravstvenimenadžment.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite21development of a comprehensive PHC concept. Applicationof this Package will stimulate the transfer of healthservices traditionally delivered at the secondary level toprimary health care.Services of this package may be paid through amix of:■■■capitation for basic services,fee-for-service payment for supplementary services,andprospective budget for each of the items as listedin Table 1 under Expanded PHC.Contracts with family medicine teams working in ruralclinics need to incorporate bonus payments as incentivemechanisms for their work and stay in such areas.Goal 3. Establishment of requiredmanagement mechanismsWith a view to transforming health centres and introducingthe family medicine model, it will be necessary toproduce trained health managers who will be capacitatedto manage reform processes in a professional manner.■■■■In order to attain this goal, it will be necessary to:create such environment that will ensure incentivesand control mechanisms for the introductionand application of modern management techniquesto PHC organisational structures;to acknowledge health management as a profession;to create conditions for unhindered educationand training of managers in the field of healthmanagement;plan, organise and continuingly implement andevaluate education and training of managers in thefield of health management;The Primary Health Care Strategy
Cilj 4. Širenje modela porodične medicine nacjelokupnoj teritoriji Republike SrpskePolazeći od dobrih rezultata postignutih uvođenjemmodela porodične medicine kroz pilot projekat Ministarstvazdravlja i socijalne zaštite u nekoliko domova zdravlja,u narednih pet godina model porodične medicine će,primjenom sveobuhvatne i integrisane strategije implementaljcije,biti proširen na cjelokupnu teritoriju RepublikeSrpske.Sveobuhvatna i integrisana strategija implementacijeporodične medicine podrazumijeva:■■■■■■■■■■■■Izradu plana sprovođenja za dom zdravlja,Utvrđivanje početnog stanja u domu zdravlja,Prilagođavanje regulative doma zdravlja,Medijsku promociju modela porodične medicine,Slobodan izbor doktora porodične medicine iregistraciju građana,Edukaciju timova porodične medicine (programspecijalizacije i program dodatne obuke),Građevinsku rekonstrukciju ambulanti porodičnemedicine,Opremanje ambulanti porodične medicine standardnimsetom medicinske opreme,Obuku iz menadžmenta promjena za timoveporodične medicine i menadžment doma zdravlja,Uvođenje informacionog sistema (hardver i aplikativnisoftver),Obuku korisnika (doktora i sestara porodičnemedicine) u vezi sa korišćenjem aplikativnog softveraza ambulante porodične medicine,Uvođenje novih oblika ugovaranja i mehanizamaplaćanja,■ plan, organise and continuingly implement andevaluate training in problem management;■ develope structures and paths of promotion ofhealth managers as a profession;■ develop incentive mechanisms for evaluating thequality of health managers’ performance;The key role in the attainment of the defined goalsof development and professionalisation of RS healthmanagement should be played by the Health ManagementInstitute.Goal 4. Expansion of the family medicinemodel to cover the whole territory of theRepublic of SrpskaFollowing good results achieved in the introductionof the family medicine model, which was implementedin several health centres as a pilot-project of theMinistry of Health and Social Welfare, the family medicinemodel will be expanded to cover the whole territoryof the Republic of Srpska through the application of acomprehensive and integrated implementation strategy,A comprehensive and integrated family medicineimplementation strategy implies the following:■■■■■Development of an implementation plan forhealth centres,Determination of the situation as found in healthcentres.Media promotion of the family medicine model,Free choice of a family medicine doctor and registrationof citizens,Training of family medicine teams (specialisationprogramme and PAT),<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite22The Primary Health Care Strategy
■■■Uvođenje vodiča za kliničku praksu u PZZ,Akreditaciju timova porodične medicine iuvođenje sistema kontrole kvaliteta,Uvođenje sistema praćenja, nadzora i vrednovanjarada timova porodične medicine.Primjenom integrisane i sveobuhvatne strategije implementacijemijenja se kompletna postojeća organizacija,planiranje i upravljanje domom zdravlja.Cilj 5. Uspostavljanje efikasnog sistemapružanja uslugaPZZ koja se bazira na modelu porodične medicinetreba da izgradi efikasan sistem koji bi predstavljao prvutačku kontakta građana sa zdravstvenim sistemom i kojibi težio ostvarenju najvažnijih principa PZZ: dostupnost,sveobuhvatnost, kontinuitet i usklađenost.Prva tačka kontakta građana sa zdravstvenim sistemom:Prvi kontakt građana sa zdravstvenim sistemomostvaruje se isključivo preko timova porodične medicine.Timovi porodične medicine predstavlja “filter za ulazaku zdravstveni sistem”.Ključne aktivnosti za ostvarenje ovog principa su:■ Slobodan izbor doktora porodične medicine, i■ Registracija porodica i građana kod izabranog timaporodične medicine.Dostupnost <strong>zdravstvene</strong> zaštite: PZZ mora biti jednakodostupna svim građanima Republike Srpske.■■Ključne aktivnosti za ostvarenje ovog principa su:Edukacija potrebnog broja timova porodičnemedicine,Pravilna raspodjela timova porodične medicine nacjelokupnoj teritoriji Republike Srpske, u skladu sa<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite23■■■■■■■■■Physical reconstruction of family medicine clinics,Equipping of family medicine clinics with a set ofmedical equipment,Training in change management for family medicineteams and health centre management,Introduction of an information system (hardwareand software applications),User training (family medicine doctors and nurses)in the usage of software applications for familymedicine clinics,Introduction of new forms of contracting andpayment mechanisms,Introduction of clinical practice guidelines intoPHC,Accreditation of family medicine teams and introductionof the quality control system,Introduction of systems of monitoring, supervisionand evaluation of the performance of familymedicine teams.Application of the integrated and comprehensiveimplementation strategy will change the overall existingorganisation, planning and managing of health centres.Goal 5. Establishment of an efficient systemof service deliveryFamily-based primary health care needs to buildan efficient system that would serve as the first level ofcontact of individuals with the health system that wouldaspire to fulfil the central principles of primary healthcare: accessibility, comprehensiveness, continuity and coordination.The first level of contact of individuals with thehealth system: The first level of contact of individualsThe Primary Health Care Strategy
ojem stanovnika i njenim geografskim karakteristikama.Domovi zdravlja obavezni su da pripreme i izrade,a jedinice lokalne samouprave da usvoje lokalnu mrežuambulanti porodične medicine.Sveobuhvatnost <strong>zdravstvene</strong> zaštite: Tim porodičnemedicine mora biti osposobljen da rješava različite <strong>zdravstvene</strong>probleme i da pruža širok spektar usluga, bez obzirana starost, pol ili vrstu zdravstvenog problema građana.Pored tradicionalnih, kurativnih i rehabilitacionihusluga, tim porodične medicine pruža i usluge promocijezdravlja i prevencije bolesti, koje su u ranijem sistemu bilepotpuno zanemarene.■■Ključne aktivnosti za ostvarenje ovog principa su:Visokokvalitetna edukacija iz porodične medicine(dodiplomska i postdiplomska), iOpremanje standardnim setom medicinske opremeambulanti porodične medicine.Kontinuitet <strong>zdravstvene</strong> zaštite: PZZ koja se zasnivana modelu porodične medicine treba da osigura kontinuiranopraćenje zdravlja opredijeljene populacije.■■■Ključne aktivnosti za ostvarenje ovog principa su:Uvođenje i održavanje aktivnog pristupa uprovođenju mjera i aktivnosti u PZZ,Zakazivanje pregleda, iObezbjeđivanje odgovarajuće njege na višim nivoima<strong>zdravstvene</strong> zaštite.Koordiniranost <strong>zdravstvene</strong> zaštite: U dobro organizovanomsistemu <strong>zdravstvene</strong> zaštite, u kojem centralnuulogu ima PZZ, nema tzv. lutanja pacijenta.■Ključne aktivnosti za ostvarenje ovog principa su:Vodiči za upućivanje i kretanje korisnika zdravstvenihusluga prema konsultantu-specijalisti udomu zdravlja ili u bolnicu;<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite24with the health system is made exclusively through thefamily medicine team. The family medicine team constitutes“an entry filter of the health system”.The key activities aimed at the attainment of thisprinciple are as follows:■■a free choice of a family medicine doctor, andregistration of families and individuals with theselected family medicine team.Accessibility of primary health care: PHC must beequally accessible to all citizens of the Republic of Srpska.The key activities aimed at the attainment of thisprinciple are as follows:■■Training of the necessary number of family medicineteams, andEqual distribution of family medicine teamsthroughout the Republic of Srpska in accordancewith the number of residents and geographiccharacteristics.Health centres are obligated to prepare and develop,while local self-governance units are obligated toadopt, their local networks of family medicine clinics.Comprehensiveness of health care: The familymedicine team must be capacitated to deal with varioushealth problems and provide a wide range of servicesirrespective of age, sex or kind of health problems. Inaddition to traditional, curative and rehabilitative services,the family medicine team will provide promotiveand preventive services as well, which were completelyneglected in the previous system.The key activities aimed at the attainment of thisprinciple are as follows:■High-quality training in family medicine (undergraduateand postgraduate studies), andThe Primary Health Care Strategy
■ Precizan i jasno definisan zahtjev prema konsultantu-specijalistiza obavljanje određenih konsultacija/usluga;■ Odgovarajuća medicinska dokumentacija kojaprati korisnika zdravstvenih usluga koji je upućenkonsultantu-specijalisti u dom zdravlja ili u bolnicu;■ Zakazivanje pregleda kod konsultanta-specijalisteu dom zdravlja ili u bolnicu;■ Praćenje stanja zdravlja/bolesti, u konsultacijisa doktorom-specijalistom u domu zdravlja ilibolničkim doktorom koji liječi upućenog korisnikazdravstvenih usluga;■ Povrat informacija i dokumentacije, formalnouspostavljenim putem, o korisniku zdravstvenihusluga, od konsultanta-specijaliste iz doma zdravljaili bolničkog doktora prema doktoru porodičnemedicine.Krajnji cilj razvoja PZZ u Republici Srpskoj je uspostavljanjetemelja na kojima će se, u budućnosti, graditisistem integrisane <strong>zdravstvene</strong> zaštite.Cilj 6. Transformacija postojećih službi domazdravlja i usklađivanje sa modelom porodičnemedicineKonsultativno-specijalistička službaOrganizacijaPostojeća organizacija konsultativno-specijalističkeslužbe u domovima zdravlja mora se prilagoditi modeluporodičine medicine.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite25■ Equipping of family medicine clinics with a standardset of medical equipment,Continuity of health care: Family-medicine basedPHC should ensure continuous monitoring of the coveredpopulation’s health.The key activities aimed at the attainment of thisprinciple are as follows:■■■Introduction and pursuing of an active approachto the implementation of PHC measures andactivities,Consultation appointment, andEnsuring adequate care at higher levels of healthcare.Coordination of health care: A well-organised healthsystem, where the central role is given to PHC, doesnot allow the so-called “meandering” of patients.The key activities aimed at the attainment of thisprinciple are as follows:■■■■■Guidelines for referral and pathways of healthcare users to consultant-specialist in the healthcentre or hospital,Precise and clearly defined requirements of consultants-specialists,for delivery of certain consultations/services;Adequate medical documentation following thehealth care user who is referred to a consultant/specialist or hospital;Setting an appointment system for consultationswith a consultant-specialist in the health care orfor admission to hospital;Monitoring of health/disease condition in consultationwith doctors-specialists in the health centreor hospital doctors responsible for the treatmentof the referred health care users;The Primary Health Care Strategy
Konsultativno-specijalistička služba se transformišeu konsultativno-specijalističke ambulante, koje, zavisnood potreba timova porodične medicine, obezbjeđuju specijalističkekonsultacije ili usluge za svoje opredijeljenegrađane.Upućivanje korisnika zdravstvenih usluga kod konsultanata- specijaliste, unutar domova zdravlja, samostalnihspecijalističkih ambulanti, bolnica, klinika, vršiće ljekar porodičnemedicine. “Kretanje” korisnika zdravstvenih uslugakroz ovako uređen sistem biće regulisano vodičima- algoritmima, protokolima (tzv. dijagnostičko - terapijskiprotokoli), te posebnim aktima koji će zahtijevati stalnureviziju i aktuelizaciju u skladu sa potrebama savremeneprakse. Na osnovu nalaza specijaliste - konsultanta, ljekarporodične medicine donosi konačnu odluku, čime se ujednoobezbjeđuje kontinuitet <strong>zdravstvene</strong> zaštiteOdređeni broj specijalista iz PZZ, zavisno od planiranihpotreba Republike Srpske, može završiti dodatnuedukaciju iz porodične medicine i obavljati poslove doktoraporodične medicine.Ugovaranje i mehanizmi plaćanjaKonsultativno-specijalističke usluge mogu ugovaratidomovi zdravlja, grupne prakse timova porodične medicinei timovi porodične medicine.Konsultativno-specijalističke usluge mogu se plaćatikombinovano: po obavljenoj usluzi i prospektivnimbudžetom.Zaštita zdravlja žena i djeceOrganizacijaPostojeća organizacija <strong>zdravstvene</strong> zaštite djece,trudnica i žena u domovima zdravlja mora se prilagoditi<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite26■ Information feedback and return of documentationconcerning the patient through formal channels,from the consultant-specialist of the healthcentre or. hospital doctor, to the family medicinedoctor.The ultimate goal of PHC development in the Republicof Srpska is to lay the foundation upon which afuture integrated health system will be constructed.Goal 6. Transformation of the existingservices of health centres and theiradjustment to the family medicine modelConsultative-specialist serviceOrganisationThe current organisation of consultative-specialistservices of health centres must be adjusted to the familymedicine model.Consultative-specialist services are to be transformedinto consultative-specialist clinics which will, dependingon the needs of family medicine teams, provide specialistconsultations or services for the population theycover.Referrals of health are users to consultants-specialistsof the health centre, independent specialist clinics,hospitals, departments will be made by the familymedicine doctor. The “movement” of health care usersthrough the system thus arranged will be regulated byguidelines – algorithms, protocols (so-called diagnostictherapeuticprotocols), and by special documents thatwill need constant revising and updating in line with theneeds of modern practices. Following the findings of aThe Primary Health Care Strategy
modelu porodične medicine. Dosadašnja organizacijaobezbjeđivala je zdravstvenu zaštitu navedenih grupakroz rad odgovarajućih specijalističkih službi i dispanzera,lociranih u principu u urbanim područjima, čime je,na samom početku, narušen princip jednakosti u zdravlju,u korist stanovništva grada u odnosu na selo.Konsultantsko - specijalističke usluge u oblasti <strong>zdravstvene</strong>zaštite djece i žena mogu se obavljati u domuzdravlja. U cilju zaštite zdravlja ovih vulnerabilnih grupa,kao i zaštite funkcije tima porodične medicine koji trebada usklađuje zdravstvenu zaštitu i ujedno obezjeđujenjen kontinuitet, kretanje korisnika zdravstvenih uslugana primarnom nivou <strong>zdravstvene</strong> zaštite između timovaporodične medicine i specijalista pedijatara - ginekologabiće definisano vodičima – algorimima.Specijalisti - konsultanti pedijatri i ginekolozi imaćeobavezu da najmanje jednom mjesečno posjete ambulanteporodične medicine i obave konsultaciju sa timovimaporodične medicine, te da im pruže potrebnu stručnupomoć.Medicina radaOrganizacijaPostojeća služba medicine rada u domovima zdravljatakođe se mora prilagoditi modelu porodične medicine.Medicina rada, zavisno od lokalnih potreba, može setransformisati u dva pravca.Prva opcija je da se postojeća služba medicine radatransformiše u konsultativno-specijalističku ambulantu.Ova ambulanta bi pružala konsultativno-specijalističkeusluge timovima porodične medicine i mogla bi obavljatidruge poslove iz svog domena, ako za to postoji potreba<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite27specialist-consultant, the family medicine doctor makesthe final decision, thereby ensuring the continuity ofhealth care.The family medicine team decides, on behalf ofthe registered individuals, when and which consultantspecialistthey will be referred to.A number of specialists working in PHC, dependingon the projected needs of the Republic of Srpska,may be additionally trained in family medicine (PAT) andperform tasks of the family medicine doctor.Contracting and provider payment mechanismsConsultative-specialist services may be contractedby health centres, shared family medicine practices andfamily medicine teams.Consultative-specialist services will be contractedby family medicine teams and family medicine sharedpractices.In both cases, these consultative-specialist servicesmay be paid through a mix of fee-for-service paymentand prospective budgeting.Health care of women and childrenOrganisationThe organisation of health care of children, pregnantwomen and women currently existing in health centresmust be adapted to the family medicine model. Theprevious organisation favoured the health care of theabove groups through the services of relevant specialistservices and clinics, located mainly in urban areas, whichbreached the principle of equality in health, favouring urbanpopulation to the detriment of rural population.The Primary Health Care Strategy
(periodični pregled radnika zaposlenih na radnim mjestimasa posebnim uslovima rada, ekspertize profesionalnihoboljenja, utvrđivanje trajne radne sposobnosti, i sl.).Druga mogućnost je da kompletan posao medicinerada, od domova zdravlja preuzme Zavod za medicinurada, kojeg je osnovala Vlada Republike Srpske i koji bise bavio aspektima zaštite na radu, te dijagnostikom i liječenjemprofesionalnih oboljenja.Prije konačnog uspostavljanja Zavoda za medicinurada, potrebno je uraditi studiju ekonomske opravdanostii finansijske održivosti, kako bi se utvrdila ekonomijaobima i kako bi se stručno verifikovala druga opcija.Ugovaranje i mehanizmi plaćanjaU prvoj opciji, u prelaznom periodu, konsultativnospecijalističkeusluge medicine rada mogu ugovarati domovizdravlja. Dugoročno, konsultativno-specijalističkeusluge medicine rada će ugovarati timovi porodične medicinei grupne prakse porodične medicine.U drugoj opciji, usluge iz domena medicine radaugovarao bi Zavod za medicinu rada.U obje opcije, konsultativno-specijalističke uslugemedicine rada se mogu plaćati kombinovano: po obavljenojusluzi i prospektivnim budžetom.Hitna medicinska pomoćOrganizacijaPostojeća služba hitne medicinske pomoći u domovimazdravlja mora se prilagoditi modelu porodičnemedicine. Hitna medicinska pomoć, zavisno od lokalnihpotreba, može se transformisati u dva pravca.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite28Consultative-specialist services in the field ofhealth care of children and women may be performedin the health centre. With a view to providing health careto these vulnerable groups, as well to protecting the interestsof family medicine teams, which should coordinatehealth care and simultaneously ensure its continuity,the movement of health care users at the primary healthcare level, from family medicine doctors to specialists inpaediatrics and gynaecology will be defined by guidelines– algorithms.Specialists-consultants – paediatricians and gynaecologists– will be obliged to visit family medicine clinicsat least once a month and consult with family medicineteams and provide necessary assistance.Occupational MedicineOrganisationThe current occupational medicine services ofhealth centres must also be adjusted to the family medicinemodel. Occupational medicine, depending on localneeds, may be transformed into two directions.The first option is transformation of the currentoccupational medicine services into a consultative-specialistclinic. This clinic would provide consultative-specialistservices to family medicine teams and may performother tasks in its domain should the need arise(periodical reviews performing jobs that require specialconditions of work, expertise related to professional diseaseand ability-to-work, etc.).The second option is that all tasks of occupationalmedicine services should be transferred from health centresto the Occupational Medicine Institute, which hasThe Primary Health Care Strategy
Hitna medicinska pomoć transformiše se tako datimovi porodične medicine, u radno vrijeme i poslije radnogvremena, zbrinjavaju hitna medicinska stanja. Ovobi se primijenilo u svim domovima zdravlja u RepubliciSrpskoj.Dom zdravlja obezbjeđuje hitni sanitetski prevoz.Potrebno je da timovi porodične medicine prođudodatnu obuku u vezi sa pružanjem hitne medicinske pomoći.Hitna medicinska pomoć organizuje se i u okviruopštih bolnica ili kliničkih centara.Potrebno je uraditi studiju ekonomske opravdanostii finansijske održivosti za eventualno uspostavljanjetrakta za urgentni prijem.Ukoliko bi transformacija hitne medicinske pomoćiišla u pravcu formiranja trakta za urgentni prijem, neophodnoje definisati precizne protokole u vezi sa preuzimanjemživotno ugroženih sa određene teritorije.Ugovaranje i mehanizmi plaćanjaHitnu medicinsku pomoć ugovaraju timovi porodičnemedicine i ona spada u Paket osnovnih usluga. Utom smislu je potrebno izvršiti prilagođavanje postojećeformule plaćanja timova porodične medicine per capita.Dom zdravlja ugovara hitni sanitetski prevoz, kojise plaća po pređenom kilometru.Opšte bolnice ili klinički centri bi preko eventualnouspostavljenih urgentnih traktova ugovarali hitnu medicinskupomoć i hitni sanitetski prevoz.U tom slučaju, usluge hitne medicinske pomoći moguse plaćati kombinovano: po obavljenoj usluzi i prospektivnimbudžetom, a hitni sanitetski prevoz plaća sepo pređenom kilometru.been established by the Government of the Republic ofSrpska and which is to deal with aspects of protectionat work, and diagnostics and treatment of job-relateddiseases.Before the Occupational Medicine Institute hasbeen fully founded, it will be necessary to conduct astudy of cost-effectiveness and financial sustainability inorder to determine the economies of scale and verify thesecond option by sound evidence.Contracting and provider payment mechanismsWith regard to the first option, in the interim period,consultative-specialist services of occupationalmedicine may be contracted by health centres. In thelong run, consultative-specialist services of occupationalmedicine will be contracted by family medicine teamsand family medicine shared practices.With regard to the second option, occupationalmedicine services will be contracted by the OccupationalMedicine Institute.In both options, consultative-specialist services ofoccupational medicine may be paid through a mix offee-for-service payment and prospective budgeting.Emergency CareOrganisationThe existing ER services in health centres must beadjusted to the family medicine model. ER, dependingon local needs, may be transformed into two directions.ER is transformed in such a way that family medicineteams, during and after working hours, take care of<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite29The Primary Health Care Strategy
Patronažna službaOrganizacijaPostojeća služba patronaže u domovima zdravljamora se u potpunosti prilagoditi modelu porodične medicine.Potrebno je da se sestre iz tima porodične medicinedodatno edukuju iz oblasti promocije zdravlja, prevencijebolesti i palijativne njege.Poslove iz domena patronažne službe preuzeće iugovarati tim porodične medicine, uz prilagođavanje postojećeformule plaćanja per capita.Centar za fizikalnu rehabilitaciju u zajednici iCentar za mentalno zdravljeOrganizacijaOrganizaciona struktura centra za fizikalnu rehabilitacijuu zajednici i centra za mentalno zdravlje neće semijenjati.U prelaznom periodu, centar za fizikalnu rehabilitacijuu zajednici i centar za mentalno zdravlje ostaju usastavu doma zdravlja. Dugoročno, ovi centri bi trebaloda se institutišu kao zasebna pravna lica.U oba slučaja, potrebno je raditi na razvoju vodičakojima bi se jasno i precizno utvrdio “modus operandi”između timova porodične medicine i centra za fizikalnurehabilitaciju u zajednici i centra za mentalno zdravlje.Da bi se uvažili principi ekonomske opravdanosti ifinansijske održivosti, ovi centri bi se osnivali u zavisnostiod lokalnih potreba i finansijskih mogućnosti.Ugovaranje i mehanizmi plaćanjaU prelaznom periodu usluge fizikalne rehabilitacijeu zajednici i mentalnog zdravlja ugovara dom zdravlja.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite30emergency conditions. This option will be applied to allhealth centres in the Republic of Srpska.Health centres will provide ambulance transportation.It will be necessary for family medicine teams toundergo training in the provision of emergency aid.ER may be established within general hospitals orclinical centres through their emergency admission services.It will be necessary to conduct a study of cost-effectivenessand financial sustainability in order to establishan urgent admission area.Should ER be transformed into emergency admissionservices, it will be necessary to define precise protocolsconcerning admission of persons with life-threateningconditions from designated territory.Contracting and provider payment mechanismsEmergency care is contracted by family medicineteams and it is covered by the Basic Services Package.In this sense, it will be necessary to refine, i. e. adjustthe currently applied formula for family medicine teamspayment on the basis of capitation.Health centres will contract ambulance transportation,which will be paid by kilometre.Emergency services and ambulance transportationwill be contracted by general hospitals or clinical centresthrough potentially organised urgent admission areas.In this case, emergency services may be paidthrough a mix of fee-for-service payment and prospectivebudgeting, whereas ambulance transportation willbe paid by kilometre.The Primary Health Care Strategy
Kasnije, centar za fizikalnu rehabilitaciju u zajednicii centar za mentalno zdravlje, kao zasebna pravna lica,će samostalno ugovarati usluge iz domena njihove djelatnosti.U oba slučaja, <strong>zdravstvene</strong> usluge iz domena radacentra za fizikalnu rehabilitaciju u zajednici i centra zamentalno zdravlje mogu se plaćati prospektivnim budžetom.Dijagnostičke uslugeOrganizacijaU domovima zdravlja se najčešće pružaju sledećevrste dijagnostičkih usluga: biohemijsko-hematološke,RTG i ultrazvuk.Potrebno je da svi domovi zdravlja u Republici Srpskojprocijene potrebe i ekonomsku opravdanost uvođenja,odnosno postojanja određenih medicinskih tehnologija.Na osnovu konačne procjene potreba, odnosno ekonomskeopravdanosti uvođenja ili postojanja medicinskihtehnologija, dijagnostičke usluge, koje ostaju u sastavudoma zdravlja, biće tehnička podrška svakodnevnom radutimova porodične medicine.Ruralne ambulante porodične medicine, koje suudaljene deset i više kilometara od doma zdravlja, moguimati opremu za najčešće laboratorijske usluge.Ugovaranje i mehanizmi plaćanjaDijagnostičke usluge ugovara dom zdravlja, a moguse plaćati kombinovano: per capita i prospektivnim budžetom.Patronage servicesOrganisationThe current patronage services of health centresmust be fully adjusted to the family medicine model. Itwill be necessary for family team nurses to undergo additionaltraining in health promotion, disease preventionand palliative care.Tasks of the patronage service will be shifted toand contracted by family medicine teams, where therecurrent payment formula based on per capita paymentwill need to be adjusted.Community-based physical rehabilitation centresand mental health centresOrganisationThe organisational structure of community-basedphysical rehabilitation centres and mental health centreswill not change.In the interim period, community-based physicalrehabilitation centres and mental health centres will remainwithin health centres. In the long run, these centresshould be incorporated as independent legal entities.In both cases, it will be necessary to develop guidelinesthat will clearly and precisely define the modus operandiof family medicine teams and community-basedphysical rehabilitation centres and mental health centres.In order to observe the principles of cost-effectivenessand financial sustainability, these centres will befounded in line with local needs and financial resources.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite31The Primary Health Care Strategy
U ruralnim ambulantama porodične medicine, dijagnostičkeusluge ugovara tim porodične medicine, aplaćaju se per capita. U ovom slučaju, potrebna su određenaprilagođavanja formule plaćanja timova porodičnemedicine.Higijensko-epidemiološki posloviOrganizacijaPotrebno je da svi domovi zdravlja u Republici Srpskojprocijene lokalne potrebe i ekonomsku opravdanostu vezi sa statusom i radom postojeće higijensko-epidemiološkeslužbe.Na osnovu konačne procjene potreba i dokazaneekonomske opravdanosti, “nova” higijensko-epidemiološkaslužba ostaje u sastavu doma zdravlja.Primarni zadaci “nove” higijensko-epidemiološkeslužbe su unapređenje i kontrola stanja higijenskih prilikana području lokalne zajednice i epidemiološko nadgledanje,preventivni rad u smislu eliminacije mogućihizvora zaraze, te kontrola i suzbijanje širenja zaraznih imasovnih nezaraznih bolesti.Ugovaranje i mehanizmi plaćanjaHigijensko-epidemiološke usluge ugovara dom zdravlja,a mogu se plaćati kombinovano: po obavljenoj usluzii prospektivnim budžetom.Osim toga, dom zdravlja može ugovarati higijensko-epidemiološkeposlove sa jedinicom lokalne samoupravei drugim pravnim i fizičkim licima na svom području.Contracting and provider payment mechanismsIn the interim period, community-based physicalrehabilitation services and mental health services will becontracted by health centres.Later on, community-based physical rehabilitationcentres and mental health centres, as independent legalentities, will autonomously contract services falling withintheir scope of responsibility.In both centres, health services falling within thescope of community-based physical rehabilitation centresand mental health centre may be paid through prospectivebudgeting.Diagnostic servicesOrganisationThe following are services most frequently providedby health centres: biochemical - haematological, RTGand ultrasound.In is necessary that all health centres in the Republicof Srpska assess their needs and economic cost-effectivenessof introduction, i. e. application of certainmedical technologies.Based on the final need assessment and cost-effectivenessof the introduction, i. e. application of medicaltechnologies, diagnostic services, which are to remainwithin health centres, will serve as a technical support toeveryday activities of family medicine teams.Rural family medicine clinics, 10 or more kilometresfrom a health centre, may have equipment for commonlaboratory services.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite32The Primary Health Care Strategy
■ Vrednovati rezultate primjene novog ugovora imehanizama plaćanja,■ Napraviti eventualne izmjene u testiranim ugovorimai mehanizmima plaćanja,■ Planirati i organizovati širenje novog ugovora imehanizama plaćanja na cijelokupnu teritorijuRepublike Srpske,■ Implementirati novi ugovor i mehanizme plaćanjana cijelokupnu teritoriju Republike Srpske.Novi ugovor i mehanizmi plaćanja testiraće se udva doma zdravlja i dvije opšte bolnice u okviru Projektatehničke pomoći socijalnom osiguranju (SITAP).Testiranje novih ugovora i mehanizama plaćanja davalacausluga u PZZ nadogradilo bi iskustva stečena uokviru Projekta osnovno zdravstvo.Cilj 8. Stvaranje adekvatnog profilazdravstvenih radnikaU cilju stvaranja odgovarajućeg profila zdravstvenihradnika u PZZ potrebno je izraditi sveobuhvatnu strategijuza ljudske resurse u zdravstvenom sistemu RepublikeSrpske, kako bi se model PZZ, fokusiran na porodičnumedicinu, proširio i učinio održivim, te osigurao optimalanbroj i odgovarajuću strukturu zdravstvenih radnika uzdravstvenom sistemu Republike Srpske.<strong>Strategija</strong> za ljudske resurse mora se izraditi na načinkojim se iskazuje snažna podrška modelu porodične medicineu okviru svih institucionalnih i organizacionih nivoazdravstvenog sistema.Ova strategija mora definisati:■ Nedostatak, odnosno višak doktora, za svaku odmedicinskih specijalnosti, odnosno sestara i ostalihzdravstvenih radnika;<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite35and conforming to the reform strategic documents ofthe Republic of Srpska.Although pharmacists and pharmaceutical servicesdo not constitute the family medicine team, it will benecessary to ensure their involvement and cooperationin order to provide safe and efficient optimal therapyto patients. Pharmacists, as experts in medicines, have acrucial role in the provision of information and adviceto the public and prescribers, which strengthens benefitsfrom administration of medicines and renders prescribingmore efficient.Through a dialogue with local pharmacists, familymedicine teams should establish mechanisms aimed atensuring regular availability and cost-effective procurementof medicines that are necessary for treatment ofcommon and priority health problems.In order to attain good evidence-based prescribingand procurement practices, it will be necessary to ensurecontinuing education of pharmacists and primary healthcare doctors.The pharmacy is a health institution where thepublic is provided with and informed about medicines,medical substances and other substances necessary fortreatment of preservation of health.Goal 7. Development, piloting andintroduction of new contracting andprovider payment mechanismsThis is one of the key goals for sustainable developmentof primary health care in the Republic of Srpska.New contracting and provider payment mechanismsshould ensure incentives for improving efficiency, effecThe Primary Health Care Strategy
■ Potreban broj doktora-specijalista porodičnemedicine;■ Potreban broj medicinskih sestara/tehničaraporodične medicine;■ Potreban broj i strukturu drugih medicinskihspecijalnosti;■ Potreban broj medicinskih sestara/tehničara iostalih zdravstvenih radnika;■ Optimalan broj studenata fakulteta zdravstvenogusmjerenja;■ Optimalan broj učenika u srednjim medicinskimškolama;■ Optimalan broj specijalizanata potrebnih za specijalizacijeiz svih grana medicine, stomatologije ifarmacije■ Način i finansijske stimulacije za prekvalifikacijuspecijalista koji rade u PZZ;■ Način na koji bi se zdravstveni radnici privlačili izadržavali da rade u ruralnim područjima.U cilju izrade Strategije za ljudske resurse u zdravstvenomsistemu Republike Srpske, neophodno je uspostavitisaradnju između Ministarstva zdravlja i socijalnezaštite i Ministarstva prosvjete i kulture u svrhu boljegplaniranju i procesa odlučivanja u vezi sa politikom upisau škole i fakultete zdravstvenog usmjerenja.Cilj 9. Uvođenje i primjena standarda kvalitetas ciljem unapređenja, osiguranja i kontrolekvalitetaLicenciranje i akreditacija zdravstvenih radnika uPZZ predstavlja kritičnu komponentu, koja za cilj imaunapređenje, održavanje i osiguranje kvaliteta rada.tiveness, efficacy and quality of service delivery at thePHC level, and reduce unnecessary referrals to consultants-specialistsand hospitals.■■■■■■■In order to attain this goal, it will be necessary to:define objective to be attained through new formof contracting and payment mechanisms,design new contracts and payment mechanisms,pilot new contracts and payment mechanisms,evaluate results of the application of new contractingand payment mechanisms,Adjust, as necessary, piloted contracts and paymentmechanisms,Plan and organise expansion of new contractingand payment mechanisms in the whole territoryof the Republic of Srpska,implement the new contract and payment mechanismsin the whole territory of the Republic ofSrpska,The new contract and payment mechanisms will bepiloted in two health centres and two general hospitalswithin the Social Insurance Technical Assistance Project.Piloting of new contracts and provider paymentmechanisms in primary health care would enrich the experiencesgained within the Basic Health Project.Goal 8. Building adequate profiles of healthworkersWith a view to creating adequate profiles of healthworkers in primary health care, it will be necessary todevelop a comprehensive strategy for human resourcesin the health system of the Republic of Srpska, in order<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite36The Primary Health Care Strategy
Sastavni dio procesa akreditacije i re-akreditacijeje i plan individualnog profesionalnog razvoja, kojim seutvrđuju potrebe za kontinuiranom medicinskom edukacijom,sa ciljem podsticanja zdravstvenih radnika u PZZda proširuju svoja znanja i kompetencije.Neophodno je da Komora doktora medicine izradiposeban pravilnik kojim bi se regulisalo licenciranjedoktora - specijalista koji su završili dodatnu edukaciju izporodične medicine.Da bi se osiguralo pružanje usluga visokog kvaliteta,neophodno je izraditi dodatne vodiče za kliničku praksuu PZZ, zasnovanih na dokazima, koji će doprinijetijačanju kontinuiteta <strong>zdravstvene</strong> zaštite.Da bi se osigurala uspješna primjena vodiča, potrebnoje:■ Revidirati program specijalizacije iz porodičnemedicine i dodatne edukacije, kako bi se u njihuključili vodiči za kliničku praksu;■ Ugraditi mehanizme plaćanja po učinku u ugovorza pružanje usluga u PZZ, čime bi se stimulisalaupotreba vodiča za kliničku praksu i vodiča zapromociju zdravlja i prevenciju bolesti;■ Uvesti kliničku reviziju primjene vodiča, kako bi sevrednovao uticaj vodiča na kliničku praksu;■ Razviti odgovarajuće pokazatelje i njihovu metriku,pomoću kojih će sistem praćenja i vrednovanjamoći evidentirati informacije u oblastima za kojesu vodiči izrađeni.Ključnu ulogu u daljem razvoju, uvođenju, primjenii kontroli standarda kvaliteta u PZZ imaće Agencija zaakreditaciju i unapređenje kvaliteta <strong>zdravstvene</strong> zaštite.for the family-based PHC model to be expanded andrendered sustainable, and to ensure an optimal numberand adequate profile of health professionals in the healthsystem of the Republic of Srpska.The Human Resources Strategy must be developedso as to strongly demonstrate support to the familymedicine model in the framework of all institutional andorganisational levels of the health system.■■■■■■■■■■This strategy must define:the lacking or excessive number of doctors ineach of the medical specialities, as well as ofnurses and other health workers;the required number of family medicine doctors;the required number of family medicine nurses/technicians;the required number and structure of other medicalspecialities;the required number of nurses/medical techniciansand other health workers;the optimal number of students of schools ofhealth vocation;the optimal number of students in secondaryschools of medicine;the optimal number of residents as needed ineach of the medical, dentistry and pharmaceuticalbranches;Manner and financial incentives for re-training ofspecialists working in primary health care;ways to attract health workers to work in ruralareas and stimulate them to stay there;With a view to developing the Strategy for humanresources in the health system of the Republic of Srpska,it will be necessary to establish cooperation between<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite37The Primary Health Care Strategy
Cilj 10. Razvoj i primjena informacionogsistemaU cilju razvoja i implementacije informacionih ikomunikacionih tehnologija u PZZ potrebno je izraditisveobuhvatnu strategiju za razvoj zdravstvenog informacionogsistema Republike Srpske.Osnov za razvoj informacionog sistema u PZZ jeaplikativni softver za timove porodične medicine, koji jerazvijen i testiran u domu zdravlja Laktaši u okviru projekta“Osnovno zdravstvo”.Aplikativni softver će omogućiti povećanje produktivnostitimova porodične medicine, stavljajući medicinske,administrativne i finansijske poslove, koje tim svakodnevnoobavlja, u jednu aplikaciju, čime je omogućenocentralizovano zakazivanje pregleda, vođenje evidencija oopredijeljenim građanima, praćenje planiranih aktivnosti,materijalno-finansijsko poslovanje, kao i izvještavanjeprema nadležnim institucijama.■■■■Da bi se ovaj cilj ostvario potrebno je:Opremiti timove porodične medicine potrebnimhardverom i komunikacionom opremom;Izraditi i provesti program obuke za korišćenjesoftvera;Obezbijediti timovima i grupnim praksamaporodične medicine profesionalnu i organizovanupodršku u vezi održavanja informacionog sistema;Razviti standarde za razmjenu, upravljanje iintegraciju zdravstvenih podataka, čime će seomogućiti elektronska razmjena podataka.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite38the Ministry of Health and Social Welfare and the Ministryof Education and Culture with the purpose of betterplanning in the process of decision-making related tothe enrolment policy of secondary schools and facultiesof health vocation.Goal 9. Introduction and application ofquality standards with a view to qualityenhancement, assurance and controlLicensing and accreditation of PHC health professionalsconstitutes a critical point, which is aimed atenhancement, sustainability and assurance of quality ofperformance.An integral part of the accreditation and re-accreditationprocess is also the plan of individual professionaldevelopment, whereby needs for continuing medicaleducation are determined, with a view to stimulatingPHC health professionals to expand their knowledgeand competence.It is necessary that the Chamber of Medical Doctorsshould develop a special rulebook regulating licensingof doctors - specialists who have undergone additionaltraining in family medicine;In order to ensure delivery of high quality services,it is necessary to develop additional evidence-basedguidelines for clinical practice in primary health care,which will contribute to strengthening of health carecontinuity.In order to ensure successful implementation ofthe guidelines, it is necessary■ to review the curricula of family medicine specialisationand PAT in order to incorporate clinicalpractice guidelines;The Primary Health Care Strategy
Cilj 11. Razvoj i implementacija sistemapraćenja i vrednovanjaU cilju razvoja i primjene sistema praćenja i vrednovanjau PZZ, potrebno je izraditi sveobuhvatnu Strategijuza monitoring i evaluaciju zdravstvenog sistema RepublikeSrpske.Razvoj i primjena sistema praćenja i vrednovanjazdravstvenog sistema Republike Srpske služiće za određivanjei praćenje aktivnosti/intervencija u zdravstvenomsistemu u smislu ostvarivanja željenih i planiranih ciljeva.Ova <strong>Strategija</strong> predviđa da će organizacioni obliciPZZ kontinuirano prikupljati podatke za sistem praćenjai vrednovanja, na osnovu definisanih indikatora.Sistem praćenja i vrednovanja funkcionisaće kao instrumentnadležnih institucija za praćenje progresa kratkoročnih,srednjeročnih i dugoročnih ciljeva definisanihokvirima zdravstvenih politika, strategija, programa i projekata.Ključnu ulogu u razvoju i implementaciji sistemapraćenja i vrednovanja zdravstvenog sistema RepublikeSrpske imaće Institut za zaštitu zdravlja Republike Srpske.Cilj 12. Jačanje učešća lokalne zajednice uobezbjeđivanju <strong>primarne</strong> <strong>zdravstvene</strong> zaštite<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite39Za planiranje <strong>zdravstvene</strong> zaštite, osim što je bitnoda znamo obilježja stanovništva, strukturu populacijeu lokalnoj zajednici, njeno zdravstveno stanje, starosnepopulacione grupe, bitno je poznavati uticaj lokalne zajednicena zdravlje stanovništva, rad i zapošljavanje, socijalnistatus, životnu sredinu, loše navike i rizična pona■ to incorporate performance-based paymentmechanisms into PHC service delivery contracts,which would stimulate the application of clinicalpractice guidelines and health promotion anddisease prevention;■ Introduce clinical revision of the guidelines’ applicationin order to evaluate the effects on clinicalpractice;■ to develop adequate indicators and related measuringin order for the monitoring and evaluationsystems to record information in the area coveredby the guidelines.The key function in further development, introduction,implementation and control of quality standards inprimary health care will be vested with the Agency foraccreditation and improvement of health care quality.Goal 10. Development and implementationof the information systemWith a view to development and implementationof IT technologies in primary health care, it is necessaryto develop a comprehensive strategy for developmentof the health information system of the Republicof Srpska.The foundation for development of the PHC informationsystem is the family medicine team softwareapplication, which has been produced and piloted in theHealth Centre Laktasi within the Basic Health Project.The software application will bring about increasedproductivity of family medicine teams, aggregating everydaymedical, administrative and financial tasks intoone application, which will enable centralised appointingThe Primary Health Care Strategy
šanja. Stoga je potrebno uskladiti sve sektore u lokalnojzajednici sa sektorom zdravstva, posebno primarnom zdravstvenomzaštitom (opštinske službe, socijalne službe,obrazovanje, vodosnabdijevanje, životna sredina, raznaudruženja)Iz svega gorenavedenog, uloga opština kao i ostalihnavedenih službi moraće se definisati u svjetlu novihorganizacijskih struktura davalaca usluga u primarnoj zdravstvenojzaštiti.■ Opštinama bi se trebalo omogućiti da finansiraju<strong>zdravstvene</strong> usluge na nivou PZZ. Opštine bitako mogle postati finansijeri, čime bi se ojačalaPZZ■ Opštine moraju razviti i unaprijediti određeni brojfunkcija koje podrazumijevaju:- Podsticanje kvaliteta usluga u primarnoj zdravstvenojzaštiti;- Osiguravanje finansiranja infrastrukture, kapitalnihtroškova i troškova iznajmljivanja prostorijaza smještaj službi PZZ- Sufinansiranje službi u zajednici (centri za fizikalnurehabilitaciju i centri za mentalno zdravlje) ihitne medicinske pomoći- Omogućiti razvijanje i održavanje osnovnih funkcijajavnog zdravstva■ Angažovanje građana i civilnog društva je odposebne važnosti za uspostavljanje uravnoteženogsistema njihovih prava, te za istovremeno podsticanjeboljeg razumijevanja obaveza i dužnosti.Ovakav vid uključivanja građana i civilnog društvaosiguraće se kroz opštinske <strong>zdravstvene</strong> savjetekoje čine predstavnici opštine, PZZ i građani,razne volonterske grupe i udruženja pacijenataof consultations, registration of patients, monitoring ofplanned activities, material - financial operations, as wellas reporting to competent institutions.In order to attain this goal, it will be necessary to:■ equip family medicine teams with necessary hardwareand communication equipment;■ develop and implement a training programme forsoftware application;■ provide professional and organised support tofamily medicine teams and shared practices in relationto maintenance of the information system;■ to develop standards for exchange, managementand integration of health data, which will enablean electronic exchange of data.Goal 11. Development and implementationof the information systemWith a view to development and implementationof the monitoring and evaluation system in primaryhealth care, it will be necessary to develop a comprehensivestrategy for monitoring and evaluation of the healthsystem of the Republic of Srpska.Development and implementation of monitoringand evaluation of the health system of the Republic ofSrpska will serve to identify and monitor activities/interventionsin the health system in terms of attainingdesired and projected goals.This Strategy foresees that PHC organisationalforms will, on a continuous basis, collect data for themonitoring and evaluation system following the establishedindicators.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite40The Primary Health Care Strategy
■Uključivanje lokalne zajednice u definisanjeprioriteta u razvoju PZZ na lokalnom području uskladu sa potrebama lokalne zajedniceDom zdravlja u reformisanoj primarnojzdravstvenoj zaštitiVizijaThe monitoring and evaluation system will act asa tool for competent institutions for monitoring theprogress of short-, medium- and long-term activities asdefined in the framework of health policies, strategies,programmes and projects.The key function in development and implementationof the health care monitoring and evaluation systemof the Republic of Srpska will be vested with the PublicHealth Institute of the Republic of Srpska.Dom zdravlja će, u reformisanoj PZZ, biti zdravstvenaustanova odgovorna za zdravstveno stanje stanovništvana području koje pokriva i koja koordinira sve organizacijei pojedince u planiranju, organizaciji, pružanjui kontroli PZZ, uz korišćenje svih raspoloživih resursana lokalnom nivou.Dom zdravlja biće zdravstvena ustanova u kojojsu zaštita i unapređenje zdravlja građana i poboljšanjekvaliteta njihovog života na prvom mjestu.MisijaDom zdravlja biće zdravstvena ustanova koja ćeplanirati, organizovati i pružati stanovništvu određenogpodručja, dostupnu, efikasnu, isplativu i visokokvalitetnuprimarnu zdravstvenu zaštitu koja se zasniva na modeluporodične medicine.■ZadaciDom zdravlja:Prati, istražuje i analizira zdravstveno stanje napodručju lokalne zajednice;<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite41Goal 12. Strengthening the involvement ofthe local community in ensuring primaryhealth careWith regard to health care planning and in additionto the characteristics of the population, the structure ofthe population in the local community, its health status,age groups, it is necessary to know in what ways the communityaffects health of the population, such as labourand employment, social status, environment, bad habitsand risky behaviour. Therefore, it will be necessary tocoordinate all sectors of the local community with thehealth sector, particularly primary health care.(municipalservices, social services, education, water supply, environment,various associations and unions).Given the above, the role of municipalities and theafore mentioned services will have to be defined in lightof new organisational structures of health care providersin primary health care.■ Municipalities should be enabled to finance healthservices at the PHC level. Thus, municipalitiescould be transformed into financiers strengtheningprimary health care.The Primary Health Care Strategy
■■■■■■■■■■■■■Prati, istražuje i analizira uticaj spoljnih faktora nazdravlje stanovništva na području lokalne zajednice;Definiše i planira strateške ciljeve, prioritete iaktivnosti za razvoj PZZ na području lokalnezajednice;Ocjeljuje stepen ostvarenja strateških ciljeva i preduzima,eventualne, korektivne mjere i aktivnosti;Planira, organizuje i pruža usluge PZZ u skladu saprocijenjenim potrebama i zdravstvenim stanjemlokalne zajednice;Planira ljudske resurse za PZZ na području lokalnezajednice;Podržava kontinuiranu i koordiniranu zdravstvenuzaštitu;Organizuje i kontroliše primjenu standardakvaliteta u PZZ;Koordinira rad timova porodične medicine napodručju lokalne zajednice;Obezbjeđuje logističku podršku timovimaporodične medicine;Obezbjeđuje snabdijevanje ampuliranim lijekovima,sanitetskim materijalom i medicinskim sredstvimaneophodnim za rad domova zdravljaObezbjeđuje osnovnu administrativnu podrškutimovima porodične medicine;Ocjenjuje rad timova porodične medicine;Vrednuje učinak implementacije programa promocijezdravlja i prevencije bolesti na poboljšanjezdravstvenog stanja na području lokalne zajednice;■■■Municipalities must develop and improve a numberof functions that entail the following:- Providing incentives for provided quality servicesin primary health care- Ensuring financing of the infrastructure, capitalcosts and rent for premises accommodatingPHC services- co-financing of community-based services(CBRs for physical rehabilitation and mentalhealth) and ER- Ensuring all fundamental functions of publichealthInvolvement of the public and civic society is ofcrucial importance for establishing a balancedsystem of their rights, as well as for better understandingof their obligations and duties on theirside. Such an aspect of involvement of the publicand civic society will be ensured through municipalhealth councils, which consist of the representativesof the municipality, PHC and citizens, variousvoluntary groups and associations of patients.Involvement of the local community in definingpriorities in PHC development in the local area inline with the needs of the local community.Health centre in reformed primaryhealth careVisionIn reformed primary health care, the Health Centrewill be a health institution responsible for the health<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite42The Primary Health Care Strategy
■■■■■■■■■■■■Definiše, razvija i predlaže programe prevencijebolesti čija bi primjena imala veliki učinakna poboljšanje zdravstvenog stanja na područjulokalne zajednice;Koordinira sve organizacije i pojedince kojina direktan ili indirektan način učestvuju uobezbjeđivanju i pružanju PZZ;Podržava izvođenje teoretske i praktične nastave izprograma specijalizacije iz porodične medicine;Planira i organizuje kontinuiranu medicinskuedukaciju i kontinuirano profesionalnousavršavanje;Podržava naučno-istraživački rad u PZZ;Komunicira i upoznaje stanovništvo sa važnimpitanjima zdravlja i zdravstvenog stanja lokalnezajednice;Uključuje lokalnu zajednicu u definisanje prioritetaza razvoj PZZ na lokalnom području;Uključuje lokalnu zajednicu u finansiranje prioritetnihprograma i projekata koji se ne finansirajusa nivoa Republike Srpske, a koji imaju velikiznačaj za lokalnu zajednicu;Obezbjeđuje centralizovano upravljanje medicinskom,materijalno-finansijskom i drugom dokumentacijom;Prikuplja, obrađuje i čuva podatke iz oblasti radau zdravstvu i podatke o zdravstvenom stanjustanovništva;Dostavlja propisane izvještaje nadležnim institucijama;Obezbjeđuje hitan sanitetski prevoz;status of the population in the area it covers, which willcoordinate all organisations and individuals in planning,organisation, delivery and control of primary health careusing all available resources at the local level.The Health Centre will be a health institutionwhere health care and better health of people as wellas enhancement of the quality of their lives will be thecore priority.MissionThe Health Centre will be a health institution thatwill plan, organise and deliver accessible, efficient, costeffectiveand high quality health care based on the familymedicine model to the population of the given area.■■■■■TasksHealth centre is to:monitor, research and analyse the health status ofthe local community in its area of living;monitor, study and analyse the effects of externalfactors on the health of the local community in itsarea of living;define and plan strategic goals, priorities andactivities for PHC development in the local community;evaluate the level of attainment of strategic goalsand undertake possible corrective measures andactivities;plan, organise and deliver PHC services in linewith the estimated needs and health status of thelocal community;<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite43The Primary Health Care Strategy
■■Održava infrastrukturu, objekte i medicinskuopremu;Upravlja svim ostalim djelatnostima u svom sastavu.Dom zdravlja će biti temelj zdravstvenog sistema ipolazna osnova objedinjene <strong>zdravstvene</strong> zaštite.■■■■■■■■■■■■■plan PHC human resources in the local community;support continuous and coordinated health care;organise and control the application of PHC qualitystandards;coordinate the work of family medicine teams inthe local community;provide logistical support to family medicineteams;procure ampouled medicines, medical suppliesand medical substances that are necessary for theof health centresprovide basic administrative support to familymedicine teams;evaluate the performance of family medicineteams;evaluate the effects of promotive and preventiveprogrammes on the improvement of health of thelocal community;define, develop and propose preventive programmes,whose implementation would significantlyaffect the improvement of the health statusof the local community;coordinate all organisations and individuals who,either directly or indirectly, participate in PHCprovision and delivery;support theoretical and practical training sessionsrelated to family medicine specialisation curricula;plan and organise continuing medical educationand professional advancement;<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite44The Primary Health Care Strategy
■■■■■■■■■■support scientific and research work in primaryhealth care;communicate with and informs the populationon important health issues and status of the localcommunity;Involve the local community in defining prioritiesconcerning PHC development in the local area;involve the local community in financing of priorityprogrammes and projects that are not financedfrom the RS level, which are of high importancefor the local community;ensures centralised management of medical, material– financial and other documentation;collect, process and store data related to healthwork and data on the health status of the population;submit required reports to competent institutions;provide emergency transportation;maintain the infrastructure, facilities and medicalequipment;manage other activities under its competence.The health centre will be the foundation of thehealth system and a starting basis of integrated healthcare.<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštite45The Primary Health Care Strategy
<strong>Strategija</strong> <strong>primarne</strong> <strong>zdravstvene</strong> zaštiteRadna grupa projekta EU/WHO“Podrška reformi <strong>zdravstvene</strong> zaštiteu Bosni i Hercegovini” 2004-2006IzdavačMinistarstvo zdravlja i socijalne zaštiteRepublike SrpskeTiraž500Mjesto i godina izdavanjaBanja Luka2006Dizajn i štampaCGM designBanja LukaMinistarstvo zdravlja i socijalne zaštiteVladike Platona bb, 78000 Banja Lukatel +387 51 348 348, fax +387 51 348 360e-mail: ministarstvo-zdravlja@blic.net