Blue Essential Open Access HMO Plans Effective 10/15/09
Blue Essential Open Access HMO Plans Effective 10/15/09
Blue Essential Open Access HMO Plans Effective 10/15/09
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
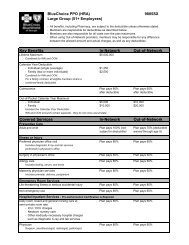
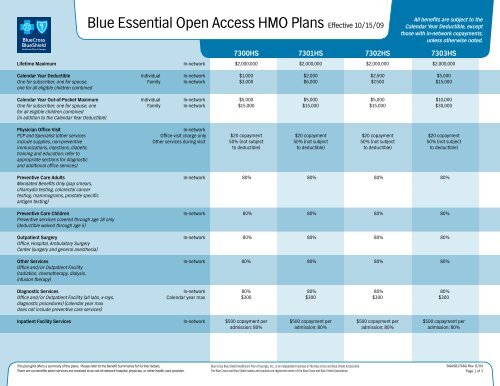
Lifetime Maximum<strong>Blue</strong> <strong>Essential</strong> <strong>Open</strong> <strong>Access</strong> <strong>HMO</strong> <strong>Plans</strong> <strong>Effective</strong> <strong>10</strong>/<strong>15</strong>/<strong>09</strong>In-networkAll benefits are subject to theCalendar Year Deductible, exceptthose with in-network copayments,unless otherwise noted.7300HS 7301HS 7302HS 7303HS$2,000,000 $2,000,000 $2,000,000 $2,000,000Calendar Year Deductible Individual In-networkOne for subscriber, one for spouse, Family In-networkone for all eligible children combinedCalendar Year Out-of-Pocket Maximum Individual In-networkOne for subscriber, one for spouse, one Family In-networkfor all eligible children combined(in addition to the Calendar Year Deductible)$1,000 $2,000 $2,500 $5,000$3,000 $6,000 $7,500 $<strong>15</strong>,000$5,000 $5,000 $5,000 $<strong>10</strong>,000$<strong>15</strong>,000 $<strong>15</strong>,000 $<strong>15</strong>,000 $30,000Physician Office VisitPCP and Specialist (other servicesinclude supplies, non-preventiveimmunizations, injections, diabetictraining and education; refer toappropriate sections for diagnosticand additional office services)Preventive Care AdultsMandated Benefits Only (pap smears,chlamydia testing, colorectal cancertesting, mammograms, prostate specificantigen testing)Preventive Care ChildrenPreventive services covered through age 18 only(deductible waived through age 5)Outpatient SurgeryOffice, Hospital, Ambulatory SurgeryCenter (surgery and general anesthesia)Other ServicesOffice and/or Outpatient Facility(radiation, chemotherapy, dialysis,infusion therapy)Diagnostic ServicesOffice and/or Outpatient Facility (all labs, x-rays,diagnostic procedures) (calendar year maxdoes not include preventive care services)Inpatient Facility ServicesIn-networkOffice visit charge onlyOther services during visitIn-networkIn-networkIn-networkIn-networkIn-networkCalendar year maxIn-network$20 copayment $20 copayment $20 copayment $20 copayment50% (not subject 50% (not subject 50% (not subject 50% (not subjectto deductible) to deductible) to deductible) to deductible)80% 80% 80% 80%80% 80% 80% 80%80% 80% 80% 80%80% 80% 80% 80%80% 80% 80% 80%$300 $300 $300 $300$500 copayment per $500 copayment per $500 copayment per $500 copayment peradmission; 80% admission; 80% admission; 80% admission; 80%This plan grid offers a summary of the plans. Please refer to the Benefit Summaries for further details.There are no benefits when services are received at an out-of-network hospital, physician, or other health care provider.<strong>Blue</strong> Cross <strong>Blue</strong> Shield Healthcare Plan of Georgia, Inc., is an independent licensee of the <strong>Blue</strong> Cross and <strong>Blue</strong> Shield Association.The <strong>Blue</strong> Cross and <strong>Blue</strong> Shield names and symbols are registered marks of the <strong>Blue</strong> Cross and <strong>Blue</strong> Shield Association.BGASB1748G Rev. 8/<strong>09</strong>Page 1 of 3
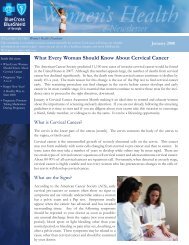
Skilled Nursing Facility<strong>Blue</strong> <strong>Essential</strong> <strong>Open</strong> <strong>Access</strong> <strong>HMO</strong> <strong>Plans</strong> <strong>Effective</strong> <strong>10</strong>/<strong>15</strong>/<strong>09</strong>In-networkCalendar year maxAll benefits are subject to theCalendar Year Deductible, exceptthose with in-network copayments,unless otherwise noted.7300HS 7301HS 7302HS 7303HS$500 copayment per $500 copayment per $500 copayment per $500 copayment peradmission; 80% admission; 80% admission; 80% admission; 80%90 days 90 days 90 days 90 daysInpatient and Outpatient Physician Services(surgeon, anesthesiologist, radiologist, pathologist)In-network80% 80% 80% 80%Mental Health/Substance Abuse Inpatient In-network$500 copayment per $500 copayment per $500 copayment per $500 copayment peradmission; 80% admission; 80% admission; 80% admission; 80%OutpatientIn-networkOffice visit charge onlyOther services during visit 1$20 copayment $20 copayment $20 copayment $20 copayment50% (not subject 50% (not subject 50% (not subject 50% (not subjectto deductible) to deductible) to deductible) to deductible)Emergency Room*Medical Emergency or Accident onlyHome Health CareAmbulance Services(when medically necessary)Hospice CareHuman Organ and Tissue TransplantsAcquistion, Harvest, Storage, andTransplant ProceduresLifetime maximum(for transportation and lodging)Lifetime maximum(for unrelated donor searches forbone marrow/stem cell transplants)Durable Medical Equipment (DME)Only DME required for the treatmentof diabetes and prosthetics are covered(all other DME is excluded)In-networkIn-networkCalendar year maxIn-networkIn-networkIn-networkIn-network$<strong>15</strong>0 copayment; 80% $<strong>15</strong>0 copayment; 80% $<strong>15</strong>0 copayment; 80% $<strong>15</strong>0 copayment; 80%80% 80% 80% 80%60 visits 60 visits 60 visits 60 visits80% 80% 80% 80%80% 80% 80% 80%$500 copayment per $500 copayment per $500 copayment per $500 copayment peradmission; 80% admission; 80% admission; 80% admission; 80%$<strong>10</strong>,000 $<strong>10</strong>,000 $<strong>10</strong>,000 $<strong>10</strong>,000$30,000 $30,000 $30,000 $30,00080% 80% 80% 80%This plan grid offers a summary of the plans. Please refer to the Benefit Summaries for further details.There are no benefits when services are received at an out-of-network hospital, physician, or other health care provider.*ER copay is waived if admitted to the hospital.1 Please refer to the physician office visit benefit for complete details.I<strong>Blue</strong> Cross <strong>Blue</strong> Shield Healthcare Plan of Georgia, Inc., is an independent licensee of the <strong>Blue</strong> Cross and <strong>Blue</strong> Shield Association.The <strong>Blue</strong> Cross and <strong>Blue</strong> Shield names and symbols are registered marks of the <strong>Blue</strong> Cross and <strong>Blue</strong> Shield Association.BGASB1748G Rev. 8/<strong>09</strong>Page 2 of 3
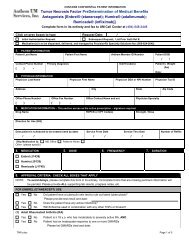
MaternityOffice Visit - 1st visit only<strong>Blue</strong> <strong>Essential</strong> <strong>Open</strong> <strong>Access</strong> <strong>HMO</strong> <strong>Plans</strong> <strong>Effective</strong> <strong>10</strong>/<strong>15</strong>/<strong>09</strong>In-networkOffice visit charge onlyOther services during visit 1All benefits are subject to theCalendar Year Deductible, exceptthose with in-network copayments,unless otherwise noted.7300HS 7301HS 7302HS 7303HS$20 copayment $20 copayment $20 copayment $20 copayment50% (not subject 50% (not subject 50% (not subject 50% (not subjectto deductible) to deductible) to deductible) to deductible)Physician Global Fee(prenatal, delivery, postpartum services)In-network80% 80% 80% 80%Prescription DrugsRetail Drugs Tier 1 (30-day supply)(includes Tier 2 diabetic drugs/supplies)Retail Drugs Tier 2 and 3 (30-day supply)Mail Order Maintenance Drugs Tier 1 (90-day supply)(includes Tier 2 diabetic drugs/supplies)Mail Order Maintenance Drugs Tier 2 (90-day supply)In-networkIn-networkIn-networkIn-network$<strong>15</strong> $<strong>15</strong> $<strong>15</strong> $<strong>15</strong>0%, but member receives 0%, but member receives 0%, but member receives 0%, but member receivesnetwork discount network discount network discount network discount$30 $30 $30 $300%, but member receives 0%, but member receives 0%, but member receives 0%, but member receivesnetwork discount network discount network discount network discountThis plan grid offers a summary of the plans. Please refer to the Benefit Summaries for further details.There are no benefits when services are received at an out-of-network hospital, physician, or other health care provider.1 Please refer to the physician office visit benefit for complete details.<strong>Blue</strong> Cross <strong>Blue</strong> Shield Healthcare Plan of Georgia, Inc., is an independent licensee of the <strong>Blue</strong> Cross and <strong>Blue</strong> Shield Association.The <strong>Blue</strong> Cross and <strong>Blue</strong> Shield names and symbols are registered marks of the <strong>Blue</strong> Cross and <strong>Blue</strong> Shield Association.BGASB1748G Rev. 8/<strong>09</strong>Page 3 of 3