Diagnosis and Treatment of Community-Acquired Pneumonia
Diagnosis and Treatment of Community-Acquired Pneumonia
Diagnosis and Treatment of Community-Acquired Pneumonia
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
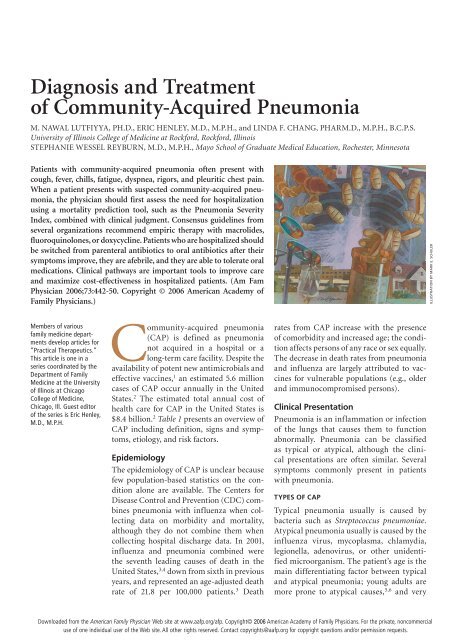
<strong>Diagnosis</strong> <strong>and</strong> <strong>Treatment</strong><strong>of</strong> <strong>Community</strong>-<strong>Acquired</strong> <strong>Pneumonia</strong>M. NAWAL LUTFIYYA, PH.D., ERIC HENLEY, M.D., M.P.H., <strong>and</strong> LINDA F. CHANG, PHARM.D., M.P.H., B.C.P.S.University <strong>of</strong> Illinois College <strong>of</strong> Medicine at Rockford, Rockford, IllinoisSTEPHANIE WESSEL REYBURN, M.D., M.P.H., Mayo School <strong>of</strong> Graduate Medical Education, Rochester, MinnesotaPatients with community-acquired pneumonia <strong>of</strong>ten present withcough, fever, chills, fatigue, dyspnea, rigors, <strong>and</strong> pleuritic chest pain.When a patient presents with suspected community-acquired pneumonia,the physician should first assess the need for hospitalizationusing a mortality prediction tool, such as the <strong>Pneumonia</strong> SeverityIndex, combined with clinical judgment. Consensus guidelines fromseveral organizations recommend empiric therapy with macrolides,fluoroquinolones, or doxycycline. Patients who are hospitalized shouldbe switched from parenteral antibiotics to oral antibiotics after theirsymptoms improve, they are afebrile, <strong>and</strong> they are able to tolerate oralmedications. Clinical pathways are important tools to improve care<strong>and</strong> maximize cost-effectiveness in hospitalized patients. (Am FamPhysician 2006;73:442-50. Copyright © 2006 American Academy <strong>of</strong>Family Physicians.)ILLUSTRATION BY MARK E. SCHULERMembers <strong>of</strong> variousfamily medicine departmentsdevelop articles for“Practical Therapeutics.”This article is one in aseries coordinated by theDepartment <strong>of</strong> FamilyMedicine at the University<strong>of</strong> Illinois at ChicagoCollege <strong>of</strong> Medicine,Chicago, Ill. Guest editor<strong>of</strong> the series is Eric Henley,M.D., M.P.H.<strong>Community</strong>-acquired pneumonia(CAP) is defined as pneumonianot acquired in a hospital or along-term care facility. Despite theavailability <strong>of</strong> potent new antimicrobials <strong>and</strong>effective vaccines, 1 an estimated 5.6 millioncases <strong>of</strong> CAP occur annually in the UnitedStates. 2 The estimated total annual cost <strong>of</strong>health care for CAP in the United States is$8.4 billion. 2 Table 1 presents an overview <strong>of</strong>CAP including definition, signs <strong>and</strong> symptoms,etiology, <strong>and</strong> risk factors.EpidemiologyThe epidemiology <strong>of</strong> CAP is unclear becausefew population-based statistics on the conditionalone are available. The Centers forDisease Control <strong>and</strong> Prevention (CDC) combinespneumonia with influenza when collectingdata on morbidity <strong>and</strong> mortality,although they do not combine them whencollecting hospital discharge data. In 2001,influenza <strong>and</strong> pneumonia combined werethe seventh leading causes <strong>of</strong> death in theUnited States, 3,4 down from sixth in previousyears, <strong>and</strong> represented an age-adjusted deathrate <strong>of</strong> 21.8 per 100,000 patients. 3 Deathrates from CAP increase with the presence<strong>of</strong> comorbidity <strong>and</strong> increased age; the conditionaffects persons <strong>of</strong> any race or sex equally.The decrease in death rates from pneumonia<strong>and</strong> influenza are largely attributed to vaccinesfor vulnerable populations (e.g., older<strong>and</strong> immunocompromised persons).Clinical Presentation<strong>Pneumonia</strong> is an inflammation or infection<strong>of</strong> the lungs that causes them to functionabnormally. <strong>Pneumonia</strong> can be classifiedas typical or atypical, although the clinicalpresentations are <strong>of</strong>ten similar. Severalsymptoms commonly present in patientswith pneumonia.types <strong>of</strong> capTypical pneumonia usually is caused bybacteria such as Streptococcus pneumoniae.Atypical pneumonia usually is caused by theinfluenza virus, mycoplasma, chlamydia,legionella, adenovirus, or other unidentifiedmicroorganism. The patient’s age is themain differentiating factor between typical<strong>and</strong> atypical pneumonia; young adults aremore prone to atypical causes, 5,6 <strong>and</strong> veryDownloaded from the American Family Physician Web site at www.aafp.org/afp. Copyright© 2006 American Academy <strong>of</strong> Family Physicians. For the private, noncommercialuse <strong>of</strong> one individual user <strong>of</strong> the Web site. All other rights reserved. Contact copyrights@aafp.org for copyright questions <strong>and</strong>/or permission requests.
SORT: KEY RECOMMENDATIONS FOR PRACTICEClinical recommendationEvidenceratingReferencesPatients with suspected community-acquired pneumonia (CAP) shouldreceive chest radiography.The <strong>Pneumonia</strong> Severity Index should be used to assist in decisionsregarding hospitalization <strong>of</strong> patients with CAP.The initial treatment <strong>of</strong> CAP is empiric, <strong>and</strong> macrolides or doxycycline(Vibramycin) should be used in most patients.Respiratory fluoroquinolones should be used when patients have failedfirst-line regimens, have significant comorbidities, havehad recent antibiotic therapy, are allergic to alternative agents, or havea documented infection with highly drug-resistant pneumococci.C 8A 8, 9, 15, 16C 8, 9, 29C 8, 9, 28, 29A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence;C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For informationabout the SORT evidence rating system, see page 374 or http://www.aafp.org/afpsort.xml.young <strong>and</strong> older persons are more predisposedto typical causes.symptomsCommon clinical symptoms <strong>of</strong> CAP includecough, fever, chills, fatigue, dyspnea, rigors,<strong>and</strong> pleuritic chest pain. Depending on thepathogen, a patient’s cough may be persistent<strong>and</strong> dry, or it may produce sputum. Other presentationsmay include headache <strong>and</strong> myalgia.Certain etiologies, such as legionella, also mayproduce gastrointestinal symptoms.<strong>Diagnosis</strong>physical examinationPhysical examination may reveal dullnessto percussion <strong>of</strong> the chest, crackles or raleson auscultation, bronchial breath sounds,table 1Overview <strong>of</strong> <strong>Community</strong>-<strong>Acquired</strong> <strong>Pneumonia</strong>DefinitionLower respiratory tract infection in anonhospitalized person that is associated withsymptoms <strong>of</strong> acute infection with or withoutnew infiltrate on chest radiographsClinical presentationTemperature greater than 38˚C (100.4˚F)Cough with or without sputum, hemoptysisPleuritic chest painMyalgiaGastrointestinal symptomsDyspneaMalaise, fatigueRales, rhonchi, wheezingEgophony, bronchial breath soundsDullness to percussionAtypical symptoms in older patientsEtiologyBacterialChlamydia speciesHaemophilus influenzaeLegionella speciesMoraxella catarrhalisMycoplasma pneumoniaeStaphylococcus aureusStreptococcus pneumoniaeViralAdenovirusInfluenza A <strong>and</strong> BParainfluenzaRespiratory syncytial virusEndemic fungiBlastomycosisCoccidioidomycosisHistoplasmosisRisk factorsAge older than 65 yearsHuman immunodeficiency virus orimmunocompromisedRecent antibiotic therapy or resistanceto antibioticsComorbiditiesAsthmaCerebrovascular diseaseChronic obstructive pulmonarydiseaseChronic renal failureCongestive heart failureDiabetesLiver diseaseNeoplastic diseaseFebruary 1, 2006 ◆ Volume 73, Number 3 www.aafp.org/afp American Family Physician 443
<strong>Community</strong>-<strong>Acquired</strong> <strong>Pneumonia</strong>tactile fremitus, <strong>and</strong> egophony (“E” to “A”changes). The patient also may be tachypneic.A prospective study 7 showed thatpatients with typical pneumonia were morelikely than not to present with dyspnea <strong>and</strong>bronchial breath sounds on auscultation.radiographyChest radiography (posteroanterior <strong>and</strong> lateralviews) has been shown to be a critical componentin diagnosing pneumonia. 8 According totable 2Sensitivity <strong>and</strong> Specificity <strong>of</strong> Diagnostic Tests for CAPDiagnostic tests by pathogen Sensitivity (%) Specificity (%)ChlamydiaRapid PCR (sputum, BAL fluid) 30 to 95 > 95Serology (fourfold rise in serum<strong>and</strong> convalescent titers)10 to 100 —Sputum culture 10 to 80 > 95Gram-negative rodsSputum Gram stain 15 to 100 11 to 100Haemophilus influenzae,Moraxella catarrhalis,<strong>Pneumonia</strong>eSputum cultureInfluenzaDiagnostic yield20 to 79*Rapid DFA (sputum, BAL fluid) 22 to 75 90Legionella pneumophilaDFA (sputum, BAL fluid) 22 to 75 90PCR (sputum, BAL fluid) 83 to 100 > 95Serum acute titer 10 to 27 > 85Urinary antigen 55 to 90 > 95Mycoplasma pneumoniaeAntibiotic titers 75 to 95 > 90Cold agglutinins 50 to 60 —PCR (sputum, BAL fluid) 30 to 95 > 95Pneumococcal pneumoniaeChest radiography (lobar infiltrate) 40† —Sputum cultureDiagnostic yield20 to 79*Diagnostic yield20 to 79*Diagnostic yield20 to 79*Sputum Gram stain 15 to 100 11 to 100CAP = community-acquired pneumonia; PCR = polymerase chain reaction; BAL =bronchoalveolar lavage; DFA = direct fluorescence antibody.*—Overgrowth <strong>of</strong> oral flora, isolation <strong>of</strong> atypical agents requires special media.†—Acute symptoms.Information from references 2, 8, 11, <strong>and</strong> 13.the latest American Thoracic Society (ATS)guidelines for the diagnosis <strong>and</strong> treatment <strong>of</strong>adults with CAP, “all patients with suspectedCAP should have a chest radiograph to establishthe diagnosis <strong>and</strong> identify complications(pleural effusion, multilobar disease).” 8 Chestradiography may reveal a lobar consolidation,which is common in typical pneumonia; orit could show bilateral, more diffuse infiltratesthan those commonly seen in atypicalpneumonia. However, chest radiographyperformed early in the course <strong>of</strong> the diseasecould be negative.laboratory testsHistorically, common laboratory tests forpneumonia have included leukocyte count,sputum Gram stain, two sets <strong>of</strong> blood cultures,<strong>and</strong> urine antigens. However, thevalidity <strong>of</strong> these tests has recently beenquestioned after low positive culture rateswere found (e.g., culture isolates <strong>of</strong> S. pneumoniaewere present in only 40 to 50 percent<strong>of</strong> cases). 9 Such low positive culture ratesare likely due to problems with retrievingsamples from the lower respiratory tract,previous administration <strong>of</strong> antibiotics, contaminationfrom the upper airways, faultyseparation <strong>of</strong> sputum from saliva whenstreaking slides or plates, 9 or viral etiology.Furthermore, sputum samples are adequatein only 52.3 percent <strong>of</strong> patients with CAP,<strong>and</strong> only 44 percent <strong>of</strong> those samples containpathogens. 10 Nonetheless, initial therapy<strong>of</strong>ten is guided by the assumption that thepresenting disease is caused by a commonbacterial pathogen.Findings 11 also cast doubt on the clinicalutility <strong>of</strong> obtaining blood cultures frompatients with suspected CAP. In a study 12 <strong>of</strong>CAP cases in 19 Canadian hospitals over asix-month period, positive blood cultureswere obtained in only 5.2 to 6.2 percent<strong>of</strong> patients, including those with the mostsevere disease. Based on these findings,other researchers 13 concluded that a positiveblood culture had no correlation with theseverity <strong>of</strong> the illness or outcome. Anotherprospective study 10 showed that blood cultureswere positive in only 10.5 percent <strong>of</strong>patients with pneumonia. Despite these <strong>and</strong>444 American Family Physician www.aafp.org/afp Volume 73, Number 3 ◆ February 1, 2006
<strong>Community</strong>-<strong>Acquired</strong> <strong>Pneumonia</strong>other research findings, current ATS guidelines8 recommend that patients hospitalizedfor suspected CAP receive two sets <strong>of</strong> bloodcultures. Blood cultures, however, are notnecessary for outpatient diagnosis. 8Legionella antigens were found in theurine <strong>of</strong> 48 percent <strong>of</strong> patients with suspectedLegionella pneumophila serogroup 1 infection.14 Table 2 2,8,11,13 includes the sensitivity<strong>and</strong> specificity <strong>of</strong> diagnostic tests for CAP.<strong>Treatment</strong>Initial treatment <strong>of</strong> CAP is based on physicalexamination findings, laboratory results,<strong>and</strong> patient characteristics (e.g., age, chronicillnesses, history <strong>of</strong> smoking, history <strong>of</strong> theillness). 15 Physicians should begin theirtreatment decisions by assessing the need forhospitalization using a prediction tool forincreased mortality, such as the <strong>Pneumonia</strong>Severity Index (Table 3 15 ), combined withclinical judgment. 9outpatient vs. inpatient treatmentChoosing between outpatient <strong>and</strong> inpatienttreatment is a crucial decision because <strong>of</strong>the possible risk <strong>of</strong> death. 9,15,16 This decisionnot only influences diagnostic testing <strong>and</strong>medication choices, it can have a psychologicalimpact on patients <strong>and</strong> their families. Onaverage, the estimated cost for inpatient care<strong>of</strong> patients with CAP is $7,500. Outpatientcare can cost as little as $150 to $350. 17-19Hospitalization <strong>of</strong> a patient should dependon patient age, comorbidities, <strong>and</strong> the severity<strong>of</strong> the presenting disease. 9,20Physicians tend to overestimate a patient’srisk <strong>of</strong> death 14 ; therefore, many low-riskpatients who could be safely treated as outpatientsare admitted for more costly inpatientcare. The <strong>Pneumonia</strong> Severity Index(Table 3 15 ) was developed to assist physiciansin identifying patients at a higherrisk <strong>of</strong> complications <strong>and</strong> who are morelikely to benefit from hospitalization. 9,15,16Investigators developed a risk model basedon a prospective cohort study 16 <strong>of</strong> 2,287patients with CAP in Pittsburgh, Boston,<strong>and</strong> Halifax, Nova Scotia. By usingthe model, the authors found that 26 to31 percent <strong>of</strong> the hospitalized patients weregood outpatient c<strong>and</strong>idates, <strong>and</strong> an additional13 to 19 percent only needed briefhospital observation. They validated thismodel using data 17 from more than 50,000patients with CAP in 275 U.S. <strong>and</strong> Canadianhospitals. 15-17,21,22TABLE 3<strong>Pneumonia</strong> Severity IndexPatient CharacteristicsPointsDemographicsMaleAge (years)Female Age (years) − 10Nursing home resident + 10Comorbid illnessNeoplastic disease + 30Liver disease + 20Congestive heart failure + 10Cerebrovascular disease + 10Renal disease + 10Physical examination findingsAltered mental status + 20Respiratory rate > 30 breaths per minute + 20Systolic blood pressure < 90 mm Hg + 20Temperature < 35˚C (95˚F) or > 40˚C (104˚F) + 15Pulse rate > 125 beats per minute + 10Laboratory <strong>and</strong> radiographic findingsArterial pH < 7.35 + 30Blood urea nitrogen > 64 mg per dL+ 20(22.85 mmol per L)Sodium < 130 mEq per L (130 mmol per L) + 20Glucose > 250 mg per dL (13.87 mmol per L) + 10Hematocrit < 30 percent + 10Partial pressure <strong>of</strong> arterial oxygen < 60 mm Hg or + 10oxygen percent saturation < 90 percentPleural effusion + 10Total points:Point totalRiskRiskclassMortality %(No. <strong>of</strong> patients)Recommendedsite <strong>of</strong> careNo predictors Low I 0.1 (3,034) Outpatient≤ 70 Low II 0.6 (5,778) Outpatient71 to 90 Low III 2.8 (6,790) Inpatient(briefly)91 to 130 Moderate IV 8.2 (13,104) Inpatient> 130 High V 29.2 (9,333) InpatientInformation from reference 15.February 1, 2006 ◆ Volume 73, Number 3 www.aafp.org/afp American Family Physician 445
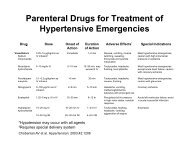
<strong>Community</strong>-<strong>Acquired</strong> <strong>Pneumonia</strong>Management <strong>of</strong> CAPNoTreat as outpatientPreferred antibioticsMacrolides (level A)Fluoroquinolones (level A)Doxycycline (Vibramycin)Alternative antibioticsAmoxicillin/clavulanate(Augmentin) (level A)Beta-lactam (cefpodoxime[Vantin], cefprozil [Cefzil],cefuroxime [Ceftin]) (level A)Although the <strong>Pneumonia</strong> Severity Indexcan serve as a general guideline for management,clinical judgment should alwayssupersede the prognostic score. 9pharmacotherapyThe primary goals <strong>of</strong> pharmacotherapy forpatients with CAP include eradicating thecausative pathogens, resolving the clinicalsigns <strong>and</strong> symptoms, minimizing hospitalization,<strong>and</strong> preventing reinfection. 23-27 Physiciansshould choose a medication based on thepharmacokinetic pr<strong>of</strong>ile, adverse reactions,drug interactions, <strong>and</strong> cost-effectiveness. 23-27Further, patient evaluation should focus onseverity <strong>of</strong> illness, patient age, comorbidities,clinical presentation, epidemiologic setting,<strong>and</strong> previous exposure. 9 The majority<strong>of</strong> patients with CAP are treated empiricallybased on the most common pathogen(s)associated with the condition. 23-27CAP diagnosisComorbidities presentAssign a risk class (see Table 3)Low risk classII <strong>and</strong> IIIFigure 1. Algorithm for the management <strong>of</strong> CAP. (CAP = communityacquiredpneumonia.)Adapted with permission from Fish D. <strong>Pneumonia</strong>. PSAP, Pharmacotherapy Self-AssessmentProgram. Kansas City, Mo.: American College <strong>of</strong> Clinical Pharmacy, 2002:202.YesModerate risk class IV<strong>and</strong> high-risk class VTreat as inpatientPreferred antibioticsIntravenous beta-lactam(cefotaxime [Claforan] orceftriaxone [Rocephin]) plusa macrolide (level A) or afluoroquinolone alone (level A)Consensus guidelines from ATS, 8 InfectiousDiseases Society <strong>of</strong> America, 9 <strong>and</strong>Canadian Guidelines for the Initial Management<strong>of</strong> <strong>Community</strong>-<strong>Acquired</strong> <strong>Pneumonia</strong> 28(Figure 1 6 ) recommend initial empiric therapywith macrolides, fluoroquinolones, ordoxycycline (Vibramycin). A fourth guideline29 developed by the Therapeutic WorkingGroup <strong>of</strong> the CDC, however, recommendsusing fluoroquinolones sparingly because <strong>of</strong>resistance concerns.Although data are limited on duration<strong>of</strong> CAP therapy, current research 30 recommendsseven to 10 days <strong>of</strong> therapy forS. pneumoniae <strong>and</strong> 10 to 14 days <strong>of</strong> therapyfor Mycoplasma pneumoniae <strong>and</strong> Chlamydiapneumoniae. After a hospitalized patient isclinically stable (i.e., temperature less than37.8° C [100.0° F], pulse under 100 beats perminute, respiratory rate below 24 breathsper minute, systolic blood pressure above90 mm Hg, <strong>and</strong> blood oxygen saturationover 90 percent) <strong>and</strong> able to tolerate oralintake, the patient may be treated with oralantibiotics for the remainder <strong>of</strong> the therapycourse. This can save money <strong>and</strong> allow forearlier hospital discharge, which minimizes apatient’s risk <strong>of</strong> hospital-acquired infection.Pneumococcal ResistanceS. pneumoniae, which accounts for 60 to70 percent <strong>of</strong> all bacterial CAP cases, canaffect all patient groups <strong>and</strong> can cause a fatalform <strong>of</strong> CAP. The alarming rate <strong>of</strong> resistanceto many commonly used antibiotics raisesgreat concern. Penicillin-resistant S. pneumoniaewas uncommon in the early 1990s buthas since become increasingly prevalent. 29,31Resistant strains are classified as havingintermediate or high-level resistance. Surveillancedata in the United States 30 revealedthat, overall, pneumococcal strains had a28 percent immediate resistance rate <strong>and</strong> a16 percent high-level resistance rate. Decreasedsusceptibility to other commonlyused antibiotics has also been observed(Table 4 32 ). 29-31 The clinical importance <strong>of</strong>these data is questionable because recruitingpatients infected with resistant pathogensfor clinical trials is difficult. Furthermore,available outcomes on the treatment <strong>of</strong>446 American Family Physician www.aafp.org/afp Volume 73, Number 3 ◆ February 1, 2006
Table 4Patterns <strong>of</strong> Resistance to Antibioticsin North America*AntibioticPenicillinsAmoxicillin/clavulanate(Augmentin)Resistance(%)†4.1Penicillin 21.3CephalosporinsCefepime (Maxipime) 0.4Cefprozil (Cefzil) 23.9Ceftriaxone (Rocephin) 1.9Cefuroxime (Ceftin) 24.7MacrolidesAzithromycin (Zithromax) 23.0Clarithromycin (Biaxin) 26.6Erythromycin 28.3FluoroquinolonesGatifloxacin (Tequin) 0.7Lev<strong>of</strong>loxacin (Levaquin) 0.7Moxifloxacin (Avelox) 0.4MiscellaneousClindamycin (Cleocin) 9.2Tetracycline 18.8Trimethoprim/sulfamethoxazole(Bactrim, Septra)29.9Vancomycin (Vancocin) 0.0*—Antibiotics tested against Streptococcus pneumoniaeisolates.†—Resistance rates averaged across all patient agegroups.Information from reference 32.pneumonia caused by resistant pneumococcalstrains are conflicting. 30The CDC <strong>and</strong> others recommend outpatientoral empirical antibiotics with a macrolide,doxycycline, or an oral beta-lactam(amoxicillin, cefuroxime [Ceftin], or amoxicillin/clavulanate[Augmentin]) or inpatienttreatment with an intravenous beta-lactam(cefuroxime, ceftriaxone [Rocephin], cefotaxime[Claforan]) or a combination <strong>of</strong>ampicillin/sulbactam (Unasyn) with a macrolide(Figure 1 6 ). 28,29 Conservative use <strong>of</strong>new fluoroquinolones (lev<strong>of</strong>loxacin [Levaquin],gatifloxacin [Tequin], moxifloxacin[Avelox]) also is recommended to minimizeresistance patterns. 28,29 The new fluoroquinolones(minimum inhibitory concentration:4 mcg per mL or greater) should be usedonly when patients have failed recommendedfirst-line regimens, are allergic to alternativeagents, or have a documented infection withhighly drug-resistant pneumococci such asthose resistant to penicillin. 28,29Cost <strong>of</strong> Antimicrobial TherapyEconomic pressures have accentuated thefocus on reducing health care costs <strong>and</strong>utilizing resources while maintaining orimproving quality <strong>of</strong> care. 31 These pressuresare exacerbated by the growing resistance<strong>of</strong> S. pneumoniae to penicillin. 31,32 This pattern<strong>of</strong> resistance increases the cost <strong>of</strong> treatmentbecause <strong>of</strong> prolonged hospitalization,relapses, <strong>and</strong> the use <strong>of</strong> more expensiveantibacterial agents. 33-37reducing costsNumerous methods for reducing costs whentreating patients with bacterial infectionscan be applied to CAP (Table 5). Choosingmonotherapy instead <strong>of</strong> combination therapyTable 5Strategies for Reducing the Cost<strong>of</strong> Antibiotic TherapyAdministrationUse the shortest appropriate course possible.Switch from parenteral to oral antibiotics assoon as clinically appropriate.Adverse eventsAvoid agents with serious or costly adverseeffects.Avoid agents known to induce resistance.Drug costCompare low impact with total hospital costs(but significant to pharmacy costs).HospitalizationUse knowledge <strong>of</strong> local resistance to initiateearly therapy with appropriate spectrumagent (few data available).Consider availability <strong>and</strong> cost-effectiveness<strong>of</strong> intravenous versus oral administration.MonitoringAvoid agents that require therapeuticmonitoring or laboratory safety tests.PharmacotherapyUse long-acting antibiotics.Use potent bactericides.Avoid antibiotics with poor tissue penetration.<strong>Community</strong>-<strong>Acquired</strong> <strong>Pneumonia</strong>February 1, 2006 ◆ Volume 73, Number 3 www.aafp.org/afp American Family Physician 447
Table 6Antimicrobial Therapies for CAPAgent Dosage* Cost per course† (generic) Common adverse reactions‡CephalosporinsCefotaxime (Claforan)Cefpodoxime (Vantin)Cefprozil (Cefzil)Ceftriaxone (Rocephin)Cefuroxime (Ceftin)1 g IV every six to eight hours200 mg orally twice per day500 mg orally twice per day1 g IV every 24 hours500 mg orally twice per day0.75 to 1.5 g IV every eight hours$355 (330)124 (110)192392219 oral250 to 358 IVMild diarrheaRashClindamycinsClindamycin (Cleocin)300 mg orally every six hours600 mg IV every eight hours238 (148 to 168) oral250 IVMild diarrheaAbdominal painPseudomembranous colitisRashFluoroquinolonesGatifloxacin (Tequin)Lev<strong>of</strong>loxacin (Levaquin)Moxifloxacin (Avelox)400 mg orally or IV once per day500 mg orally or IV once per day400 mg orally once per day98 oral, 382 IV56 oral, 438 IV107Mild diarrheaNauseaVomitingConstipationDizzinessHeadacheMacrolidesAzithromycin (Zithromax)Clarithromycin (Biaxin)Erythromycin500 mg orally for one dose, then250 mg once per day for four doses500 mg IV every 24 hours500 mg orally twice per day500 mg orally every six hours500 to 1,000 mg IV every six hours49 to 60 oral295 IV9617 (8 to 10) oral(167) IVMild diarrheaNauseaVomitingAbdominal painRashPenicillinsAmoxicillinAmoxicillin/clavulanate(Augmentin)Penicillin GPenicillin V500 mg orally every eight hours875 mg orally every 12 hours875 mg/125mg orally every 12 hours1 to 3 mU IV every four hours500 mg orally four times per day4 (4 to 8)20 (18 to 19)166 (110 to 115)(273)15 (9 to 15)Mild diarrheaNauseaVomitingRashTetracyclinesDoxycycline (Vibramycin) 100 mg orally twice per day 102 (16 to 21)Mild diarrheaNauseaVomitingPhototoxicityCAP = community-acquired pneumonia; IV = intravenously.*—Usual duration for adults with CAP <strong>and</strong> normal renal function is 10 to 14 days.†—Estimated cost to the pharmacist based on average wholesale prices in Red Book. Montvale, N.J.: Medical Economics Data, 2005. Cost to thepatient will be higher, depending on prescription filling fee.‡—Adverse events occurring at a rate <strong>of</strong> approximately 1 to 10 percent.Adapted with permission from Fish D. <strong>Pneumonia</strong>. Pharmacotherapy Self-Assessment Program. 4th ed. Kansas City, Mo.: American College <strong>of</strong> ClinicalPharmacy 2002:198.reduces costs associated with administeringan antibacterial. 33-37 Using agents with longerhalf-lives allows for once-daily administration,which in turn leads to improvedcompliance <strong>and</strong> outcomes <strong>and</strong> decreasedcosts. 33-37 In addition, transitioning patientsto oral therapy as soon as they are clinicallystable can significantly reduce the length<strong>of</strong> hospitalization—the major contributingfactor to health care costs. 33-37448 American Family Physician www.aafp.org/afp Volume 73, Number 3 ◆ February 1, 2006
<strong>Community</strong>-<strong>Acquired</strong> <strong>Pneumonia</strong>cost-effective careWhen choosing a treatment, it is essential tocompare costs <strong>and</strong> outcomes <strong>of</strong> all recommendeddrug therapies. 31 Table 6 6 includesthe costs <strong>of</strong> <strong>and</strong> common adverse reactionsto antimicrobial therapies for CAP.The goal <strong>of</strong> a formal pharmacoeconomicassessment is to enhance overall patient careusing available resources. The evaluationshould lead to a decision that will maximizethe value <strong>of</strong> health care services, not simplyreduce the costs <strong>of</strong> drug therapy. For instance,a particular drug may be more expensive, butit may also be more effective, thus loweringoverall costs. Another drug may have a higherrate <strong>of</strong> treatment failures, creating addedcosts associated with managing the failures.The overall cost <strong>of</strong> each therapy should beobtained by comparing the end cost with theprobability <strong>of</strong> achieving a positive outcome.Depending on the relative costs associatedwith treatment failures compared with thecosts <strong>of</strong> cures, the decision to choose oneagent over another may change.The best way to apply cost-savingapproaches to the treatment <strong>of</strong> patients withCAP is by using a clinical pathway. 38 Thisis a method <strong>of</strong> facilitating multidisciplinarypatient care by moving processes <strong>of</strong> caresequentially through various stages, withinspecified time frames, toward a desired outcome.These pathways should be specific toeach institution, taking into account resistancerates in the community <strong>and</strong> encouraging theuse <strong>of</strong> the most active, cost-effective agents toproduce rapid, positive clinical outcomes. 31,39The authors thank Joel Emery McCullough, M.D., M.S.,M.P.H., <strong>and</strong> Adam Reyburn, M.D., for their assistance inthe preparation <strong>of</strong> the manuscript.The AuthorsM. NAWAL LUTFIYYA, PH.D., is assistant pr<strong>of</strong>essor <strong>and</strong>director <strong>of</strong> research in the Department <strong>of</strong> Family <strong>and</strong><strong>Community</strong> Medicine at the University <strong>of</strong> Illinois College <strong>of</strong>Medicine at Rockford. She also is adjunct assistant pr<strong>of</strong>essorin the University <strong>of</strong> Illinois at Chicago (UIC) School <strong>of</strong> PublicHealth. Dr. Lutfiyya earned her doctorate at the University <strong>of</strong>Massachusetts at Amherst after completing other graduateleveltraining at the University <strong>of</strong> Iowa, Iowa City.ERIC HENLEY, M.D., M.P.H., is associate pr<strong>of</strong>essor <strong>and</strong> head<strong>of</strong> the Department <strong>of</strong> Family <strong>and</strong> <strong>Community</strong> Medicine atthe University <strong>of</strong> Illinois College <strong>of</strong> Medicine at Rockford.He is an adjunct faculty member in the UIC School <strong>of</strong>Public Health. Dr. Henley received his medical degree fromGeorgetown University, Washington, D.C., <strong>and</strong> completed afamily medicine residency at the University <strong>of</strong> ConnecticutSchool <strong>of</strong> Medicine, Hartford. He earned his master’s inpublic health at Harvard Medical School, Boston, Mass.LINDA F. CHANG, PHARM.D., M.P.H., B.C.P.S., is clinicalassistant pr<strong>of</strong>essor in the Department <strong>of</strong> Family <strong>and</strong><strong>Community</strong> Medicine <strong>and</strong> the Department <strong>of</strong> PharmacyPractice at the University <strong>of</strong> Illinois College <strong>of</strong> Medicineat Rockford. She received a doctorate in pharmacy at UIC<strong>and</strong> completed a general practice pharmacy residency atthe Chicago Veterans Administration Hospital.STEPHANIE WESSEL REYBURN, M.D., M.P.H., is a familypractice resident at the Mayo School <strong>of</strong> Graduate MedicalEducation, Rochester, Minn. She received her medical degreeat the University <strong>of</strong> Illinois College <strong>of</strong> Medicine at Rockford<strong>and</strong> her master’s at the UIC School <strong>of</strong> Public Health.Address correspondence to M. Nawal Lutfiyya, Ph.D.,University <strong>of</strong> Illinois College <strong>of</strong> Medicine at Rockford,Department <strong>of</strong> Family <strong>and</strong> <strong>Community</strong> Medicine, 1601Parkview Ave., Rockford, IL 61107 (email: lutfiyya@uic.edu). Reprints are not available from the authors.Author disclosure: Nothing to disclose.REFERENCES1. Andrews J, Nadjm B, Gant V, Shetty N. <strong>Community</strong>acquiredpneumonia. Curr Opin Pulm Med 2003;9:175-80.2. Niederman MS. <strong>Community</strong>-acquired pneumonia: managementcontroversies, part 1; practical recommendationsfrom the latest guidelines. J Respir Dis 2002;23:10-7.3. Arias E, Anderson RN, Kung HC, Murphy SL, KochanekKD. Deaths: final data for 2001. Natl Vital Stat Rep 2003;52:1-115.4. Hall MJ, DeFrances CJ. 2001 National hospital dischargesurvey. Adv Data 2004:1-20.5. File TM. <strong>Community</strong>-acquired pneumonia. Lancet2003;362:1991-2001.6. Fish D. <strong>Pneumonia</strong>. In: Pharmacotherapy self-assessmentprogram. 4th ed. Kansas City: American College<strong>of</strong> Clinical Pharmacy, 2002.7. Beovic B, Bonac B, Kese D, Avsic-Zupanc T, Kreft S,Lesnicar G, et al. Aetiology <strong>and</strong> clinical presentation <strong>of</strong>mild community-acquired bacterial pneumonia. Eur JClin Microbiol Infect Dis 2003;22:584-91.8. Niederman MS, M<strong>and</strong>ell LA, Anzueto A, Bass JB,Broughton WA, Campbell GD, et al. American ThoracicSociety. Guidelines for the management <strong>of</strong> adults withcommunity-acquired pneumonia. <strong>Diagnosis</strong>, assessment<strong>of</strong> severity, antimicrobial therapy, <strong>and</strong> prevention.Am J Respir Crit Care Med 2001;163:1730–54.9. M<strong>and</strong>ell LA, Bartlett JG, Dowell SF, File TM Jr, MusherDM, Whitney C. Infectious Diseases Society <strong>of</strong> America.Update <strong>of</strong> practice guidelines for the management <strong>of</strong>community-acquired pneumonia in immunocompetentadults. Clin Infect Dis 2003;37:1405-33.10. Sopena N, Sabria M, Pedro-Botet ML, ManterolaJM, Matas L, Dominguez J, et al. Prospective study <strong>of</strong>February 1, 2006 ◆ Volume 73, Number 3 www.aafp.org/afp American Family Physician 449
<strong>Community</strong>-<strong>Acquired</strong> <strong>Pneumonia</strong>community-acquired pneumonia <strong>of</strong> bacterial etiology inadults. Eur J Clin Microbiol Infect Dis 1999;18:852-8.11. Campbell SG, Marrie TJ, Anstey R, Dickinson G, Ackroyd-StolarzS. The contribution <strong>of</strong> blood cultures to theclinical management <strong>of</strong> adult patients admitted to thehospital with community-acquired pneumonia: a prospectiveobservational study. Chest 2003;123:1142-50.12. Feagan BG. A controlled trial <strong>of</strong> a critical pathwayfor treating community-acquired pneumonia: theCAPITAL study. <strong>Community</strong>-<strong>Acquired</strong> <strong>Pneumonia</strong> InterventionTrial Assessing Lev<strong>of</strong>loxacin. Pharmacotherapy2001;21(pt 2):S89-94.13. Priebe DL, Chambliss ML. Blood cultures not helpfulfor community-acquired pneumonia. J Fam Pract2003;52:599-600.14. Sopena N, Sabria-Leal M, Pedro-Botet ML, Padilla E,Dominguez J, Morera J, et al. Comparative study <strong>of</strong>the clinical presentation <strong>of</strong> Legionella pneumonia <strong>and</strong>other community-acquired pneumonias. Chest 1998;113:1195-200.15. Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA,Singer DE, et al. A prediction rule to identify low-riskpatients with community-acquired pneumonia. N EnglJ Med 1997;336:243-50.16. Fine MJ, Hough LJ, Medsger AR, Li YH, Ricci EM, SingerDE, et al. The hospital admission decision for patientswith community-acquired pneumonia. Results from the<strong>Pneumonia</strong> Patient Outcomes Research Team cohortstudy. Arch Intern Med 1997;157:36-44.17. Fine MJ, Pratt HM, Obrosky DS, Lave JR, McIntosh LJ,Singer DE, et al. Relation between length <strong>of</strong> hospitalstay <strong>and</strong> costs <strong>of</strong> care for patients with communityacquiredpneumonia. Am J Med 2000;109:378-85.18. Goss CH, Rubenfeld GD, Park DR, Sherbin VL, GoodmanMS, Root RK. Cost <strong>and</strong> incidence <strong>of</strong> socialcomorbidities in low-risk patients with communityacquiredpneumonia admitted to a public hospital.Chest 2003;124:2148-55.19. Hoe LK, Keang LT. Hospitalized low-risk communityacquiredpneumonia: outcome <strong>and</strong> potential for costsavings.Respirology 1999;4:307-9.20. Ruiz M, Ewig S, Marcos MA, Martinez JA, Arancibia F,Mensa J, et al. Etiology <strong>of</strong> community-acquired pneumonia:impact <strong>of</strong> age, comorbidity, <strong>and</strong> severity. AmJ Respir Crit Care Med 1999;160:397-405.21. Arnold FW, Ramirez JA, McDonald LC, Xia EL. Hospitalizationfor community-acquired pneumonia: the pneumoniaseverity index vs clinical judgment. Chest 2003;124:121-4.22. Roson B, Carratala J, Dorca J, Casanova A, ManresaF, Gudiol F. Etiology, reasons for hospitalization, riskclasses, <strong>and</strong> outcomes <strong>of</strong> community-acquired pneumoniain patients hospitalized on the basis <strong>of</strong> conventionaladmission criteria. Clin Infect Dis 2001;33:158-65.23. M<strong>and</strong>ell LA. <strong>Community</strong>-acquired pneumonia. Etiology,epidemiology, <strong>and</strong> treatment. Chest 1995;108(suppl):S35-42.24. M<strong>and</strong>ell LA. Antibiotic therapy for community-acquiredpneumonia. Clin Chest Med 1999;20:589-98.25. M<strong>and</strong>ell LA. Antimicrobial approaches to therapy forpneumonia. Curr Opin Pulm Med 1996;2:218-27.26. Mundy LM, Oldach D, Auwaerter PG, Gaydos CA,Moore RD, Bartlett JG, et al., for the Hopkins CAPteam. Implications for macrolide treatment in community-acquiredpneumonia. Chest 1998;113:1201-6.27. M<strong>and</strong>ell LA. Antibiotics for pneumonia therapy. MedClin North Am 1994;78:997-1014.28. M<strong>and</strong>ell LA, Marrie TJ, Grossman RF, Chow AW, Hyl<strong>and</strong>RH, for the Canadian <strong>Community</strong>-<strong>Acquired</strong> <strong>Pneumonia</strong>Working Group. Canadian guidelines for the initialmanagement <strong>of</strong> community-acquired pneumonia: anevidence-based update by the Canadian Infectious DiseasesSociety <strong>and</strong> the Canadian Thoracic Society. ClinInfect Dis 2000;31:383-421.29. Heffelfinger JD, Dowell SF, Jorgensen JH, Klugman KP,Mabry LR, Musher DM, et al. Management <strong>of</strong> community-acquiredpneumonia in the era <strong>of</strong> pneumococcalresistance: a report from the Drug-Resistant Streptococcuspneumoniae Working Group. Arch InternMed 2000;160:1399-408.30. M<strong>and</strong>ell LA, Bergeron MC, Gribble MJ, et al. Sequentialantibiotic therapy: effective cost management <strong>and</strong>patient care. Can J Infect Dis 1995;6:306.31. Kuti JL, Capitano B, Nicolau DP. Cost-effective approachesto the treatment <strong>of</strong> community-acquired pneumonia inthe era <strong>of</strong> resistance. Pharmacoeconomics 2002;20:513-28.32. Jones RN, Biedenbach DJ, Beach ML. Influence <strong>of</strong>patient age on the susceptibility patterns <strong>of</strong> Streptococcuspneumoniae isolates in North America (2000-2001):report from the SENTRY Antimicrobial Surveillance Program.Diagn Microbiol Infect Dis 2003;46:77-80.33. Begg EJ, Barclay ML, Kirkpatrick CM. The therapeuticmonitoring <strong>of</strong> antimicrobial agents. Br J Clin Pharmacol2001;52(suppl 1):S35–43.34. Milkovich G. Intravenous-to-oral transition therapy incommunity-acquired pneumonia: the INOVA Health Systemexperience. Pharmacotherapy 2001;21(pt 2):S83-8.35. Weingarten SR, Riedinger MS, Varis G, Noah MS, BelmanMJ, Meyer RD, et al. Identification <strong>of</strong> low-riskhospitalized patients with pneumonia. Implications forearly conversion to oral antimicrobial therapy. Chest1994;105:1109-15.36. Siegel RE, Halpern NA, Almen<strong>of</strong>f PL, Lee A, Cashin R,Greene JG. A prospective r<strong>and</strong>omized study <strong>of</strong> in-patientiv. antibiotics for community-acquired pneumonia. Theoptimal duration <strong>of</strong> therapy. Chest 1996;110:965-71.37. Ramirez JA, Vargas S, Ritter GW, Brier ME, Wright A,Smith S, et al. Early switch from intravenous to oralantibiotics <strong>and</strong> early hospital discharge: a prospectiveobservational study <strong>of</strong> 200 consecutive patients withcommunity-acquired pneumonia. Arch Intern Med1999;159:2449-54.38. C<strong>of</strong>fey RJ, Richards JS, Remmert CS, LeRoy SS, SchovilleRR, Baldwin PJ. An introduction to critical paths. QualManag Health Care 1992;1:45-54.39. Marrie TJ, Lau CY, Wheeler SL, Wong CJ, VanervoortMK, Feagan BG. A controlled trial <strong>of</strong> a critical pathwayfor treatment <strong>of</strong> community-acquired pneumonia.CAPITAL Study Investigators. <strong>Community</strong>-<strong>Acquired</strong><strong>Pneumonia</strong> Intervention Trial Assessing Lev<strong>of</strong>loxacin.JAMA 2000;283:749-55.450 American Family Physician www.aafp.org/afp Volume 73, Number 3 ◆ February 1, 2006