SYNDROME OF LESER-TRELAT: A CASE PRESENTATION
SYNDROME OF LESER-TRELAT: A CASE PRESENTATION
SYNDROME OF LESER-TRELAT: A CASE PRESENTATION

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
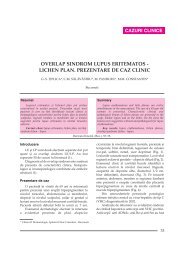
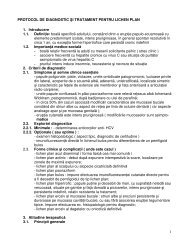
CAZURI CLINICE<strong>SYNDROME</strong> <strong>OF</strong> <strong>LESER</strong>-<strong>TRELAT</strong>: A <strong>CASE</strong> <strong>PRESENTATION</strong>CARMEN MARIA SÃLÃVÃSTRU*, MARIA MAGDALENA CONSTANTIN*, B. MATEESCU*,G.S. ÞIPLICA**BucharestSummaryRezumatThe abrupt onset of numerous seborrheic keratosesApariþia bruscã a numeroase keratoze seboreice(Leser-Trelat sign) can evolve in association with an (semnul Leser-Trélat) poate evolua în asociere cu o afecþiuneinternal malignancy (Leser-Trelat syndrome). A 65-yearoldman was seeking a dermatological consult for a pruritic de ani a solicitat consult dermatologic pentru o erupþiemalignã (sindromul Leser-Trélat). Un bãrbat în vârstã de 65eruption consisting in multiple seborrheic keratoses. The pruriginoasã constând din keratoze seboreice multiple.lesions had a precipitate onset and a rapid enlargement. The Leziunile apãruserã de scurt timp ºi se mãreau rapid îngastroscopy revealed a gastric carcinoma type Bormann III. dimensiuni. Examenul gastroscopic a decelat un carcinomEven if a strong physiopathological relation between Bormann de tip III. Deºi o legãturã fiziopatologicã întreseborrheic keratoses and internal malignancy is not yet keratozele seboreice ºi neoplaziile organelor interne nu a fostestablished, all patients with Leser-Trelat sign should be identificatã se recomandã ca pacienþii cu semnul Leserevaluatedfor occult neoplastic disease.Trélat sã fie evaluaþi pentru o eventualã neoplazie.Keywords: Leser-Trelat, seborrheic keratoses, gastricCuvinte cheie: laser-trelat, keratozã seboreicã,carcinoma.carcinom gastric.DermatoVenerol. (Buc.), 52: 89-91IntroductionNumerous dermatological changes can revealan underlying internal malignancy. In some casesthe association is well defined and accepted(pemphigus, dermatomyositis, acrokeratosis ofBazex etc.) while in other this correlation is poordefined and not unanimous accepted (chronicurticaria, erythema multiforme, acne, acanthosisnigricans etc.). The surgeons Dr. Edmund Leserand Dr. Ulysse Trelat were separately andconcomitantly searching to demonstrate thatcherry angiomas are linked to internalmalignancies. After 1900 their names wereassociated (by error or by extension) to theseborrheic keratoses eruption [1]. The Leser-Trelat sign is described as the sudden appearanceand rapid increase in size and number ofseborrheic keratoses [2]. In 2000 it was proposeda definition for the syndrome of Leser-Trelat as aparaneoplastic syndrome in patients with thesign of Leser-Trelat in whom an occultmalignancy was discovered after the appearanceof the sign [3]. It is difficult to demonstrate thevalidity of this association as it is described inelderly, where both the seborrheic keratoses andthe internal malignancies are not rare. A review ofthe literature [1] indicate that most frequent thesyndrome of Leser-Trelat is associated withadenocarcinomas (of the stomach and of thebreast) or with lymphomas.* „Carol “Carol Davila” University of Medicine and Pharmacy, Colentina Clinical Hospital.** Clinic of Gastroenterology.89
DermatoVenerol. (Buc.), 52: 89-91Case reportIn December 2002 a 65 year old man wasseeking a dermatological consult complaining ofa pruritic eruption disposed on his upper andlower back (photo 1). The clinical examinationrevealed sessile exophytic tumors of round orovalar aspect, with the diameter of 2 - 5 cm. Thelesion surface was verrucous and friable orsmooth, coloured brown-black respectivelybrown-red with numerous black keratotic plugs.On general examination epigastric tendernesswas present.The patient declared that the lesionsdeveloped rapidly, over a period of 6 months. Thepruritus was severe, interfering with dailyactivities and sleep. The patient complained ofthe rapid development of the lesions in the last 60days and of the pruritus intensification. He alsonoticed from 3 months an epigastric pain(burning type) that occurred after the meals. Thepatient was worried of a weight loss of 4 kgoccurred during the last month. He describednight sweats and a decreased appetite for thisperiod of time. The patient did not observedchanges in his stools. There was no family historyof similar lesions of seborrheic keratosis.Laboratory usual investigations showedhemoglobin of 11,5 g/dL, RBC 4,9 x 10 6 /µL, WBC5,8 x 10 3 /µL, PLT 180 x 10 3 /µL, ESR 16 mm/h. Allother values were in normal range.One small, new arise lesion was excised andthe dermatopathologic examination showed anacanthotic type of seborrheic keratosis (photo 2)with hyperkeratosis, papillomatosis and thickepidermis. Horny invaginations and horn cystswere also present. Large numbers of basaloidcells are present between the cysts.The patient was referred to the Gastroenterologydepartment for endoscopy. Anulcerative and infiltrative tumor (Bormann III)was identified on the lesser curve of the stomach(photo 3). An endoscopic biopsy specimen wasnot taken because of the risk of bleeding. Thepatient was then referred to the Oncologydepartment for further surgical treatment.Histopathology of the tumor was relevant foradenocarcinoma and confirmed the stadialisationas Bormann III (ulceration with invasion of thegastric wall).DiscusionThe existence of Leser-Trelat syndrome isunder debate and it is due to the high frequencyof seborrheic keratosis in elderly people. Theassociation of seborrheic keratosis with theinternal malignancy can be fortuite. APhoto 1. Seborrheic keratosis on the upper and lower backPhoto 2. Acanthotic type of seborrheic keratosis90
DermatoVenerol. (Buc.), 52: 89-91ConclusionsThe patients presenting the sign of Leser-Trelat should be careful investigated for theexistence of an occult malignancy. Physicalexamination, endoscopic investigation,radiologic and imaging studies (CT, MRI)should be performed by a medical teamincluding dermatologist, gastroenterologist,and oncologist.Intrat în redacþie: 11.09.2007Photo 3. Endoscopic view of the gastric carcinomaretrospective study concludes that the evidencefor a causal relation between eruptive seborrheickeratoses and cancer is meager [4]. There aresome case reports of patients with internalmalignancies and paraneoplastic acanthosisnigricans in which the role of transforminggrowth factor-a (TGF-a) acts as epidermal inducerof hyperplasia [5]. More recent observationssuggested that TGF-a produced by the internalmalignancy could be responsible for the acuteeruption of seborrheic keratosis [3]. In support ofthis theory is the observation that after theremoval of the internal neoplasm there is aregression of the seborrheic keratoses [3].Bibliography1 Schwartz R.A. Sign of Leser-Trelat, J Am AcadDermatol 1996; 35: 88-95.2 Flugman S.L, McClain S.A, Clark R.A.F. Transienteruptive seborrheic keratoses associated witherythrodermic psoriasis and erythrodermic drugeruption: Report of two cases, J Am Acad Dermatol2001; 45: S212-4.3 Heaphy Jr. M.R, Millns J.L., Schroeter A.L. The signof Leser-Trelat in a case of adenocarcinoma of thelung. J Am Acad Dermatol 2000; 43: 386-90.4 Rampen H.J. The sign of Leser-Trélat: does it exist?J Am Acad Dermatol. 1990 Jul; 23 (1): 151-35 J.S.M. Yeh, S..E Munn. Coexistence of acanthosisnigricans and the sign of Leser-Trelat in a patient withgastric adenocarcinoma: A case report and literaturereview. J Am Acad Dermatol 2000; 42: 357-62.91