Diabetes guidance 1766.pdf - East Cheshire NHS Trust
Diabetes guidance 1766.pdf - East Cheshire NHS Trust Diabetes guidance 1766.pdf - East Cheshire NHS Trust
Glycaemic Control in Type 2 DiabetesNon-Insulin therapyThe first line drug is metformin.• It should be prescribed in all appropriate patients as the standard release tablet with a usual maximumdaily dose of 2 grams in divided doses.• The modified release formulation should be offered if the patient is intolerant of the standard releaseformulation prior to trialling other classes of medication. See BNF.• Prescribe with caution if eGFR is
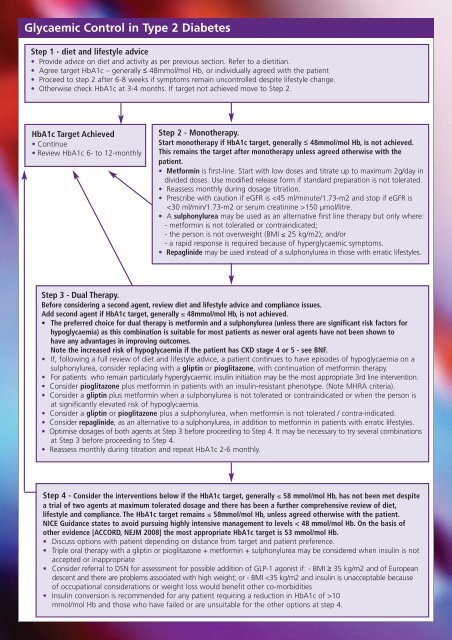
Glycaemic Control in Type 2 DiabetesStep 1 - diet and lifestyle advice• Provide advice on diet and activity as per previous section. Refer to a dietitian.• Agree target HbA1c – generally ≤ 48mmol/mol Hb, or individually agreed with the patient• Proceed to step 2 after 6-8 weeks if symptoms remain uncontrolled despite lifestyle change.• Otherwise check HbA1c at 3-4 months. If target not achieved move to Step 2.HbA1c Target Achieved• Continue• Review HbA1c 6- to 12-monthlyStep 2 - Monotherapy.Start monotherapy if HbA1c target, generally ≤ 48mmol/mol Hb, is not achieved.This remains the target after monotherapy unless agreed otherwise with thepatient.• Metformin is first-line. Start with low doses and titrate up to maximum 2g/day individed doses. Use modified release form if standard preparation is not tolerated.• Reassess monthly during dosage titration.• Prescribe with caution if eGFR is
- Page 1 and 2: Eastern CheshireVale RoyalSouth Che
- Page 3 and 4: The Newly Diagnosed Diabetic Patien
- Page 5 and 6: Glycaemic ControlHbA1c MeasurementH
- Page 7: Self-Monitoring of Blood Glucose -
- Page 11 and 12: Insulin therapy - continuedPatients
- Page 13 and 14: HypertensionBP targets are the same
- Page 15 and 16: Lipids - continuedHDL Cholesterol a
- Page 17 and 18: Screening for Diabetic NephropathyS
- Page 19 and 20: Active Foot DiseaseUlcerRefer to Sp
Glycaemic Control in Type 2 <strong>Diabetes</strong>Step 1 - diet and lifestyle advice• Provide advice on diet and activity as per previous section. Refer to a dietitian.• Agree target HbA1c – generally ≤ 48mmol/mol Hb, or individually agreed with the patient• Proceed to step 2 after 6-8 weeks if symptoms remain uncontrolled despite lifestyle change.• Otherwise check HbA1c at 3-4 months. If target not achieved move to Step 2.HbA1c Target Achieved• Continue• Review HbA1c 6- to 12-monthlyStep 2 - Monotherapy.Start monotherapy if HbA1c target, generally ≤ 48mmol/mol Hb, is not achieved.This remains the target after monotherapy unless agreed otherwise with thepatient.• Metformin is first-line. Start with low doses and titrate up to maximum 2g/day individed doses. Use modified release form if standard preparation is not tolerated.• Reassess monthly during dosage titration.• Prescribe with caution if eGFR is


