Table 1.1: MLFSA's financial resources allocated to drug-related social security programmes, 2008–2011Year:MDDSZ'sresourcesallocated to:Social rehabilitationprogrammes foraddicts (EUR)Therapeutic communityprogrammes and other programmesthat provide housing for drug users,together with associated <strong>net</strong>worksof reception and day centres,reintegration centres, programmesfor parallel therapeutic support forthe families of drug addicts, andother programmes for drug users oralternatives to therapeuticcommunities (EUR)Low-thresholdprogrammes for drugusers, <strong>net</strong>works ofcentres for counsellingand social rehabilitationof illicit drug addictswho need treatments orassistance every day(EUR)2011 3,213,519.002010 2,713,129.37* 1,575,993.26 587,876.522009 2,558,798.00* 1,514,458 544,492.502008 2,290,728.00* 1,445,691 399,013.40*This figure does not represent the sum of the amounts in the third and fourth column of the table, since, in addition to drugrelatedprogrammes, some other social security programmes (prevention programmes, programmes dealing with alcoholismand other forms of addiction as well as eating disorders) are funded with resources from the “Social rehabilitation programmesfor addicts” budget lineSource: Report of the Ministry of Labour, Family and Social Affairs of the RS 220The Ministry of Public Administration issued a public tender for the implementation ofEuropean Cohesion Policy projects for the period 2010–2012, and selected two substantive<strong>net</strong>works of non-governmental organizations. The Institute for Research and DevelopmentUtrip received EUR 160,000.00 for the establishment of a prevention platform of NGOsworking in the field of addiction prevention. The DrogArt Association received EUR156,426.00 for the project of empowerment of NGOs working in the field of harm reduction.The purpose of public co-funding is to promote the development of the non-governmentalsector and the civil dialogue in relevant thematic areas. Financial resources were allocatedfor the implementation of all activities carried out over the mentioned two-year period, andare not included in the summary tables in this year's financial report.The Slovenian Criminal Police uses more than half a million Euros each year in its fightagainst organized crime. Data show that financial resources used for the implementation ofcovert investigative measures and technical equipment amounted to EUR 657,254.05 in2011, whereas a year before they amounted to EUR 576,040.00. A large part of theseresources is allocated to the fight against illicit drugs. Since information on such resourcesoften refer to a number of different offences, we cannot present accurate data on theamounts of financial resources allocated to the field of illicit drugs.The Health Insurance Institute of Slovenia provided EUR 5,623,535.27 for the operation ofcentres for the prevention and treatment of drug addiction in 2011. EUR 2,709,098.00 wasspent on operational costs (personnel, facilities, etc.), and EUR 2,914,437.27 on substitutedrugs (methadone and other drugs).2 Available from the author. Received via e-mail. The report is not publicly available yet
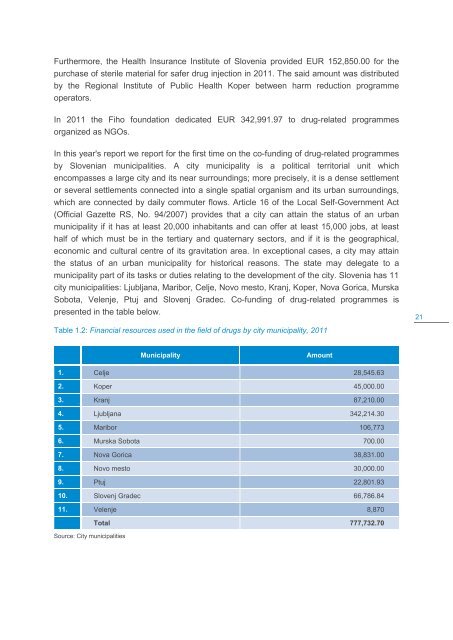
Furthermore, the Health Insurance Institute of Slovenia provided EUR 152,850.00 for thepurchase of sterile material for safer drug injection in 2011. The said amount was distributedby the Regional Institute of Public Health Koper between harm reduction programmeoperators.In 2011 the Fiho foundation dedicated EUR 342,991.97 to drug-related programmesorganized as NGOs.In this year's report we report for the first time on the co-funding of drug-related programmesby Slovenian municipalities. A city municipality is a political territorial unit whichencompasses a large city and its near surroundings; more precisely, it is a dense settlementor several settlements connected into a single spatial organism and its urban surroundings,which are connected by daily commuter flows. Article 16 of the Local Self-Government Act(Official Gazette RS, No. 94/2007) provides that a city can attain the status of an urbanmunicipality if it has at least 20,000 inhabitants and can offer at least 15,000 jobs, at leasthalf of which must be in the tertiary and quaternary sectors, and if it is the geographical,economic and cultural centre of its gravitation area. In exceptional cases, a city may attainthe status of an urban municipality for historical reasons. The state may delegate to amunicipality part of its tasks or duties relating to the development of the city. Slovenia has 11city municipalities: Ljubljana, Maribor, Celje, Novo mesto, Kranj, Koper, Nova Gorica, MurskaSobota, Velenje, Ptuj and Slovenj Gradec. Co-funding of drug-related programmes ispresented in the table below.21Table 1.2: Financial resources used in the field of drugs by city municipality, 2011MunicipalityAmount1. Celje 28,545.632. Koper 45,000.003. Kranj 87,210.004. Ljubljana 342,214.305. Maribor 106,7736. Murska Sobota 700.007. Nova Gorica 38,831.008. Novo mesto 30,000.009. Ptuj 22,801.9310. Slovenj Gradec 66,786.8411. Velenje 8,870Total 777,732.70Source: City municipalities
- Page 3 and 4: 2012 NATIONAL REPORT (2011 data) TO
- Page 7 and 8: SUMMARYChapter 1Amendments to the C
- Page 9 and 10: parents, girls with associated prob
- Page 11 and 12: elated social security programmes,
- Page 13 and 14: Chapter 12Slovenia's gross domestic
- Page 15 and 16: DRUG POLICY: LEGISLATION, STRATEGIE
- Page 17 and 18: part of an addiction treatment prog
- Page 19: In addition to coordination, the In
- Page 23 and 24: The declaration also highlights the
- Page 25: DRUG USE IN THE GENERAL POPULATION
- Page 31 and 32: Age group comparison shows that the
- Page 33 and 34: Field procedureData collection was
- Page 35 and 36: Table 2.5: Lifetime use of illicit
- Page 37 and 38: The fact that data on the prevalenc
- Page 39 and 40: Observational visits in night venue
- Page 41 and 42: Customer intoxication and incidents
- Page 43 and 44: Focus groups of high-school student
- Page 45 and 46: Figure 3.1: Excise duty per hl of e
- Page 47 and 48: Some tobacco control measures in Sl
- Page 49 and 50: data on the sale of these products,
- Page 51 and 52: individual to have an (imparted) se
- Page 53 and 54: Co-creating community responses in
- Page 55 and 56: As regards the intention of student
- Page 57 and 58: according to the usual schedule dur
- Page 59 and 60: Community-based preventionAnalysis
- Page 61 and 62: programme carried out in the USA an
- Page 63 and 64: They also plan to conduct workshops
- Page 65 and 66: PROBLEM DRUG USE4.‘Problem drug u
- Page 67 and 68: (with their grandmother, brother, i
- Page 69 and 70: Almost two thirds of those who inje
- Page 71 and 72:
DRUG RELATED TREATMENT: TREATMENT D
- Page 73 and 74:
Social protectionProfessional activ
- Page 75 and 76:
5.2 Access to treatmentIn Slovenia,
- Page 77 and 78:
Figure 5.2: Number of programme use
- Page 79 and 80:
42.9% of drug users who re-entered
- Page 81 and 82:
used opiates once a week, 12 (13.5%
- Page 83 and 84:
The main reason for first-time admi
- Page 85 and 86:
survey results, which show that onl
- Page 87 and 88:
Correlation between first-time admi
- Page 89 and 90:
hepatitis B free of charge in CPTDA
- Page 91 and 92:
The proportion of drug users who ha
- Page 93 and 94:
Trends in the proportion of users w
- Page 95 and 96:
2. The decrease in the proportion o
- Page 97 and 98:
HEALTH CORRELATES AND CONSEQUENCES6
- Page 99 and 100:
on the prevalence of infections tha
- Page 101 and 102:
6.2 Other drug-related health corre
- Page 103 and 104:
Table 6.3 shows the number of illic
- Page 105 and 106:
In conclusion, we can say that emer
- Page 107 and 108:
In all observed years, the number o
- Page 109 and 110:
Figure 6.4: Trends in the number of
- Page 111 and 112:
The Obalno-kraška and the Zasavska
- Page 113 and 114:
Cohort studyMortalityOnly drug user
- Page 115 and 116:
CPTDAs covering the three largest S
- Page 117 and 118:
drug users had been treated in othe
- Page 119 and 120:
Violent deaths (V01.0 - Y98.9, F11.
- Page 121 and 122:
and benzodiazepines. Three quarters
- Page 123 and 124:
life than deaths of their peers (th
- Page 125 and 126:
RESPONSES TO HEALTH CORRELATES ANDC
- Page 127 and 128:
Low-threshold programmes include fr
- Page 129 and 130:
8.1 Social exclusion and drug useTa
- Page 131 and 132:
Table 8.2: Users and capacities in
- Page 133 and 134:
9.1 Drug-related crimeStaša Šavel
- Page 135 and 136:
Secondary crimeCompared to 2010, th
- Page 137 and 138:
9.2 Prevention of drug-related crim
- Page 139 and 140:
Table 9.7: Number of persons having
- Page 141 and 142:
Patients take substitute medicine u
- Page 143 and 144:
information required for solving pr
- Page 145 and 146:
groups from other countries. Most o
- Page 147 and 148:
Table 10.1: Total amounts of seized
- Page 149 and 150:
10.3 Quality and purity of illicit
- Page 151 and 152:
CannabisThe most common type of can
- Page 153 and 154:
amounts of active components and ad
- Page 155 and 156:
Data on the purity of various illic
- Page 157 and 158:
RESIDENTIAL TREATMENT OF DRUG-USERS
- Page 159 and 160:
Photo 11.1: The old school which wa
- Page 161 and 162:
(source: Terapevtska skupnost Cenac
- Page 163 and 164:
social assistance networks is of hi
- Page 165 and 166:
schedules and through work therapy,
- Page 167 and 168:
provides drug users with medical ca
- Page 169 and 170:
programme, and draw up a report on
- Page 171 and 172:
It seems that we will have to devot
- Page 173 and 174:
Despite the absence of radical meas
- Page 175 and 176:
Purpose Funder YearAmount(EUR)Cofog
- Page 177 and 178:
that co-funding is relatively stabl
- Page 179 and 180:
Table 12.2: Drug-related expenditur
- Page 181 and 182:
12.5 ConclusionsBy 2011, the effect
- Page 183 and 184:
BIBLIOGRAPHYList of referencesAnder
- Page 185 and 186:
Klavs I, Poljak M. (2003) Unlinked
- Page 187 and 188:
SURS. (2011) Oddelek za cene življ
- Page 189 and 190:
OECD. (2012a) Country Statistical p
- Page 191 and 192:
Zakon o omejevanju porabe alkohola
- Page 193 and 194:
Table 8.2: Users and capacities in
- Page 195 and 196:
Figure 5.12: Number of first-time a