Specialist Palliative Care Referral Form - St Christopher's Hospice
Specialist Palliative Care Referral Form - St Christopher's Hospice
Specialist Palliative Care Referral Form - St Christopher's Hospice
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
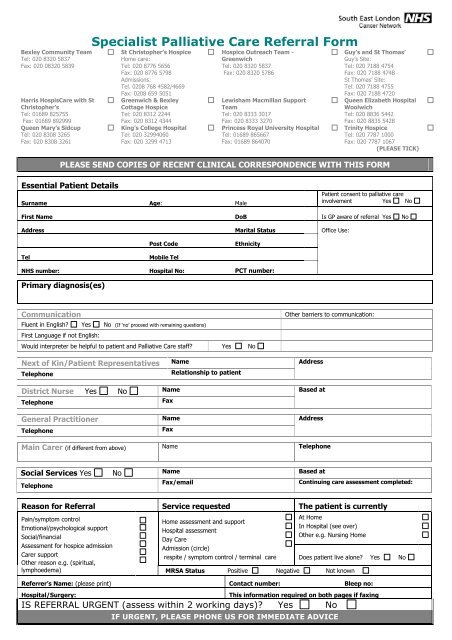
Bexley Community TeamTel: 020 8320 5837Fax: 020 08320 5839Harris Hospis<strong>Care</strong> with <strong>St</strong>Christopher’sTel: 01689 825755Fax: 01689 892999Queen Mary’s SidcupTel: 020 8308 3265Fax: 020 8308 3261<strong>Specialist</strong> <strong>Palliative</strong> <strong>Care</strong> <strong>Referral</strong> <strong>Form</strong><strong>St</strong> Christopher’s <strong>Hospice</strong>Home care:Tel: 020 8776 5656Fax: 020 8776 5798Admissions:Tel. 0208 768 4582/4669Fax: 0208 659 5051Greenwich & BexleyCottage <strong>Hospice</strong>Tel: 020 8312 2244Fax: 020 8312 4344King’s College HospitalTel: 020 32994060Fax: 020 3299 4713<strong>Hospice</strong> Outreach Team -GreenwichTel: 020 8320 5837Fax: 020 8320 5786Lewisham Macmillan SupportTeamTel: 020 8333 3017Fax: 020 8333 3270Princess Royal University HospitalTel: 01689 865667Fax: 01689 864070Guy’s and <strong>St</strong> Thomas’Guy’s Site:Tel: 020 7188 4754Fax: 020 7188 4748<strong>St</strong> Thomas’ Site:Tel: 020 7188 4755Fax: 020 7188 4720Queen Elizabeth HospitalWoolwichTel: 020 8836 5442Fax: 020 8835 5428Trinity <strong>Hospice</strong>Tel: 020 7787 1000Fax: 020 7787 1067(PLEASE TICK)PLEASE SEND COPIES OF RECENT CLINICAL CORRESPONDENCE WITH THIS FORMEssential Patient DetailsSurname Age: MalePatient consent to palliative careinvolvement Yes NoFirst Name DoB Is GP aware of referral Yes NoAddress Marital <strong>St</strong>atus Office Use:Post CodeEthnicityTelMobile TelNHS number: Hospital No: PCT number:Primary diagnosis(es)CommunicationFluent in English? Yes No (If ‘no’ proceed with remaining questions)First Language if not English:Would interpreter be helpful to patient and <strong>Palliative</strong> <strong>Care</strong> staff? Yes NoOther barriers to communication:Next of Kin/Patient Representatives Name AddressTelephoneRelationship to patientDistrict Nurse Yes No Name Based atTelephoneFaxGeneral Practitioner Name AddressTelephoneFaxMain <strong>Care</strong>r (if different from above) Name TelephoneSocial Services Yes No Name Based atTelephoneFax/emailContinuing care assessment completed:Reason for <strong>Referral</strong> Service requested The patient is currentlyPain/symptom controlEmotional/psychological supportSocial/financialAssessment for hospice admission<strong>Care</strong>r supportOther reason e.g. (spiritual,lymphoedema)Home assessment and supportHospital assessmentDay <strong>Care</strong>Admission (circle)respite / symptom control / terminal careAt HomeIn Hospital (see over)Other e.g. Nursing HomeDoes patient live alone? Yes NoMRSA <strong>St</strong>atus Positive Negative Not knownReferrer’s Name: (please print) Contact number: Bleep no:Hospital/Surgery:This information required on both pages if faxingIS REFERRAL URGENT (assess within 2 working days)? Yes NoIF URGENT, PLEASE PHONE US FOR IMMEDIATE ADVICE
<strong>Specialist</strong> <strong>Palliative</strong> <strong>Care</strong> <strong>Referral</strong> <strong>Form</strong>PATIENT NAME ……………………………………………In-Patient detailsHospitalTelephoneWard Direct Ward Ext. Date of discharge (if known)Consultant Is <strong>Palliative</strong> <strong>Care</strong> team involved? Yes NoBrief History of diagnosis(es) and Key treatmentsDate Progression of disease and investigations/treatment Consultant and hospitalCurrent problems (including psychosocial or spiritual issues)1. 4.2. 5.3. Patient Mobility:Any other comments/informationReferrer’s expectation of current treatment Symptom controlEstimated prognosis daysInsightHas patient been told diagnosis? Yes No Is the carer aware of patient’s diagnosis? Yes NoDoes patient discuss the illness freely Yes No Has resuscitation been discussed? Yes NoPast Medical and PsychiatricHistoryCurrent MedicationKnown Drug Sensitivities/Allergies:Yes NoDetails:Please ensure patients are aware information will be held on computer according to the Data Protection Act.Referrer’s signature:Name: (please print)Job title: Contact number: Bleep no:Surgery or Hospital:Date:Revised South East London Cancer Network April 2010