

Medical History Questionnaire
Medical History Questionnaire
Medical History Questionnaire
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
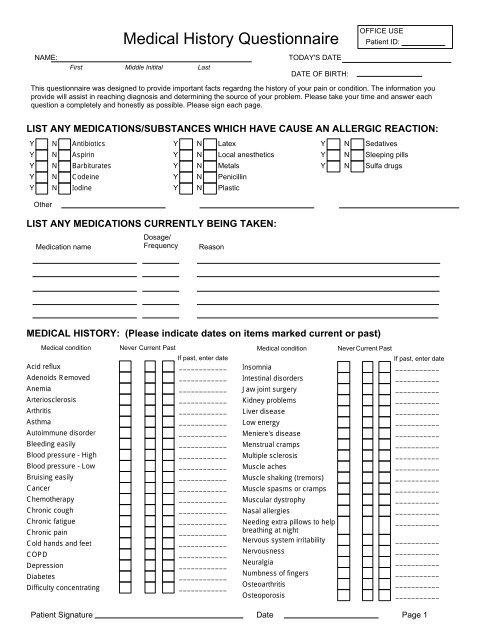
<strong>Medical</strong> condition Never Current PastIf past, enter dateDifficulty sleeping____________Dizziness____________Emphysema____________Epilepsy____________Excessive thirst____________Fibromyalgia____________Fluid retention____________Frequent cough____________Frequent illnesses____________Frequent stressful situations____________General anesthesia____________Glaucoma____________Gout____________Hay fever____________Hearing impaired____________Heart attack____________Heart disorder____________Heart murmur____________Heart pacemaker____________Heart palpitations____________Heart valve replacement____________Hemophilia____________Hepatitis____________Hypertension____________Hypoglycemia____________Immune system disorder____________Injury to face____________Injury to mouth____________Injury to neck____________Injury to teeth____________Ovarian cystsParkinson's diseasePoor circulationPrior orthodontic treatmentPsychiatric careRadiation treatmentRheumatic feverRheumatoid arthritisScarlet feverScoliosisShortness of breathSinus problemsSkin disorderSleep apneaSlow healing soresSpeech difficultiesStrokeSwelling in ankles or feetSwollen, stiff or painful jointsTendency for ear infectionsTendency for frequent coldsTendency for sore throatsThyroid disorderTired musclesTonsils RemovedTuberculosisTumors<strong>Medical</strong> conditionUrinary disordersWisdom teeth (third molar)extractionNever Current PastIf past, enter date_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Current Past If past, enter date Current PastOther ______________________ ______________ _______________________ ______________________________________ ______________ _________________________ ______________________________________ ______________ _________________________ __________ADDITIONAL MEDICAL HISTORY ITEMS:Never Past Never PastCurrent If past, enter dateCurrent If past, enter dateRecreational drugs____________HIV/AIDS____________LIST ANY SURGICAL OPERATIONS YOU HAVE HAD:Y N AppendectomyY N HeartY N BackY N Hernia repairY N EarY N LungY N GallbladderY N NasalY N ThyroidY N TonsillectomyY N UvulectomyY N PeriodontalOtherPatient Signature Date Page 2
FAMILY HISTORYHas any member of you family had (parent, sibling or grandparent):Y N CancerY N Heart diseaseY N DiabetesY N High blood pressureOtherSOCIAL HISTORY:Y N StrokeY N Sleep disorderY N ObesityY N Thyroid troubleY N Father snoresY N Mother snoresY N Father has sleep apneaY N Mother has sleep apneaTobacco Use:CigarettesNever smokedCurrent smokerQuit# packs per dayWhen did you quit?# of yearsOther tobacco: Pipe Snuff CigarChewAlcohol Use:Do you drink alcohol?YesNoIf yes, # of drinks per week:Caffeine Intake: None Coffee/Tea/Soda # cups per day:Additional:Y N Regular exercise Y NI authorize the release of a full report of examination findings, diagnosis, treatment program etc., to any referring or tratingdentist or physician. I additionally authorize the release of any medical information to insurance companies or for legaldocumentation to process claims. I understand that I am responsible for all charges for treatment to me regardless of insurancecoverage.Patient SignatureDateI certify that the medical history information is complete and accurate.Patient SignatureDatePatient Signature Date Page 3

