- Page 2 and 3:
PERFORMANCE-BASED SEISMIC DESIGNCON
- Page 4 and 5:
CONTENTSTable of Contents..........
- Page 6 and 7:
REAL-TIME DYNAMIC HYBRID TESTING OF
- Page 8 and 9:
PREFACEThe workshop on “Seismic D
- Page 10 and 11:
LIST OF PARTICIPANTSSergio M. Alcoc
- Page 12 and 13:
RESOLUTIONSThe International Worksh
- Page 14 and 15:
CONCLUSIONS AND RECOMMENDATIONSThe
- Page 16 and 17:
nonlinear dynamic) and when they sh
- Page 18 and 19:
exists to develop testing protocols
- Page 20 and 21:
to be sent soon to the 28 members o
- Page 22 and 23:
factor γ I is 1.4 or 1.2 for essen
- Page 24 and 25:
i. The well-known relation µ θ -
- Page 26 and 27:
γ s =1.15. Values less than 1.0 me
- Page 28 and 29:
efore (factor α in Eq.(4)). Materi
- Page 30 and 31:
the force demand from the analysis,
- Page 32 and 33:
OVERVIEW OF A COMPREHENSIVE FRAMEWO
- Page 34 and 35:
ground motion Intensity Measure (IM
- Page 36 and 37:
2.2 Simulation of Engineering Deman
- Page 38 and 39:
describing the economic losses asso
- Page 40 and 41:
practice the localized gravity load
- Page 42 and 43:
Whereas financial and insurance org
- Page 44 and 45:
AN OUTLINE OF AIJ GUIDELINES FOR PE
- Page 46 and 47:
(7) a method of performance evaluat
- Page 48 and 49:
where, T: natural period of structu
- Page 50 and 51:
6. DAMAGE AND LIMIT DEFORMATIONSThe
- Page 52 and 53:
The limit inter-story deformations
- Page 54 and 55:
DirectionX-directionY-directionSkew
- Page 56 and 57:
HAZARD, GROUND MOTIONS AND PROBABIL
- Page 58 and 59:
of events with [X1>x 1 , X 2 >x 2 ,
- Page 60 and 61:
2.4 Option C: Sufficient IMs: Estim
- Page 62 and 63:
predictions and hence required samp
- Page 64 and 65:
PEER has put forward PBSA methodolo
- Page 66 and 67:
3.2.1 A DCF Displacement-Based Form
- Page 68 and 69:
parameter k (the slope of the hazar
- Page 70 and 71:
POST-EARTHQUAKE FUNCTION OF HIGHWAY
- Page 72 and 73:
ln( EDP) a b ln ( IM )= + (1)Probab
- Page 74 and 75:
terms of global and local bridge pe
- Page 76 and 77:
Figure 3. Bridge column component d
- Page 78 and 79:
5.2 Method B: MDOF Residual Displac
- Page 80 and 81:
calculated using a 2 dimensional mu
- Page 82 and 83:
MODELING CONSIDERATIONS IN PROBABIL
- Page 84 and 85:
location. Transverse reinforcement
- Page 86 and 87:
2.50.1000Spectral Accel. (g)2.01.51
- Page 88 and 89:
Results indicate that 33% of the re
- Page 90 and 91:
4.1.2 Elastic vs. Inelastic ModelsF
- Page 92 and 93:
The increased dispersion leads to h
- Page 94 and 95:
AN ANALYSIS ON THE SEISMIC PERFORMA
- Page 96 and 97:
The survey stood on the condition t
- Page 98 and 99:
who decide the design force levels
- Page 100 and 101:
It is interesting to clarify whethe
- Page 102 and 103:
concluded that the dependence of in
- Page 104 and 105:
Table 10. Problems of performance-b
- Page 106 and 107:
DEVELOPMENT OF NEXT-GENERATION PERF
- Page 108 and 109:
ground shaking hazard, probable str
- Page 110 and 111:
Vulnerability of buildings to losse
- Page 112 and 113:
Peak Interstory Drfit Ratio0.120.10
- Page 114 and 115:
Conditional Probability ofDamage St
- Page 116 and 117:
Probability of Non-Exceedance10.80.
- Page 118 and 119:
APPLICATIONS OF PERFORMANCE-BASED E
- Page 120 and 121:
PRACTICAL ADAPTATION FOR STAKEHOLDE
- Page 122 and 123:
cost premium for the more expensive
- Page 124 and 125:
The future techniques will improve
- Page 126 and 127:
Benefit-cost ratio(BCR) 2.5UC Berke
- Page 128 and 129:
motivation to change the way they w
- Page 130 and 131: CHANGING THE PARADIGM FOR PERFORMAN
- Page 132 and 133: Ideally, the preliminary design of
- Page 134 and 135: ModelM1M2M3Table 1. Description of
- Page 136 and 137: Sample results from the response-hi
- Page 138 and 139: In FEMA 273/356, the intersection o
- Page 140 and 141: (M8 and M9) and the isolated frames
- Page 142 and 143: THE ATC-58 PROJECT PLAN FOR NONSTRU
- Page 144 and 145: The development of next-generation
- Page 146 and 147: for these flexible nonstructural co
- Page 148 and 149: spectra is several times larger tha
- Page 150 and 151: The variability is associated with
- Page 152 and 153: functions for a wide variety of non
- Page 154 and 155: SIMPLIFIED PBEE TO ESTIMATE ECONOMI
- Page 156 and 157: One can show (Porter et al. 2004) t
- Page 158 and 159: ( )FDM| EDP= xdm = 1 −FRdm , + 1,
- Page 160 and 161: 1. Facility definition. Same as in
- Page 162 and 163: Table 1. Approximation of seismic r
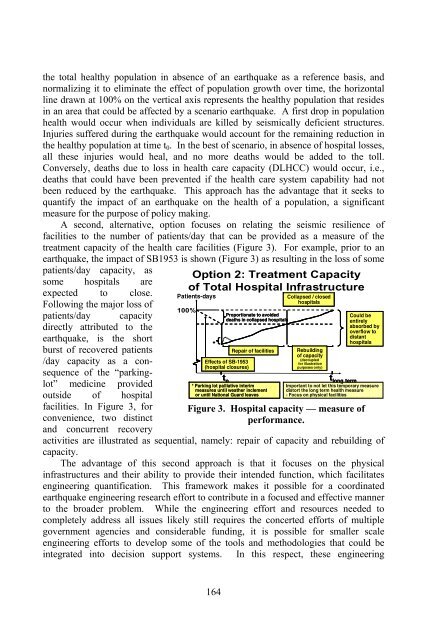
- Page 164 and 165: The EAL values shown in Figure 3 mi
- Page 166 and 167: ASSESSMENT OF SEISMIC PERFORMANCE I
- Page 168 and 169: where e -λτ is the discounted fac
- Page 170 and 171: IDR 3[rad]σPFAIDR34(g)σ PFA4media
- Page 172 and 173: Figure 3a, shows an example of frag
- Page 174 and 175: P(C LVCC i |IM )1.00.80.60.40.20.00
- Page 176 and 177: E [ L T | IM ]$ 10 M$ 8 M$ 6 M$ 4 M
- Page 178 and 179: SEISMIC RESILIENCE OF COMMUNITIES
- Page 182 and 183: quantification tools could be used
- Page 184 and 185: structure remains elastic. This is
- Page 186 and 187: of Figure 7a will be used. It is as
- Page 188 and 189: Nigg, J. M. (1998). Empirical findi
- Page 190 and 191: acceleration with a 475-year return
- Page 192 and 193: limit states, the suggestions given
- Page 194 and 195: ∆NSLsi= SϑH(5)iTFor column-sway
- Page 196 and 197: Pinto et al., 2004). The probabilit
- Page 198 and 199: The main difficulty in assigning a
- Page 200 and 201: Crowley, H., R. Pinho, and J. J. Bo
- Page 202 and 203: analytical models generally have si
- Page 204 and 205: Figure 2. Structure of the response
- Page 206 and 207: can be used as a random variable of
- Page 208 and 209: 4. DERIVATION OF THE VULNERABILITY
- Page 210 and 211: 5. CONCLUSIONSDerivation of vulnera
- Page 212 and 213: REFERENCESAbrams, D. P., A. S. Elna
- Page 214 and 215: In general, these types of bench-mo
- Page 216 and 217: where & x&(t ) = acceleration at th
- Page 218 and 219: science building. The lateral load-
- Page 220 and 221: emain the same, the magnitude of sl
- Page 222 and 223: of sliding thresholds, are desirabl
- Page 224 and 225: Retrofit of Nonstructural Component
- Page 226 and 227: was developed to accommodate these
- Page 228 and 229: tested by Meinheit and Jirsa are us
- Page 230 and 231:
where D is the maximum drift and N
- Page 232 and 233:
in predicting damage as well as rep
- Page 234 and 235:
4.2.2 Modeling the Data Using Stand
- Page 236 and 237:
that the defining demand using a no
- Page 238 and 239:
• The influence on the dynamic re
- Page 240 and 241:
deviations σ and correlation coeff
- Page 242 and 243:
The first three modes of vibration
- Page 244 and 245:
Details about the ten records selec
- Page 246 and 247:
to allow a quantitative assessment
- Page 248 and 249:
Cornell A. C., F. Jalayer, R. Hambu
- Page 250 and 251:
limited possibilities of overcoming
- Page 252 and 253:
uildings, up to five stories high (
- Page 254 and 255:
Efficiency η, %100806040203D-RWBW-
- Page 256 and 257:
Table 1. Performance criteria for c
- Page 258 and 259:
Because the analytical model strong
- Page 260 and 261:
REFERENCESAguilar, G., R. Meli, R.
- Page 262 and 263:
tests of its type ever conducted. T
- Page 264 and 265:
end work-point to work-point). And
- Page 266 and 267:
Fig. 5 shows the actual application
- Page 268 and 269:
3Roof Disp. (mm)250200150100500-50-
- Page 270 and 271:
Base Shear (kN)Base Shear (kN)40002
- Page 272 and 273:
8. CONCLUSIONSBased on the test and
- Page 274 and 275:
REAL-TIME DYNAMIC HYBRID TESTING OF
- Page 276 and 277:
:::::2004) can be formulated using
- Page 278 and 279:
The structure to be simulated is di
- Page 280 and 281:
measurements, to the modeling of th
- Page 282 and 283:
Figure 8. Two stories (left) and hy
- Page 284 and 285:
ROLES OF LARGE-SCALE TEST FOR ASSES
- Page 286 and 287:
mid-height in the third story, at w
- Page 288 and 289:
cycles were repeated for each ampli
- Page 290 and 291:
the tests with ALC panels were excl
- Page 292 and 293:
the relationship between the moment
- Page 294 and 295:
attachment details adopted for inst
- Page 296 and 297:
FULL-SCALE LABORATORY TESTING: STRA
- Page 298 and 299:
economic losses resulting from the
- Page 300 and 301:
4. OBJECTIVES AND OUTCOME OF STRUCT
- Page 302 and 303:
15001000500Shear [kN]0-8.0 -6.0 -4.
- Page 304 and 305:
5.1 3D Tests on a Torsionally Unbal
- Page 306 and 307:
Non-linear substructuring was recen
- Page 308 and 309:
PERFORMANCE BASED ASSESSMENT — FR
- Page 310 and 311:
4 x 50 m = 200 mC1 C2 C3h u = 7 mh
- Page 312 and 313:
some procedures are (contrary to th
- Page 314 and 315:
5 th floor disp. [cm]0.60.0-0.6CC =
- Page 316 and 317:
While the global drift of the build
- Page 318 and 319:
the use of such connections in eart
- Page 320 and 321:
I d = 0.25elastic limitmaximum resi
- Page 322 and 323:
As regards the influence of differe
- Page 324 and 325:
ON GROUND MOTION DURATION AND ENGIN
- Page 326 and 327:
time between the first and last acc
- Page 328 and 329:
FyFyFyFFFkk0.03kδδδcover a large
- Page 330 and 331:
T5b, T13a, T13b, T20a and T20b can
- Page 332 and 333:
Tabled results show that in the cas
- Page 334 and 335:
0 0.25 0.5 0.75 1Dkin PfSa[g]0 0.25
- Page 336 and 337:
ON DRIFT LIMITS ASSOCIATED WITH DIF
- Page 338 and 339:
BehaviourElasticInelasticCollapseDa
- Page 340 and 341:
Other factors such as the applied l
- Page 342 and 343:
4. MOMENT RESISTING FRAMES4.1 Ducti
- Page 344 and 345:
5Ductility factor432100 0.2 0.4 0.6
- Page 346 and 347:
5.1 Flexural Structural WallsAn exa
- Page 348 and 349:
MODAL PUSHOVER ANALYSIS: SYMMETRIC-
- Page 350 and 351:
Floor963SeattleNonlinear RHAFEMA1st
- Page 352 and 353:
The peak modal demands r n are then
- Page 354 and 355:
9BostonSeattleLos AngelesFloor63RSA
- Page 356 and 357:
5. EVALUATION OF MPA: UNSYMMETRIC-P
- Page 358 and 359:
Without additional conceptual compl
- Page 360 and 361:
AN IMPROVED PUSHOVER PROCEDURE FOR
- Page 362 and 363:
for a response governed by the fund
- Page 364 and 365:
2.2 Modal ScalingThe principal aim
- Page 366 and 367:
2.3 Pushover-History AnalysisSubsti
- Page 368 and 369:
(3) Calculate cumulative scale fact
- Page 370 and 371:
46.4 58 58 58 58 58 58 58 58 58 58
- Page 372 and 373:
EXTENSIONS OF THE N2 METHOD — ASY
- Page 374 and 375:
The strength reduction factor due t
- Page 376 and 377:
The relations apply to SDOF systems
- Page 378 and 379:
in X-direction pushover curves prac
- Page 380 and 381:
As an example, an idealized force-d
- Page 382 and 383:
The IN2 curve can be used in the pr
- Page 384 and 385:
HORIZONTALLY IRREGULAR STRUCTURES:
- Page 386 and 387:
Dutta and Das (2002, 2002b and refs
- Page 388 and 389:
They tested the procedure on three
- Page 390 and 391:
Table 1. Properties of the 4 WallsW
- Page 392 and 393:
The following is a summary of two s
- Page 394 and 395:
ectangular concrete deck supported
- Page 396 and 397:
REFERENCESAlmazan, J. L., and J. C.
- Page 398 and 399:
Rosenblueth, E. (1957). “Consider
- Page 400 and 401:
instantaneous period of vibration a
- Page 402 and 403:
value of the maximum plastic deform
- Page 404 and 405:
(a) elastic-perfectly plastic type(
- Page 406 and 407:
where a is the constant peculiar to
- Page 408 and 409:
Referring to Eq. (15), the natural
- Page 410 and 411:
-The effective period obtained by u
- Page 412 and 413:
eal damage data, rather than theore
- Page 414 and 415:
liquefaction-induced damage. This i
- Page 416 and 417:
Figure 5. Selected damage distribut
- Page 418 and 419:
Figure 6. Idealized capacity spectr
- Page 420 and 421:
I’ for the ductile case, as expec
- Page 422 and 423:
This study has shown that a modific
- Page 424 and 425:
thickness of the inner wall is usua
- Page 426 and 427:
4. EARTHQUAKE GROUND MOTION INPUT A
- Page 428 and 429:
5.2 Performance Levels and Limit St
- Page 430 and 431:
where λ I jis the occurrence rate
- Page 432 and 433:
intensity VI because the number of
- Page 434 and 435:
and thus are not considered in seis
- Page 436 and 437:
The values of the displacement modi
- Page 438 and 439:
constant amplitude loading (CA) or
- Page 440 and 441:
deterioration. These are the type o
- Page 442 and 443:
members, is the main feature of the
- Page 444 and 445:
RESULTS, DISCUSSIONS AND CONCLUSION
- Page 446 and 447:
systems, where FEMA estimations are
- Page 448 and 449:
The case study is a Hospital in the
- Page 450 and 451:
Table 1. Dimensions and amount of r
- Page 452 and 453:
4.2 Incremental AnalysisBase shear
- Page 454 and 455:
When adding jackets to columns, the
- Page 456 and 457:
storyShear in interior Column [ton]
- Page 458 and 459:
PERFORMANCE-BASED SEISMIC ASSESSMEN
- Page 460 and 461:
2. HYBRID FRAME BUILDINGSTwo precas
- Page 462 and 463:
15’ - 0” 15’ - 0”Hybrid fra
- Page 464 and 465:
and maximum residual inter-story fr
- Page 466 and 467:
As the first step in understanding
- Page 468 and 469:
Table 3. Comparison of calculated m
- Page 470 and 471:
NEW MODEL FOR PERFORMANCE BASED DES
- Page 472 and 473:
(a) interior beam-column joint(b) k
- Page 474 and 475:
yxVN =VADjDBABLD jDOV cOVCN= VLV bV
- Page 476 and 477:
3.3.2 B-modeThe equilibrium conditi
- Page 478 and 479:
3.6 Failure ModeBased on the calcul
- Page 480 and 481:
Name ofSpecimenTable 2. Comparison
- Page 482 and 483:
EARTHQUAKE ACTIONS IN SEISMIC CODES
- Page 484 and 485:
examination of the risk implication
- Page 486 and 487:
Bozorgnia and Campbell (2004) find
- Page 488 and 489:
structure, the results of inelastic
- Page 490 and 491:
hazard curves will often vary throu
- Page 492 and 493:
large uncertainties associated with
- Page 494 and 495:
A PRAGMATIC APPROACH FOR PERFORMANC
- Page 496 and 497:
Relative Height20118160.8140.6 1210
- Page 498 and 499:
Yield Strength Coefficient, Cy2.01.
- Page 500 and 501:
Yield Strength Coefficient, Cy*1.61
- Page 502 and 503:
2.6 Preliminary DesignIn the preced
- Page 504 and 505:
4. CONCLUSIONSIn the space availabl
- Page 506 and 507:
EXAMINATION OF THE EQUIVALENT VISCO
- Page 508 and 509:
of the bilinear model with the ener
- Page 510 and 511:
3. STUDY PARAMETERS AND ASSESSMENT
- Page 512 and 513:
decided to investigate the accuracy
- Page 514 and 515:
DISPLACEMENT(m)DISPLACEMENT (m)DISP
- Page 516 and 517:
The results for all 100 earthquake
- Page 518 and 519:
CONTRASTING PERFORMANCE-BASED DESIG
- Page 520 and 521:
Conceptual design is greatly facili
- Page 522 and 523:
2. The availability of cost-of-repa
- Page 524 and 525:
There are many questions to be answ
- Page 526 and 527:
assess expected NSASS losses. For t
- Page 528 and 529:
3.2.2 Design for Tolerable Mean Ann
- Page 530 and 531:
THE PERFORMANCE REQUIREMENTS IN JAP
- Page 532 and 533:
2.1 Law Enforcement and InspectionT
- Page 534 and 535:
Splices and development of reinforc
- Page 536 and 537:
as for the rising part of continuou
- Page 538 and 539:
compressive stress of concrete is t
- Page 540 and 541:
MOLIT Notification No. 1461 outline
- Page 542 and 543:
AUTHOR INDEXH. Akiyama.............
- Page 544 and 545:
F. Taucer .........................
- Page 546 and 547:
PEER 2003/06PEER 2003/05PEER 2003/0
- Page 548 and 549:
PEER 2001/13PEER 2001/12Modeling So
- Page 550:
PEER 1999/04 Adoption and Enforceme