RAPID RESPONSE TEAM CONSULT FORM
RAPID RESPONSE TEAM CONSULT FORM
RAPID RESPONSE TEAM CONSULT FORM

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
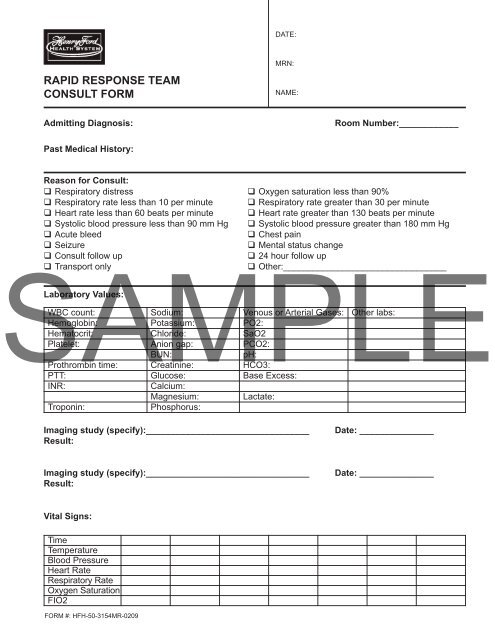
DATE:<strong>RAPID</strong> <strong>RESPONSE</strong> <strong>TEAM</strong><strong>CONSULT</strong> <strong>FORM</strong>MRN:NAME:Admitting Diagnosis:Room Number:____________Past Medical History:Reason for Consult: Respiratory distress Oxygen saturation less than 90% Respiratory rate less than 10 per minute Respiratory rate greater than 30 per minute Heart rate less than 60 beats per minute Heart rate greater than 130 beats per minute Systolic blood pressure less than 90 mm Hg Systolic blood pressure greater than 180 mm Hg Acute bleed Chest pain Seizure Mental status change Consult follow up 24 hour follow upSAMPLE Transport only Other:_________________________________Laboratory Values:WBC count: Sodium: Venous or Arterial Gases: Other labs:Hemoglobin: Potassium: PO2:Hematocrit: Chloride: SaO2Platelet: Anion gap: PCO2:BUN:pH:Prothrombin time: Creatinine: HCO3:PTT: Glucose: Base Excess:INR:Calcium:Magnesium: Lactate:Troponin:Phosphorus:Imaging study (specify):_________________________________Result:Date: _______________Imaging study (specify):_________________________________Result:Date: _______________Vital Signs:TimeTemperatureBlood PressureHeart RateRespiratory RateOxygen SaturationFIO2<strong>FORM</strong> #: HFH-50-3154MR-0209
Assessment: Deferred; transport onlyNeurological:Cardiovascular:Respiratory:Gastrointestional:Genitourinary:Output:____________________Fluid Balance:______________SAMPLEInterventions: Pulse Oximetry IV Start: Gauge:_________________ Arterial/Venous Blood GasSite:_________________ Nebulizer Treatment IV Fluid Bolus: Type of Fluid: _______________ BIPAP/CPAPTotal Amount: _______________ Chest X-ray Blood Product: Type: _____________________ SuctionAmount :______ Units: _______ EKG Vasoactive: Drug: _______________________ Intubation*Dosage: _____________________ No intervention required Labs (specify):Medications/Other Interventions:Plan:Outcome: Transferred to __________ Stay in present level of care Code Blue- survived* Code Blue- expired*Date:__________ Time: _______ Signature:_________________________ Pager:_______________0688<strong>FORM</strong> #: HFH-50-3154MR-0209*See Code Blue Form See General Notes