Complexity of Type 2 Diabetes: Nursing Focus - therapy areas
Complexity of Type 2 Diabetes: Nursing Focus - therapy areas
Complexity of Type 2 Diabetes: Nursing Focus - therapy areas

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
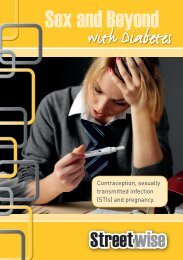
<strong>Complexity</strong> <strong>of</strong> type 2 diabetes: A hands-on guideto simplifying care in clinical practiceThis report, written by SB Communications Group, is based on a meeting forhealthcare pr<strong>of</strong>essionals that took place on 22 November 2012 in Wembley, London.The management <strong>of</strong> type 2 diabetes in clinical practice is complex for a number <strong>of</strong> reasons. The condition has thepotential to affect multiple organs in the body, and owing to the fact that it is a progressive condition, there is a needfor on-going monitoring and <strong>of</strong>ten treatment intensification over time (NICE, 2009b). Furthermore, the evidencebase that shapes clinical practice is constantly evolving, and in recent years, several newer classes <strong>of</strong> glucose-lowering drugshave become available and controversies have arisen in relation to some <strong>of</strong> the older agents (Inzucchi et al, 2012). A number <strong>of</strong>meetings designed to help healthcare pr<strong>of</strong>essionals examine some <strong>of</strong> the key complexities in type 2 diabetes in greater detail wereheld across the UK during the autumn <strong>of</strong> 2012, with the aim <strong>of</strong> providing clarity, insight and guidance on how they might beaddressed pragmatically in “real-life” clinical practice. This report is based on one <strong>of</strong> the London meetings in the series.Introduction: In what ways is type 2diabetes complex?Richard Brice, GP with a Special Interestin <strong>Diabetes</strong>, Whitstable“<strong>Type</strong> 2 diabetes can be called ‘complex’for a whole range <strong>of</strong> reasons,” said DrRichard Brice as he welcomed delegatesto this afternoon meeting. “It’s not just adisease <strong>of</strong> the beta-cells <strong>of</strong> the pancreas,but it’s a condition affecting the alphacellsas well. It’s a disease <strong>of</strong> the eyes,the kidneys, the nerves, the feet, theautonomic nervous system, the gut, theheart – so, for healthcare pr<strong>of</strong>essionals,there’s a lot to think about.” More thanthis, though, the progressive nature <strong>of</strong>the condition means that the clinicalmanagement <strong>of</strong> the individual with type 2diabetes <strong>of</strong>ten increases in complexity astime goes on, said Dr Brice (Figure 1).Aside from these “medical” issues, thereare various additional practical intricaciesthat must be borne in mind, such askeeping up with the rapidly evolvingevidence base regarding diabetes therapiesand the need to balance or reconcilepotentially conflicting influences onprescribing. “For example, we’ve got DVLAguidance [Driver and Vehicle LicensingAgency, 2012] drawing attention to thefact that sulphonylureas [SUs] can causehypoglycaemia, and therefore people whodrive on SUs ideally need to test theirglucose levels each time before they drive,”said Dr Brice. “But, how do we resolve thiswith the focus on less testing and moreuse <strong>of</strong> SUs in QIPP [Quality ImprovementProductivity and Prevention; NationalPrescribing Centre, 2012]?” He finished byexplaining that the afternoon would focuson providing guidance on complexities infour key <strong>areas</strong> in the current management<strong>of</strong> type 2 diabetes.<strong>Complexity</strong> 1: All change! What youneed to know about diagnosing type 2diabetes now.Grace Vanterpool MBE, Consultant Nursein <strong>Diabetes</strong>, Central London CommunityHealthcare NHS Trust & ImperialHealthcare NHS Trust“In the 25 or so years that I’ve been workingin diabetes I’ve seen so many changes in thediagnostic criteria for diabetes, and they’verecently undergone another importantupdate in that we can now diagnose thecondition on the basis <strong>of</strong> HbA 1c,” said GraceDiagnosis <strong>of</strong>type 2 diabetesTime/age<strong>of</strong> patientas she began her presentation. In 2011,the World Health Organization publishedits latest diagnostic criteria for diabetes,stating that an HbA 1clevel <strong>of</strong> 48 mmol/mol[6.5%] is recommended as the cut point(World Health Organization, 2011), withthis value chosen because it corresponds tothe approximate level <strong>of</strong> HbA 1cat which, inepidemiological studies, there is an upwardinflection in the risk <strong>of</strong> diabetes-specificretinopathy (Colagiuri et al, 2011).Regarding the practical implementation<strong>of</strong> the revised criteria, Grace highlightedrecommendations from a UK consensusgroup on the use <strong>of</strong> HbA 1cfor diagnosis(John et al, 2012). The key points from thepublication are:• For most patients, an HbA 1clevel <strong>of</strong>≥48 mmol/mol (≥6.5%) can be used todiagnose diabetes in most situations.Development <strong>of</strong> complications and comorbidities (e.g. renal impairment, CVD)Figure 1: The complexity <strong>of</strong> type 2 diabetes.CVD=cardiovascular disease.Age-related changes (e.g. reduced mobility, cognitive impairment)Continuous monitoring and review<strong>Complexity</strong> increasingChanges in lifestyle, personal goalsReducing beta-cell function, counter-regulatory mechanismsIncreasing number <strong>of</strong> glucose-lowering agents3
MEETING REPORTIn those without diabetes symptoms,a repeat venous HbA 1ctest shouldbe conducted in the same laboratorywithin 2 weeks.• If the second sample is
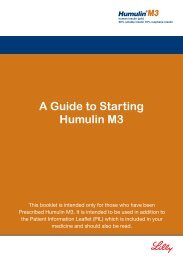
MEETING REPORTTable 1. Summary <strong>of</strong> glucose-lowering drugs commonly used in the management <strong>of</strong> type 2 diabetes. 1Drug classAvailable agentsPrimary physiologicalactionAdvantagesDisadvantagesBiguanides Metformin i Hepatic glucoseproduction• Extensive clinical experience• No weight gain• Low inherent risk <strong>of</strong>hypoglycaemia• Likely i CV events (UKPDS)• Low unit cost• Gastrointestinal side-effects (diarrhoea,abdominal cramping)• Lactic acidosis risk (rare)• Vitamin B 12deficiency• Multiple contraindications: CKD, acidosisSulphonylureasGlibenclamide, h Insulin secretion •gliclazide,•Extensive clinical experiencei Microvascular risktolbutamide 2glimepiride,(UKPDS)glipizide,• Low unit cost• Hypoglycaemia• Weight gain• Blunts myocardial ischaemicpreconditioningTZDs Pioglitazone h Insulin sensitivity • Low inherent risk <strong>of</strong>hypoglycaemia• Durable glucose lowering• h HDL-cholesterol• i Triglycerides• i CV events• Weight gain• Oedema/heart failure• Bone fractures• Possible increase in bladder cancerDPP-4inhibitorsLinagliptin,saxagliptin,sitagliptin,vildagliptin 3h Insulin secretion(glucose-dependent),i glucagon secretion(glucose-dependent)• Low inherent risk <strong>of</strong>hypoglycaemia• Weight neutrality• Well tolerated• High unit cost• Lack <strong>of</strong> long-term efficacy andtolerability data• Concern regarding possible risk <strong>of</strong>pancreatitisGLP-1 receptoragonistsExenatide onceweekly, exenatidetwice daily,liraglutide 3 ,lixisenatideh Insulin secretion(glucose-dependent),i glucagon secretion(glucose-dependent),slows gastric emptying,h satiety• Low inherent risk <strong>of</strong>hypoglycaemia• Potential for weight reduction• Potential for blood pressurereduction• Gastrointestinal side effects (nausea,vomiting)• Injectable• Training requirements• High unit cost• Concerns regarding possible risk <strong>of</strong>pancreatitisSGLT2inhibitorsDapagliflozin 3i Renal glucose • Low inherent risk <strong>of</strong>• Not recommended in moderate to severeabsorption 3 hypoglycaemia 4renal impairment 5• Potential for weight reduction 4 • h Incidence <strong>of</strong> genital infections andreduction 5 • Potential risk <strong>of</strong> breast, bladder and• Potential for blood pressure urinary tract infections relative to placebo 5prostate malignancies (to be furtherinvestigated in post-authorisation studies) 5InsulinVariouspreparationsavailableh Glucose disposal,i hepatic glucoseproduction• Universally effective• Theoretically unlimitedefficacy• i Microvascular risk(UKPDS)• Hypoglycaemia• Weight gain• Injectable• Training• “Stigma” (for patients)CKD=chronic kidney disease; CV=cardiovascular; DPP-4=dipeptidyl peptidase-4; GLP-1=glucagon-like peptide-1; SGLT2; sodium–glucose co-transporter 2;TZDs=thiazolidinediones; UKPDS=UK Prospective <strong>Diabetes</strong> Study.1. Adapted from: Inzucchi et al (2012) 2. British National Formulary (2013a) 3. British National Formulary (2013b) 4. Chao (2012) 5. Bristol Myers Squibb-AstraZeneca EEIG (2013b).cardiovascular outcomes studies are dueto report in the next few years.“So, with all this in mind, which drugshould we use, and when?” asked DrDarko, after running through the mainglucose-lowering classes. He began thediscussion by displaying an abbreviatedversion <strong>of</strong> the current NICE algorithmfor the management <strong>of</strong> hyperglycaemiain type 2 diabetes (NICE, 2009a),commenting that “after metformin, itsuggests that you add in an SU as theusual approach, but it does gives you thealternatives <strong>of</strong> using a DPP-4 inhibitoror thiazolidinedione in people who youconsider to be at risk <strong>of</strong> hypoglycaemiaor its consequences.” At the third-linelevel <strong>of</strong> the algorithm, adding insulin tothe combination <strong>of</strong> metformin and anSU is the usual approach, with alternativeoptions being exenatide or sitagliptinin particular circumstances (the otherDPP‐4 inhibitors and GLP-1 receptoragonists were either not available at the5
MEETING REPORTtime the guideline was published or notlicensed for third-line use).Reflecting the fact that the NICEalgorithm is now nearing 4 years <strong>of</strong> ageand hence is somewhat out <strong>of</strong> date in terms<strong>of</strong> the agents it incorporates, Dr Darkobrought delegates’ attention to a morerecent, pragmatic, joint position statementfrom the American <strong>Diabetes</strong> Association(ADA) and European Association for theStudy <strong>of</strong> <strong>Diabetes</strong> (EASD) regarding themanagement <strong>of</strong> hyperglycaemia in type 2diabetes (Inzucchi et al, 2012). One <strong>of</strong> thekey messages <strong>of</strong> the statement, he said,is that “individualisation <strong>of</strong> treatmentis the cornerstone <strong>of</strong> success”, withindividualisation referring both to thelevel <strong>of</strong> stringency with which glycaemiais addressed and the choice <strong>of</strong> the agentsused to tackle hyperglycaemia. Readersare urged to review the algorithm forblood glucose lowering <strong>therapy</strong> containedwithin the position statement (Inzucchiet al, 2012).<strong>Complexity</strong> 3: Understanding therelationship between diabetes,glucose-lowering drugs andcardiovascular diseaseRichard Brice, GP with a Special Interestin <strong>Diabetes</strong>, Whitstable“Amazingly, in diabetes, unlike in the field<strong>of</strong> hypertension or lipids, we don’t havethat many really long-term studies tosee whether or not diabetes medicationsactually make people’s lives longer,” saidDr Brice, as he took the stage for the thirdsession <strong>of</strong> the afternoon. In this respect,the long-term effect <strong>of</strong> intensive glucoselowering,and indeed individual glucoseloweringagents, on cardiovascular (CV)risk is <strong>of</strong> high importance because themain cause <strong>of</strong> mortality for people withdiabetes is cardiovascular disease (CVD;Morrish et al, 2001).Dr Brice continued by outlining the keypoints arising from the four major clinicaltrials that have examined the CV effects<strong>of</strong> intensive glucose lowering in peoplewith type 2 diabetes: the UKPDS (UKProspective <strong>Diabetes</strong> Study), ACCORD(Action to Control Cardiovascular Riskin <strong>Diabetes</strong>), ADVANCE (Action in<strong>Diabetes</strong> and Vascular Disease: Preteraxand Diamicron), and the VADT (VeteransAffairs <strong>Diabetes</strong> Trial) (UKPDS Group,1998; ACCORD Study Group et al, 2008;ADVANCE Collaborative Group et al,2008; Holman et al, 2008; Duckworthet al, 2009).In the first <strong>of</strong> these, intensivemanagement <strong>of</strong> glucose levels was foundto yield improvements in the incidence<strong>of</strong> both micro- and macrovasculardisease, as compared with “conventional”management <strong>of</strong> glycaemia. A protectiveeffect <strong>of</strong> intensive glucose lowering onmacrovascular risk was not replicatedin the ACCORD, ADVANCE or theVADT studies – and indeed, in the case <strong>of</strong>ACCORD, the intensively treated patientsexperienced an increased mortality rate– but the patient populations studied inthese trials were different to those enrolledin the UKPDS, explained Dr Brice. Inthe UKPDS, patients were enrolled at thepoint <strong>of</strong> diagnosis and followed in therandomised phase <strong>of</strong> the trial for a median<strong>of</strong> approximately 11 years, whereas theother trials enrolled participants withestablished CVD risk factors later in thecourse <strong>of</strong> the disease process, and followedthem for shorter randomised periods.Dr Brice explained that a number <strong>of</strong>reasons have been proposed to explainthe increased rate <strong>of</strong> mortality in theintensively treated group in ACCORD,including an increased prevalence <strong>of</strong>hypoglycaemia, weight gain, a heightenedrisk <strong>of</strong> drug–drug interactions, the rapiditywith which glucose levels were loweredand more participants in the group takingrosiglitazone (Matthews, 2011; Wintersteinet al, 2011; Inzucchi et al, 2012). Afterconsidering in more detail some <strong>of</strong> theCV sequelae <strong>of</strong> hypoglycaemia (Marqueset al, 1997) that might have explained theresults <strong>of</strong> ACCORD, Dr Brice summarisedthe discussion: “When considering CVrisk in type 2 diabetes, it is certain thatthe higher a person’s HbA 1clevel is, thegreater their likelihood <strong>of</strong> CVD. But whatis more difficult to prove is whether or notlowering their glucose levels per se willbring down their risk.”This statement naturally leads to aconsideration <strong>of</strong> whether the means bywhich glucose is lowered – that is, thespecific blood glucose-lowering drugsused – is important to CV health. “Inother words,” said Dr Brice, “can I usetwo different drugs, get the same glucoseresults but achieve very different CVoutcomes? I believe that the answeris probably ‘yes’. Just because a drugimproves glucose levels, we cannotassume that it lowers CV risk. In fact,quite the opposite might be true.”Indeed, concerns regarding the CVeffects <strong>of</strong> rosiglitazone (Rosen, 2010) ledthe US Food and Drug Administration(FDA) to issue guidance to thepharmaceutical industry in 2008 aimingto ensure that all drug developmentprogrammes for type 2 diabetes should“rule out an unacceptable increase in CVrisk” (FDA, 2008).A range <strong>of</strong> glucose-lowering agentsfor type 2 diabetes have been approvedin the UK and the USA since theintroduction <strong>of</strong> the FDA restrictions,including liraglutide, exenatide onceweekly, saxagliptin and linagliptin. Anumber <strong>of</strong> prospective, randomisedCV outcome trials are currently inprogress for these agents and Dr Bricesummarised the CV outcome data thatcurrently exists while these results areawaited. For example, in the case <strong>of</strong>linagliptin, a prospective pre-specifiedmeta-analysis <strong>of</strong> CV events from eightphase III, placebo- or active-comparatorcontrolled, clinical studies has beenconducted and published (Johansen et al,2012). The hazard ratio (HR) for theprimary endpoint <strong>of</strong> occurrence or timeto first occurrence <strong>of</strong> CV death, nonfatalmyocardial infarction, non-fatalstroke or hospitalisation for unstableangina, suggested a significantly lowerrisk with linagliptin than comparators(HR 0.34 [95% confidence interval(CI) 0.16–0.70]) as did estimates for all6
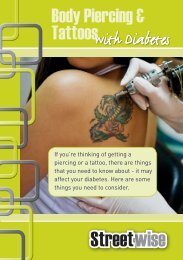
MEETING REPORTTable 2. Comparison <strong>of</strong> renal restrictions related to the use <strong>of</strong> DPP-4 inhibitors.Drugsecondary endpoints (HRs ranging from0.34 to 0.55 [all upper 95% CIs
Prescribing Information (UK)t Trajenta® (linagliptin)TRAJENTA® 5 mg film-coated tabletsFilm-coated tablets containing 5 mg linagliptin. Indication: Trajenta isindicated in the treatment <strong>of</strong> type 2 diabetes mellitus to improve glycaemiccontrol in adults: as mono<strong>therapy</strong>: - in patients inadequately controlledby diet and exercise alone and for whom metformin is inappropriatedue to intolerance, or contraindicated due to renal impairment; ascombination <strong>therapy</strong>: - in combination with metformin when diet andexercise plus metformin alone do not provide adequate glycaemic control;- in combination with a sulphonylurea and metformin when diet andexercise plus dual <strong>therapy</strong> with these medicinal products do not provideadequate glycaemic control; - in combination with insulin with or withoutmetformin, when this regimen alone, with diet and exercise, does notprovide adequate glycaemic control. Dose and Administration:5 mg once daily. If added to metformin, the dose <strong>of</strong> metformin shouldbe maintained and linagliptin administered concomitantly. When usedin combination with a sulphonylurea or with insulin, a lower dose <strong>of</strong>the sulphonylurea or insulin, may be considered to reduce the risk <strong>of</strong>hypoglycaemia. Patients with renal impairment: no dose adjustmentrequired. Patients with hepatic impairment: pharmacokinetic studiessuggest that no dose adjustment is required for patients with hepaticimpairment but clinical experience in such patients is lacking. Elderly: nodose adjustment is necessary based on age however, clinical experience inpatients > 80 years <strong>of</strong> age is limited and caution should be exercised whentreating this population. Paediatric population: the safety and efficacy <strong>of</strong>linagliptin in children and adolescents has not yet been established. Nodata are available. Trajenta can be taken with or without a meal at any time<strong>of</strong> the day. If a dose is missed, it should be taken as soon as possible but adouble dose should not be taken on the same day. Contraindications:Hypersensitivity to the active substance or to any <strong>of</strong> the excipients.Warnings and Precautions: Trajenta should not be used in patientswith type 1 diabetes or for the treatment <strong>of</strong> diabetic ketoacidosis. Cautionis advised when linagliptin is used in combination with a sulphonylureaand/or insulin; a dose reduction <strong>of</strong> the sulphonylurea or insulin may beconsidered. Pancreatitis: In post-marketing experience <strong>of</strong> linagliptin therehave been spontaneously reported adverse reactions <strong>of</strong> acute pancreatitis.Patients should be informed <strong>of</strong> the characteristic symptom <strong>of</strong> acutepancreatitis: persistent, severe abdominal pain. Resolution <strong>of</strong> pancreatitishas been observed after discontinuation <strong>of</strong> linagliptin. If pancreatitis issuspected, Trajenta should be discontinued. Interactions: Linagliptin isa weak competitive and a weak to moderate mechanism-based inhibitor<strong>of</strong> CYP isozyme CYP3A4, but does not inhibit other CYP isozymes. It isnot an inducer <strong>of</strong> CYP isozymes. Linagliptin is a P-glycoprotein substrateand inhibits P-glycoprotein mediated transport <strong>of</strong> digoxin with lowpotency. Based on these results and in vivo interaction studies, linagliptinis considered unlikely to cause interactions with other P-gp substrates.The risk for clinically meaningful interactions by other medicinal productson linagliptin is low and in clinical studies linagliptin had no clinicallyrelevant effect on the pharmacokinetics <strong>of</strong> metformin, glibenclamide,simvastatin, warfarin, digoxin or oral contraceptives (please refer toSummary <strong>of</strong> Product Characteristics for information on clinical data).Fertility, pregnancy and lactation: Avoid use during pregnancy.A risk to the breast-fed child cannot be excluded. A decision must bemade whether to discontinue breast-feeding or to discontinue/abstainfrom Trajenta <strong>therapy</strong> taking into account the benefit <strong>of</strong> breast-feedingfor the child and the benefit <strong>of</strong> <strong>therapy</strong> for the woman. No studieson the effect on human fertility have been conducted for Trajenta.Undesirable effects: Adverse reactions reported in patients whoreceived linagliptin 5 mg daily as mono<strong>therapy</strong> or as add-on therapies(frequencies identified from pooled analysis <strong>of</strong> placebo-controlledstudies) in clinical trial and from post-marketing experience. The adversereactions are listed by absolute frequency. Frequencies are defined asvery common (≥1/10), common (≥1/100 to




![Humalog Mix50 (50% insulin lispro [rDNA origin] injection ... - LillyPro](https://img.yumpu.com/44269187/1/184x260/humalog-mix50-50-insulin-lispro-rdna-origin-injection-lillypro.jpg?quality=85)

![Humalog Mix25 (25% insulin lispro [rDNA origin] injection 75 ...](https://img.yumpu.com/35487335/1/184x260/humalog-mix25-25-insulin-lispro-rdna-origin-injection-75-.jpg?quality=85)