EVERY WOMEN EVERY CHILD UN COMMISSION ON LIFE-âSAVING
EVERY WOMEN EVERY CHILD UN COMMISSION ON LIFE-âSAVING
EVERY WOMEN EVERY CHILD UN COMMISSION ON LIFE-âSAVING
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
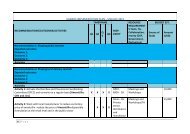
Implementation plan Five immediate actions will help to save lives with this intervention: a) Immediate plan • Integrate use of ACS for lung maturation in preterm labor in existing pre-‐service training programs/packages including Em<strong>ON</strong>C, Helping Babies Breathe (HBB Plus) etc. and conduct training of in-‐service staff up to health center level II including private sector • To ensure equitable access by the poorest ACS will be integrated into existing financial protection mechanism e.g. RH voucher system. • Develop, adapt and disseminate job aids, protocols, checklists, messages and social marketing in line with international guidance and systems to promote the management of preterm labor using corticosteroids. • Include Dexamethasone indication for fetal lung maturation/management of preterm labor in the Uganda EM List and other service standards guidelines. Professional body engagement is key (obstetricians and mid wives) – guidelines to support this should be developed. b) Intermediate plan • Establish tracking mechanism to measure use as a percentage of preterm births to facilitate progressive adoption of this best practice including the mobile phone tracking system (m-trac) and digital HMIS in the ministry of health. Indicators and a scorecard will be developed and used to assess progress towards increased access to ACS. • Conduct a rapid assessment of on status, barriers to access, use and supplies of high quality ACS, supply chain-‐related problems, regulating the quality, accessing, awareness and use barriers for management of preterm labor using the RAIC tool 3.3.2 Injectable Antibiotics for Neonatal Sepsis Problem statement There is insufficient use of injectable antibiotics and lack of appropriate products and formulations for neonates at health facility levels where first contact of a neonate with sepsis is most likely (HC II and HC III). This is in addition to the very low recognition of neonatal sepsis by mothers and other family members, and even lower care seeking, presenting a huge barrier to scaling up this intervention. From the regulation and policy point of view, there is lack of approval for the use of antibiotics by nurses and midwives.