Consultation document.pdf - Shaping a healthier future
Consultation document.pdf - Shaping a healthier future
Consultation document.pdf - Shaping a healthier future
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Shaping</strong> a <strong>healthier</strong> <strong>future</strong><strong>Shaping</strong> a<strong>healthier</strong><strong>future</strong> <strong>Consultation</strong> <strong>document</strong>
ContentsWhat this <strong>document</strong> is forForewordSummary1| Describing the NHS in NW London2| The challenges facing the NHS in NW London3| What will happen if we do nothing?4| So what is the answer?5| Our vision for healthcare in NW London6| World-class healthcare outside of hospital7| Making hospitals centres of excellence8| What will our vision mean for you?9| Delivering the vision10| Where will care be provided in <strong>future</strong> under the proposals?11| Proposals for delivering care outside hospitals12| Our recommendations for local hospitals across NW London13| Elective hospitals using our high-quality buildings14| Five major hospitals for NW London15| Where should the major hospitals be located?16| Which options are practical?17| The three options for major hospitals18| Proposals for changes to specialist services19| Making this work for patients20| Next stepsGlossary248121418202224263032343640434448525769717476
What this <strong>document</strong> is forThis <strong>document</strong> sets outproposals to improve yourlocal NHS services in NorthWest London as part of aprogramme called ‘<strong>Shaping</strong> a<strong>healthier</strong> <strong>future</strong>’.It is a consultation <strong>document</strong> and we wouldlike to hear your views on the changes thatwe propose to make. We have distributedthe <strong>document</strong> widely throughout NorthWest London and neighbouring areaswhere people use services in North WestLondon. The London boroughs defined bythe NHS as North West London are Brent,Ealing, Hammersmith and Fulham, Harrow,Hillingdon, Hounslow, Kensington andChelsea, and Westminster.‘<strong>Shaping</strong> a <strong>healthier</strong> <strong>future</strong>’ is being takenforward by eight clinical commissioninggroups (CCGs), made up of GPs representingNW London’s eight primary care trusts (PCTs).They have worked with hospital doctors,nurse leaders, providers of community caresuch as mental-health services, social services,patient and volunteer groups and charities todevelop the proposals.Or, you can order a copy from our Freepostaddress or Freephone number which are bothshown on the next page.Throughout this <strong>document</strong> you will seea number of questions in boxes, lookinglike this. These questions relate to theresponse form that comes with this<strong>document</strong>, which contains the actualconsultation questions we would like youto answer.Please read the consultation <strong>document</strong> all theway through and then, in the response form,give us your answers to these questions. Inthe response form we have shown whichsections of the <strong>document</strong> cover the issuesraised by each of the questions. Please referback to these sections as you answer thequestions.If you want to explain any of your answers, oryou feel the questions have not given you thechance to give your views fully, or if you thinkthere are options we have not consideredthat we should have done, please say so inthe box at the end of the response form.If you would like to know more about theextensive work behind this <strong>document</strong>, pleaseread our pre-consultation business case(PCBC). You can find this on our websiteat www.<strong>healthier</strong>northwestlondon.nhs.uk2What this <strong>document</strong> is for
You can fill in the questions on the printedresponse form and post it to our Freepostaddress:FREEPOST SHAPING A HEALTHIER FUTURE CONSULTATIONThis must be written exactly as it is shownabove (in capital letters and on one line) andyou will not need a stamp.Or, you can fill it in online on our website:www.<strong>healthier</strong>northwestlondon.nhs.ukIf you have any complaints about theconsultation please contact:Lynne Spencer,Head of Corporate Affairs,NHS NW London,Southside,105 Victoria Street,London,SW1E 6QTWe must receive your response form by nolater than 8 October 2012.This <strong>document</strong> is also available in otherlanguages, in large print, and in audio format.Please ask us if you would like it in one ofthese formats.0800 881 5209consultation@nw.london.nhs.ukWhat this <strong>document</strong> is for 3
ForewordForeword by the chairs of the NWLondon clinical commissioning groupsOur aim is to deliver the best possiblehealthcare to our patients. But people’s healthneeds are changing, and we aren’t able todeliver care to the standards we would like.We believe we need to change the way wedeliver healthcare now, so that we can providehigh-quality care in the medium andlong term.This need for change in the NHS is partlya response to ongoing changes in thepopulation. NW London is growing, people areliving longer, and more people are developingconditions such as diabetes and obesity. Thisis putting pressure on our health services. Weneed a system where we can deliver the rightkind of healthcare, in the right setting.In many cases, the best setting isn’t inhospitals. We know that increasing theamount of care delivered closer to your homewill help care to be better co-ordinated, andimprove the quality of that care and its valuefor money. When people do need hospitalcare, we have shown that making someservices more central will mean that patientsalways have access to the best possible care.As the chairs of the eight clinicalcommissioning groups for NW London,and leaders of this programme to deliverthis change, we have made four maincommitments which support our vision forhow services should work in the <strong>future</strong>.The first is a commitment to help peopletake better care of themselves, understandwhere and when they can get treatment, andunderstand different options for treatment.Secondly, when patients have an urgent4 Foreword What this <strong>document</strong> is for
healthcare problem, we are committed tomaking sure they can easily consult a GP orcommunity-care provider 24 hours a day,seven days a week by phone, email orface-to-face.Our third commitment is that if patients needto see a specialist or receive support fromcommunity or social care services, this will beorganised quickly and GPs will be responsiblefor co-ordinating their healthcare.Finally, if patients need to be admitted tohospital, we are committed to making surethe hospital will be properly maintained andup to date and a place where they can receivetreatment delivered by specialists, 24 hoursa day.We will need to make significant changesto achieve these commitments, and we willhave to make some difficult decisions, but webelieve the changes are essential. The changesmay be substantial, but the rewards of gettingit right will be too, with better healthcare,better support, more lives saved, and asustainable, efficient system.Dr Ethie KongNHS Brent CCG ChairDr Ruth O’HareNHS Central London (Westminster) CCG ChairDr Mark SweeneyNHS West London (Kensington and Chelsea,Queen’s Park and Paddington) CCG ChairDr Mohini ParmarNHS Ealing CCG ChairDr Tim SpicerNHS Hammersmith and Fulham CCG ChairDr Amol KelshikerNHS Harrow CCG ChairDr Ian GoodmanNHS Hillingdon CCG ChairDr Nicola BurbidgeNHS Hounslow CCG ChairForeword5
Foreword by the Medical Director of‘<strong>Shaping</strong> a <strong>healthier</strong> <strong>future</strong>’Dr Mark SpencerAs a doctor trained at Charing Cross Hospitaland as a GP trained at HammersmithHospital, I have been a GP in Acton for 23years. I reluctantly became involved in buyingservices for my patients as a fundholding GPin the 1990s, but found that my patientsbenefited if I paid more attention toinformation that showed where the best carewas available and that together we couldwork with hospitals to improve some stagesof care.Over the last 10 years it has becomeincreasingly clear that the health systemlocally needs to change – and not just alittle bit.As I talk to people, they complain aboutaccess to their GP practice, and about apoorly co-ordinated system, and while theysometimes talk about spectacularly greattreatment, they too often tell me about thelack of care and communication.But as I look at the examples of best practice,and evidence that shows that specialist teamscan do better in some conditions whenworking as part of a larger team, I realisethat the good outcomes we sometimes getare more often because doctors, nurses andother care workers make that happen despitethe organisations they work for, rather thanbeing supported by them.We have too many small hospital units inNorth West London that can’t provide thebest specialist care or make sure that anexpert is available round the clock. Thisprovides average, rather than the best, care.By concentrating specialist care onto fewermajor hospitals and still providing excellentaccess to networked care at local hospitalswe can get better care. This also allowsinvestment into community and primary care,which is where most patients are treated.I was leading a local group of GPs, but havehad the opportunity over the last year toco-ordinate and work with GPs with similarcares and concerns for people across NorthWest London. We have worked with hospitaldoctors and nurses and considered how wecan make things better, and affordable. Itis this group of GPs, supported by seniordoctors from every hospital in the region,that has led this work and drawn up theserecommendations.Change is rarely welcomed, and manyattempts have been made in the past toimprove care in North West London. Butas clinicians come together to take on theresponsibilities of making sure the best careis available for the local population, we havean opportunity that we must take. If wedon’t take this opportunity we will face thinlyspread services or unplanned closures onsafety grounds. But if we work to make thesechanges, we will save many lives and improvethe care that people experience every day.This is an opportunity not to be missed.I do hope that you read this <strong>document</strong>,consider and discuss it. We reallyhaven’t made any decisions yet – ourrecommendations will benefit fromyour response.Dr Mark SpencerMedical Director, <strong>Shaping</strong> a <strong>healthier</strong> <strong>future</strong>6 Foreword What this <strong>document</strong> is for
Foreword by the Chair of the JointCommittee of Primary Care TrustsJeff ZitronFor those of us who live in North WestLondon, having a strong local NHS is a toppriority. Many residents owe their lives andgood health to the quality of our staff andfacilities. However, others are not able toaccess the services they need or do notalways receive the highest standard of care.Demands on the NHS are increasing becauseof its very success – for example, people areliving longer and medical advances meanmore conditions can be treated than everbefore. As a result, standards of care keep onrising, so the NHS must change to keep pace.these PCTs will consider the results of theconsultation, and will then decide whetherchanges should be made and, if so, whatthese changes should be.We are very keen to hear your views. Aswell as reading this <strong>document</strong>, we hopethat you are able to take part in otherconsultation events (see our website atwww.<strong>healthier</strong>northwestlondon.nhs.uk formore details). ‘<strong>Shaping</strong> a <strong>healthier</strong> <strong>future</strong>’is about planning how we can have thestrongest local NHS possible in the yearsahead and I hope you will be able tocontribute to this.Jeff ZitronChair, NHS North West London and the JointCommittee of Primary Care TrustsThis <strong>document</strong> explains why and howhealth services in North West Londonneed to change, and describes options forachieving this. The proposals within the<strong>document</strong> have been developed by localdoctors, nurses and other healthcare staff, inconsultation with patients, councils and careorganisations. We propose major changesto how services are provided in hospitalsand within the community. The proposalsdraw on experience − in North West Londonand beyond – of how health services canbe improved by making better use of staffexpertise, buildings and funds.Before any decision is made on theseproposals, we are asking the public inthe areas affected for their views. Thisconsultation is being overseen by the NHSprimary care trusts (PCTs) in North WestLondon, together with other PCTs whoseresidents may be affected by the proposedchanges. The joint committee formed byForeword7
Summary‘<strong>Shaping</strong> a <strong>healthier</strong> <strong>future</strong>’proposes changes that willimprove care both in hospitalsand the community and willsave many lives each year. Thissummary explains how.We look after nearly two million people in NWLondon and have high aims for the way theyare cared for and the services they receive. Ourstaff are totally committed to this high-qualitycare, but need to have the right workforce, skillsand surroundings to deliver this for patients.Increasingly, a number of different factors inNW London are making it very difficult for us tolook after patients in this way.These factors include the challenges of lookingafter a growing and ageing population, withtoo few specialists in hospitals to provide highqualityround-the-clock care, working frominadequate NHS facilities, and working withinan increasingly tight budget. These challengesneed to be met – or the NHS and its servicesin NW London will deteriorate. This wouldmean inequalities continuing, people dyingunnecessarily, hospitals and other servicesfailing, hospitals being unable to recruit andkeep staff, and some NHS trusts facing severefinancial pressure.Since it would be irresponsible not to tacklethese challenges and simply allow patientsto get a worse service, we (GPs, hospitaldoctors, community providers, nurses, andwider NHS staff) have looked at ways inwhich health services are being improved inLondon and around the world to develop avision for healthcare in NW London.We have based this vision on the principlesthat you should have:• the support you need to take better careof yourself;• a better understanding of where, whenand how you can be treated;• the tools and support you need to bettermanage your own medical condition;• easy access (24 hours a day, seven daysa week) to primary-care clinicians suchas GPs – by phone, email or in person –when you need to be seen urgently;• fast and well-co-ordinated access tospecialists, community and social-careproviders, (this access would be managedby GPs); and• properly maintained and up-to-datehospital facilities with highly trainedspecialists available all the time.The way in which we would deliver thisvision, which would meet all these demands,is by:8 Summary What this <strong>document</strong> is for
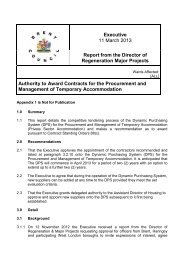
provide this more complicated healthcare,people in surrounding areas would, onaverage, have to travel too far to get tothe next hospital providing those kinds ofservices.If these proposals are accepted – with twoof the five proposed major hospitals atNorthwick Park Hospital and HillingdonHospital, and Central Middlesex Hospital asan elective hospital – we propose that servicesat the remaining three major hospitals shouldbe distributed evenly across NW London tokeep the effect of changes on local residentsto a minimum. This means that there wouldbe a choice of:• one major hospital at either EalingHospital or West Middlesex Hospital; and• one major hospital at either HammersmithHospital or St Mary’s Hospital.We have assessed these choices in detail,looking at which would deliver the bestclinical quality of care and access to care,whether they are affordable and can bedelivered, and which would be best forresearch and education, and this has resultedin three options for the public to consider.• one major hospital at either Charing CrossHospital or Chelsea and WestminsterHospital;Option A Option B Option CSt Mary’s Major hospital Major hospital Major hospitalHammersmith Specialist hospital Specialist hospital Specialist hospitalCharing Cross Local hospital Major hospital Local hospitalChelsea &WestminsterMajor hospital Local hospital Major hospitalWest Middlesex Major hospital Major hospitalLocal hospital andelective hospitalEaling Local hospital Local hospital Major hospitalCentral MiddlesexLocal hospital and Local hospital and Local hospital andelective hospital elective hospital elective hospitalNorthwick Park Major hospital Major hospital Major hospitalHillingdon Major hospital Major hospital Major hospital10 Summary
We prefer option A because it:• will improve quality of care;• makes good use of buildings;• represents the best value for money;• is the easiest option to carry out; and• supports research and education.We have considered carefully whether thereshould be a ‘preferred option’ to put to thepublic, since the three options – A, B and C –are all potentially suitable. However, becausethe Joint Committee of Primary Care Trusts,who will make the final decision on anychanges, believe that option A would give thegreatest benefits for NW London, it would bemisleading not to say so. However, this is alsoa consultation aimed at gathering people’sviews. So we are putting all three optionsforward and inviting your views on whichoption will have the greatest benefits.can make a difference. In this <strong>document</strong>, wehave asked you specific questions on eachof the changes that we are proposing. Theconsultation will run from 2 July to 8 October2012. We will then spend a few monthslooking at your responses, and make a finaldecision in early 2013.If these changes are agreed, it will take atleast three years to put them in place. Weare already putting in place services thatcan be provided in the home, GP surgeriesand health centres and only once theseservices are running successfully will we makechanges to hospitals.If Charing Cross Hospital is not a majorhospital, we are proposing that the hyperacutestroke unit at Charing Cross Hospitalmoves to be alongside the major traumacentre at St Mary’s Hospital. The London-widestroke and major trauma consultation carriedout in 2009 by NHS London preferred puttinghyper-acute stroke units on the same site asmajor trauma centres, as they need similarback-up and support.Finally, we propose that the Western EyeHospital is moved to be alongside the majorhospital at St Mary’s Hospital. This willimprove the quality of care for patients.We are now consulting everyone in NWLondon about these options for change togive them the chance to give their views andcomments. We have not made any decisionsand your feedback and explanations of howwe could do things differently or better reallySummary11
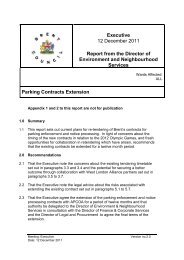
1. Describing the NHS inNW LondonWe look after nearly twomillion people in NW London,providing the best possible carewith the resources available.Local GPs, hospital doctors and other clinicians– including nurses, midwives, pharmacists,those providing community services, andmany others – are devoted to delivering thehighest-quality services they can.We do this because we are committed toour patients within the eight boroughs. InNW London there are 10 acute and specialisthospital trusts, 423 GP practices, twocommunity trusts and two mental-health trusts.The NHS in NW LondonHospitals in NW London8 London boroughs2 million people£3.4 billion annual health budgetHarefieldMountVernonRoyal NationalOrthopaedicMore than 400 GP practices and 1100 GPs8 clinical commissioning groups10 acute and specialist hospital trusts2 mental-health trusts2 community-health trustsHillingdonNorthwickParkCentral MiddlesexHammersmithSt Mary’sWestern EyeEalingWestMiddlesexCharingCrossChelseaandWestminsterRoyalMarsdenRoyalBrompton12Describing What this <strong>document</strong> the NHS in is NW for London
The rich diversity of NW London, with itshundreds of different communities andwide range of people, makes deliveringhealthcare a demanding challenge. Everysingle employee of the NHS understands thisand is committed to meeting the challenge. Itis what the NHS was created to do – to carefor its patients, no matter how complex ordifficult that might be.may include you. The next part of this<strong>document</strong> explains why.This means delivering more care insurroundings which are better for patients– for example in community facilities, GPsurgeries, and in the home. It means makingsure that centres of excellence, such as thehospitals in NW London, have access 24hours a day, seven days a week, to the bestdoctors, equipment and back-up.To provide services of the highest qualityacross this diverse part of London, weneed to have the right resources. We needa high-quality workforce of expert, welltrainedcolleagues, the latest equipmentand technology, backed by world-classresearch and education, and the best possiblesurroundings in which to work.If you live in NW London, it means providingcare for you across the many organisationsthat are involved in that care, so you alwaysknow what is happening, have full access tothe best advice when and where you need it,and if things do not go as planned you knowyou can quickly get the very best back-up.These might seem obvious and entirelyunderstandable requirements for a healthservice, given the importance to the NHS ofcaring for so many people across so manyboroughs. But it is easy to lose sight of justhow complex and challenging the healthneeds of an area can be, and just howchallenging it can be to meet these needs.Increasingly, many different factors in NWLondon are making it very difficult for us tolook after our patients in this way – whichDescribing the NHS in NW London 13
2. The challenges facing theNHS in NW LondonThere are a number ofchallenges facing the NHS asa whole and those of us whodeliver health services inNW London.Many of the challenges are part of the natureof a thriving, bustling, successful city. Some ofthem apply only to certain communities andareas, others are the same as those faced bymajor cities the world over.Population challenges• A growing population. NW London is avery densely populated area, and overthe next 10 years the number of peopleliving here is expected to increase fromjust under 1.9 million to 2 million. Thesheer number of people needing care,‘from cradle to grave’, represents a majorchallenge for the NHS.• A population with different lifeexpectancy. NW London varies hugelyfrom place to place in economic terms,with very poor and very wealthyhouseholds often living side by side. Andhealth varies with wealth: the poorer youare, the more likely you are to suffer illhealth. Within NW London, there is a 17-year difference in the life expectancy ofthose living in the most deprived wards,compared with those in the wealthiestwards. These differences can be causedby many things, such as living conditions,diet, levels of smoking and drinking,access to sport and leisure facilities, andeven language barriers. Better healthcarecannot overcome all these things but itcan make a major difference to them,and is known to reduce inequalitiesbetween people.• An ageing population. In NW Londonthe good news is that life expectancy isimproving and so people are living longer.Ten years ago, life expectancy in NWLondon was 77 years for men and 82years for women. Today, it is about threeyears longer. For the NHS, this increasesthe pressure on services because olderpeople are more likely to develop longtermhealth conditions such as diabetes,heart disease, breathing difficulties anddementia.• A population with modern lifestyles. Poordiet and lack of exercise are the hallmarksof a typical, western lifestyle. They leadto increased rates of obesity and diabetesand, in NW London, we are treating moreand more of these conditions. Similarly,smoking is the UK’s single greatest causeof preventable illness and early death,and alcohol abuse (which is increasingin NW London) is leading to increasingrates of death from liver disease and otherconditions.14 The What challenges this <strong>document</strong> facing is the forNHS in NW London
Clinical challenges• It is difficult for people to get to see a GPwhen they need to and too many peopleend up in A&E. 75% of people say theymanage to see their GP when they needto but this means that one in four patientsin NW London feels it takes too long. Thesame number feel they are not treatedwith care and concern by their GP. Thesesatisfaction rates are below the nationalaverage.• At the same time, NW London has moreA&E departments per person than otherparts of the country and more peoplethan average use A&E services. This ispartly because people who cannot accessprimary care (such as GP services) oftenend up going to hospital instead. Butproviding healthcare through A&E ismore expensive, and lacks the kind ofco-ordinated care that a GP can providebecause, for example, they know thepatient’s family and their health history.Many GPs offer good-quality care, butfor too many patients that care is notavailable when they need it.• More people are now living with longtermmedical conditions, such as diabetes,heart disease, and respiratory problemssuch as asthma, which are creatingparticular problems in NW London. Onecomplication of diabetes for example isreduced blood flow to the legs. If nottreated early, this can lead to amputation.When people are managed by GPswith specialised clinics, supported by adiabetic nurse, amputation is much lesslikely to happen. But not everyone inNW London has access to such a service.The ‘integrated care pilot’ we describe insection 4 has already improved outcomesfor diabetics, but NW London still needslocal specialist services to improvetreatments.• Too many elderly people end up inhospital when, with appropriate careoutside hospital, they could be treatedin the community and looked after athome. There are good reasons for caringfor people outside hospital, becauseelderly people are at risk of developingfurther conditions in hospital. Equally, atthe end of people’s lives, the NHS needsto do more to support them to die athome if this is what they want. In NWLondon, only 18% of people die at homecompared with a national average of23%, even though 54% of patients saythey would prefer to die at home.• As shown by the reorganisation of strokeservices in London (see section 4), thereis clear evidence that in emergency cases,having senior hospital staff on hand meansa better outcome for the patient. In otherwords, people suffer fewer complicationsand are less likely to die when there is asenior doctor there to care for them whenthey arrive seriously ill. Statistics show thatin London as a whole, people who areadmitted to hospital as an emergency caseat the weekend are 10% more likely to diethan people who are admitted during theweek. At present, the number of seniordoctors available drops by more thanhalf at many London hospitals during theweekend. Solving this issue could save 130lives in NW London every year.• The number of women who needmaternity services is increasing andpregnancies are becoming morecomplicated. The rate of maternal deathsin London has doubled in the last fiveyears, reaching twice the rate in the restof the UK. Many of these deaths couldhave been prevented. Babies born outsideof normal working hours are also at ahigher risk of dying. This is associatedwith a lack of access to senior staff atthese times, and maternity units cannotmeet recommended midwife staffingThe challenges facing the NHS in NW London15
levels. We also do not have enough nursesto care for sick babies in NW London (wehave the highest vacancy rate in London)and we do not have enough seniordoctors to provide round-the-clock carefor children in hospital.• These issues won’t be solved simply bytraining and hiring more doctors. Thosedoctors also need experience of dealingwith complications regularly, so they canprovide the best specialist care. If theydo not see enough patients, they losetheir skills and cannot provide such highqualitycare. If they are spread acrossmany hospitals, doctors will not get thatexperience.NHS buildings and facilitieschallenges• You might think having lots of bighospitals would help if a population hasmany health problems, but this is actuallynot the case, and NW London proves thepoint. The fact that there are a lot of bighospitals here causes more problems thansolutions. With 50% more building spaceper hospital bed in NW London than inthe rest of the country, it means:> > we spend much more on hospitalmaintenance and running costs than inmany other places and this means wehave less money to spend on servicessuch as GPs than in other parts of thecountry;> > two-thirds of hospitals in NW Londonwould ideally need significantinvestment and refurbishment to meetmodern standards. The ‘backlog’maintenance bill to correct just the veryworst issues is around £53 million; and> > there are so many big expensive NHSbuildings in NW London that even withthis level of spending on maintenance,NHS buildings in NW London aregenerally not in a good condition.16 The What challenges this <strong>document</strong> facing is the forNHS in NW London
• The best way to treat a population withlots of increasing health demands isactually to spend more money on servicesoutside hospitals – and the more moneyspent in the community, the better theoverall health of the population becomes.• Equally, some health services in NWLondon are delivered from very modern,up-to-date facilities which have the latesttechnology. Clearly it would be a poordecision not to make the most of thesebuildings, especially at a time when theNHS cannot afford to find and buy newland and build new hospitals.the way we deliver services and by doingwhat we can to reduce demand forservices. Unless things change, we predictthat most of the hospitals in NW Londonwill end up in financial difficulties.• It would be wrong to say the NHS, andthese proposed changes, are drivenmainly by the need to save money. We areactually first and foremost driven by thechallenge of delivering high-quality care.But money is an important consideration.Financial challenges• Not surprisingly, looking after such alarge population with so many healthneeds costs a lot of money and theNHS currently spends approximately£3.6 billion a year in NW London – some24% of all NHS spending in London. Butas we all know, the world, the UK andLondon are facing particularly difficulteconomic times right now. Although theGovernment has promised to protecthealth budgets, the amount of moneyavailable to the NHS in real terms is likelyto increase only very slightly in the yearsup to 2015.• In other words, keeping up with newtechnology and better treatmentsand managing the health needs of apopulation that is getting older meansthat the NHS needs to find an extra£20 billion a year by 2015. In NW Londonwe estimated that by 2014/2015 wewould need an extra £1 billion a year.However, we already know that there isn’tanywhere near this amount of moneyavailable. We have to find savings of atleast 4% a year – something which hasnever been done by the NHS before – bybecoming more productive, by changingThe challenges facing the NHS in NW London17
3. What will happen if wedo nothing?Even with all the challengesfacing the NHS, why is there aneed for such drastic change?Surely the extra money should just be found,more doctors and nurses recruited, buildingsrepaired and more community facilitiesbuilt? Then what is now pretty good, wouldbecome very good. If only it were that easy.Unfortunately, the situation facing the NHSin NW London is a lot worse than this, andneeds more drastic solutions. The fact is, ifnothing is done within the next few years,some major things will start going very badlywrong with the NHS in NW London:• Inequalities would continue and perhapsget worse. Currently people in some partsof NW London die on average 17 yearsearlier than those in nearby areas. This isneither fair nor reasonable and we needto try to reduce those differences.• People would continue to dieunnecessarily. A recent study showedpatients treated at weekends andevenings in London hospitals – whenfewer senior doctors are available – standa higher chance of dying than if theyare admitted during the week. We needa system that allows all of our hospitalsto benefit from having senior, expertconsultants on-site at all times.• Our dependency on hospital serviceswould continue when this is not the bestuse of resources – resources which couldbe better used to help people to stay wellin the community. The issue of the currentpoor state of many of our buildings wouldnot be dealt with – two-thirds of ourhospital buildings need upgrading.• Existing hospital trusts would be undersevere financial pressure, which meansthey could literally run out of money.And while the NHS can cope with somefinancial losses, this is obviously farfrom ideal and the deeper ‘into the red’that trusts go, the more difficult it is tokeep services running, to keep staff andmaintain morale, and to provide highqualitypatient care. As there is a limit tothe money available, some of the hospitalsin NW London would simply have to stopproviding services. Crucially, this wouldhappen in a disorganised way – meaning aworse effect on patients and staff.• There would also be problems with theNHS workforce. As it is, some serviceshave already had to be reduced becausethere are not enough clinicians to providethem safely. Recruiting and keepingclinical staff in London is always achallenge and if we do not offer the bestplaces to work, and the best places totrain, we will not attract the best staff.Equally, if there are not enough seniorstaff, trainee doctors can’t be supervisedand are withdrawn from the hospital. Allthis means patients will not get the bestcare, and services will be reduced.18 What will happen if we do nothing?
While this may sound alarming, it is worthnoting that many clinicians working for theNHS in NW London feel that we have notexplained in strong enough terms whatwould happen if we did nothing. Thoughservices are mostly providing good standardsof care at the moment, they cannot do so formuch longer and it will be patients, and theclinicians who treat them and care for them,who will be the first to feel the consequences.1Do you agree or disagree that there areconvincing reasons to change the waywe deliver healthcare in NW London?2What comments, if any, do you have onany of the issues raised in sections 1, 2or 3 of this consultation <strong>document</strong>?What will happen if we do nothing?19
4. So what is the answer?Those of us leading the NHSin NW London – its leadingGPs, hospital doctors, nurses,pharmacists and others – donot believe that things shouldjust be allowed to deteriorate.We do not believe that allowing unplannedcuts to services is the best way to managethe NHS either now, or in the <strong>future</strong>. It wouldbe highly irresponsible not to act in thesecircumstances.So, we have developed a vision for how wewant health services to be developed andimproved. Importantly, we have involvedpatient groups and representatives indeveloping this vision. In this consultation wewant to find out what you think.We have based this vision of care onimprovements and innovations which arealready being made in many parts of NWLondon and the rest of the country. This isimportant because it means the changes aretried or tested ways of delivering healthcare– we already know that they work, that theyimprove care and that they can be delivered.20 So what is the answer?
Example Stroke servicesLondon has made giant strides in tackling oneof the biggest killers – stroke – over the lastfew years. Just three years ago, stroke carewas spread across the city, with all 31 acutehospitals trying to deliver it.Now, a dedicated network of eight hyper-acutestroke units provide the immediate, specialistcare that stroke patients need – in NW Londonthese include Northwick Park Hospital andCharing Cross Hospital – and another 24 strokesupport units around London provide ongoingcare once a patient is stabilised.This is estimated to have prevented around400 deaths in London and 100 in NW Londonevery year since the changes were made andproves an important principle – that hospitalcare for certain conditions is much betterwhen centralised at a specific, limited numberof specialist sites.There was of course some opposition to thischange when it was suggested as it meantthat some hospitals ‘lost’ services. However,it is now clear that it is much more importantthat an ill patient gets to the best placewhich has the right, expert consultants andsurgeons, even if it means driving straightpast their nearest hospital.Example Integrated care pilotA major frustration of patients with longtermconditions is that their care is not wellmanaged across different NHS organisations.So an integrated care pilot (ICP) was set upin Westminster, Kensington and Chelsea,Hammersmith and Fulham, and in partsof Ealing and Hounslow to look into this,concentrating on people aged over 75,or with diabetes.The ICP makes sure hospitals, communitycareservices, social care and local authoritiesall work as a team, so patients receiveco-ordinated care across different services.It has proved so successful that it has wonnational awards for its pioneering work.The ICP shows what can be done outsidehospitals, particularly when the various healthand social care teams in a community pulltogether for the benefit of the patient. It isnow being expanded to include all boroughsin NW London and to includemore conditions.The GP practices taking part in the pilot haveso far reduced emergency admissions tohospital for elderly people by 7% and havecreated 20,000 individual care plans fortheir patients.So what is the answer?21
5. Our vision for healthcarein NW LondonSo we can make sure thathealth services do notdeteriorate severely in the<strong>future</strong>, we have a vision that inNW London you will have:• the support you need to take better careof yourself;• a better understanding of where, whenand how you can be treated;• the tools and support you need to bettermanage your own medical conditions;• easy access to primary care providers,such as GPs, 24 hours a day, seven daysa week; by phone, email or in person –when you need to be seen urgently• fast and well-co-ordinated access tospecialists, community and social careproviders, (this access will be managed byGPs); and• properly maintained and up-to-datehospital facilities with highly trainedspecialists available all the time.There are three major principles that sum upour vision for the NHS in NW London.They are:• localising routine medical care (deliveringas much care as possible, as soon aspossible, in convenient places which areeasy to access);• centralising the most specialist services(bringing more services together on anumber of specific sites); and• integrating care between primary,secondary and social care providers(making sure all parts of the NHSand social services work more closelytogether).Our vision of careThree main principles formour vision for care1 LocalisingLocalising routine medicalservices means better accesscloser to home and improvedpatient experience2 CentralisingCentralising most specialistservices means better clinicaloutcomes and safer services forpatients3 IntegratedWhere possible, care should beintegrated between primary andsecondary care, with involvementfrom social care, to give patientsa co-ordinated service22Our vision for healthcare in NW London
3Please say how important you think it isthat we should aim to make sure thatyou and everyone else in NW London willhave each of the following:a) The support you need to take bettercare of yourselfb) A better understanding of where,when and how you can be treatedc) The tools and support you need tobetter manage your own medicalconditionsd) Easy access to primary care providers,such as GPs, 24 hours a day, sevendays a week; by phone, email or inperson – when you need to be seenurgentlye) Fast and well-co-ordinated access tospecialists, community and social careproviders (this access will be managedby GPs)f) Properly maintained and up-to-datehospital facilities with highly trainedspecialists available all the timeOur vision for healthcare in NW London23
6. World-class healthcareoutside of hospitalThe vision for care outsideof hospital developed by theNHS and particularly our localGP leaders is based on theprinciples of localisationand integration (see section 5).the need for emergency and urgent care ata later stage. This approach, with differentproviders delivering care in an integratedpackage, will help people get better morequickly so they can get on with their lives.IntermediatecareRehabilitationHospitaldischargeCare outside hospital includes all thoseservices provided in community settings suchas in your home by community nurses, atyour GP’s surgery and in health centres. It alsoincludes all the ways that you can look afteryourself better.This means delivering as much care aspossible which is local to you at a convenienttime – so either in your home or at your GP’ssurgery, for example, or even in your localhospital. By offering a much wider range ofhigh-quality services within the community,we can make sure people have easier andearlier access to care.Your GP practice will be at the heart ofdelivering an integrated service, using arange of providers. With more co-ordinatedprimary health and social care services, yourGP practice will co-ordinate care across allservices and have overall responsibility foryour health. GPs and other primary-careprofessionals will be able to pick up onhealth issues at an earlier stage, and providetreatment that prevents patients ending upin hospital. This kind of planned care avoidsEnd-of-lifecareSpecialists incommunityLinked ITCarenavigatorsCare planco-ordinatorsCasemanagementof long-termconditionsGPpracticeHealth andsocial careco-ordinatorsSingle pointof accessCommunitynursingservices111Rapid responseto urgentneedsUrgent careservices(urgent carecentres, walk-incentres)To make sure that the quality of care improves,every care provider will have to keep tohigh standards of care. The new clinicalcommissioning groups, the organisationsthat are being led by GPs to plan healthcareservices, will work with partners includinghealth and well-being boards to make sure thestandards are kept to.The leaders of all the eight clinicalcommissioning groups in NW London havemade the same commitment to change howprimary and community care is delivered,based on four main quality standards.24 World-class healthcare outside of hospital
Quality standards for care outside hospital (please see note below)Individual Empowermentand Self-CareAccess, Convenienceand ResponsivenessCare Planning andMulti-Disciplinary CareDeliveryInformation andCommunicationIndividuals will be provided with up-to-date, evidence-based and accessibleinformation to support them in taking personal responsibility when makingdecisions about their own health, care and wellbeing.Out-of-hospital care operates as a seven day a week service. Communityhealth and care services will be accessible, understandable, effective andtailored to meet local needs. Service access arrangements will include face-toface,telephone, email, SMS texting and video consultation.Individuals using community health and care will experience co-ordinated,seamless and integrated services using evidence-based care pathways, casemanagement and personalised care planning. Effective care planning andpreventative care will anticipate and avoid deterioration of conditions.With an individual’s consent, relevant parts of their health and social carerecord will be shared between care providers. Monitoring will identify anychanging needs so that care plans can be reviewed and updated by agreement.By 2015, all patients will have online access to their health records.Note: Plain English Campaign’s Crystal Mark does not apply to these standards as they were agreed by the leaders of the eightclinical commissioning groups in NW London before this consultation <strong>document</strong> was written.Delivering this vision will:• improve access to GPs and to other servicesso patients can be seen more quickly andat a time that is convenient to them;• mean more people can take control oftheir own health conditions;• help carers to support those with healthand social care needs;• mean that healthcare providers andpatients will be able to access informationabout patients’ health, so reducing possibleerrors and avoiding patients having to givethe same information many times;• deliver co-ordinated care plans for people,preventing deterioration in health andreducing admissions to hospital; and• reduce complications and poor outcomesfor people with long-term conditions byproviding more specialist services in thecommunity.How far do you support or oppose thestandards that have been agreed forcare outside hospital?4aWorld-class healthcare outside of hospital25
7. Making hospitalscentres of excellenceOur vision for hospital care isbased on centralising services– that is, bringing moreservices together on fewersites to create a greater levelof expertise so that we canprovide better care and savemore lives.It has been shown that having more expertiseand more senior doctors available in hospitalsimproves the outcome for patients. Asshown in section 4, we know that thisapproach works, based on what has beendone to centralise heart-attack care, majorarterial surgery, stroke care and traumacare in London. Other countries around theworld have used exactly the same approachsuccessfully.In NW London however, as explained insection 2, not enough services have beencentralised, leaving some hospitals withstretched senior medical cover and notenough expertise – particularly at theweekends and at night. Across NW London,the quality of hospital care differs too much.It sometimes meets high standards, but quiteoften it does not and this can, in the worstcases, lead to unnecessary deaths.Clinicians have looked closely at this and atthe latest research and evidence and believeit is clear that by centralising certain services,patients will have better outcomes. This maymean reducing recovery time, preventingrelapse or the need to go back to hospital or,in the most extreme cases, saving lives.Naturally, people may be concerned abouttravel times. It is important that we canstill provide emergency care close to, or at,the scene of an accident. However, oncesomeone is being treated by an ambulancecrew, the time it takes to get to hospital ismuch less important. These days so muchmore care can be provided at the scene ofaccidents, actually within ambulances, or inthe community. And, of course, ambulancesdo not station themselves at hospitals, but atmore spread-out locations to provide the bestcover for a certain area.Outcomes for patients improve much more ifthey are taken to the right place for treatmenteven if this is not the place nearest to wherethey were taken ill. This is already happeningin some situations and is getting excellentresults. For example, in a major accident thathappened anywhere in NW London, theambulance crew would stabilise the patientand then take the patient straight to the besthospital to treat their injuries, even if it meantdriving past several hospitals on the way.The big difference that centralising servicesmakes is that it means we can provide accessto senior doctors and lots of back-up services24 hours a day, seven days a week. Traveltimes need to be within an acceptable limit,but are not as critical as they used to be26 What Making this hospitals <strong>document</strong> centres is forof excellence
in deciding exactly where services such asemergency care should be located.Centralising services onto fewer, more specialistsites also has important benefits for trainingclinicians. Academic and training institutions,such as medical specialties, work best whenthey are located closer together. Sharingideas, innovations, new technology and newtechniques becomes much easier. This is whythe most successful health education andresearch institutions all over the world, as inLondon, are often ‘clustered’ together arounda well-known campus or area.NW London has some excellent centres ofacademic and medical institutions already –such as the Academic Health Science Centre,covering Imperial College and ImperialCollege Hospital Trust in West London,and the specialist services in Chelsea andWestminster Hospital which cover heart, lungand cancer services. Making sure we build onthis excellence is important to us. We want tomake sure we not only have a current, highlyskilled workforce which is able to deliver thebest services, but that we can protect thatworkforce for <strong>future</strong> generations.To make sure that the quality of care isimproved, every provider will have to meethigh clinical standards of care. The local GPcommissioners will monitor this. All hospitalsin NW London will have to meet thesestandards, which we have agreed.Quality standards for hospital care (please see note 1 below)Emergency Surgery and A&EAccess tosenior andspecialistskillsAccess todiagnosticsand multiprofessionalteams• All emergency admissions to be seen and assessed by a relevant consultant within 12hours of the decision to admit or within 14 hours of the time of arrival at the hospital• Acute medicine inpatients should be seen twice daily by a relevant consultant• When on-take for emergency / acute medicine and surgery, a consultant andtheir team are to be completely freed from any other clinical duties / electivecommitments that would prevent them from being immediately available• Any surgery conducted at night should meet NCEPOD (National Confidential Enquiryinto Patient Outcome and Death) requirements and be under the direct supervisionof a consultant surgeon• All hospitals admitting emergency general surgery patients should have access to anemergency theatre immediately and aspire to have an appropriately trained consultantsurgeon on site within 30 minutes at any time of the day or night• The Critical Care Unit should have dedicated medical cover present in the facility 24hours per day, seven days per week• All hospitals admitting medical and surgical emergencies should have access to all keydiagnostic services (e.g. interventional radiology) in a timely manner 24 hours a day,seven days a week, to support decision making• Prompt screening of all complex needs inpatients should take place by a multiprofessionalteam which has access to pharmacy, psychiatric liaison services andtherapy services (including physiotherapy and occupational therapy, seven days a weekwith an overnight rota for respiratory physiotherapy)• Single call access for mental health referrals should be available 24/7 with an aspiredmaximum response time of 30 minutesProcesses • The majority of emergency general surgery should be done on planned emergencylists on the day that the surgery was originally planned and any surgery delaysshould be clearly recorded• On a site without 24/7 emergency general surgery cover, patients must betransferred, following a clear management process, to an Emergency Surgery site ifa surgical emergency is suspected without delayMaking hospitals centres of excellence27
MaternityPaedatrics• Women with complex medical conditions must be offered assessment by a consultant obstetrician• Units with more than 6000 births a year should provide 168 hours of consultant presence (24/7)• Units with between 2500 and 6000 births a year or classed as high risk should provide 98 hours aweek of consultant presence (please see note 2 below)• Units with up to 2500 births a year are strongly recommended to have 40 hours of consultantobstetric presence but should conduct a risk assessment exercise to determine their individualrequirements• Outside the recommended minimum 40 hours of consultant obstetrician presence, the consultant willconduct a physical ward round as appropriate at least twice a day during Saturdays, Sundays and bankholidays, with a physical round every evening, reviewing midwifery-led cases following referral• All women’s care should be co-ordinated by a named midwife throughout pregnancy, birth and thepostnatal period. Where specialist care is needed this should be facilitated by her named midwife.Clinical responsibility for women with complex care needs should remain with the specialist, butthese women should still receive midwife-co-ordinated care• Consultant-delivered obstetric services should include a co-located midwife-led unit to provide bestcare and choice for women and babies. Women should be able to choose the option of an out ofhospital pathway (home birth and standalone midwife-led unit) if appropriate• Obstetric units will need support from different services, including onsite access to emergencysurgery (some have argued this can be provided by emergency gynaecological surgery cover),interventional radiology, and critical care, in addition to support from an onsite neonatal inpatientunit but not necessarily paediatrics• There must be 24-hour availability in obstetric units of a clinical worker fully trained in neonatalresuscitation and stabilisation of a new born baby for immediate advice and urgent attendance• Midwifery staffing levels are calculated and implemented according to birth setting and case mixcategories to provide a one-to-one midwife-to-woman standard ratio during active labour withimmediate effect• There must be access to emergency theatre when required• All paediatric inpatient admissions to be seen and assessed by a relevant consultant within 12 hoursof the decision to admit or within 14 hours of the time of arrival at the hospital• When on-take for emergency and acute paediatric medicine and surgery, a consultant and theirteam are to be completely freed from any other clinical duties or elective commitments that wouldprevent them from being immediately available• All inpatient paediatric services units need to have paediatric consultant availability within 30 minutes• Paediatric inpatients should be seen twice daily by a paediatric consultant• Paediatric Assessment Units (PAUs) should have clearly defined responsibilities, with clear pathways,and should be appropriately staffed to deliver high quality care as locally as possibleNote 1: Plain English Campaign’s Crystal Mark does not apply to these standards as they were agreed by our clinical leadersbefore this consultation <strong>document</strong> was written.Note 2: Royal College guidance says that units with over 5000 births a year should provide 168 hours of consultant presence.Over time local maternity units in NW London will move to meet this standard.Delivering this vision will:4b• save lives by providing better access tomore senior doctors for more of the time;• mean that people will be treated morequickly by more senior doctors, leading tofewer complications; and• allow doctors to develop their specialistskills, so they can provide the bestpossible specialist care.How far do you support or oppose thestandards that have been agreed forcare in hospital?28Making hospitals centres of excellence
Making hospitals centres of excellence29
8. What will our visionmean for you?A main part of this vision is thatall the different parts of the NHSsystem will work together muchmore closely and effectively –whether they are hospitals, GPpractices, community providers,or local authorities providingsocial services.It will mean all these organisations, theirleaders and workforces working acrossboundaries and without barriers, and as aresult, patients in NW London all receivingbetter care.In short, the vision will mean:• you can be supported to take bettercare of yourself, lead a <strong>healthier</strong>lifestyle, understand where and whenyou can get treatment if you have aproblem, understand different treatmentoptions and better manage your ownconditions with the support of healthcareprofessionals if you prefer;• you can easily see a GP or communitycareprovider 24 hours a day, seven days aweek by phone, email, or face-to-face inlocal, convenient facilities;• you will be able to see a specialist orreceive support from community orsocial care services if necessary (thiswill be organised quickly and GPs willbe responsible for co-ordinating yourhealthcare); and• if you need to go into hospital, it will bea properly maintained and up-to-datehospital where you receive care fromhighly trained specialists, available sevendays a week, who have the specific skillsneeded to treat you.The following stories show how care willimprove for typical NW London patientsbefore and after the proposed changes areput in place.Do you agree or disagree that someservices which are currently delivered inhospital could be delivered more locally?How far do you support or oppose theidea of bringing more healthcare servicestogether on fewer sites?What further comments, if any, doyou have on any of the issues raised insections 4, 5, 6, 7 or 8 of this consultation<strong>document</strong>? (For example, if you disagreewith our proposals, why is that?)56730 What this will <strong>document</strong> our vision mean is for for you?
Easy access tohigh-qualitycareMelanie is 36. She is a workingmother with a young daughterwho has a fever.Now• Melanie rings her GP but cannotget through, and takes Maya toA&E.• The traffic is heavy and aftera stressful journey they finallyarrive. Maya is quickly assessedbut not classed as high risk.• After three hours they finally seea doctor who diagnoses thatMaya is teething.Future• Melanie rings 111 and is givenadvice and an appointment forthat evening at a local practicewith extended hours, or aprimary care centre by GP’s outof-hoursservice.Simplerplanned carepathwaysMaria is 48. She has made anurgent appointment with herGP after bleeding vaginally forthe last two days.Now• Maria sees her GP, who is notsure of the best treatmentoptions and refers her to anoutpatient clinic.• Maria has an appointment andis scheduled for a follow-upappointment which takes severalweeks to arrange.• The results are not sent toher GP.Future• Maria sees her GP who booksher for a one-stop assessmentand diagnosis on-site.• Two hours later the GP checkson the results and phonesa consultant for a specialistopinion and together they agreeon an appropriate procedure.Quickresponses tourgent healthproblemsArchie is 80. A family memberhas taken him to the doctor ashe is in some pain and havingdifficulty passing urine.Now• The GP has diagnosed Archie ashaving a urinary tract infection.He is given a course of oralantibiotics and sent home.• The next day his son visits andfinds Archie in a confused state.Unsure what to do, he takesArchie to A&E.• The strange surroundings makeArchie more confused and he isadmitted.• Three weeks later, Archie is stillin hospital and his mental statehas deteriorated.Future• The GP has left a contactnumber for the rapidresponse service, following hisappointment.• Archie’s son visits and findsArchie in a confused stateand rings the rapid responsehelpline.• A GP, social worker andphysiotherapist from the rapidresponse team arrive and assessArchie at home, authorising aseven-day package of care tostabilise him at home.Co-ordinatedcare forpeople witha long-termconditionSameera is 45. She sees her GPcomplaining of shortness ofbreath and tightness in her chest.Now• After visiting her GP, Sameerais diagnosed with chronicobstructive pulmonary disorder,is put on an inhaler and given astronger dose of drugs.• Sameera continues to struggleat home with her condition andafter a series of complications isadmitted to A&E.Future• Sameera’s GP thinks she needsan integrated care plan and heraises this at a case conferencewith a specialist chest doctor.• They identify that Sameeraneeds advice on how to use herinhaler properly, rather than astronger dose of drugs.Less timespent inhospitalDavid is 80. He has recentlyfallen, fractured his hip andbeen admitted to hospital.Now• Following treatment, David’ship is mending well so the dutydoctor reviews his case and sayshe is fit to leave following aphysiotherapist’s review.• The review happens on a Fridayand physiotherapists are notavailable until Monday, leavingDavid in hospital over theweekend.• Social care takes three weeks toorganise a package of care forwhen David leaves hospital.Future• When David is admitted tohospital his history is availableto staff.• His health and social careco-ordinator is told andplans to discharge him beginimmediately.• The next steps are recorded ina clear care plan and everythingis in place for when the timecomes for David to leavehospital.What will our vision mean for you?31
9. Delivering the visionIf we are to deliver this newvision for health services acrossNW London, a lot needs to bedone, and major changes needto be made to the way the NHScurrently works.Of course this will not be easy, nor will it bevery popular among certain groups of people orcommunities. People understandably get veryattached to local hospitals, whether they livenearby, have been treated there, or work there.But that does not mean it is wrong to changeservices – healthcare is constantly changing,as are the ways it is delivered, where it isdelivered from, and who delivers it. So whilepeople feel strongly about local health services,this does not mean it is wrong to change theservices. But it does mean we should makethese changes thoughtfully, carefully, and byconsulting patients – and many of you readingthis <strong>document</strong> – first.Changes, above all, must lead to improvementsin the quality of care and so it is important thatGPs, hospital clinicians, nurses, communityservice staff and others lead the way in howthese changes are designed and put in place.Clinicians need to work with patients andpatient groups and senior managers to makesure that proposals are good for patients as wellas being realistic.Delivering this vision will also significantlyimprove the finances of the NHS in NWLondon. It will take at least three years to deliverthis vision and lots of work has been done tomake sure the NHS can afford it. Delivering thevision for care outside hospitals will cost up to£120 million. On top of this, it is estimated thatit will cost between £60 million and£90 million to run new and old services atthe same time while changes are made.However, once made, the changes will meanthat hospitals in NW London will be in a muchimproved financial position than if we donothing. The pre-consultation business case(volume 1, chapter 6) available on our websiteat www.<strong>healthier</strong>northwestlondon.nhs.ukcontains more detail on this financial analysis.In the rest of this <strong>document</strong>, we describe:• which services will be delivered where;• how we will deliver the vision for servicesoutside hospital;• what services will be delivered in whichtype of hospital;• how many hospitals we believe we needin NW London;• the process we have used to recommendwhere these hospitals will be; and• three different options for where thesehospitals should be.32 Delivering the vision
Delivering the vision 33
10. Where will care beprovided in <strong>future</strong>under the proposals?We have looked at the way inwhich we deliver healthcare,particularly the settings wherewe can deliver it, and haveidentified eight differentsettings for care.Home – some services can beprovided in people’s homes, forexample through nursing care ortelephone support services.GP practice – GP practices canprovide lots of services otherthan GP appointments, such asimmunisations, screening, bloodtests and therapy services.Care network – there are someservices that can be provided by GPpractices but we need practices togroup together so there are enoughpatients to make it cost-effective to providethe skilled workforce and specialist equipmentneeded. This includes some diagnostic tests(such as ECGs) and therapies, and servicesfor some long-term conditions. Groupingpractices together can also mean urgent casescan be seen within four hours.Health centre – sometimes abuilding is needed to provide‘networked’ GP services such astherapy, rehabilitation or specialist imagingequipment.Local hospital – this type ofhospital provides all the mostcommon things people needhospitals for, such as less severeinjuries and less severe urgent care, nonlifethreatening illnesses, care for mostlong-term conditions such as diabetes andasthma, and diagnostic services. It basicallyprovides the kinds of services that mostpeople going to hospital in NW Londoncurrently go there for.Major hospital – this is theclosest to what is currentlyknown as an ‘acute’ or districtgeneral hospital, and providesmost types of care, right up to highly complexand urgent services. Major hospitals alsoprovide care for children and maternityservices, since these both sometimes needcomplex emergency services. In theseproposals these hospitals will have moresenior clinicians and specialist services thannow – they will have investment so thatthey can be better than our current ‘acute’hospitals. If patients at a local hospitalsuddenly need more urgent or complex care,they will be transferred by ambulance tothese major hospitals. Major hospitals willalso provide local hospital services.Elective hospital – this hospital iswhere you go if you need an operationwhich is not urgent, so it could be34 Where What this will <strong>document</strong> care be provided is for in <strong>future</strong> under the proposals?
8planned (or ‘elected’) by you or your doctorto happen when necessary. These hospitalscover things like hip replacements and cataractoperations. They are particularly good places tobe treated because they are not disrupted byemergency cases which have to be dealt withbefore less urgent ones, and can more easily bekept clean and free from hospital infections.Specialist hospital – this is whereclinicians have specialised in treatingcertain conditions, for example canceror heart conditions or lung diseases.So you only tend to go to these places if youhave a condition which needs really specialistcare, perhaps because your condition isparticularly life-threatening or complex.The names of these eight settings of care andthe services associated with them have beendetermined by clinicians and commissioners inNW London. However, we recognise there is aconfusing array of different titles in use acrossLondon and nationally. The Department ofHealth is currently undertaking a piece of workon urgent and emergency care to support amore consistent approach across the country.Once the work is published, we will makesure that our proposals are aligned with theDepartment’s recommendations.We have described the proposalsto deliver different forms of care indifferent settings. How far do yousupport or oppose these proposals?HomeGP practiceCarenetworkHealthcentreLocalhospitalMajorhospital• GP, community and social careservices• Patient rings 111 for advice• Response within four hours• GP consultations• Management of long-termconditions• Health promotion and preventativeservices• Multi-disciplinary care• Diagnostic and therapy services• GP, therapy and rehabilitation anddiagnostic services• Specialist GP services• Urgent care centres• Outpatients and diagnostics• Further services including– specialist clinics– outpatient rehabilitation• A&E, urgent care centres andtrauma care• Emergency surgery and intensivecare• Obstetrics and midwifery unit• Inpatient paediatrics9What further comments, if any, doyou have on any of the issues raisedin sections 9 or 10 of this consultation<strong>document</strong>? (For example, do you haveany concerns about arranging care inthis way, or about the way we proposeto classify hospitals? Can you suggesta better way of delivering care?)ElectivehospitalSpecialisthospital• Elective surgery and medicine• Outpatients and diagnostics• High-dependency care• Highly specialised care such ascardiothoracics and cancerWhere will care be provided in <strong>future</strong> under the proposals?35
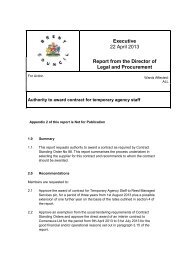
11. Proposals for deliveringcare outside hospitalsTo deliver the vision for careoutside hospitals, GP practiceswill work together to servetheir patients, making the bestuse of their skills and resourcesto improve access and quality.Networks of GP practices will work with otherhealth and social care providers to deliverco-ordinated services to the local community,improving care planning and local servicesand information and communicationstandards. We have developed plans showingwhere services will be provided.Hospital with urgentcare centrePossible site for localhealth centre, not on acurrent hospital site1. Mount Vernon2. Hesa health centre3. The Pinn4. Alexandra Avenue5. Grand Union Village6. Jubilee Gardens7. Featherstone Road8. Matlock Lane9. Wembley Centre10. Willesden Centre11. White City12. St Charles13. Earls Court14. Heart of Hounslow15. HestonBusiness case neededfor health centreA. Exact locationto be confirmedB. Church StreetC. East FitzroviaHounslow5 networks54 practicesHillingdon6 networks48 practices1Hillingdon21575146348EalingWestMiddlesexEaling6 networks79 practicesANorthwickPark9Harrow6 networks36 practicesBrent5 networks69 practices101211H&F4 to 5 networks31 practicesCentral MiddlesexHammersmith13BSt Mary’sCCharingCrossCentralLondon3 networks35 practicesChelsea andWestminsterWest London2 networks55 practices36 <strong>Shaping</strong> Proposals What this a for <strong>document</strong> <strong>healthier</strong> delivering <strong>future</strong> is for care outside Delivery hospitals of care outisde hospitals
Proposals for delivering care outside hospitals37
Within the home, GP surgeries, networks andhealth centres, we will deliver:• easy access to high-quality care, withlonger opening hours for GPs, and urgentcare centres open 24 hours a day, sevendays a week (these centres will see manyof the people who would currently go toA&E);• simpler planned care pathways (thedifferent stages of NHS care you may gothrough), with specialists available to giveadvice, more clinics in the communityfor common health issues and patientsable to have simple operations withoutneeding to go to hospital;• quick responses to urgent healthproblems, by setting up services in eachborough to prevent 16,000 patients fromhaving to go to hospital each year;although they may have to work differently inthe <strong>future</strong>. The full pre-consultation businesscase (volume 2, chapter 7) on our website,www.<strong>healthier</strong>northwestlondon.nhs.uk setsout the plans for developing the workforce inmore detail. There will also need to be an extra130 to 140 beds in the community.GP leaders in NW London have agreeddetailed plans for every borough to coverthese new services. Because the people wholive in each borough are different, services ineach borough will be different. You can findmore details of each borough plan for healthservices outside hospital on our website atwww.<strong>healthier</strong>northwestlondon.nhs.ukHow far do you support or oppose ourplans to improve the range of serviceswe deliver outside hospital?10• co-ordinated care for people with along-term condition, by setting up 38multi-disciplinary health and social careteams covering the whole of NW London(this will mean people with a long-termcondition will have a personal care plan);and• less time spent in hospital because careproviders will know when someone is inhospital and will make sure services are inplace for them to leave hospital as soonas they can.Up to £120 million will be invested in theseservices over the next three years, paid forout of savings made from working differently,to make sure that we can care for peopleoutside hospital. We have promised thatservices will be in place before changes aremade to hospital-based services.There will need to be between 750 and 900extra staff to run these new services. Many ofthese staff are already working in NW London,What further comments, if any, doyou have on any of the issues raisedin section 11 of this consultation<strong>document</strong>? (For example, whatcomments do you have on our plansto improve the range of services wedeliver outside hospital?)1138 Proposals for delivering care outside hospitals
Delivery of care Proposals outisde for hospitals delivering care outside hospitals 39
12. Our recommendationsfor local hospitals acrossNW LondonMost care that is currentlydelivered in hospitals willstill be delivered locally in alocal hospital, under changesproposed by ‘<strong>Shaping</strong> a<strong>healthier</strong> <strong>future</strong>’.The local hospitals in our plans will havespecialist staff (who may also work in a majorhospital) and specialist equipment and will beopen 24 hours a day, seven days a week to seepeople with urgent health problems. Specialiststaff will work with GPs and other communityclinicians to deliver personalised healthcare. GPservices, community services and social carewill be based in these local hospitals, bringingservices together around your needs.Local hospitals will also be part of the localcommunity. This means local patients, patientgroups, the voluntary sector, the local councilincluding the health and well-being board, andlocal clinicians will be involved in developingand running them. They will offer servicesbased on what is needed locally, so these mightbe different in each local hospital.The local hospital will also act as a ‘home’for local clinicians – a place for educationand training, for continuing professionaldevelopment, as a centre for research andfor clinicians and other professionals to cometogether to review and improve patient care.Local hospitals will offer slightly differentservices depending on the health needs of thedifferent local communities across NW London,but these services will include, for example,the following:• Quicker and more co-ordinatedhealthcare. The local hospital will providespecialist care for people with long-termconditions. Patients and carers will be ableto come together in self-care and supportgroups, either at the local hospital or closerto home. Some GP practices, communityservices and social services may be based inthe local hospital, and will make sure careis co-ordinated for individual patients.• Access to specialist skills. In some cases,patients may need specialist appointments.Many of these appointments will beavailable in local hospitals, including forpeople who are going to have, or havehad, an operation. Some patients, forexample, those with Parkinson’s diseaseor children who need insulin for diabetes,need a lifetime of specialist care, muchof which will be available at the localhospital. Also, some local hospitals will beable to provide treatments such as medicaloncology, renal dialysis and simple surgery.• Tests. Clinicians sometimes need tests sothey can find out what is wrong with apatient or understand whether a treatmentis working. Tests such as x-ray, ultrasound,endoscopy or MRI scans will be available insome local hospitals.40 Our What recommendations this <strong>document</strong> is for local hospitals across NW London
• Bringing services together. The localhospital will bring services together forpatients. This could include assessments,transport to and from home and painmanagementservices. This will make iteasier for patients to get to services and forclinicians to find out what is wrong withthe patient and treat them.• Better nursing, therapy andrehabilitation services. Local hospitalswill offer better nursing, therapy,rehabilitation and community servicessuch as physiotherapy, well-baby clinics,chiropody and wound clinics. This willinclude appointments with specialists. Itmight also include beds for patients whoare at risk of deteriorating, and beds forpatients who have been to a major hospitalbut who no longer need specialist care andcan be cared for nearer to their home.Urgent care centresLocal hospitals will have an urgent carecentre, open 24 hours a day, seven daysa week. Urgent care centres specialise intreating patients with urgent illnesses andinjuries and conditions that can be seen andtreated without the patient having to stay inhospital.Clinicians in urgent care centres will alsobe skilled in stabilising patients who needto be transferred to more specialist A&Ecentres. There will be special processes tomake sure these transfers happen quicklyand some urgent care centres may also havebeds where patients can be admitted if theirproblem can be dealt with locally.NW London has led the way with some ofthe most successful urgent care centres inLondon. The centres are staffed by GPs andnurse practitioners. Many of these urgentcare centres are inside A&E departmentsand are already treating a wide range ofpatients. People who go there get a veryhigh quality of care. Patient satisfaction ishigh and waiting times are low. Today, thereare different ‘models’ of urgent care centresin NW London and the proposed changeswould encourage higher standards of urgentcare centres across the area. For example,urgent care centres in NW London currentlyhave different opening times and treatdifferent problems. This can be confusingfor patients and we will make sure that, in<strong>future</strong>, all urgent care centres in NW Londonare open 24 hours a day, seven days a weekand all have the same level of services.We want all urgent care centres in NWLondon to:• see and treat patients within four hours ofthem arriving;• be led by primary-care clinicians suchas GPs;• be linked with other services such as thenew non-emergency phone number forthe NHS (111); and• have access to tests and specialistclinicians.The kinds of health problems all urgent carecentres would be able to treat include:• illnesses and injuries not likely to need astay in hospital;• x-rays and other tests;• minor fractures (breaks);• stitching wounds;• draining abscesses that don’t need ageneral anaesthetic; and• minor ear, nose, throat and eye infections.Our recommendations for local hospitals across NW London41
Urgent care centres will see people andchildren of any age.It is important to note that urgent carecentres do not treat problems such as majorburns, head injuries, strokes, sickle-cell crisis,severe shortness of breath, heart failure,overdoses and self-harm. All these problemscan be a sign of serious conditions that mayneed to be treated in a major hospital.The best example in London of a localhospital is Queen Mary’s Hospital inRoehampton, North East Wandsworth, whichis described in the pre-consultation businesscase (volume 2, chapter 8) on our website atwww.<strong>healthier</strong>northwestlondon.nhs.uk. StCharles’ Centre for Health and Wellbeing inLadbroke Grove in NW London also providesmany local hospital services, including anurgent care centre. The patients who usethese services rate them very highly and theyare an important part of the local community.The kinds of services we want to see providedin local hospitals are currently deliveredat all nine acute hospitals in North WestLondon (Charing Cross Hospital, Chelseaand Westminster Hospital, Central MiddlesexHospital, Ealing Hospital, HammersmithHospital, Hillingdon Hospital, NorthwickPark Hospital, St Mary’s Hospital and WestMiddlesex Hospital). Our proposals would seeall these hospitals continuing to provide localhospital services, including an urgent carecentre and outpatient and diagnostic services.Do you agree or disagree that localhospital services such as urgent carecentres (those open 24 hours a day,seven days a week) and outpatientappointments should continue to beprovided at the nine acute hospitals inNorth West London that currentlydo so?How far do you agree or disagree withour plans for urgent care centres?What further comments, if any, doyou have on any of the issues raisedin section 12 of this consultation<strong>document</strong>? (For example, if youdisagree with our proposals, whatwould you do differently?)12131442 Our recommendations for local hospitals across NW London
13. Elective hospitals usingour high-quality buildingsIf our proposals are agreed,elective hospitals would carryout operations on patientsin NW London which aredescribed as ‘elective’ ratherthan ‘urgent’ – such as hipreplacements, and cataractoperations.In an elective hospital, treatment is notdisrupted by emergency cases – which cantake priority over less urgent ones at othertypes of hospital – and, partly because of this,they can more easily be kept clean and freefrom hospital infections.Elective hospitals can be located within, orindependently of, major hospitals as theydo not rely on any of the back-up servicesof a major hospital. We are proposing thatwe should use any high-quality buildingsthat have spare space to house our electivehospitals. This would particularly include thebuildings at West Middlesex Hospital andCentral Middlesex Hospital, which havebeen built especially to deliver high-qualityelective care.Major hospitals would still continue toprovide elective services and patients wouldstill be able to choose where they hadtheir operation.How far do you support or oppose ourrecommendation that we should useour high quality hospital buildings withspare space as elective hospitals?What further comments, if any, doyou have on any of the issues raisedin section 13 of this consultation<strong>document</strong>?1516Elective hospitals using our high-quality buildings43
14. Five major hospitals forNW LondonIn developing a vision forhospital services, we focusedon different areas: emergencysurgery, A&E, maternity(pregnancy and birth), andpaediatrics (children).Doctors often need these specialised areas tobe based in the same hospital to treat certainconditions.Under our proposals, major hospitalswould provide a full range of high-qualityclinical services for patients with urgentor complicated needs (or both). They willhave investment to equip and staff an A&Edepartment (open 24 hours a day, seven daysa week) with urgent surgery and medicine anda ‘level 3’ intensive care unit. Major hospitalswould usually also provide consultant-ledmaternity services and radiology services. Theymay also have complicated surgery, a hyperacutestroke unit (HASU), inpatient paediatrics(children), a heart attack centre and a majortrauma centre.In NW London each major hospital wouldalso provide local hospital services, includingan urgent care centre.major hospitals would be needed to:• deliver the clinical standards shown insection 7;• deliver them within a realistic timewithout affecting the high quality ofservices; and• be financially affordable.We looked at all the evidence and agreed theideal number of major hospitals would befive. This is for the following reasons.• Having six or more major hospitals wouldsolve some of the problems we face inNW London as shown in section 2. Butthere would still be too many hospitalsbecause we would not be able to recruitenough clinicians to provide servicessafely enough for six or more hospitals.We cannot solve this problem by hiringmore clinicians because clinicians needexperience of dealing regularly withcomplications to keep up their expertise –and there are not enough cases of certaincomplicated conditions to do this in NWLondon.We looked at how many major hospitals wewould need in NW London to deliver thehighest-quality care. We used a set of ‘hurdlecriteria’ (a series of tests) to help us decide.To pass these tests, we looked at how many44 Five What major this <strong>document</strong> hospitals for is for NW London
• A good example of this is the number ofsurgeons needed to provide the highestquality of emergency surgery. We knowthat having senior surgeons available atnight and at the weekends means betterhealth outcomes for patients. Today, thereare only 45 surgeons working in NWLondon, but we would need at least 60surgeons to meet the clinical standards atsix hospitals.Number of beds needed for each majorhospital if there are five or fewerhospitals in the areaThree majorhospitalsAbout 800 to1000Four major hospitals About 600 to 700Five major hospitals About 500 to 600Minimumnumber ofsurgeons forclinicalstandardsCurrent number of bedsNorthwick ParkCharing Cross498576Hillingdon408X 9Hammersmith407Current45 currentSt Mary’s399Ealing327X 6About 60FTEWest MiddlesexChelsea and Westminster323311Central Middlesex233X 5About 50FTEX 4X 3FTE = Full-time equivalentAbout 40FTEAbout 30FTE• To begin with, some cliniciansrecommended that we should havefour or fewer major hospitals but it wasagreed that this would not be enough.This is because we would have to buildmuch bigger hospitals and move lots ofservices which would be high risk, difficultto deliver, and expensive. For example,if there were only three major hospitalsin NW London, we would need to buildhospitals that are twice the size of theones we have now.We agreed that all A&E departments wouldneed a maternity service as part of backupservices. And we agreed that maternityservices need the back-up of a major orspecialist hospital and so should not be put inother types of care settings (for example, localhospitals). We propose that all major hospitalswill have a consultant-led maternity unit.To give women in NW London more choiceabout where they give birth, the new majorhospitals would also have a midwife-ledmaternity unit. We are not suggestingthat we have any midwife-led units in NWLondon that are not within major hospitals.You can see the explanation for this in thepre-consultation business case (volume 2,chapter 8) which you can find on our websitewww.<strong>healthier</strong>northwestlondon.nhs.uk. Allmaternity services will work to support womenwho choose to have their baby at home.Five major hospitals for NW London45
Maternity services also need a paediatric(children’s) service to provide support for newbabies. So we propose that all major hospitalsin NW London in <strong>future</strong> will have an inpatientpaediatric service, unless there are enoughspecialist maternity services to support apaediatric consultant rota. The only hospitalwhere this is possible in NW London currentlyis at Queen Charlotte’s and Chelsea Hospitalat Hammersmith Hospital. We propose thatwe should keep the consultant-led maternityunit at Queen Charlotte’s and ChelseaHospital. This means there would be sixconsultant-led maternity units in NW Londonif Hammersmith Hospital were not classed asa major hospital.How far do you support or oppose therecommendation that there shouldbe five major hospitals in North WestLondon?How far do you support or opposethe recommendation that all majorhospitals should have inpatientpaediatric (children’s) units?171819How far do you support or opposethe recommendation that all majorhospitals in North West London shouldhave consultant-led maternity units,with an extra consultant-led maternityunit at Queen Charlotte’s and ChelseaHospital if Hammersmith Hospital isnot a major hospital?What further comments, if any, doyou have on any of the issues raisedin section 14 of this consultation<strong>document</strong>? (For example, if youoppose the recommendations,how many major hospitals do youthink there should be in North WestLondon? Why do you think that?)2046 What Five major this <strong>document</strong> hospitals for is for NW London
Five major hospitals for NW London47
15. Where should the majorhospitals be located?We recommended that NWLondon should have five majorhospitals and then carried outan in-depth evaluation to lookat where these major hospitalsshould be.Patients and clinicians told us that being ableto access services easily was very important.So, to help them think about where to putthe major hospitals, we looked at:• ambulance journeys;• car journeys at peak traffic hours andnon-peak hours; and• public transport at peak hours.way, both Hillingdon and Northwick Park arethe furthest distance away from any otherpossible major hospital site in NW London.For example, people would have to travel upto 34 minutes by ambulance to get to theirnearest hospital if Hillingdon Hospital nolonger provided some services. This is muchfurther than for people living near the otherhospitals in NW London.This means that two of the five majorhospitals would be at Hillingdon Hospital andNorthwick Park Hospital.You can find more information on thisanalysis in our pre-consultation business case(volume 3, chapter 12) on our website atwww.<strong>healthier</strong>northwestlondon.nhs.ukThese were categorised by ‘lower superoutput area’ (similar to postcode areas). Welooked at how long it would take peopleliving in each area to get to a hospital if theirnearest hospital for a particular service wereto change. It was important to look at howlong it would take people on average andalso what the longest journeys might be.After looking at the evaluation, we proposedthat Hillingdon Hospital and NorthwickPark Hospital should be major hospitals,due mainly to their location. If eitherof these hospitals were not to providemore complicated healthcare, people insurrounding areas would have to travel muchfurther to get to the next hospital providingthose kinds of services. To put it another48 Where What this should <strong>document</strong> the major is for hospitals be located?
There is not as much difference in travel timesfor people living near other hospitals in NWLondon. However, we wanted to make surethat the other three major hospitals werespread evenly across NW London. This is tomake it easy for people to get to them. Welooked at where people are likely to go iftheir nearest hospital did not provide someservices, and proposed a choice of:• a major hospital at either Ealing Hospitalor West Middlesex Hospital;• a major hospital at either Charing CrossHospital or Chelsea and WestminsterHospital; and• a major hospital at either HammersmithHospital or St Mary’s Hospital.This map shows these possible choices.NorthwickParkto West Middlesex Hospital (although theycould of course choose to go to any otherhospital) if some services were no longerprovided at Ealing. And most patients whogo to West Middlesex Hospital now wouldgo to Ealing Hospital if some services were nolonger provided at West Middlesex Hospital.We have based this on information on traveltimes provided by Transport for London. Asa further test, we also looked at what wouldhappen if both hospitals no longer providedsome services and this showed that the timeto get to the next nearest hospital wouldincrease significantly. Assessing the choicebetween Charing Cross Hospital and Chelseaand Westminster Hospital and between StMary’s Hospital and Hammersmith Hospitalgave similar results.You can find more details on all the travel-timeanalysis in the pre-consultation business case(volume 3, chapter 12) on our website atwww.<strong>healthier</strong>northwestlondon.nhs.ukDuring the consultation, we will do furtherwork on the effect of the proposals on traveland on plans for dealing with any travel issues(for example, access to public transport forpeople with a disability).HillingdonWestMiddlesexEalingHammersmithCharingCrossSt Mary’sThere are eight possible combinations ofhospitals where there is a major hospital at:• Hillingdon Hospital;ChelseaandWestminster• Northwick Park Hospital;Proposed major hospitalsNorthwick ParkHillingdonPossible furthermajor hospitalsSt Mary’s or HammersmithCharing Cross or Chelseaand WestminsterEaling or West MiddlesexAs an example, we would expect mostpatients who go to Ealing Hospital would go• either Ealing Hospital or West MiddlesexHospital;• either Charing Cross Hospital or Chelseaand Westminster Hospital; and• either Hammersmith Hospital or St Mary’sHospital.The next section looks at these options inmore detail.Where should the major hospitals be located? 49
Option 1 Option 2 Option 3 Option 4 Option 5 Option 6 Option 7 Option 8St Mary’s Local hospital Local hospital Local hospital Local hospital Major hospital Major hospital Major hospital Major hospitalHammersmithMajor hospitalandspecialisthospitalMajor hospitalandspecialisthospitalMajor hospitalandspecialisthospitalMajor hospitaland Specialistspecialist hospitalhospitalSpecialisthospitalSpecialisthospitalSpecialisthospitalCharing Cross Local hospital Major hospital Local hospital Major hospital Local hospital Major hospital Local hospital Major hospitalChelsea andWestminsterMajor hospital Local hospital Major hospital Local hospital Major hospital Local hospital Major hospital Local hospitalWestMiddlesexMajor hospital Major hospitalLocal hospitalandLocal hospitaland Major hospital Major hospitalLocal hospitalandLocal hospitalandelective hospital elective hospital elective hospital elective hospitalEaling Local hospital Local hospital Major hospital Major hospital Local hospital Local hospital Major hospital Major hospitalCentralMiddlesexLocal hospitalandLocal hospitalandLocal hospitalandLocal hospitalandLocal hospitalandLocal hospitalandLocal hospitalandLocal hospitalandelective hospital elective hospital elective hospital elective hospital elective hospital elective hospital elective hospital elective hospitalNorthwickParkMajor hospital Major hospital Major hospital Major hospital Major hospital Major hospital Major hospital Major hospitalHillingdon Major hospital Major hospital Major hospital Major hospital Major hospital Major hospital Major hospital Major hospital50 Where should the major hospitals be located?
Where should the major hospitals be located?51
16. Which optionsare practical?We asked the public and awide range of clinicians whatcriteria (or measures) we shoulduse to review the options andassess which were practical.For example, at a public event in February2012, 200 representatives of public andpatient groups and clinicians ranked themost important criteria for them as follows.Count of ‘votes’ as shown by stickersCriteriaPublicClinicians1. Quality of care24%19928%2272. Access to care10%846%453. Affordability7%5811%884. Capacity (hospital space)4%334%335. Deliverability8%697%576. Workforce10%8214%1117. Education and research7%5810%848. Alignment with other plans8%684%319. Patient choice8%643% 2210. Patient experience13%10813%107Total‘votes’823Total‘votes‘80552 Which What this options <strong>document</strong> are practical? is for
From this work, we used the followingcriteria to review the options and assesswhich were practical.Criteria1. Quality ofcare2. Access tocare3. Value formoney4.Deliverability5. ResearchandeducationSub criteria• Clinical quality• Patient experience• Distance and time to access services• Patient choice• Capital cost to system• Transition costs• Viable Trusts and sites• Surplus for acute sector• Net present value• Workforce• Expected time to deliver• Alignment with other plans• Disruption• Support current and developingresearch and educationTo review how practical each option wasusing this criteria, we then asked a number ofquestions as follows.• Clinical quality − Which options wouldprovide better clinical quality in <strong>future</strong>using clinical surveys and measures?• Patient experience − Which optionswould provide a better experience forpatients using patient experience surveysand looking at the quality of the buildingsand facilities?• Distance and time to access services– Would any options keep to a minimumthe increase in the average or total timeit takes people to get to hospital byambulance, car (at off-peak and peaktimes) and public transport?• Patient choice – Which options wouldgive people in NW London the greatestchoice of hospitals for emergency care,maternity care and planned care acrossthe greatest number of trusts?• Capital cost to the system – Whichoptions would have the lowest capitalcosts (cost of buildings and equipment)?• Transition costs – Which options wouldhave the lowest cost of transferring servicesbetween hospitals?• Viable trusts and sites – Which optionswould have the lowest yearly subsidy andthe fewest hospitals and trusts with afinancial surplus of less than 1% (the lowestacceptable level of financial surplus allowedfor trusts in the NHS)?• Surplus for acute sector – Which optionswould give the largest financial surplusacross all hospitals, to make sure that theproposed changes are affordable?• Net present value – Which options wouldgive the largest net present value (overallfinancial benefit) over the next 20 years?• Workforce – Which options would providethe best workplace for staff (using staffsatisfaction surveys)?• Expected time to deliver – How long wouldit take to deliver the proposed changes in eachoption? A shorter delivery time means thatbenefits can be delivered earlier.• Fitting in with other strategies – Howwell would each option fit with what ishappening, or may happen, nationally or inLondon?• Disruption – Which options best fit withcurrent research and education to minimisedisruption in these areas?• Support current and developingresearch and education delivery –Which options would best support what ishappening in research and education?You can find all the information and analysiswe used to answer these questions in thepre- consultation business case (volume 3,chapter 14) on our website atwww.<strong>healthier</strong>northwestlondon.nhs.ukOnce we had answered these questions, welooked at the overall evaluation, which isshown in the table overleaf.Which options are practical? 53
54 Which options are practical?
2122You can find the detailed evaluation in ourpre-consultation business case (volume3, chapter 14) on our website at www.<strong>healthier</strong>northwestlondon.nhs.uk.This showed that three options (option 5,option 6 and option 7) were practical. Theother options were not practical becausethey were assessed poorly against a numberof criteria or because they did not showvalue for money (or both). We assessedoption 5 as being much more practical thanthe other options and so this became thepreferred option following this exercise. Inthe next section we describe the three mostpractical options in more detail and explainwhy option 5 is the preferred option.Please consider the way we decidedwhich hospitals to recommend asmajor hospitals, as set out in sections15 and 16. Do you agree or disagreethat this is the right way to choosebetween the various possibilities inorder to decide which options torecommend?Please say how important you thinkeach of these criteria (measures)should be in choosing which hospitalsshould be major hospitals, ratingtheir importance on a scale where 10means ‘absolutely vital’ and 0 means‘not important at all’. (We have givenmore details on the criteria in the liston page 53).Hammersmith HospitalAs we have assessed options 1 to 4 as notpractical, this means we do not proposeHammersmith Hospital as a major hospitalin any of the consultation options. Today,Hammersmith Hospital provides a widerange of specialist services, a very limitedA&E service and maternity services. Under allthe options for consultation, HammersmithHospital will keep all of its specialist servicesand its maternity unit. The only proposedchange is to the A&E department, whichwould become an urgent care centre, and thenon-specialist services that support this.The reasons that we are not proposingHammersmith Hospital as a major hospital areas follows.• Significant extra cost. HammersmithHospital doesn’t provide importantservices such as emergency generalsurgery and orthopaedics at the moment,and significant capital spending (spendingon buildings and equipment) wouldbe needed to provide these services atHammersmith Hospital.• Complicated to deliver. A majorhospital at Hammersmith Hospital ratherthan St Mary’s Hospital would meanmoving a large number of services fromSt Mary’s Hospital, including the majortrauma centre and paediatric services,which would be a challenge.• Allows an extra maternity unit. Thematernity unit at Queen Charlotte’sand Chelsea Hospital would continueto be provided under options whereHammersmith Hospital is not a majorhospital (the specialist services at theHammersmith Hospital means that theHammersmith Hospital can provide thesenior clinicians and back-up neededto run a safe maternity unit even ifHammersmith Hospital were not a majorWhich options are practical? 55
hospital), giving an extra maternity unit inNW London.23• Better support for research andeducation. Most medical research inNW London is currently carried outat Hammersmith Hospital, with someresearch at St Mary’s Hospital andChelsea and Westminster Hospital.If Hammersmith Hospital becomes aspecialist hospital and St Mary’s Hospitalbecomes a major hospital, currentresearch arrangements can continue atboth those sites.What further comments, if any, doyou have on any of the issues raised insections 15 or 16 of this consultation<strong>document</strong>? (For example, please tellus if you think there are any criteriathat we have missed and which shouldalso be taken into account in choosingwhich hospitals should be majorhospitals).Central Middlesex HospitalWe have not proposed Central MiddlesexHospital as a major hospital in any of theconsultation options. We have recommendedthat Central Middlesex Hospital should notbe a major hospital but an elective hospitalwith local hospital services. This is because itis already providing these services, its majorA&E services are already under pressure(A&E emergency round-the-clock care hadto be suspended in late 2011 because notenough senior emergency care doctorswere available on-site), essential servicesfor a major hospital – emergency surgery,paediatrics and maternity – are not providedon-site and patients could access these majoremergency care services elsewhere in othernearby hospitals.56 Which What this options <strong>document</strong> are practical? is for
17. The three optionsfor major hospitalsIn this section, we describethe three options for majorhospitals. We also explain whythere is a preferred option.To make consultation easier, we haverenumbered the options.• Option 5 has become option A• Option 6 has become option B• Option 7 has become option CAll our options for consultation will meanthat quality of care will improve outside andin hospitals.• Improved care outside hospital. Underall options, improved quality of healthcareoutside hospitals will support people tolead <strong>healthier</strong> lifestyles, improve access toservices, allow people to take control oftheir own health and mean care is moreco-ordinated.• Improved quality of care in hospitals.Under all options, reducing the numberof hospitals providing some services willmean there will be more specialist andexperienced doctors available for moreof the time, and that they will be able tobuild and maintain the skills and expertisethey need to deliver high-quality care.There will also be more back-up forservices.All options will mean that some patientswould have to travel a little longer for someaspects of their care, but on average nomore than 6 minutes longer. As described insection 7, clinicians agree it is more importantthat patients are taken to the right place fortreatment by the right clinicians even if theyneed to travel further.Option A (preferred option)This option is the preferred option. It hasChelsea and Westminster Hospital, HillingdonHospital, Northwick Park Hospital, St Mary’sHospital and West Middlesex Hospital asmajor hospitals. It has Central MiddlesexHospital as a local and elective hospital andHammersmith Hospital as a specialist hospital.Ealing Hospital and Charing Cross Hospitalare proposed as local hospitals.Some services will no longer be available insome hospitals and instead will be providedat neighbouring hospitals where there wouldbe more senior, experienced staff availableand extra back-up in case of problems. Somespecialist services will also need to movewhere hospitals become local hospitals. Wehave outlined the services provided at eachsite before and after the proposed changes inthe table on page 59.Under this option, around 91% of serviceswould not be affected by the proposedchanges. The proportion of services thatwould be affected under this option isThe three options for major hospitals57
Option A (preferred option)MountVernonRoyal NationalOrthopaedicSpecialist hospitalHarefieldHillingdonNorthwickParkCentral MiddlesexLocal and elective hospitalLocal and major hospital withinpatient paediatric unit andconsultant-led maternity unitLocal hospital onlyConsultant-ledmaternity unitHammersmithEalingSt Mary’sWestMiddlesexCharingCrossChelseaandWestminsterRoyalBromptonRoyalMarsdenrelatively low, with 22% of inpatient cases,14% of A&E cases and 5% of outpatientcases likely to move. Similarly, it is estimatedthat 81% of the workforce would not beaffected by the changes, with most of thoseaffected needing to move location to provideservices either within a neighbouring hospitalor within the community.We believe this option would deliver thegreatest benefits for NW London for thefollowing reasons.• Good use of buildings. Chelsea andWestminster Hospital and West MiddlesexHospital both consist of very recently builtbuildings, with space that is suitable forboth current and <strong>future</strong> requirements.Given what we have already said aboutthe need to manage and maintain NHSbuildings in NW London, and the difficultyof building new ones, this is a majorfactor.• Value for money. This option wouldneed relatively limited amounts of capitalspending (on buildings and equipment)and it would leave NW London witha predicted overall financial surplusgreater than 2%. Only one trust (onehospital) is predicted to have a deficit inthis option. We predict this option willprovide the best return on investment ofall the options. It means the NHS in NorthWest London would be in a much betterfinancial position than if nothing wereto change.• Easy to deliver. This option correspondsmost closely with services already beingdelivered at each hospital, and with otherchanges taking place outside the ‘<strong>Shaping</strong>a <strong>healthier</strong> <strong>future</strong>’ programme. So, thescale of the change needed would besmallest under this option.• Supports research and education. Mostimportant medical research in NW Londonis currently carried out at HammersmithHospital, St Mary’s Hospital and Chelseaand Westminster Hospital. Under thisoption, Hammersmith Hospital becomesa specialist hospital and St Mary’s Hospitalbecomes a major hospital, which wouldmean current research arrangements cancontinue at both those sites.58The What three this options <strong>document</strong> for is major for hospitals
The three options for major hospitals59
Option BThis option has Charing Cross Hospital,Hillingdon Hospital, Northwick Park Hospital,St Mary’s Hospital and West MiddlesexHospital as major hospitals. It has CentralMiddlesex Hospital as a local and electivehospital, and Hammersmith Hospital asa specialist hospital. Ealing Hospital andChelsea and Westminster Hospital would belocal hospitals.Some services will no longer be available insome hospitals and instead will be providedat neighbouring hospitals where there wouldbe more senior, experienced staff availableand extra back-up in case of problems. Somespecialist services will also need to movewhere hospitals become local hospitals. Wehave outlined the services provided at eachsite before and after the proposed changes inthe table opposite.Under this option, around 87% of serviceswould not be affected by the proposedchanges. The proportion of services thatwould be affected under this option isrelatively low, with 25% of inpatient cases,17% of A&E cases and 9% of outpatientcases likely to move. Similarly, it is estimatedthat 79% of the workforce would not beaffected by the changes, with most of thoseaffected needing to move location to provideservices either within a neighbouring hospitalor within the community.MountVernonRoyal NationalOrthopaedicSpecialist hospitalHarefieldHillingdonNorthwickParkCentral MiddlesexLocal and elective hospitalLocal and major hospital withinpatient paediatric unit andconsultant-led maternity unitLocal hospital onlyConsultant-ledmaternity unitHammersmithEalingSt Mary’sWestMiddlesexCharingCrossChelseaandWestminsterRoyalBromptonRoyalMarsden60 The What three this options <strong>document</strong> for is major for hospitals 60
The three options for major hospitals61
This option would deliver benefits for NWLondon.• Good use of some buildings. Thisoption has West Middlesex Hospital as amajor hospital, which would be a gooduse of high-quality buildings but doesnot include a major hospital at Chelseaand Westminster Hospital, which also hashigh-quality buildings.• Value for money. This option wouldneed relatively limited amounts of capitalspending (on buildings and equipment).Two trusts (two hospitals) would continueto have a predicted deficit in this optionand the predicted overall financialsurplus would be less than 2% acrossNW London. This option is predicted toprovide a positive return on investment,although less than for option A. It meansthe NHS in NW London would be in abetter financial position than if nothingchanges.• Fairly easy to deliver. This optioncorresponds reasonably well with servicesalready being delivered at each hospital,and with other changes taking placeoutside the ‘<strong>Shaping</strong> a <strong>healthier</strong> <strong>future</strong>’programme. However, the maternityand paediatric units at Chelsea andWestminster Hospital would have to bemoved elsewhere under this option.• be more difficult to deliver – Chelseaand Westminster Hospital has a largeobstetric unit, and if it were not chosen asa major hospital, these beds would needto be moved elsewhere;• be a poor use of buildings – it wouldnot make the best use of the high-qualitybuildings at Chelsea and WestminsterHospital;• give worse value for money – it wouldbe more expensive to put in place thanoption A and would result in a lowerfinancial surplus across NW London;• leave two trusts (two hospitals)in deficit – two trusts (two hospitals)would still lose money compared withoption A; and• reduce patient choice – includingCharing Cross Hospital rather thanChelsea and Westminster Hospital wouldmean only four trusts running majorhospitals, rather than five.• Supports research and education. Mostimportant medical research in NW Londonis currently carried out at HammersmithHospital, St Mary’s Hospital and Chelseaand Westminster Hospital. Under thisoption, Hammersmith Hospital becomes aspecialist hospital and St Mary’s Hospital amajor hospital, which would mean currentresearch arrangements can continue atboth those sites.Option B gives fewer benefits than option A,because it would:62 The What three this options <strong>document</strong> for is major for hospitals
The three options for major hospitals63
Option CThis option has Chelsea and WestminsterHospital, Ealing Hospital (with the stroke unitat West Middlesex Hospital moved to EalingHospital), Hillingdon Hospital, Northwick ParkHospital and St Mary’s Hospital as the majorhospitals. It has Central Middlesex Hospitaland West Middlesex Hospital as a local andelective hospital and Hammersmith Hospitalas a specialist hospital. Charing Cross Hospitalis proposed as a local hospital.Some services will no longer be available insome hospitals and instead will be providedat neighbouring hospitals where there wouldbe more senior, experienced staff availableand extra back-up in case of problems. Somespecialist services will also need to movewhere hospitals become local hospitals. Wehave outlined the services provided at eachsite before and after the proposed changesin the table opposite.Under this option, around 91% of serviceswould not be affected by the changes.The proportion of services that would beaffected under this option is relatively low,with 18% of inpatient cases, 15% of A&Ecases and 5% of outpatient cases likely tomove. Similarly, it is estimated that 81% ofstaff would not be affected by the changes,with most of those affected needing tomove location to provide services eitherwithin a neighbouring hospital or withinthe community.MountVernonRoyal NationalOrthopaedicSpecialist hospitalHarefieldHillingdonNorthwickParkCentral MiddlesexLocal and elective hospitalLocal and major hospital withinpatient paediatric unit andconsultant-led maternity unitLocal hospital onlyConsultant-ledmaternity unitHammersmithEalingSt Mary’sWestMiddlesexCharingCrossChelseaandWestminsterRoyalBromptonRoyalMarsden64 The What three this options <strong>document</strong> for is major for hospitals
The three options for major hospitals65
This option would deliver benefits for NWLondon.• Good use of some buildings. Thisoption has Chelsea and WestminsterHospital as a major hospital, which wouldbe a good use of high-quality buildingsbut does not include a major hospital atWest Middlesex Hospital, which also hashigh-quality buildings.• Value for money. This option wouldneed more capital spending on buildingsand equipment than option A. Wepredict that two trusts (three hospitals)would have a deficit in this option andthe predicted financial surplus would beless than 2% across NW London. So, thisoption would provide a positive return oninvestment, but less than for option A.It means the NHS in NW London wouldbe in a better financial position than ifnothing changes, under this option.• Supports research and education. Mostimportant medical research in NW Londonis currently carried out at HammersmithHospital, St Mary’s Hospital and Chelseaand Westminster Hospital. Under thisoption, Hammersmith Hospital becomes aspecialist hospital and St Mary’s Hospital amajor hospital, which would mean currentresearch arrangements can continue atboth those sites.would still lose money compared withoption A; and• be more difficult to deliver – the strokeunit at West Middlesex Hospital wouldneed to be moved as it would not beable to provide this service safely withoutmajor hospital back-up.We have carefully considered whetherthere should be a ‘preferred option’ forconsultation, since the three options – A, Band C – are all practical. However, becausethe Joint Committee of Primary Care Trusts,which is leading this consultation, believesthat option A delivers the greatest benefitsfor NW London, it would be misleading notto say so.Having said that, this is a consultation aimedat gathering people’s views. So we areputting all three options forward and invitingyour views on which option will have themost benefits.As part of the consultation, we wouldencourage healthcare providers, includingfrom the independent and voluntary sectors,to make proposals for new and innovativeways of delivering services. We will make surethat information is available so that anyonewho is interested in making proposals is ableto do so, and we will fully and fairly considerany responses.Option C is not as good an option as optionA, because it would:• give worse value for money – it wouldnot save as much money, and is predicted tobe the least financially secure of the options;• be a poor use of buildings – it wouldnot make the best use of the high-qualitybuildings at West Middlesex Hospital;• leave two trusts (three hospitals)in deficit – two trusts (three hospitals)66 The What three this options <strong>document</strong> for is major for hospitals
Thinking about the proposals put forward in sections 16 and 17, please say howfar you support or oppose each of the three proposed options for the locationof major hospitals in North West London. (You can support more than one of theoptions if you want.) Please explain why you support or oppose each option.242524a. Option A (the preferred option):Major hospitals – Chelsea andWestminster Hospital, HillingdonHospital, Northwick Park Hospital, StMary’s Hospital and West MiddlesexHospital.Elective and local hospital – CentralMiddlesex Hospital.Local hospitals – Charing CrossHospital, Ealing Hospital.Specialist hospital (with maternity unit)– Hammersmith Hospital24b. Why is this your answer?25a. Option B:Major hospitals – Charing CrossHospital, Hillingdon Hospital, NorthwickPark Hospital, St Mary’s Hospital andWest Middlesex Hospital.Elective and local hospital – CentralMiddlesex Hospital.Local hospitals – Chelsea andWestminster Hospital, Ealing Hospital.Specialist hospital (with maternity unit) –Hammersmith Hospital.25b. Why is this your answer?2626a. Option C:Major hospitals – Chelsea and Westminster Hospital, Ealing Hospital (with the stroke unitat West Middlesex Hospital moved to Ealing Hospital), Hillingdon Hospital, Northwick ParkHospital and St Mary’s Hospital.Elective and local Hospital – Central Middlesex Hospital and West Middlesex Hospital.Local hospitals – Charing Cross Hospital.Specialist hospital (with maternity unit) – Hammersmith Hospital.26b. Why is this your answer?The three options for major hospitals67
273027a. All the options above include therecommendation that Central MiddlesexHospital should be an elective andlocal hospital. How far do you supportor oppose the recommendation thatCentral Middlesex Hospital should be anelective and local hospital?27b. Why is this your answer?30a. All the options above include therecommendation that HammersmithHospital should be a specialisthospital. There would continue to bea maternity unit at Hammersmith.How far do you support or oppose therecommendation that HammersmithHospital should be a specialist hospitalwith a maternity unit?2830b. Why is this your answer?28a. All the options above includethe recommendation that HillingdonHospital should be a major hospital.How far do you support or opposethe recommendation that HillingdonHospital should be a major hospital?28b. Why is this your answer?Are there any other options we shouldconsider when making our decisions?If so, please give your reasons forsuggesting these.312929a. All the options above include therecommendation that Northwick ParkHospital should be a major hospital.How far do you support or oppose therecommendation that Northwick ParkHospital should be a major hospital?29b. Why is this your answer?68 The What three this options <strong>document</strong> for is major for hospitals
18. Proposals for changesto specialist servicesSpecialist hospitals alreadyprovide high-quality services inNW London and cover the localpopulation (and many otherparts of London too) very well.So specialist hospitals will stay largely asthey are.However, as part of this consultation, weare recommending two particular changesto specialist services, as well as changes tospecialist services where hospitals becomelocal hospitals.1. Moving the hyper-acute stroke unit(HASU) from Charing Cross Hospital toSt Mary’s Hospital under options whereCharing Cross Hospital is not a majorhospital.If Charing Cross Hospital were to become alocal hospital, we could not maintain a hyperacutestroke unit (HASU) there. The HASUwould need to move to a major hospitalclose to the Charing Cross Hospital site. Thestroke and major trauma consultation in 2009showed a preference for putting HASUs onthe same site as major trauma centres, as theyneed similar back-up and support. As thereis now a major trauma centre at St Mary’sHospital, we propose to move the HASU fromCharing Cross Hospital to St Mary’s Hospital inoption A and option C, where Charing CrossHospital is a local hospital.2. Moving services from the Western EyeHospital to St Mary’s HospitalThe Western Eye Hospital is the specialistophthalmology hospital in NW London andpart of Imperial Healthcare NHS Trust. It is theonly hospital to offer a 24-hour emergencyeye-care service in NW London for ambulanceand walk-in cases. The service uses a minorsurgical theatre, a triage system, inpatientbeds and theatres. The Western Eye Hospitalalso offers outpatients, inpatients and daycaresurgery.The hospital is located on its own just offMarylebone Road. As part of Imperial’sstrategy, they would like to move theseservices to one of their other hospital sitesand, so that people can understand all thechanges being proposed in NW London,we have included this proposal in thisconsultation.Separating Western Eye Hospital servicesfrom the main hospital services at St Mary’sHospital creates service and financial waste.By combining services, Imperial will be ableto offer an integrated ophthalmologic servicefor urgent and non-urgent patient needs.There will be one place for all ophthalmologicemergencies, reducing the need fortransferring patients and allowing clinicians towork more economically and effectively.Imperial have looked at the option ofmoving services to each of its other sites(St Mary’s Hospital, Charing Cross Hospitaland Hammersmith Hospital). It thinks thatProposals for changes to specialist services69
the best option is to move the Western EyeHospital to St Mary’s Hospital as this would:• have little effect on patient accesscompared with the current site;• improve clinical performance because ofcombining services and putting them withmajor trauma and paediatrics at St Mary’sHospital; and• be the better long-term option (clinicallyand financially) for Imperial.Imperial estimates the net costs of movingto St Marys would be between £5 millionand £15 million, with the lower amountbeing more likely as part of broader siteredevelopment at St Mary’s.You can find more details in our preconsultationbusiness case (Appendix K)on our website atwww.<strong>healthier</strong>northwestlondon.nhs.uk32a. Do you agree or disagree thatthe hyper-acute stroke unit, whichwas designated to Charing Crossfollowing the stroke and major traumaconsultation, should move to be withthe major trauma unit at St Mary’s?32b. Why is this your answer?33a. Do you agree or disagree thatthe Western Eye Hospital should berelocated with the major hospital at StMary’s?33b.Why is this your answer?323370 Proposals What this for <strong>document</strong> changes is to for specialist services
19. Making this workfor patientsWe have worked long and hard,with patient representativegroups and others, to makesure that the ‘<strong>Shaping</strong> a<strong>healthier</strong> <strong>future</strong>’ programme asit is put in place over the nextfew years in NW London shouldbenefit patients, not have anegative effect on them.But because there is understandable concernabout some areas of change to NHS services,we want, in particular, to highlight thefollowing.• We are investing in developing bigger,better specialist teams in major hospitalsand in community services.• We are investing to increase servicesoutside hospital and have plans for newfacilities to deliver these services.• The main parts of the proposed changeshave all been delivered before, in thiscountry and around the world, and soare known to be a successful way toreorganise health services to prepare for<strong>future</strong> demands.• Most patients using NW London hospitals’emergency services are already usingminor injuries units or urgent care centres– they are not actually using, or needingto use, major A&E departments. Somoving the major A&E departments awayfrom some locations would not affectmany of the patients using these samehospital sites already.• It will take longer for some people toget to some services, or visit relatives.But the benefits of better, specialisedcare at these hospitals, and from morecare being delivered closer to home, faroutweigh the inconvenience of theseincreased journeys. Those using the NHShave consistently said in surveys that theywould rather travel further to receivebetter care – and would want the samefor their families.• Many health services provided in thecommunity – such as GP services andmental-health services – are already beingimproved and would need a relativelymodest investment of time and money tocope with the extra services that wouldswitch from being provided in hospitals atthe moment to being provided by facilitiescloser to home, such as in improved GPsurgeries, new health centres, and newcommunity facilities. We have promisedthat we will not make changes tohospitals until any alternative services thatare necessary are in place.• To find out whether our proposals mightunfairly disadvantage some communities,we have done an independent equalitiesimpact review which looked at howMaking this work for patients71
the proposed changes would affectpeople such as young children, ethniccommunities, women and the elderly.This review showed that in most casesthese groups would not be unfairlydisadvantaged. We are developingan action plan to tackle any potentialdisadvantages that have been reported.You can see the full report for thisreview on our website atwww.<strong>healthier</strong>northwestlondon.nhs.ukIs there anything else you want to sayabout the consultation or the issues itcovers? If you want to explain any ofyour answers, or you feel the questionshave not given you the chance to giveyour views fully, or if you think thereare options we have not consideredthat we should have done, please sayso here.3472 Making this work for patients
Making this work for patients73
20. Next stepsWe are keen to continue thediscussion with patients, thepublic, and those who maybe affected by the proposedchanges to health services inNW London.There is a recognised process for doing this as,by law, the NHS has to consult patients andthe public on any major change to local healthservices. Government guidance on this sayswe must:1. Consult widely throughout the process,“allowing a minimum of 12 weeks forwritten consultation at least once during thedevelopment of the policy.2. Be clear about what the proposals are, whomay be affected, what questions are beingasked and the timescale for responses.3. Ensure that the consultation is clear, conciseand widely accessible.4. Give feedback regarding the responsesreceived and how the consultation processinfluenced the policy.5. Monitor the effectiveness of theconsultation, including through the use of adesignated consultation co-ordinator.6. Ensure the consultation follows betterregulation best practice, including carryingout a Regulatory Impact Assessment ifappropriate.“So, through a large-scale consultationrunning for 14 weeks from 2 July to 8October, we are asking people for theiropinions on these options for change,making sure we involve patients and thepublic more widely. (We have added an extratwo weeks to the minimum consultation timebecause it is taking place over the summer.)There will be focus groups, roadshows, events inhospitals, and other events around all eight NWLondon boroughs (and the three outside NWLondon who may be affected by the changes),to make sure we involve as many people andcommunities as possible, including some whoare sometimes referred to as ‘seldom heard’groups. The aim is to explain, to listen, and toreceive views from as many people as possible.We will then spend some time assessingpeople’s views, before making a further report,in early 2013. The Joint Committee of PrimaryCare Trusts will then make the final decisionon changes to services. The Joint HealthOverview and Scrutiny Committee, which ismade up of representatives from each of thelocal authorities in NW London, will closelycheck our consultation and proposed plans.If the changes are agreed they will take at leastthree years to put in place. Work to developservices that can be provided in the home,GP surgeries and health centres has alreadystarted and only once these services are inplace will changes to hospitals be made.74 What Next steps this <strong>document</strong> is for
<strong>Shaping</strong> a <strong>healthier</strong> <strong>future</strong> Next steps 75
GlossaryA&E – accident & emergency is a serviceavailable 24 hours a day, seven days a weekwhere people receive treatment for medicaland surgical emergencies that are likely toneed admission to hospital. This includessevere pneumonia, diabetic coma, bleedingfrom the gut, complicated fractures that needsurgery, and other serious illnesses.Acute care – acute care refers to short-termtreatment, usually in a hospital, for patientswith any kind of illness or injury.Acute trust – NHS acute trusts managehospitals. Some are regional or nationalcentres for specialist care, others are attachedto universities and help to train healthprofessionals. Some acute trusts also providecommunity services.Bundle – a combination of relevant‘packages of care’ for a patient. For example,a bundle for a patient with diabetes couldinclude podiatry, dietetics, diabetes nursingand ophthalmology.Cardiothoracic − is the field of medicineinvolved in surgical treatment of diseasesaffecting organs inside the thorax (the chest)− generally treatment of conditions of theheart (heart disease) and lungs (lung disease).Cardiovascular – this refers to the heart andblood vessels. Cardiovascular diseases affectthe function of the cardiovascular system,which carries nutrients and oxygen to thetissues of the body while removing carbondioxide and other wastes from them.CCG – clinical commissioning group. Theseare the health commissioning organisationswhich will replace primary care trusts (PCTs)in April 2013. CCGs are led by GPs andrepresent a group of GP practices in a certainarea. They are currently shadowing the PCTsand will be responsible for commissioninghealthcare services in both community andhospital settings from April 2013 onwards.Care outside hospital – care that takesplace outside of hospital, in a communitysetting. This could be a patient’s home,community bed or community health centre.Centralise – a principle of the ‘<strong>Shaping</strong> a<strong>healthier</strong> <strong>future</strong>’ programme, which is aboutbringing more services together on a numberof specific sites to create a greater level ofexpertise.Complex elective medicine or surgery – aplanned operation or medical care where thepatient may need to be in a high-dependencyunit while recovering from the operation,either because the operation is complex orbecause they have other health problems.Continuity of care – an integratedcare project that has been launched inHammersmith and Fulham. The project aimsto improve outcomes for patients at minimalcosts and reduce treatment or stays in hospital.COPD – chronic obstructive pulmonarydisease. COPD is a lung disease which causesdifficulty or discomfort in breathing.CQC – Care Quality Commission – this is anorganisation funded by the Government to76 Glossary What this <strong>document</strong> is for
check all hospitals in England to make surethey are meeting government standards, andto share their findings with the public.Deficit – when spending is greater than income.Elective hospital – this is where patients goif they need an operation which is not urgentand so can be planned.Emergency surgery – surgery that is notplanned and which is needed for urgentconditions. This includes surgery forappendicitis, perforated or obstructed bowel,and gallbladder infections. It is also known asnon-elective surgery.Financial surplus – when income is greaterthan spending.Foundation trust (FT) − NHS FoundationTrusts are not-for-profit corporations. Theyare part of the NHS yet they have greaterfreedom to decide their own plans and theway services are run. Foundation trusts havemembers and a council of governors. The aimis that eventually all NHS trusts will be FTs.GP network or cluster – a smaller group ofGP practices within a borough or CCG area(see CCG above).HealthWatch – these are new organisationswhich will replace LINks (see below) as partof the restructure of the NHS. Their roleis to make sure patients are involved indeveloping and changing NHS services andto provide support to local people. There willbe a national HealthWatch to oversee thelocal HealthWatch and provide advice as anindependent part of the CQC (see above).Health centre or ‘hub’ – a setting for careoutside hospital which will be adapted fromexisting community sites to provide otherservices locally, serving as a support ‘hub’ tolocal healthcare teams. The services offeredwill vary depending on local needs andwill range from bases for multidisciplinaryteams to ‘one-stop’ centres for GP services,diagnostics and outpatient appointments.Heart attack centre – a centre which treatspeople who have had a heart attack.Health and well-being board (HWB)− part of the NHS restructure, the aim ofthese boards is to encourage joint workingbetween the NHS and local authorities acrosshealth and social care. HWBs are expected tobe up and running in April 2013.High-dependency unit – treats conditionsthat need intensive nursing support, such aspeople who are ill with pneumonia or whohave had major surgery.Hyper-acute stroke unit (HASU) − hospitalwards that specialise in treating people whoare having a stroke.Integrated care pilot (ICP) − a joint ventureled by commissioners and providers ofprimary, community, acute, social and mentalhealthcare for people aged 75 and over withdiabetes. The aim is to offer integrated careto improve the outcome for patients andreduce unnecessary stays in hospital.Inpatient – a patient who is admitted to ahospital, usually for 24 hours, for treatmentor an operation.Inpatient paediatrics – these units treat sickchildren who require a stay in hospital.Integrate – a principle of this programmewhich refers to creating more co-ordinatedcare for the patient, making sure all parts ofthe NHS and social services work more closelyand effectively together.Interdependency – where some clinicalservices need other clinical services to be basedon the same site for particular types of care tobe successfully and fully delivered together.Glossary77
Interventional radiology − uses minimallyinvasive image-guided procedures todiagnose and treat diseases in nearly everyorgan system.Intensive care − these units provide supportfor patients after complex surgery, or patientsneeding multiple organ support such asventilation and dialysis.Key performance indicator (KPI) − targetsthat are agreed between the providerand commissioner of each service, whichperformance can be tracked against.Level 3, as in level 3 intensive care unit- ICUs are sections within a hospital thatlook after patients whose conditions arelife-threatening and need constant, closemonitoring and support from equipment andmedication to keep normal body functionsgoing. Level 3 ICU is for patients who needadvanced respiratory support alone or basicrespiratory support with the support of atleast two organ systems. This level includesall patients with complex needs who needsupport for multi-organ failure.LINks – local involvement networks. LINksare made up of individuals and communitygroups whose goal is to improve health andsocial care services. They are funded by localcouncils, although they are independentof the Government. In 2013 they will bereplaced by HealthWatch (see above).Local hospital – a type of hospital proposedin the changes. Local hospitals will includeurgent care centres, which provide theservices that three-quarters of people goto hospital for – such as everyday illnesses,minor injuries and long-term conditions suchas diabetes or asthma.Localise – a principle of this programme, whichis to deliver as much care as possible in themost convenient locations, making sure peoplehave earlier and easier access to treatment.Major hospital – a type of hospital proposedin the changes. A major hospital will includefull A&E, paediatrics and maternity services.Maternal deaths – death of a womenwhile pregnant or within 42 days of end ofpregnancy, from any cause related to thepregnancy.Maternity − relating to pregnancy, childbirthand immediately following childbirth.Multi-disciplinary group (MDG) −sometimes referred to as a multidisciplinaryteam. These are groups of professionals fromprimary, community, social care and mentalhealthservices who work together to plan apatient’s care.Neonatal – relating to newborn infants.Non-complex elective surgery ormedicine (or both) – this includes herniarepairs, knee replacements and plannedgallbladder operations, usually as day cases.Non-elective medicine – treatment forillnesses that is not planned, including severepneumonia, flare-ups of inflammatory boweldisease, severe asthma attacks and worseningof COPD, needing admission to hospital.Non-elective surgery – see emergency surgeryObstetric – the care associated with givingbirth.Obstetrics and maternity unit – wherebabies are delivered and women with complexpregnancies, such as expectant mothers withdiabetes or heart disease, or who are pregnantwith triplets, are monitored.Overview and Scrutiny Committee (OSC),Health OSC (HOSC) and Joint Health OSC(JHOSC) − the committee of the relevant localauthority, or group of local authorities, madeup of local councillors who are responsiblefor monitoring, and if necessary challenging,78 Glossary What this <strong>document</strong> is for
programmes such as the ‘<strong>Shaping</strong> a <strong>healthier</strong><strong>future</strong>‘ programme. Parts of consultation, suchas the length of the consultation period, haveto be agreed by them.Outpatient – a patient who attends anappointment to receive treatment withoutneeding to be actually admitted to hospital,unlike an inpatient. Outpatient care can beprovided by hospitals, GPs and communityproviders and is often used to follow up aftertreatment or to assess for further treatment.Outpatients and diagnostics – for peoplewho need specialist advice or investigationin hospital. This includes support forinsulin-dependent diabetics or neurologicalconditions such as multiple sclerosis. Italso includes minor surgery, ECGs, x-rays,ultrasounds, CT and MRI scans.Package of care – a term used to describe acombination of services put together to meet aperson’s assessed healthcare needs. It outlinesthe care, services and equipment a personneeds to live their life in a dignified way.Patient pathway or journey – this is a termused to describe the care a patient receivesfrom start to finish of a set timescale, indifferent stages. There can be integrated carepathways which include multi-disciplinaryservices for patient care (see MDG above).Paediatric services – this refers to healthcareservices for babies, children and adolescents.Patient and public advisory group (PPAG)– there is a London-wide PPAG as well as aPPAG in NW London. Their role is to makesure the interests of patients and the publicare represented in the NHS. Members usuallyinclude representatives of local LINks, hospitalpatient groups, local clinical commissioninggroups, the London PPAG and NHS staff.Primary care – services which are the main orfirst point of contact for the patient, providedby GPs, community providers and so on.Primary care trust (PCT) – PCTs commissionprimary, community and secondary care fromproviders. To be replaced by CCGs (see above)in April 2013.Quality, innovation, productivity andprevention (QIPP) – the Department ofHealth QIPP agenda aims to achieve up to£20 billion of efficiency savings by 2015 bymaking sure that each pound spent is used tobring maximum benefit and quality of care topatients.Secondary care – hospital or specialist carethat a patient is referred to by their GP orother primary care provider.Specialist hospital – a hospital whichprovides specialist care for particularconditions, for example cancer or lungdisease.Stroke – a stroke is the sudden deathof brain cells in a particular area due toinadequate blood flow.Trauma, as in major trauma centreor trauma centre – these centres treatmajor trauma patients who have complexinjuries – either one very serious injury or anumber of injuries – which make managingthese patients very challenging. They needexpert care from a large number of differentspecialties to give them the best chance ofsurvival and recovery.Urgent care centre (UCC) − a centre thatis open 24 hours a day, seven days a week.These centres will treat most illnesses andinjuries that people have which are not likelyto need treatment in hospital. This includeschest infections, asthma attacks, simplefractures, abdominal pain and infections ofthe ear, nose and throat.Value for money (VFM) − a term often usedto demonstrate the quality of a healthcareservice balanced against the cost of deliveringthat service.Glossary79
This <strong>document</strong> is also available in other languages, in large print,and in audio format. Please ask us if you would like it in one ofthese formats.Glossary What this <strong>document</strong> 0800 is for 881 5209 consultation@nw.london.nhs.uk
t: 0800 881 5209e: consultation@nw.london.nhs.ukwww.<strong>healthier</strong>northwestlondon.nhs.uk