pOSt Operative Order Set
pOSt Operative Order Set
pOSt Operative Order Set

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
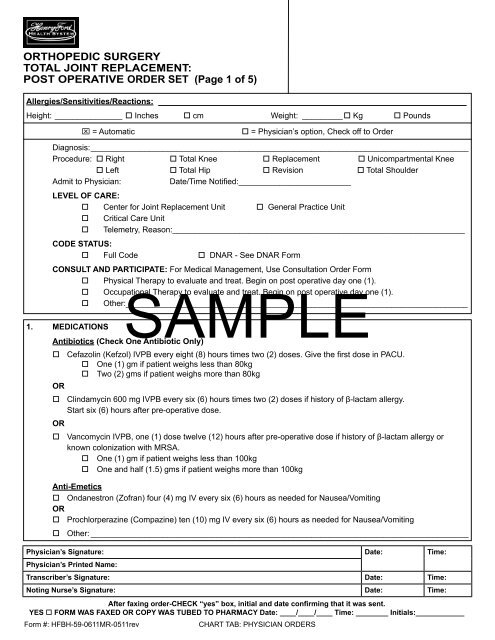
Orthopedic SurgeryTotal Joint Replacement:Post <strong>Operative</strong> <strong>Order</strong> <strong>Set</strong>(Page 1 of 5)Allergies/Sensitivities/Reactions:Height:________________ Inches cm Weight:_ _________ Kg Pounds = Automatic = Physician’s option, Check off to <strong>Order</strong>Diagnosis:____________________________________________________________________________________Procedure: Right Total Knee Replacement Unicompartmental Knee Left Total Hip Revision Total ShoulderAdmit to Physician:Date/Time Notified:_________________________Level of Care: Center for Joint Replacement Unit General Practice Unit Critical Care Unit Telemetry, Reason:_________________________________________________________________Code Status: Full Code DNAR - See DNAR FormConsult and Participate: For Medical Management, Use Consultation <strong>Order</strong> Form Physical Therapy to evaluate and treat. Begin on post operative day one (1). OccupationalSAMPLETherapy to evaluate and treat. Begin on post operative day one (1). Other:____________________________________________________________________________1. MedicationsAntibiotics (Check One Antibiotic Only) Cefazolin (Kefzol) IVPB every eight (8) hours times two (2) doses. Give the first dose in PACU. One (1) gm if patient weighs less than 80kg Two (2) gms if patient weighs more than 80kgOR Clindamycin 600 mg IVPB every six (6) hours times two (2) doses if history of β-lactam allergy.Start six (6) hours after pre-operative dose.OR Vancomycin IVPB, one (1) dose twelve (12) hours after pre-operative dose if history of β-lactam allergy orknown colonization with MRSA. One (1) gm if patient weighs less than 100kg One and half (1.5) gms if patient weighs more than 100kgAnti-Emetics Ondanestron (Zofran) four (4) mg IV every six (6) hours as needed for Nausea/VomitingOR Prochlorperazine (Compazine) ten (10) mg IV every six (6) hours as needed for Nausea/Vomiting Other:_____________________________________________________________________________________Physician’s Signature: Date: Time:Physician’s Printed Name:Transcriber’s Signature: Date: Time:Noting Nurse’s Signature: Date: Time:After faxing order-Check “yes” box, initial and date confirming that it was sent.YES FORM was faxed or copy was tubed to Pharmacy Date: ____/____/____ Time: ________ Initials:____________Form #: HFBH-59-0611MR-0511revCHART TAB: PHYSICIAN ORDERS
Orthopedic SurgeryTotal Joint Replacement:Post <strong>Operative</strong> <strong>Order</strong> <strong>Set</strong> (Page 2 of 5)1. Medications Continued...Comfort/Pain Management MedicationsPCA pump (See PCA order sheet). Discontinue: Morning of ______ post-op day. Other:__________ Anesthesia to manage epidural pain controlChoose One (1) of the following: IV Dextrose five (5) percent/0.45 normal saline:______ ml, infuse at ______ ml/hr. IV Normal saline 0.90 percent: ______ ml, infuse at ______ ml/hr. Saline lock IV when PCA discontinued and last dose of IVPB antibiotics given and tolerating oral diet. Other:_______________________________________________________________________________When PCA pump discontinued begin:FOR SEVERE PAIN Morphine two (2) mg IVP every two (2) hours as needed for severe breakthrough pain OR ______ mgevery ______ hours as needed for severe breakthrough pain or if patient cannot tolerate oral pain medications.OR Hydromorphone (Dilaudid) ______ mg IVP every ______ hours as needed for severebreakthrough pain or if patient cannot tolerate oral pain medications. Oxycodone (Oxycontin)SAMPLE20 mg orally every 12 hours around the clock for severe pain.OR Oxycodone (Oxycontin) 10 mg orally every 12 hours around the clock for severe pain. Ketorolac (Toradol) IVP every six (6) hours as needed for severe pain. Choose one dose 15 mg if 65 years of age or older, less than 50 kg, or renal insufficiency. 30 mgFOR MODERATE PAIN (Choose one) Hydrocodone 7.5 mg/Acetaminophen 500 mg (Lortab 7.5/500) orally ______ tabletevery ______ hours as needed for moderate pain.*OR Oxycodone 5 mg/Acetaminophen 325mg (Percocet 5/325) orally ______ tablet every ______ hoursas needed for moderate pain.*FOR MILD PAIN Acetaminophen 325 mg/Codeine 30 mg (Tylenol #3) orally ______ tablet every ______ hours as needed for mildpain.* Acetaminophen (Tylenol) 650 mg orally as needed every four (4) hours for temperature over 101.5 or headachepain.**WARNING: No more than four (4) grams of Acetaminophen per 24 hours from all sources or two (2)grams of Acetaminophen per 24 hours from all sources in chronic liver disease.Elimination Bowel ProtocolPhysician’s Signature: Date: Time:Physician’s Printed Name:Transcriber’s Signature: Date: Time:Noting Nurse’s Signature: Date: Time:After faxing order-Check “yes” box, initial and date confirming that it was sent.YES FORM was faxed or copy was tubed to Pharmacy Date: ____/____/____ Time: ________ Initials:____________Form #: HFBH-59-0611MR-0511revCHART TAB: PHYSICIAN ORDERS
Orthopedic SurgeryTotal Joint Replacement:Post <strong>Operative</strong> <strong>Order</strong> <strong>Set</strong> (Page 3 of 5)1. Medications Continued...Sleep Zolpidem (Ambien) five (5) mg orally at bed time if needed for sleep Other:__________________________________________________________________________Deep Vein Thrombosis Prophylaxis as per risk assessment (Complete risk assessment sheet) Warfarin (Coumadin) five (5) mg orally the evening of surgery. Physician to dose Warfarin (Coumadin) Pharmacy to dose Warfarin (Coumadin) Enoxaparin (Lovenox) 30 mg Subcutaneously twice a day or 40 mg Subcutaneously daily.Begin post operative day one (1).Knee: Lovenox 30 mg Subcutaneously twice daily for 14 days from date of surgery.Hip: Lovenox 40 mg Subcutaneously every day for 21 days from date of surgery. On day of epidural catheter removal, hold dose of Enoxaparin (Lovenox) for a minimumof two (2) hours after catheter discontinued by anesthesiology. Instruct patient regarding self-administration of Enoxaparin (Lovenox).SAMPLE2. Activity Chair sitting to tolerance. Post operative day number one (1). Bathroom with walker and assistance post operative day one (1). Activity as tolerated TOE-TOUCH, 25%, 50%, 75%, 100% weight bearing Continuous Passive Motion exerciser during the day. Start in Recovery RoomDate:________________________ Degree Range____________________Date:________________________ Degree Range____________________Date:________________________ Degree Range____________________Date:________________________ Degree Range____________________Hip Precautions: Circle: Right or Left extremity pertaining to following orders. Do not internally rotate Do not externally rotate. Do not flex greater than 90 degree. Do not adduct. Abduction pillow (may use regular pillow) day of surgery, then during sleep only. Abduction pillow at all times when in bed. Discontinue after ambulating. <strong>Set</strong> up overhead bar with trapeze. Elevated toilet seat in bathroom. Compression boots bilateral while in bed.Physician’s Signature: Date: Time:Physician’s Printed Name:Transcriber’s Signature: Date: Time:Noting Nurse’s Signature: Date: Time:After faxing order-Check “yes” box, initial and date confirming that it was sent.YES FORM was faxed or copy was tubed to Pharmacy Date: ____/____/____ Time: ________ Initials:____________Form #: HFBH-59-0611MR-0511revCHART TAB: PHYSICIAN ORDERS
Orthopedic SurgeryTotal Joint Replacement:Post <strong>Operative</strong> <strong>Order</strong> <strong>Set</strong>(Page 4 of 5)2. Activity contiued... Knee High TEDS / Thigh High TEDS: Bilateral ACE Wraps: Right / Left / Bilateral Elevate surgical leg. Keep heel off bed. Keep knee straight. Pillow not to be above mid calf ordirectly under knee. Non weight bearing to Right upper extremity Left upper extremity Maintain sling to Right upper extremity Left upper extremity3. SURGICAL SITE CARE Check dressing status every four (4) hours, reinforce as needed After initial dressing change, nurse to change as needed Ice to incision twenty minutes out of every hour Ice to incision continuously Other:____________________________________________________________________________4. Nutritional NeedsCulinary Options from Room Service: Clear liquid initially, advance as tolerated Regular SAMPLEHeart Healthy Consistent Carbohydrate Mechanical Soft5. Monitoring Post-operative vital signs with pulse oximetry reading every 15 minutes times four (4), then every 30 minutes times(2), then every four (4) hours.Notify Physician if: Systolic Blood Pressure greater than 180 or less than 90, Diastolic greater than100 or less than 60, Pulse Oximetry less than 92% Neuro-vascular checks every one (1) hour times (4), then every four (4) hours times 24 hours, then every shift. Jackson Pratt drain Hemovac Drain, monitor and record drainage every shift. Notify surgeon if drainage isgreater than ______ ml. Intake and Output every four (4) hours times 24 hours, then every shift. Notify Physician if urine output less than30 ml per hour if foley present or 120 ml in four (4) hours, notify Physician if less than 240 ml in eight (8) hourswhen no foley present. Assess for other: ___________________________________________________________________6. Labs CBC Post <strong>Operative</strong> day one (1), Post <strong>Operative</strong> day two (2), Post <strong>Operative</strong> day three (3) Electrolytes Post <strong>Operative</strong> day one (1), Post <strong>Operative</strong> day two (2), Post <strong>Operative</strong> day three (3)Physician’s Signature: Date: Time:Physician’s Printed Name:Transcriber’s Signature: Date: Time:Noting Nurse’s Signature: Date: Time:After faxing order-Check “yes” box, initial and date confirming that it was sent.YES FORM was faxed or copy was tubed to Pharmacy Date: ____/____/____ Time: ________ Initials:____________Form #: HFBH-59-0611MR-0511revCHART TAB: PHYSICIAN ORDERS
Orthopedic SurgeryTotal Joint Replacement:Post <strong>Operative</strong> <strong>Order</strong> <strong>Set</strong>(Page 5 of 5)6. Labs continued... BUN Post <strong>Operative</strong> day one (1), Post <strong>Operative</strong> day two (2), Post <strong>Operative</strong> day three (3) Creatinine Post <strong>Operative</strong> day one (1), Post <strong>Operative</strong> day two (2), Post <strong>Operative</strong> day three (3) Glucose Post <strong>Operative</strong> day one (1), Post <strong>Operative</strong> day two (2), Post <strong>Operative</strong> day three (3) Daily PT/INR while on Warfarin (Coumadin)7. Medical Imaging XRAY two (2) VIEWS (AP/LATERAL) OF HIP OR KNEE Circle one: (Right or Left)reason: Prosthesis Placement Do in Recovery Room Done in Recovery Room8. Ancillary <strong>Order</strong>s If Foley present,SAMPLEremove in the morning. If unable to void, perform bladder scan and straight cath for volumegreater than 300ml every six (6) hours. Spirometer 10 times every one (1) hour while awake. Oxygen at ____ liters per nasal cannula until fully reactive, wean off oxygen when room air oxygen saturation isgreater than 92 percent. Peripheral blood glucose before meals and at bed time. See sliding Insulin scale orders.9. CASE MANAGEMENT TO FOLLOWPhysician’s Signature: Date: Time:Physician’s Printed Name:Transcriber’s Signature: Date: Time:Noting Nurse’s Signature: Date: Time:After faxing order-Check “yes” box, initial and date confirming that it was sent.YES FORM was faxed or copy was tubed to Pharmacy Date: ____/____/____ Time: ________ Initials:____________Form #: HFBH-59-0611MR-0511revCHART TAB: PHYSICIAN ORDERS