VIRAPID MONO M&G_EN_05.10.pdf - MD Doctors Direct
VIRAPID MONO M&G_EN_05.10.pdf - MD Doctors Direct
VIRAPID MONO M&G_EN_05.10.pdf - MD Doctors Direct
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
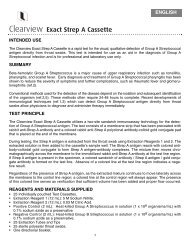
1<strong>EN</strong>Analyte to be detected<strong>VIRAPID</strong> ® <strong>MONO</strong> M&GConjugatepadAntigentest lineAntibodycontrol lineVR001: Immunochromatographic test for the qualitative detection ofEpstein-Barr virus (EBV) markers in serum/citrated plasma samples.25tests.FlowINTRODUCTION:<strong>VIRAPID</strong> ® <strong>MONO</strong> M&G is an immunoassay for the qualitative detectionof 4 serologic markers of Epstein-Barr virus (EBV), two of the IgM class,VCA and heterophile antibodies, and two of the IgG class, VCA andEBNA. This test is for professional use and helps to the diagnosis ofinfectious mononucleosis in serum and citrated plasma samples.Epstein-Barr virus (EBV) is a member of the herpesvirus family and one ofthe most common human viruses. The virus is present worldwide, andmost people become infected with EBV at some point during their lives. Ingeneral terms, as many as 95% of adults between 35 and 40 years of agehave been infected. Infectious mononucleosis is the most common diseasecaused by EBV, leading to fever, cervical adenopathies, splenomegaly, andpharyngitis. Some cases can be caused by cytomegalovirus, Toxoplasmagondii, adenovirus, etc. EBV is also in the origin of proliferativesyndromes in immunosuppressed patients, as well as EBV infection isassociated with Burkitt´s lymphoma and nasopharyngeal carcinoma.Antibodies to several antigen complexes may be measured for detection ofEpstein-Bar virus. These antigens are the viral capsid antigen (VCA), theearly antigen (EA), and the EBV nuclear antigen (EBNA).The presence of IgM antibodies to VCA and absence of antibodies toEBNA, are indicative of primary EBV infection.An increase or high IgG antibody titers to VCA, and a lack of antibodyresponse to EBNA after at least 4 weeks of illness, strongly suggestprimary infection also.In addition, 80% of patients with active EBV infection produce antibodiesto EA. The presence of antibodies to both VCA IgG and EBNA IgG isindicative of past infection (infections ocurred 4-6 months, or even years,earlier). Since 95% of adults have been infected with EBV at some point,most adults will show antibodies to EBV, from earlier infections. High orelevated antibody levels may be present for years and are not necessarilyan indicator of recent infection.The presence of antibodies against erythrocytes of other animal species,called heterophile antibodies, in sera of infectious mononucleosis patientshas been described. The proteins responsible of this agglutination areglycoproteins from the erythrocyte membranes called Paul-Bunnellantigens. These antibodies are present in 80-85% of the adult andadolescent patients and peak in the first month of infection; its detectionhas a high diagnostic value.PRINCIPLE OF THE TEST:When the sample is added into each well of the double cassette, togetherwith the developer solution (VIRCELL DEVELOPER SOLUTION), thecolloidal gold is solubilIzed and the first immunological reaction betweenthe specific antibodies of the serum/citrated plasma and the proteincoupled to the gold particles takes place.The M part bears two conjugates, one coupled with Paul-Bunnell antigen(purified from bovine erythrocytes) and another with EBV p18. Theseproteins react with the Paul-Bunnell heterophile antibodies (PB HA) andthe antibodies against the EBV capside, respectively. The G part bears oneconjugate prepared with a secondary anti-human IgG antibody.Then, these complexes move along the membrane to the correspondingreaction lines (test lines). For the M assay, the first test line corresponds tothe VCA IgM antibodies and contains anti human IgM. The second testline contains Paul-Bunnell antigen. The G part has two lines, EBV p18 andEBNA respectively.Each strip contains a control line for the validation of the assay. This linehas to appear always even if the sample is negative. In both parts, M andG, the control line consists of a secondary antibody against one of theproteins of the conjugate.Sample padKIT FEATURES:<strong>VIRAPID</strong> ® <strong>MONO</strong> M&G test covers in a single assay the four majorserological markers used for the diagnosis of infectious mononucleosiscaused by EBV. The test is accomplished in minutes with the help of amicropipette and a timer and can be read visually.We recommend to read carefully the “Recommendations and precautions”section.KIT CONT<strong>EN</strong>TS:1 VIRCELL <strong>MONO</strong> M&G CASSETTE: 25 cassettes for the specificdetection of Epstein-Barr virus (EBV) markers.2 VIRCELL <strong>MONO</strong> M&G DEVELOPER SOLUTION: 4 ml of bufferedsolution, containing sodium azide.Store at 2-30ºC and check expiration date.Materials required but not supplied:Automatic micropipette and the corresponding tipsChronometerSTORAGE REQUIREM<strong>EN</strong>TS:Store at room temperature or refrigerated, 2-30ºC. DO NOT FREEZE.Do not use the kit reagents beyond the expiry date. This will be valid onlyif reagents are capped and stored at 2-30ºC.STABILITY OF REAG<strong>EN</strong>TS ONCE OP<strong>EN</strong>ED:COMPON<strong>EN</strong>TVIRCELL CASSETTERest of the componentsNitrocellulosemembraneSTABILITY AND HANDLING OF REAG<strong>EN</strong>TS:STABILITYOnce opened, use in the next hourStore at 2-30ºC and use until expiration dateThe kit is stable until the expiration date at 2-30ºC.Handle reagents in aseptic conditions to avoid microbial contaminations.VIRCELL, S.L. does not accept responsibility for the mishandling of thereagents included in the kit.RECOMM<strong>EN</strong>DATIONS AND PRECAUTIONS:Absorbent pad1. For in vitro diagnostic use only. For professional use only.2. Use kit components only. Do not exchange VIRCELL CASSETTESand VIRCELL DEVELOPER SOLUTION between lots and kits.3. Specimens should be handled as in the case of infectious samplesusing safety laboratory procedures.4. Wear protective disposable gloves, laboratory coats and eyeprotection when handling specimens. Wash hands thoroughly aftermanipulating samples.5. Do not use the kit after expiration date.FOR IN VITRO DIAGNOSTIC USEManufacturer: VIRCELL, S.L. Pza. Domínguez Ortiz 1. Polígono Industrial Dos de Octubre.18320 Santa Fe *GRANADA* SPAIN* Tel.+34.958.441264* Fax+34.958.510712http://www.vircell.com
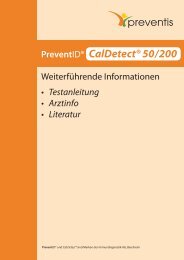
<strong>EN</strong>26. Dispose of unused reagents and waste in accordance with allapplicable regulations.7. Reagents in this kit could include substances of animal and/or humanorigin. Although that material is not infectious, it should be handledas potentially infectious. All material should be handled and disposedas potentially infectious. Observe the local regulations for clinicalwaste disposal.8. The developer solution contains sodium azide. Sodium azide mayreact with metal plumbing, forming explosive components. Upondisposal, flush with plenty of water.9. If the kit or its components (cassettes or developer solution) arestored in the refrigerator, please bring them at room temperaturebefore use.10. The cassettes are stable in their closed pouch until the expiry dateindicated in the label. Do not open until you are ready to perform atest.11. Several tests can be performed at the same time.12. Do not let that the tip of the developer solution bottle touch thesample well in order to prevent contaminations.13. A good performance of the test depends on the correct size of thedrops of developer solution. For this purpose, push the droppersmoothly, allowing the air to pass through into the bottle betweeneach two samples.14. Avoid the use of samples subjected to repeated freezing-thawingcycles as well as hemolyzed samples. Both can produce erroneousresults (signal decrease) or reading failures (lack of visibility).If specific antibodies to each conjugate are present in the sample, thecorresponding test lines will show a positive reaction. A citratedplasma/serum is considered positive if one or several test lines plus thecontrol line appear. The interpretation of the results is carried outaccording to the following chart.Control line1 st Test line: VCA IgMControl line2 nd Test line: PB HA 2 nd Test line: EBNA IgG1 st Test line: VCA IgGSPECIM<strong>EN</strong> COLLECTION AND HANDLING:Blood should be collected aseptically using venipuncture techniques byqualified personnel. Use of sterile or aseptic techniques will preserve theintegrity of the specimen. Serum samples are to be refrigerated (2-8ºC)upon collection or frozen (-20ºC) if the test cannot be performed within 7days. Samples should not be repeatedly frozen and thawed. Do not usehyperlipemic, hemolysed or contaminated sera. Samples containingparticles should be clarified by centrifugation.PRELIMINARY PREPARATION OF THE REAG<strong>EN</strong>TS:All reagents supplied are ready to use.TEST PROCEDURE:1.-Bring all reagents to room temperature before use (approximately 1hour), without removing the cassettes from the pouches.2.-Open the pouch and put the cassette 1 on a flat surface.3.-Add 40 µl of sample into each well with an automatic micropipette,always beginning with the M test. Let the drop be absorbed.4.-Add 2 drops of developer solution 2 onto each well. Do not wait morethan 5 minutes after the sample addition.5.-The result must be read in the following 10-20 minutes.Discard any reading made after 30 minutes.INTERNAL QUALITY CONTROL:Each batch is subjected to internal quality control testing before releasing,complying with highly strict specifications. Final quality control results foreach particular lot are available.INTERPRETATION OF RESULTS AND VALIDATIONPROTOCOL FOR USERS:In order to perform the reading of the test and to determine the positivity ofthe samples, the intensity card included in the kit should be used. 4 levelsof color intensity ranging from 0.5 to 3 can be read. When the intensity islower than 0.5, the result is considered negative. When the intensity ishigher than or equal to 0.5, the result is considered positive.The control line must be always positive and legible if the test has beenperformed correctly. If this line does not appear, the test must beconsidered invalid.Anti-EBV antibodiesPBHAVCA-IgMVCA-IgGEBNA-IgGConditionInterpretation- - - - No infection No contact with EBV+/-* + +/- -- - + +/-***+/- + + +Table. Interpretation of serological markers of the infectious mononucleosis due to EBV.HA: Heterophile antibodies.All the results with the following combination: EBNA-G positive andVCA-G negative, should be considered invalid and repeated and/or othertechniques should be used.LIMITATIONS:Detection of anti-EBVIgM antibodiesRecentinfection**PastinfectionLate primaryinfection+ - - - InconclusiveDetection of anti-EBVIgG antibodies*Children younger than 4 years oldand 20% of adults do not developheterophile antibodies.**In case of getting only the VCA-M positive, it is recommended toanalyze a second sample in 1-2weeks.***When EBNA-G is positive, itcorresponds to a latent pastinfection without evidence of recentinfection.When EBNA-G appears negative, itmay be an EBNA-G false negativeresult and checking with othertechniques is recommended..It is a past infection with IgMlevels still detectableAnalyze a second sample and/or useother techniques.1-This kit is intended to be used with human citrated plasma/serum.2.-The user of this kit is advised to carefully read and understand thepackage insert. Strict adherence to the protocol is necessary to obtainreliable test results.3.-This test will not indicate the site of infection. It is not intended toreplace isolation.4.-As with any diagnostic test, results must be interpreted withconsideration of all clinical and laboratory findings. The kit results may beused in conjunction with clinical evaluation and other diagnosticprocedures.5.-The test provides qualitative results. No correlation can be drawnbetween the magnitude of a positive result and the titer of antibodies in thesample.FOR IN VITRO DIAGNOSTIC USEManufacturer: VIRCELL, S.L. Pza. Domínguez Ortiz 1. Polígono Industrial Dos de Octubre.18320 Santa Fe *GRANADA* SPAIN* Tel.+34.958.441264* Fax+34.958.510712http://www.vircell.com
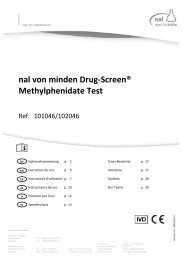
<strong>EN</strong>36.-This test has been verified to be used with human citrated plasma/serum.This test has not been verified with other kinds of samples.7.-Reliable results are dependent on adequate specimen collection,transport, storage and processing procedures.8.-A negative result does not exclude the possibility of infection.9.-A positive test does not rule out the possibility that other pathogens maybe implicated in the disease.10.-CMV infected patients may give false positive results in Epstein-Barrvirus assays.11.-Sera from immunosuppressed patiens may show false negative results.12.-Other diseases (cytomegalovirus, toxoplasmosis, adenovirus andrubella) produce similar syndroms to infectious mononucleosis, and shouldalso be tested in suspected cases of this syndrom.13.-The performance characteristics have not been studied for patients withnasopharyngeal carcinoma, Burkitt´s lymphoma and other EBV associateddiseases different from infectious mononucleosis.14.-Since 95% of adults have been infected with EBV at some point, mostadults will show antibodies to EBV, from earlier infections. High orelevated IgG antibody levels may be present for years and are notnecessarily an indicator of recent infection.15.-The absence of heterophile antibodies is frequent in children.16.-The presence of heterophile antibodies can persist for several monthsin some people.17.-Some patients with past infection do not present IgG response againstEBNA, but only against VCA. In order to rule out a possible acuteinfection, it is recommended to use alternative techniques.PERFORMANCES<strong>EN</strong>SITIVITY AND SPECIFICITY:390 samples were assayed against a commercial available ELISA kit forVCA-G line.390 samples were assayed against a commercial available ELISA kit forEBNA-G line.197 samples were assayed against a commercial available ELISA kit forVCA-M line.197 samples were assayed against a commercial available agglutination kitfor PB line.The results were as follows:Test lines Sensitivity (%) Specificity (%)VCA-M 91 97PB 94 99VCA-G 92 95EBNA-G 91 92INTRA-ASSAY PRECISION:3 samples (one positive close to the detection limit for each test and onenegative) were tested 5 times in a single assay performed by the sameoperator in essentially unchanged conditions.The same results were observed in all the assays.SYMBOLS USED IN LABELS:x∑xyIn vitro diagnostic medical deviceUse by (expiration date)Store at x-y CContains sufficient for testsBatch codeCatalogue numberConsult instructions for useNegative resultPositive result: Low intensityPositive result: High intensity<strong>VIRAPID</strong> ® interpretation chartSUMMARY OF THE ASSAY PROCEDUREAdd 40 µl ofsimple intoeach wellBIBLIOGRAPHY:Add 2 dropsofDevelopersolutionReadingresultsINTER-ASSAY PRECISION:3 samples (one positive close to the detection limit for each test and onenegative) were individually tested on 3 consecutive days by 2 differentoperators.The same results were observed in all the assays.CROSS REACTIVITY AND INTERFER<strong>EN</strong>CES:Sera with high rheumatoid factor titer can produce false positive results inthe VCA IgM test.46 positive samples for rheumatoid factor (RF equal or higher to 2+ in acommercial latex kit) were assayed. 19 of them were false positive forVCA M.All these false positives were negative to HA and positives for Gdeterminations. Because of this the risk of a wrong diagnosis is very low.1. Bruu, A. L., R. Hjetland, E. Holter, L. Mortensen, O. Natas, W.Petterson, A. G. Skar, T. Skarpaas, T. Tjade, and B. Asjo. 2000. Evaluationof 12 commercial tests for detection of Epstein-Barr virus- specific andheterophile antibodies. Clin Diagn Lab Immunol 7:451-6.2. De Paschale, M., Agrappi, C., Manco, MT., Mirri, P., Viganó, EF. AndClerici, P. 2008. Seroepidemiology of EBV and interpretation of the“isolated VCA IgG” pattern. J. Med. Virol. Dec. 23; 81(2):325-331.3. Debyser, Z., M. Reynders, P. Goubau, and J. Desmyter. 1997.Comparative evaluation of three ELISA techniques and an indirectimmunofluorescence assay for the serological diagnosis of Epstein-Barrvirus infection. Clin Diagn Virol 8:71-81.4. Dolken, G., U. Weitzmann, C. Boldt, M. Bitzer, W. Brugger, and G. W.Lohr. 1984. Enzyme-linked immunosorbent assay for IgG antibodies toEpstein-Barr virus-associated early antigens and viral capsid antigen. JImmunol Methods 67:225-33.5. Ho, D. W., P. R. Field, and A. L. Cunningham. 1989. Rapid diagnosis ofacute Epstein-Barr virus infection by an indirect enzyme-linkedimmunosorbent assay for specific immunoglobulin M (IgM) antibodywithout rheumatoid factor and specific IgG interference. J Clin Microbiol27:952-8.FOR IN VITRO DIAGNOSTIC USEManufacturer: VIRCELL, S.L. Pza. Domínguez Ortiz 1. Polígono Industrial Dos de Octubre.18320 Santa Fe *GRANADA* SPAIN* Tel.+34.958.441264* Fax+34.958.510712http://www.vircell.com
<strong>EN</strong>46. Hofmann H, P.-K. Th. 1994. Diagnosis of EBV infection by means ofELISA. Serodiagn Immunother Infect Dis 6:133-139.7. Luka, J., R. C. Chase, and G. R. Pearson. 1984. A sensitive enzymelinkedimmunosorbent assay (ELISA) against the major EBV-associatedantigens. I. Correlation between ELISA and immunofluorescence titersusing purified antigens. J Immunol Methods 67:145-56.8. Niederman, J. C. 1985. Chronicity of Epstein-Barr virus infection. AnnIntern Med 102:119-21.9. Okano, M., G. M. Thiele, J. R. Davis, H. L. Grierson, and D. T. Purtilo.1988. Epstein-Barr virus and human diseases: recent advances indiagnosis. Clin Microbiol Rev 1:300-12.10. CDC (Nacional Center for Infectious Diseases). Epstein-Barr Virus andInfectious Mononucleosis. www.cdc.gov/ncidod/diseases/ebv.htm.11. Valent, C. and Ench, Y. 1985. Epstein-Barr Virus InfectiousMononucleosis in Children. II. Heterophil Antibody and Viral-SpecificResponses. Pediatric, vol. 75, nº 6, June 1985, 1011-1019.For any question please contact:customerservice@vircell.comREVISED: May-10FOR IN VITRO DIAGNOSTIC USEManufacturer: VIRCELL, S.L. Pza. Domínguez Ortiz 1. Polígono Industrial Dos de Octubre.18320 Santa Fe *GRANADA* SPAIN* Tel.+34.958.441264* Fax+34.958.510712http://www.vircell.com